copd and pht - intensivistenopleidingintensivistenopleiding.nl/downloads/files/copd and pht.pdf ·...
TRANSCRIPT
COPD and PHTIntensive Care Training Program
Radboud University Nijmegen Medical Centre

PAO2 ↓
Hypoxic Pulmonary Vasoconstriction
Chronic Obstructive Pulmonary Disease
Pulmonary vascular resistance ↑ / Pulmonary arterial pressure ↑
Cor Pulmonale and RV failure
PHT in COPD
• mPAP > 20 mm Hg (in rest)
• Incidence unknown
• Risk factors: FEV1 < 50% of predicted and PaO2 < 55 mm Hg

Pathology
• Changes in muscular pul- monary arteries and arterioles
• Intima thickening with longitudinal muscle and elastin/collagen deposits
• Increase in smooth muscle cells in media
RV hypertrophy correlates with degree of hypoxemia

PAP = CO
PVR
PCWP

Factors affecting PVR
• Alveolar hypoxia - hypoxic pulmonary vasoconstriction
• Increased PaCO2 and acidosis relatively little effect
• Intrinsic positive end-expiratory pressure
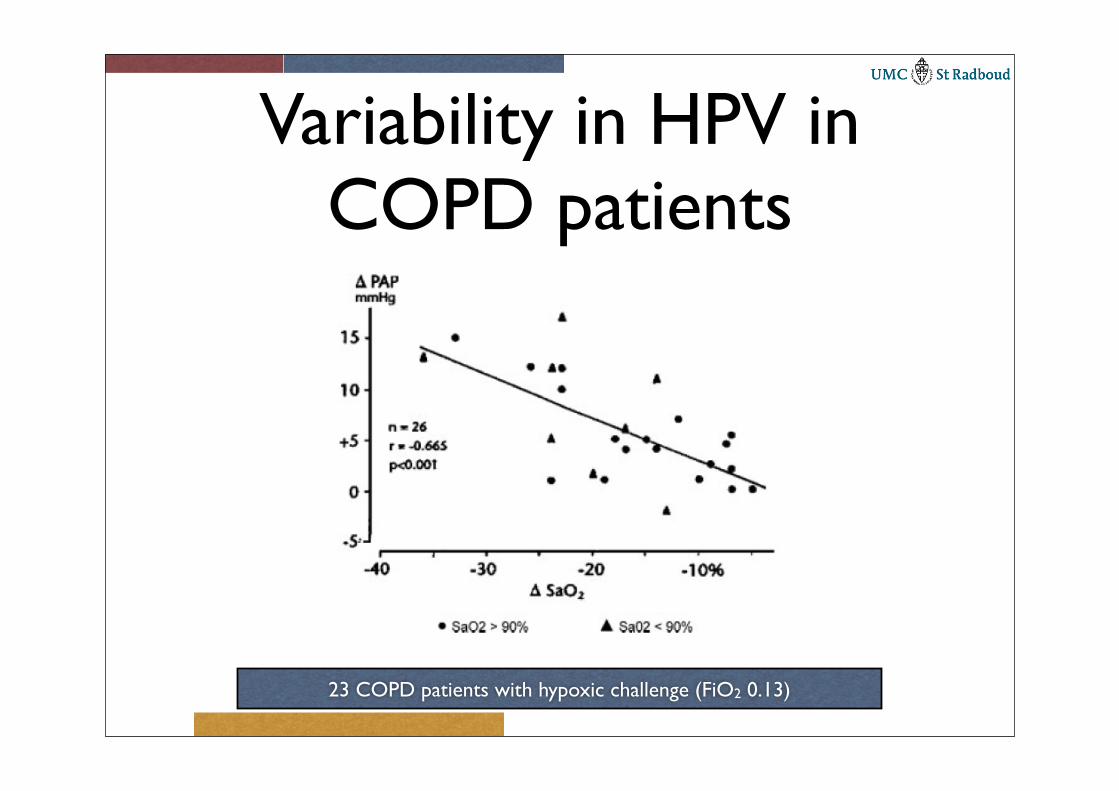
Variability in HPV in COPD patients
23 COPD patients with hypoxic challenge (FiO2 0.13)

Pulmonary hemodynamics in COPD
• mPAP usually between 25 - 30 mm Hg - ≥ 40 mm Hg unusual (FEV1 < 50% and profound hypoxemia)
• mPAP transiently increases during exercise and sleep due to alveolar desaturations
• During exacerbations mPAP may increase with another 20 mm Hg
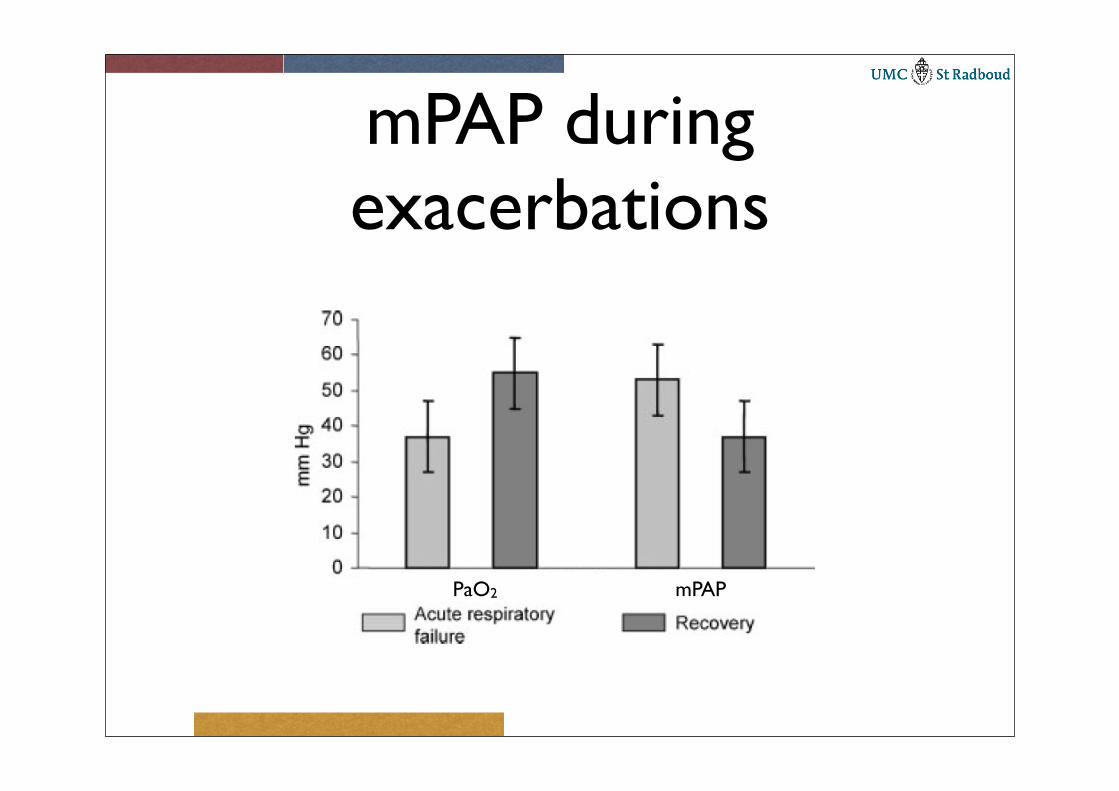
mPAP during exacerbations
PaO2 mPAP
Consequences
• Untreated mPAP increases approximately 3 mm Hg / year
• Longterm survival lower

Longterm survival
RV function in COPD
• Right ventricle has time to adapt
• mPAP ↑ induces hypertrophy and dilatation resulting in dysfunction
• RV stroke work index increases but RV operates on extension of normal RV function
• CO is usually normal (even with edema) and RVEF is decreased

RV function in COPDStrokevolumeml/m2

RV contractilityContractility appears to be well preservedMeasure SV, EF and RVP
24 patients with COPD
RV failure relatively rare
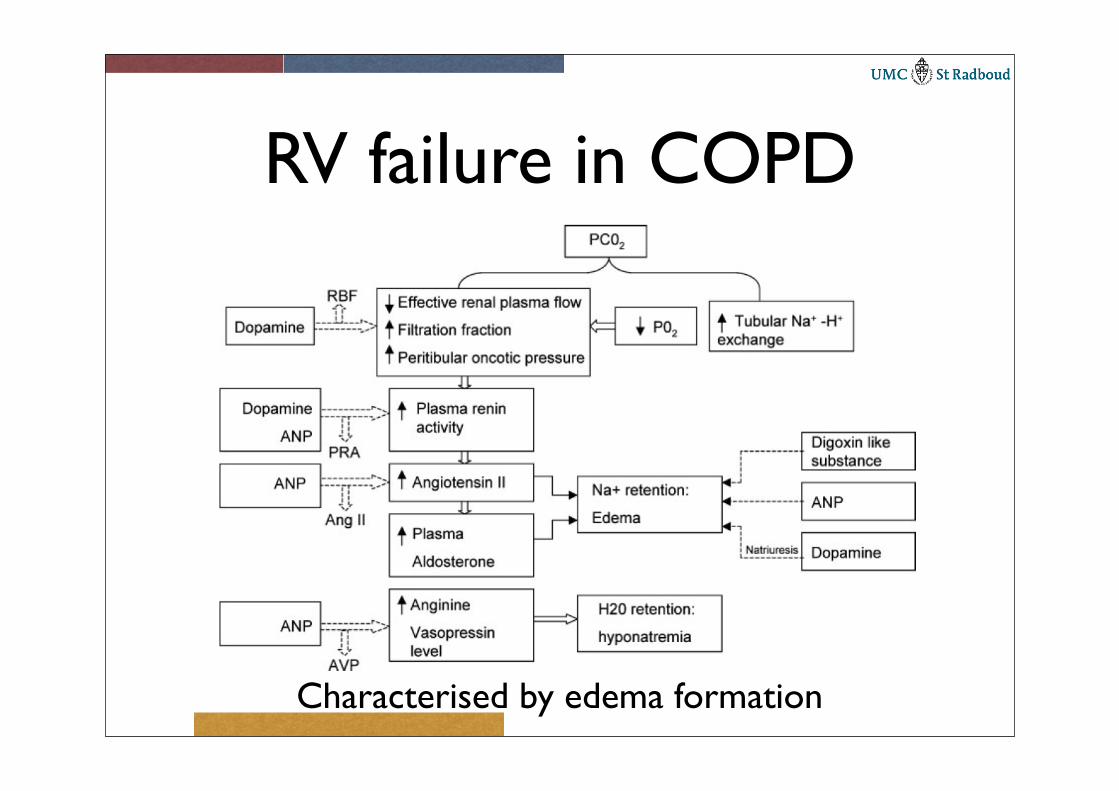
RV failure in COPD
Characterised by edema formation

Basic principles of pressure measurements
P1
P2
V2V1
Modified Bernoulli’s equationGradient (P2 - P1) = 4V22
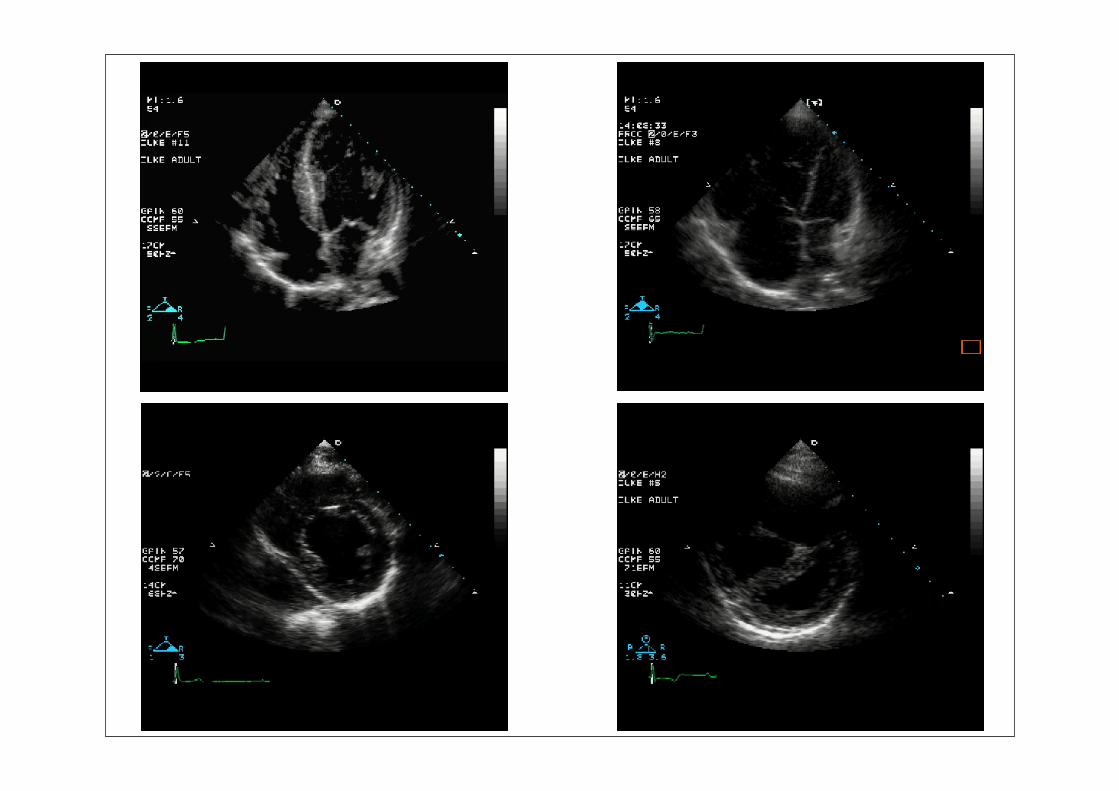
Right-sided pressures
• Size, wall thickness, function, septal shift
• Systolic septal flattening → RVsys ↑
• Diastolic septal flattening → RVdias ↑ unless volume overloaded (suggests RV failure)
Qualitative assessment
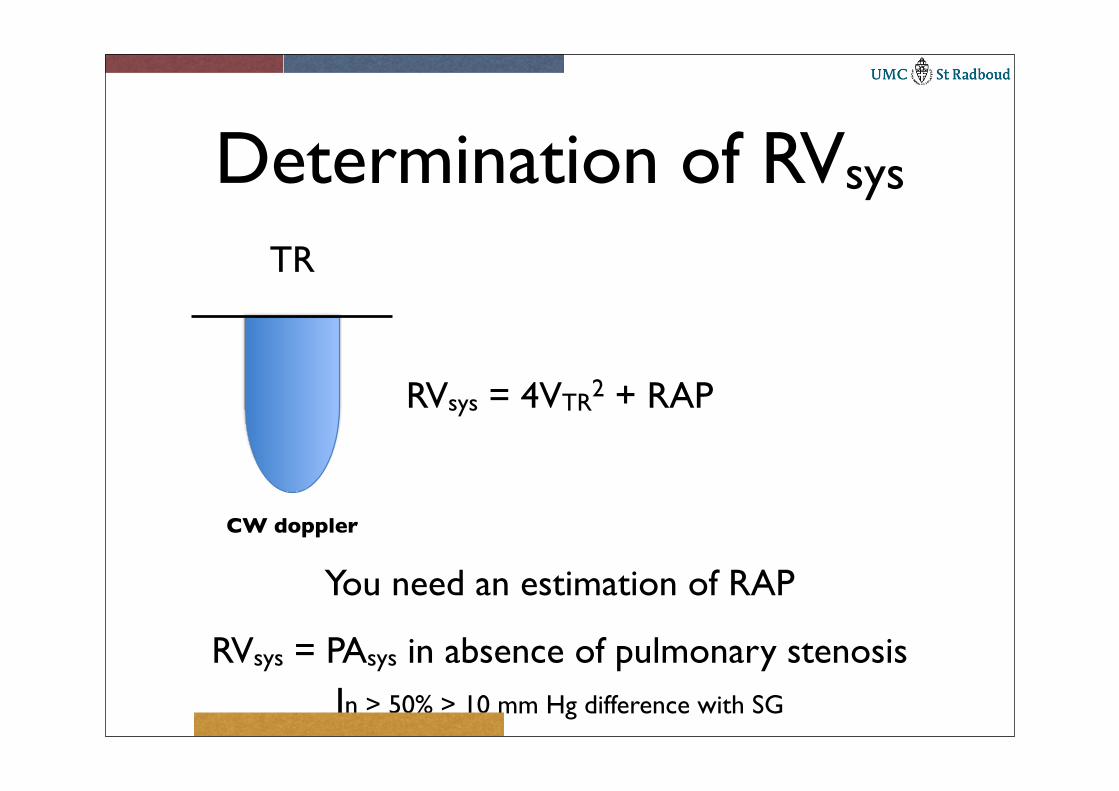
Determination of RVsys
You need an estimation of RAP
RVsys = PAsys in absence of pulmonary stenosis
CW doppler
TR
RVsys = 4VTR2 + RAP
In > 50% > 10 mm Hg difference with SG

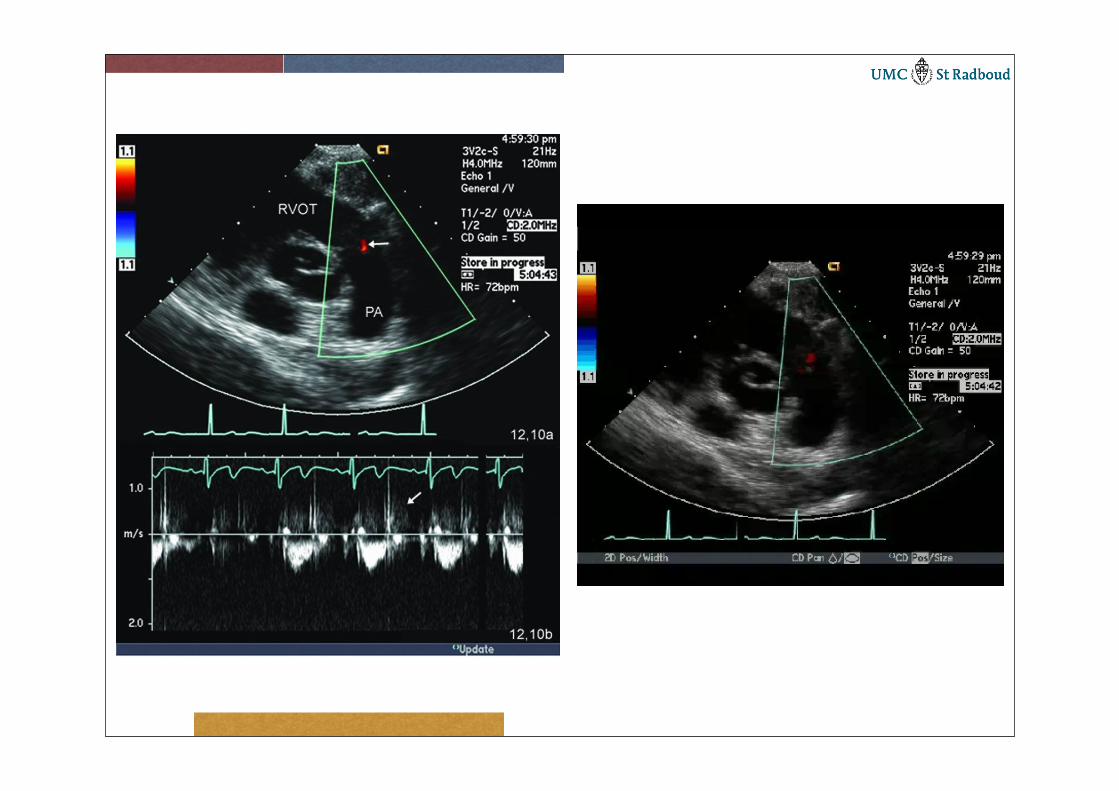
Estimation of PAsys
PAsys = RAP + 4×Vti4
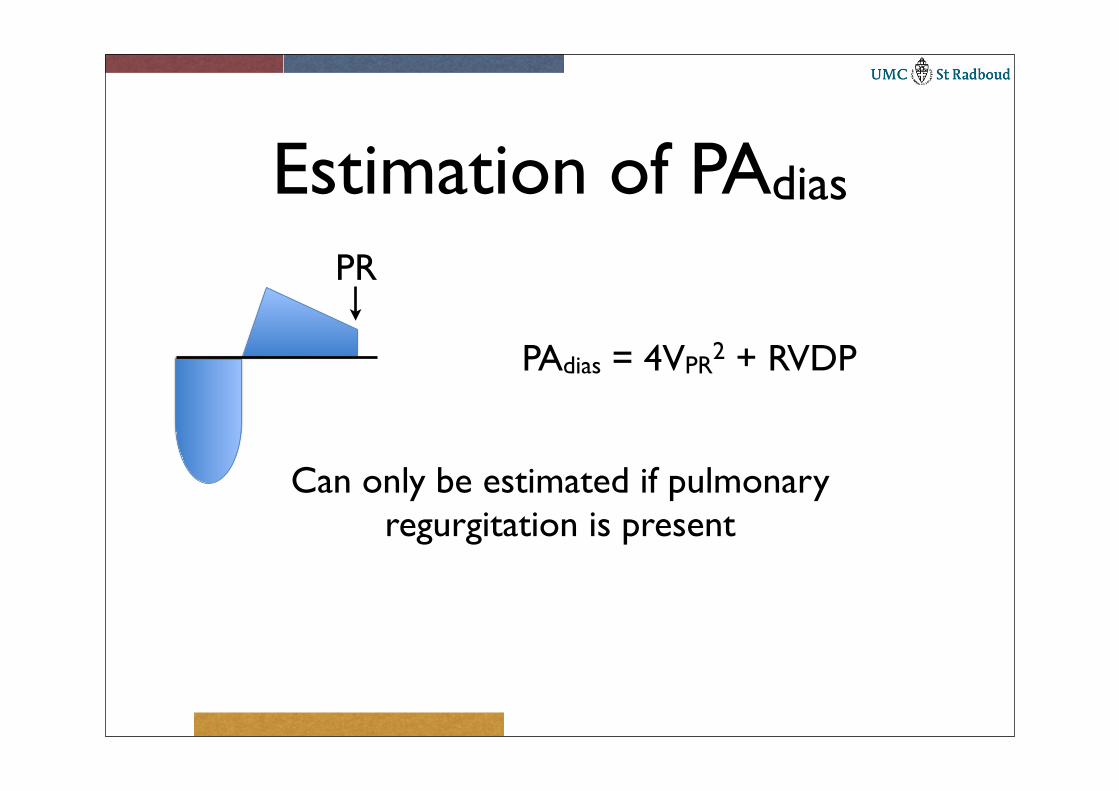
Estimation of PAdias
Can only be estimated if pulmonaryregurgitation is present
PR
PAdias = 4VPR2 + RVDP
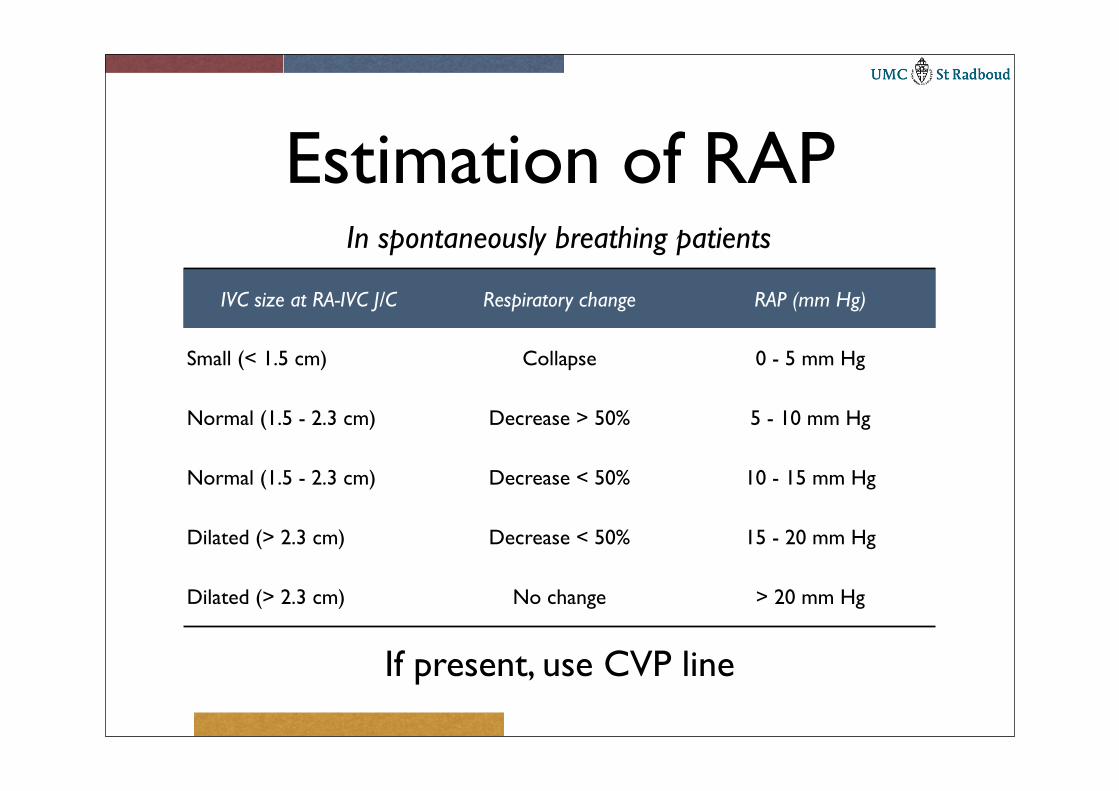
Estimation of RAP
If present, use CVP line
IVC size at RA-IVC J/C Respiratory change RAP (mm Hg)
Small (< 1.5 cm) Collapse 0 - 5 mm Hg
Normal (1.5 - 2.3 cm) Decrease > 50% 5 - 10 mm Hg
Normal (1.5 - 2.3 cm) Decrease < 50% 10 - 15 mm Hg
Dilated (> 2.3 cm) Decrease < 50% 15 - 20 mm Hg
Dilated (> 2.3 cm) No change > 20 mm Hg
In spontaneously breathing patients

IVC at RA junction

Right ventricular function
• TAPSE
• Right Ventricular Performance Index
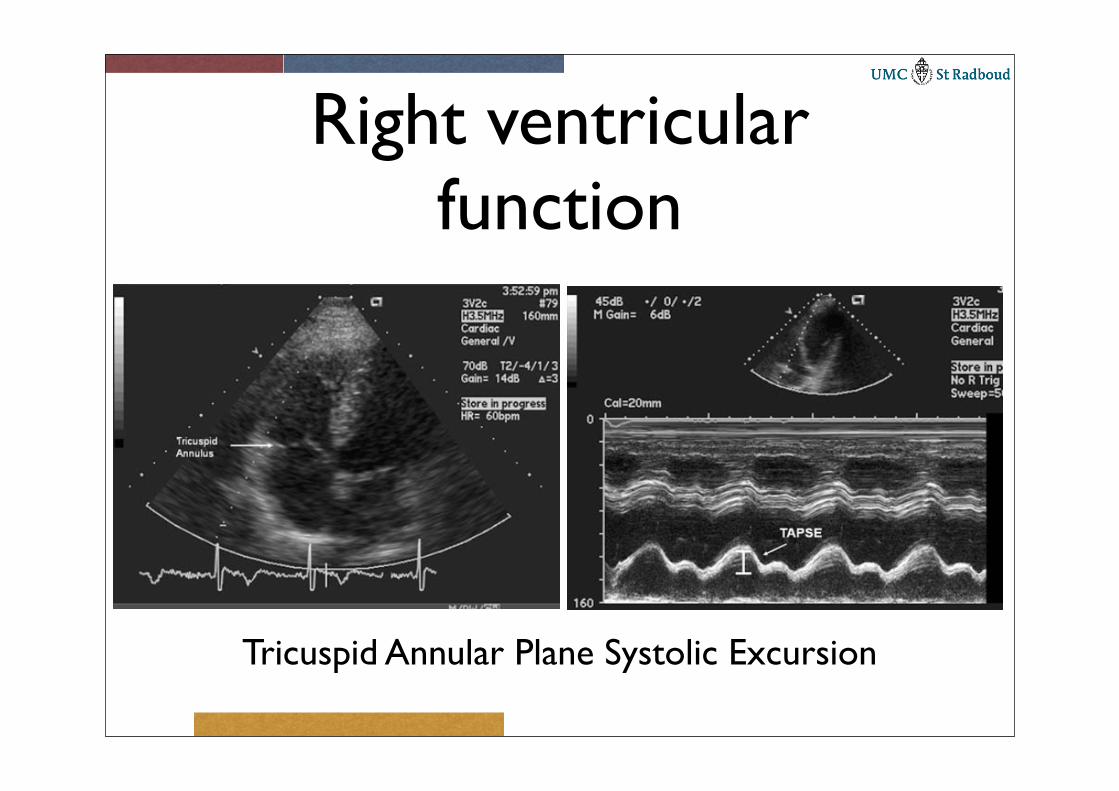
Right ventricular function
Tricuspid Annular Plane Systolic Excursion
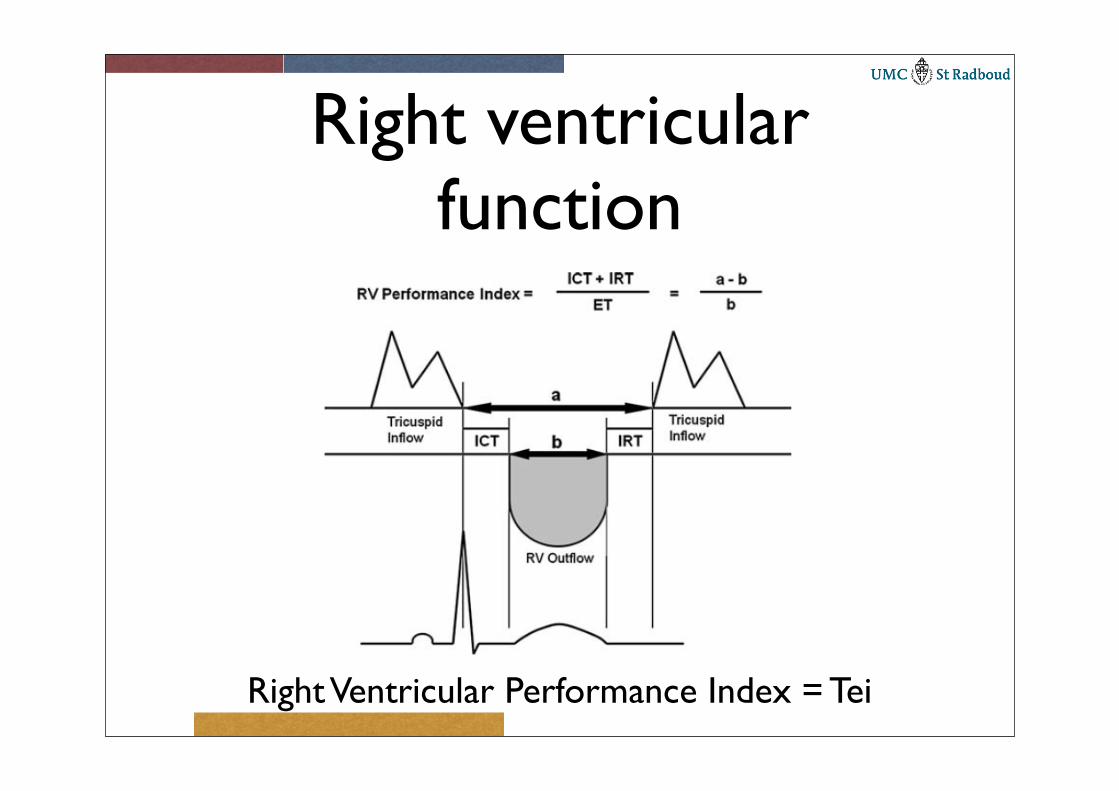
Right ventricular function
Right Ventricular Performance Index = Tei
Treatment
• Oxygen
• Vasodilators
• Reduction in hematocrit
• Diuretics