cost analysis of amlodipine versus enalapril in patients with coronary artery disease and normal...
TRANSCRIPT

Cost Analysis of Amlodipine versusEnalapril in Patients with Coronary ArteryDisease and Normal Blood PressureFindings from the CAMELOT Economic Substudy
Joseph Menzin,1 Luke Boulanger,1 Simon Tang,2 Kamlesh Thakker2 and Steven E. Nissen3
1 Boston Health Economics, Inc., Waltham, Massachusetts, USA
2 Pfizer Inc., New York, New York, USA
3 Cleveland Clinic Foundation, Cleveland, Ohio, USA
Abstract Objectives: To analyse 2-year hospitalization and cost data collected during a
prospective, double-blind, randomized, controlled trial comparing amlodi-
pine, enalapril and placebo in normotensive patients with coronary artery
disease (CAD).
Methods: All patients who were enrolled in the CAMELOT study were in-
cluded in this economic substudy. Patients with CAD and normal blood
pressure were randomized to amlodipine, enalapril or placebo, and followed
up for 24 months (between 1999 and 2004). Data on hospitalizations and
medication use were obtained from the clinical trial. Costs were assigned from
secondary sources. Total costs ($US, year 2004 values) were estimated as the
sum of costs associated with cardiovascular hospitalizations, study medica-
tions and concomitant cardiovascular medications. Costs and resource use
were analysed by treatment arm overall and for selected patient subgroups.
Cost differences were evaluated using nonparametric bootstrap techniques.
Results: Of 1991 patients enrolled, 663 were treated with amlodipine, 673
were treated with enalapril and 655 were treated with placebo. Significantly
fewer patients were hospitalized for cardiovascular reasons in the amlodipine
group (16.4%) than in the placebo group (22.7%; p < 0.01), but not compared
with the enalapril group (20.1%; p = 0.09). The amlodipine group also had
numerically fewer days in hospital per patient (1.1) than the enalapril (1.3)
and placebo (1.5) groups. Mean 2-year per-patient costs in the amlodipine
group were estimated to be $US609 and $US717 lower than for the placebo
and enalapril groups, respectively.
Conclusions: These results suggest that use of amlodipine may reduce costs of
care among CAD patients with normal blood pressure.
ORIGINAL RESEARCH ARTICLEAppl Health Econ Health Policy 2008; 6 (2-3): 157-162
1175-5652/08/0002-0157/$48.00/0
ª 2008 Adis Data Information BV. All rights reserved.

Background and Objectives
The CAMELOT (Comparison of Amlodipineversus Enalapril to Limit Occurrences ofThrombosis) study was a multicentre, double-blind, randomized, controlled trial designed tocompare the efficacy of a calcium channel an-tagonist (amlodipine) with that of an ACE in-hibitor (enalapril) and with placebo to evaluatewhether patients with coronary artery disease(CAD) and normal blood pressure can benefitfrom further antihypertensive therapy.[1,2] Thestudy found that, over 2 years, participantsrandomized to amlodipine had a significantly(p< 0.05) lower likelihood of cardiovascularevents than those administered placebo, butnot significantly lower than those administeredenalapril (p= 0.09).[1]
Economic outcomes are increasingly collectedalongside health outcomes in clinical trials, aspayers grow more interested in the cost effec-tiveness of available therapies.[3] While differ-ences in the number of cardiovascular events maytranslate into differences in hospitalization ratesand costs, the cost of drug therapy needs to beplaced in the context of these potential benefits.For this reason, we undertook a prospectiveeconomic substudy in conjunction with CAME-LOT. The objectives were to document the ratesof cardiovascular-related hospitalizations andcosts of care during the 2 years of each patient’sparticipation in the study.
Methods
All patients who were randomized to receivetreatment during the CAMELOT trial were in-cluded in this economic substudy. The patientcharacteristics and methods of the CAMELOTstudy have been reported previously.[1] Briefly, atotal of 1991 patients with CAD (defined as >20%stenosis by coronary angiography) and normaldiastolic blood pressure (defined as <100 mmHg)were randomized in a double-blind manner toreceive amlodipine besylate (10 mg), enalapril(20 mg) or placebo for 24 months. The study wasconducted between April 1999 and March 2004at 100 study sites in the US, Canada and Europe.
Study Measures
Resource utilization data were prospectivelycollected in the CAMELOT clinical trial todocument hospitalizations (cardiovascular andother), study medications and concomitantcardiovascular-related medications. Several sec-ondary sources of data were employed toestimate unit costs for cardiovascular hospitali-zations andmedications. Overall, cardiovascular-related costs of care were estimated as the sumof costs for study medications, concomitantcardiovascular medications and cardiovascularhospitalizations.
Hospitalization data were obtained for allacute-care admissions that occurred during the2 years after study enrollment. Both overall andICU lengths of stay were calculated for eachhospitalization. Cardiovascular hospitalizationswere defined as acute-care admissions for one ormore of the following major coronary events pre-specified in the CAMELOT protocol as end-points: myocardial infarction, congestive heartfailure, resuscitated cardiac arrest, coronary re-vascularization, new-onset peripheral vasculardisease, hospitalized angina, non-fatal stroke andtransient ischaemic attack. When multiple trialendpoint events occurred during a single hospi-talization, multiple reasons for admission wereassigned to the stay (e.g. angina and revascular-ization occurring during same stay were countedas both angina and revascularization).
Secondary sources of data were used to esti-mate costs. For cardiovascular hospitalizations,the mean total charge per stay was estimatedbased on discharge diagnoses and proceduresused for acute-care hospital stays included in theHealthcare Cost and Utilization Project (HCUP)database.[4] Charges were converted to costsusing hospital-specific cost-to-charge ratios[5]
and the costs for inpatient physician services wereassigned using the Medicare physician fee sche-dule.[6] These costs per stay were then calculatedas the cost per day of inpatient treatment andapplied to the number of hospital days docu-mented for CAMELOT participants for the samediagnosis. The HCUP database did not containICU days, so the estimated mean daily costs were
158 Menzin et al.
ª 2008 Adis Data Information BV. All rights reserved. Appl Health Econ Health Policy 2008; 6 (2-3)
based on the overall length of stay for each admis-sion. Average wholesale prices were obtainedfrom the RED BOOK� database[7] to assign unitcosts to study medications and other cardiovas-cular medications used by CAMELOT partici-pants. Generic prices were used where applicable,including for enalapril. Costs incurred in thesecond year of follow-up were discounted at arate of 3%. All costs were expressed in $US,year 2004 values.
Data Analyses
The proportion of patients in each study armwho experienced at least one cardiovascular hos-pitalization was analysed using the Cochran-Mantel-Haenszel test. This was the only economicmeasure that was tested, as specified prospectivelyin the substudy analytic plan. In addition, a de-scriptive analysis of this measure was undertakenfor patient subgroups defined by the followingbaseline characteristics: age (<65 vs ‡65 years); sex;sitting systolic blood pressure (relative to theCAMELOT study mean); statin dispensed versusnot dispensed; and presence of diabetes mellitus,metabolic syndrome and impaired fasting glucose.
To estimate 95% confidence intervals for costs,nonparametric bootstrapping techniques wereused, as cost data were notNormally distributed.[8]
Based on the simulated distribution of costs, wealso calculated the likelihood that amlodipinewas cost saving relative to placebo and enalapril.[9]
All data analyses were conducted using SASversion 9.1 (SAS Institute, Cary, NC, USA).
Results
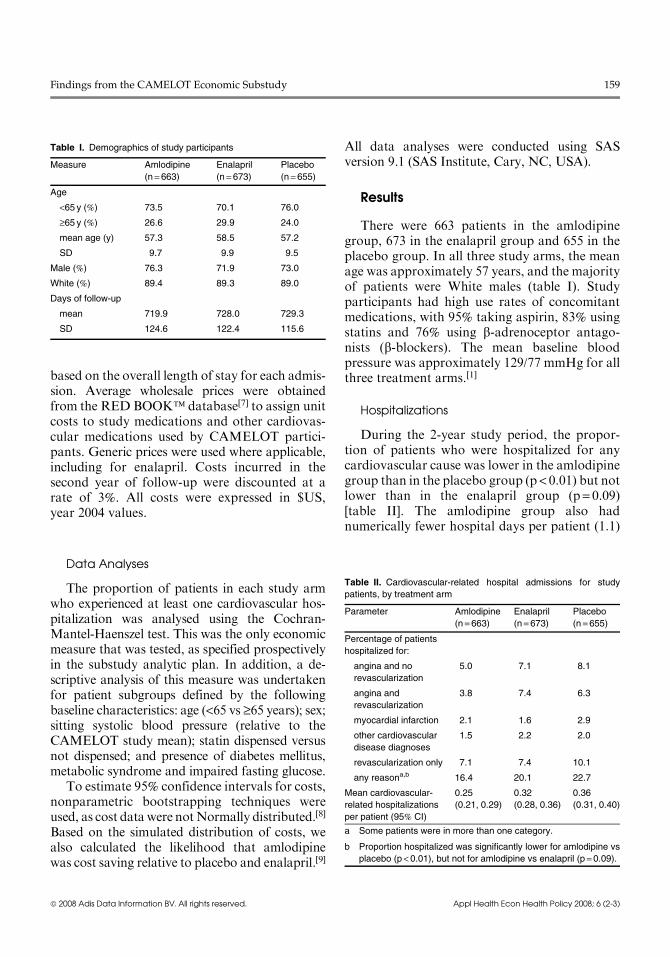
There were 663 patients in the amlodipinegroup, 673 in the enalapril group and 655 in theplacebo group. In all three study arms, the meanage was approximately 57 years, and the majorityof patients were White males (table I). Studyparticipants had high use rates of concomitantmedications, with 95% taking aspirin, 83% usingstatins and 76% using b-adrenoceptor antago-nists (b-blockers). The mean baseline bloodpressure was approximately 129/77 mmHg for allthree treatment arms.[1]
Hospitalizations
During the 2-year study period, the propor-tion of patients who were hospitalized for anycardiovascular cause was lower in the amlodipinegroup than in the placebo group (p < 0.01) but notlower than in the enalapril group (p = 0.09)[table II]. The amlodipine group also hadnumerically fewer hospital days per patient (1.1)
Table I. Demographics of study participants
Measure Amlodipine
(n= 663)Enalapril
(n = 673)Placebo
(n =655)
Age
<65 y (%) 73.5 70.1 76.0
‡65 y (%) 26.6 29.9 24.0
mean age (y) 57.3 58.5 57.2
SD 9.7 9.9 9.5
Male (%) 76.3 71.9 73.0
White (%) 89.4 89.3 89.0
Days of follow-up
mean 719.9 728.0 729.3
SD 124.6 122.4 115.6
Table II. Cardiovascular-related hospital admissions for study
patients, by treatment arm
Parameter Amlodipine
(n =663)Enalapril
(n =673)Placebo
(n =655)
Percentage of patients
hospitalized for:
angina and no
revascularization
5.0 7.1 8.1
angina and
revascularization
3.8 7.4 6.3
myocardial infarction 2.1 1.6 2.9
other cardiovascular
disease diagnoses
1.5 2.2 2.0
revascularization only 7.1 7.4 10.1
any reasona,b 16.4 20.1 22.7
Mean cardiovascular-
related hospitalizations
per patient (95% CI)
0.25
(0.21, 0.29)
0.32
(0.28, 0.36)
0.36
(0.31, 0.40)
a Some patients were in more than one category.
b Proportion hospitalized was significantly lower for amlodipine vs
placebo (p <0.01), but not for amlodipine vs enalapril (p =0.09).
Findings from the CAMELOT Economic Substudy 159
ª 2008 Adis Data Information BV. All rights reserved. Appl Health Econ Health Policy 2008; 6 (2-3)

than the enalapril (1.3 days) and placebo (1.5days) groups (table III). The largest benefits ofamlodipine in terms of the likelihood of cardio-vascular hospitalization were seen in women,patients aged >65 years, patients with diabetesmellitus and those who were dispensed HMG-CoA reductase inhibitors (statins) [table IV].
Costs
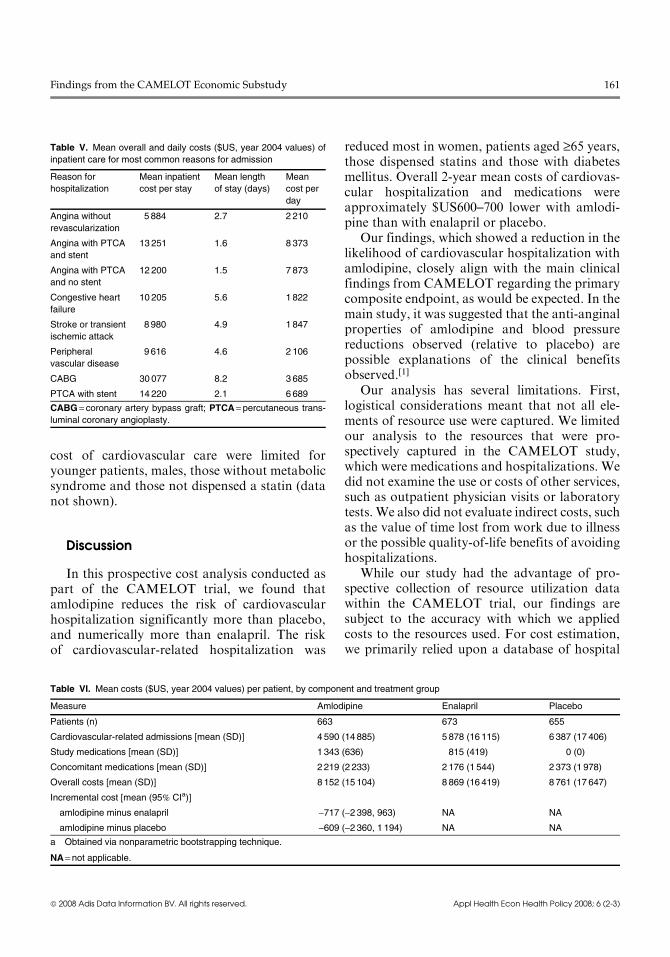
The mean inpatient costs assigned to the staysobserved in the CAMELOT study are shown intable V. The average cost per stay ranges fromabout $US5900 for angina without revascular-ization to $US30 100 for coronary artery bypassgraft. Mean daily costs are highest for anginawith percutaneous transluminal coronary angio-plasty and stent, and lowest for congestive heartfailure.
The overall mean cost per patient over 2 yearswas $US8152 for the amlodipine group, whichwas an average of $US717 less than for theenalapril group and $US609 less than for theplacebo group (table VI). Use of amlodipineresulted in cost savings versus placebo andenalapril in 74% and 81% of bootstrap simula-tions, respectively.
Mean costs varied among patient subgroups.For females, patients aged ‡65 years, statin usersand patients with metabolic syndrome, mean2-year per-patient costs of cardiovascular-relatedcare were estimated to be approximately$US1000–5000 lower with amlodipine than withenalapril, and approximately $US1000–2000lower than with placebo; however, the effects ofamlodipine versus enalapril or placebo on the
Table III. Cardiovascular-related hospital days per patient, by
treatment arm
Cardiovascular-related
hospital days
Amlodipine
(n = 663)Enalapril
(n =673)Placeboa
(n= 654)
ICU or CCU days
Mean 0.3 0.4 0.4
SD 1.5 1.8 1.8
Non-ICU and non-CCU days
Mean 0.8 0.9 1.0
SD 2.8 2.9 3.3
Total
Mean 1.1 1.3 1.5
SD 3.5 3.8 4.0
Minimum 0 0 0
Median 0 0 0
Maximum 41 46 41
a One patient was excluded from this analysis due to missing
admission and discharge dates.
CCU = coronary care unit.
Table IV. Cardiovascular hospitalizations by treatment arm and patient subgroup
Patient subgroup Cardiovascular hospitalizations (%) Rate ratio (95% CI)
AML ENA PL AML vs ENA AML vs PL
<65 years old 16.8 18.6 21.5 0.90 (0.63, 1.23) 0.78 (0.54, 1.02)
‡65 years old 15.3 23.4 26.8 0.66 (0.35, 1.00) 0.57 (0.29, 0.85)
Male 17.4 18.2 22.6 0.96 (0.68, 1.31) 0.77 (0.53, 0.99)
Female 13.4 24.9 23.2 0.54 (0.26, 0.82) 0.58 (0.29, 0.91)
Blood pressure < CAMELOT mean 15.0 19.1 21.2 0.79 (0.50, 1.12) 0.71 (0.44, 0.97)
Blood pressure ‡CAMELOT mean 18.0 21.2 24.4 0.85 (0.55, 1.20) 0.74 (0.46, 1.00)
Statin dispensed 16.7 21.8 24.1 0.77 (0.53, 0.97) 0.69 (0.47, 0.85)
Statin not dispensed 15.2 12.2 15.5 1.24 (0.61, 2.72) 0.98 (0.46, 2.04)
Diabetes mellitus 19.1 29.7 29.2 0.64 (0.30, 1.03) 0.65 (0.31, 1.04)
No diabetes mellitus 15.9 18.0 21.1 0.88 (0.63, 1.18) 0.75 (0.52, 0.96)
Metabolic syndrome 14.9 23.4 21.9 0.64 (0.37, 0.88) 0.68 (0.40, 0.96)
No metabolic syndrome 17.6 17.9 23.3 0.98 (0.67, 1.41) 0.75 (0.49, 1.00)
Impaired fasting glucose 12.6 19.8 23.1 0.64 (0.29, 1.19) 0.55 (0.24, 0.95)
Normal fasting glucose 17.4 20.1 22.7 0.86 (0.62, 1.13) 0.76 (0.53, 0.97)
AML = amlodipine; ENA = enalapril; PL =placebo.
160 Menzin et al.
ª 2008 Adis Data Information BV. All rights reserved. Appl Health Econ Health Policy 2008; 6 (2-3)
cost of cardiovascular care were limited foryounger patients, males, those without metabolicsyndrome and those not dispensed a statin (datanot shown).
Discussion
In this prospective cost analysis conducted aspart of the CAMELOT trial, we found thatamlodipine reduces the risk of cardiovascularhospitalization significantly more than placebo,and numerically more than enalapril. The riskof cardiovascular-related hospitalization was
reduced most in women, patients aged ‡65 years,those dispensed statins and those with diabetesmellitus. Overall 2-year mean costs of cardiovas-cular hospitalization and medications wereapproximately $US600–700 lower with amlodi-pine than with enalapril or placebo.
Our findings, which showed a reduction in thelikelihood of cardiovascular hospitalization withamlodipine, closely align with the main clinicalfindings from CAMELOT regarding the primarycomposite endpoint, as would be expected. In themain study, it was suggested that the anti-anginalproperties of amlodipine and blood pressurereductions observed (relative to placebo) arepossible explanations of the clinical benefitsobserved.[1]
Our analysis has several limitations. First,logistical considerations meant that not all ele-ments of resource use were captured. We limitedour analysis to the resources that were pro-spectively captured in the CAMELOT study,which were medications and hospitalizations. Wedid not examine the use or costs of other services,such as outpatient physician visits or laboratorytests. We also did not evaluate indirect costs, suchas the value of time lost from work due to illnessor the possible quality-of-life benefits of avoidinghospitalizations.
While our study had the advantage of pro-spective collection of resource utilization datawithin the CAMELOT trial, our findings aresubject to the accuracy with which we appliedcosts to the resources used. For cost estimation,we primarily relied upon a database of hospital
Table V. Mean overall and daily costs ($US, year 2004 values) of
inpatient care for most common reasons for admission
Reason for
hospitalization
Mean inpatient
cost per stay
Mean length
of stay (days)
Mean
cost per
day
Angina without
revascularization
5 884 2.7 2 210
Angina with PTCA
and stent
13 251 1.6 8 373
Angina with PTCA
and no stent
12 200 1.5 7 873
Congestive heart
failure
10 205 5.6 1 822
Stroke or transient
ischemic attack
8 980 4.9 1 847
Peripheral
vascular disease
9616 4.6 2 106
CABG 30 077 8.2 3 685
PTCA with stent 14 220 2.1 6 689
CABG = coronary artery bypass graft; PTCA = percutaneous trans-
luminal coronary angioplasty.
Table VI. Mean costs ($US, year 2004 values) per patient, by component and treatment group
Measure Amlodipine Enalapril Placebo
Patients (n) 663 673 655
Cardiovascular-related admissions [mean (SD)] 4 590 (14 885) 5 878 (16 115) 6 387 (17 406)
Study medications [mean (SD)] 1 343 (636) 815 (419) 0 (0)
Concomitant medications [mean (SD)] 2 219 (2 233) 2 176 (1 544) 2 373 (1 978)
Overall costs [mean (SD)] 8 152 (15 104) 8 869 (16 419) 8 761 (17 647)
Incremental cost [mean (95% CIa)]
amlodipine minus enalapril -717 (-2398, 963) NA NA
amlodipine minus placebo -609 (-2360, 1 194) NA NA
a Obtained via nonparametric bootstrapping technique.
NA= not applicable.
Findings from the CAMELOT Economic Substudy 161
ª 2008 Adis Data Information BV. All rights reserved. Appl Health Econ Health Policy 2008; 6 (2-3)

discharge summaries, which are vulnerable tocoding inaccuracies.[10] Furthermore, approxi-mately 10% of subjects were from non-UScentres. We applied US costs to all observedhospitalizations regardless of country. Finally,the CAMELOT trial was powered around clin-ical rather than economic outcomes, and costdata often exhibit considerable variability. Forthis reason, cost data were analyzed descriptively.However, it is notable that nonparametric boot-strap analyses suggest that amlodipine is reason-ably likely to be cost saving.
Our results align with the conclusions of pre-vious model-based economic analyses that foundcost savings and lower cardiovascular hospitali-zation rates with amlodipine. Casciano et al.[11]
constructed a Markov model using data fromPREVENT (Prospective Evaluation of the Vas-cular Effects of Norvasc Trial), a pilot study forCAMELOT. As in CAMELOT, PREVENTparticipants had CAD and were randomized toeither amlodipine or placebo. In the model,healthcare payers saved $US2566 when CADpatients were administered amlodipine over a3-year period (year 1999 value). Most of thesesavings were realized through reductions in car-diovascular hospitalizations.
Conclusion
This economic substudy of the CAMELOTtrial suggests that amlodipine may reduce costs ofcare among CAD patients with normal bloodpressure. Further analyses of the cost effective-ness of amlodipine in this patient population arewarranted.
Acknowledgements
The authors gratefully acknowledge Lisa M. Lines, MPH,ELS, of Boston Health Economics for editorial assistancewith the manuscript. Financial support for this studywas provided by Pfizer Inc., Global Outcomes Research,
New York, NY, USA, to Boston Health Economics, Inc. Jo-seph Menzin and Luke Boulanger received research fundingfrom Pfizer Inc. Simon Tang and Kamlesh Thakker are em-ployees of Pfizer Inc. For Steven E. Nissen’s conflicts of in-terest, please see the supplementary material [‘ArticlePlus’] athttp://healtheconomics.adisonline.com.
References1. Nissen SE, Tuzcu EM, Libby P, et al. Effect of anti-
hypertensive agents on cardiovascular events in patientswith coronary disease and normal blood pressure: theCAMELOT study. A randomized controlled trial. JAMA2004; 292: 2217-25
2. Pepine CJ. What is the optimal blood pressure and drugtherapy for patients with coronary artery disease? JAMA2004; 292: 2271-3
3. Cook J, Drummond M, Heyse JF. Economic endpoints inclinical trials. Stat Methods Med Res 2004; 13: 157-76
4. Agency for Healthcare Research and Quality (AHRQ), U.S.Department of Health and Human Services. HealthcareCost and Utilization Project (HCUP) April, 2006 [online].Available from URL: http://www.ahrq.gov/data/hcup[Accessed 2006 Apr 30]
5. US Department of Health and Human Services, Centers forMedicare and Medicaid Services. Hospital cost report,CMS-2552-96: fiscal years 1996-2000, fiscal years 2001-current. 2005 Dec 19 [online]. Available from URL: http://www.cms.hhs.gov/CostReports/02_HospitalCostReport.asp[Accessed 2006 Dec 1]
6. US Department of Health and Human Services, Centers forMedicare and Medicaid Services. Physician fee schedule:overview. 2005 Dec 14 [online]. Available from URL:http://www.cms.hhs.gov/PhysicianFeeSched/ [Accessed 2006Dec 1]
7. RED BOOK� data services. Greenwood Village (CO):Thomson Micromedex, 2006
8. Chaudhary MA, Stearns SC. Estimating confidence inter-vals for cost-effectiveness ratios: an example from a ran-domized trial. Stat Med 1996; 15: 1447-58
9. Vera-Llonch M, Menzin J, Richner RE, et al. Cost-effectiveness results from the US Carvedilol Heart FailureTrials Program. Ann Pharmacother 2001; 35: 846-51
10. Iezzoni LI. Assessing quality using administrative data. AnnIntern Med 1997; 127: 666-74
11. Casciano R, Doyle JJ, Chen J, et al. Economic benefits ofamlodipine treatment in patients with coronary arterydisease. Pharmacoeconomics 2002; 20: 553-63
Correspondence: Dr Joseph Menzin, Boston Health Eco-nomics, Inc., 20 Fox Road, Waltham, MA 02451, USA.E-mail: [email protected]
162 Menzin et al.
ª 2008 Adis Data Information BV. All rights reserved. Appl Health Econ Health Policy 2008; 6 (2-3)