couple relationship quality and contraceptive … relationship quality and contraceptive...
TRANSCRIPT

COUPLE RELATIONSHIP QUALITY AND
CONTRACEPTIVE DECISION-MAKING IN
, GHANA
Wednesday Noon Seminar Series
Johns Hopkins Bloomberg School of Public Health
Department of Population, Family and Reproductive Health
October 24, 2012
Carie Muntifering Cox, MPH, PhD
Monitoring, Evaluation and Research Advisor
IntraHealth International

Overview 2
Background
Contraceptive Use
Relationship Quality
Study Design and Results
Objective
Methods
Findings
Implications and Next Steps

Contraceptive Use 3
Beneficial for women, families, communities, and countries
Over 200 million women have an unmet need for family planning*
2012 London Summit on Family Planning – Renewed efforts and commitment in family planning
Contraceptive use is stagnant or declining in many West African countries
*Singh, S., & Darroch, J. E. (2012). Adding it up: Costs and benefits of contraceptive
services - Estimates for 2012. New York: Guttmacher Institute and UNFPA

What is Couple Relationship Quality
and Why Does it Matter? 4
Spanier & Lewis’ definition of marital quality:
The subjective evaluation of a married
couple’s relationship on a number of
dimensions and evaluations*
Majority of individuals spend a substantial
portion of their adult lives in one or more
intimate relationships.
*Spanier G.B. & Lewis R.A. 1980. Marital Quality: A Review of the Seventies. Journal of
Marriage and Family, 42:4, 825-839.

Relationship Quality, Health, and
Well-Being 5
Relationship quality is associated with:
Individual well-being
Physical and mental health
Family health and development
Emerging research also suggests that it is
associated with contraceptive use

Relationship Quality and Contraceptive
Use 6
Research in high-income countries:
Measures various aspects of relationship quality
Mixed research results
Majority of findings suggest a positive association
Research in sub-Saharan Africa:
Recent focus on couple characteristics as potential
determinants of contraceptive use
Limited research on relationship quality

Study Objective 7
Better understand how
various components of
relationship quality
among married and
cohabitating couples in
Kumasi, Ghana are
associated with the use
of contraception.
Kumasi

Marriage and Contraceptive Use in
Ghana 8
Median age of marriage
Females: 20 years
Males: 26 years
Contraceptive Prevalence Rate
(Married Women):
24%-all methods
17%-modern methods
7%- traditional methods
Unmet Need for Contraception: 35%
Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF Macro. 2009. Ghana
Demographic and Health Survey 2008. Accra, Ghana: GSS, GHS, and ICF Macro.

Data Source
9
Family Health and Wealth Study-Ghana
Longitudinal, cohort study in peri-urban communities
Used baseline data from Kumasi, Ghana
800 married and cohabitating couples of reproductive
age
Measurement of Relationship Quality 10
Five dimensions of relationship quality measured in FHWS:
1. Commitment Subscale (Sternberg Triangular Love Scale)
2. Dyadic Trust Scale
3. Constructive Communication Subscale (Communication Patterns Questionnaire)
4. Destructive Communication Subscale (Communication Patterns Questionnaire)
5. Single item on relationship satisfaction
Scales adapted based on results of Confirmatory Factor Analysis

Examples of Scale Items 11
SCALE ITEM
Commitment Subscale
I am committed to maintaining my
relationship with my current partner
Dyadic Trust Scale
My partner treats me fairly and justly
Constructive Communication
Subscale
We try to discuss the problem
Destructive Communication
Subscale
We threaten each other with negative
consequences
Relationship Satisfaction
(Single Question)
Please rate how happy you are in your
relationship

Dependent Variable 12
Dependent Variable: Current Contraceptive Use
No Use
Non-Awareness Method Use
Injectable, pill, IUD, implants, and diaphragm
Awareness Method Use
Periodic abstinence, withdrawal, condoms, and spermicide
Respondents who were pregnant, used permanent
methods or “other” methods were excluded

Data Analysis 13
Bivariate and Multivariate Multinomial Logistic Regression Analysis
Controlled for the following variables:
Age, Religion, and Education of the female respondent
Household wealth
Number of children
Difference in partners’ age and education
Relationship type (monogamous or polygynous)
Relationship duration
Relationship status (married or cohabitating)
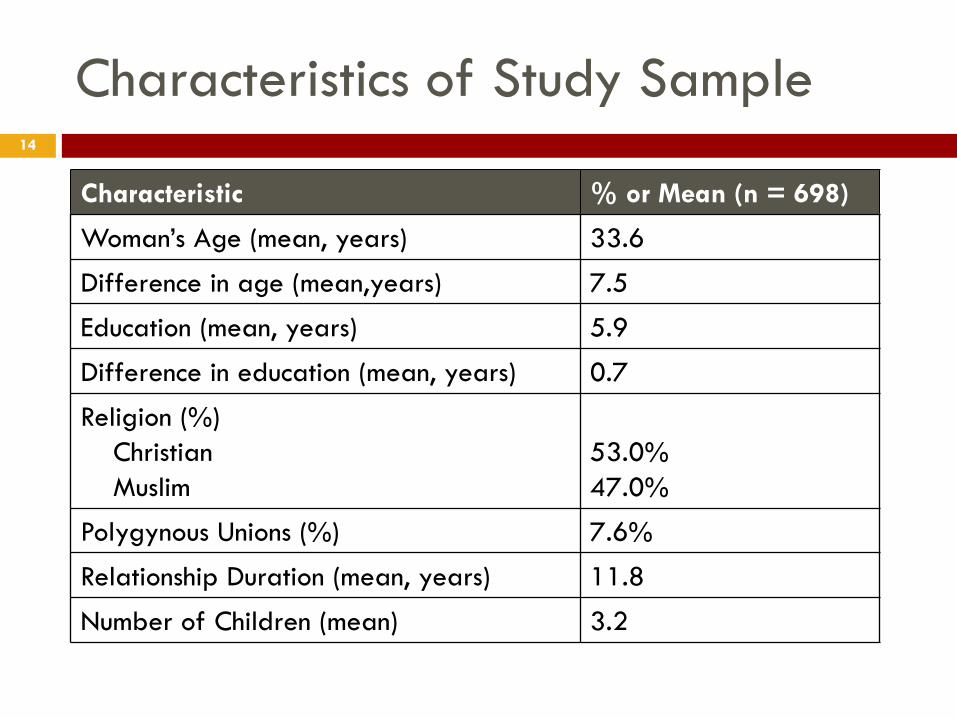
Characteristics of Study Sample 14
Characteristic % or Mean (n = 698)
Woman’s Age (mean, years) 33.6
Difference in age (mean,years) 7.5
Education (mean, years) 5.9
Difference in education (mean, years) 0.7
Religion (%)
Christian
Muslim
53.0%
47.0%
Polygynous Unions (%) 7.6%
Relationship Duration (mean, years) 11.8
Number of Children (mean) 3.2

Contraceptive use among women in
study sample 15
Contraceptive Method % of Women (n=698)
No Method Use
No Method
77.5
Non-Awareness Method Use
Pills
Injectables
IUD
Implants
Diaphragm
7.0
3.2
0.4
0.1
0.1
Awareness Method Use
Periodic Abstinence
Condoms
Withdrawal
Spermicide
8.3
2.3
0.7
0.3

Mean Relationship Quality Scores 16
Relationship Quality
(Possible Score Range)
Women’s Mean
Score
Men’s Mean
Score
Commitment
(4-36)
29.92
33.59
Trust
(5-35)
25.40 28.68
Satisfaction
(1-6)
4.51 4.84
Constructive Communication
(3-30)
21.80 25.51
Destructive Communication
(3-30)
4.85 4.54

Unadjusted Multinomial Logistic
Regression: Relationship Quality 17
Non-Awareness Method
Use vs. Non-Use
Awareness Method Use
vs. Non-Use
Women Partner Women Partner
Commitment 1.00 1.07 1.02 1.08***
Trust 0.99 1.05† 1.01 1.04
Satisfaction 0.96 1.35† 1.18** 1.31
Constructive
Communication
1.00 1.05 1.05*** 1.16***
Destructive
Communication
1.06 0.92 1.05 0.97
† p<0.10, *p<0.05, **p<0.01, ***p<0.001

Unadjusted Multinomial Logistic Regression:
Demographic Characteristics 18
Non-Awareness Method
Use vs. Non-Use
Awareness Method Use
vs. Non-Use
Age 0.94*** 0.95*
Education 1.07*** 1.09
Religion Christian
Muslim
Ref
0.46**
Ref
0.68
Wealth Lowest
Lower
Middle
Higher
Highest
Ref
1.16
0.86
0.59
0.75
Ref
1.24
1.22
1.29
1.80
† p<0.10, *p<0.05, **p<0.01

Unadjusted Multinomial Logistic
Regression: Couple Characteristics 19
Non-Awareness
Method Use vs.
Non-Use
Awareness
Method Use vs.
Non-Use
Relationship Type (Mono -Ref)
Polygynous
0.27***
0.12
Relationship Status (Married-Ref)
Cohabitating
1.17
0.90
Relationship Duration 0.98 0.96**
Difference in Age 0.96† 0.98
Difference in Education 0.96*** 1.02
Number of Children 1.01 0.93
† p<0.10, *p<0.05, **p<0.01, ***p<0.001
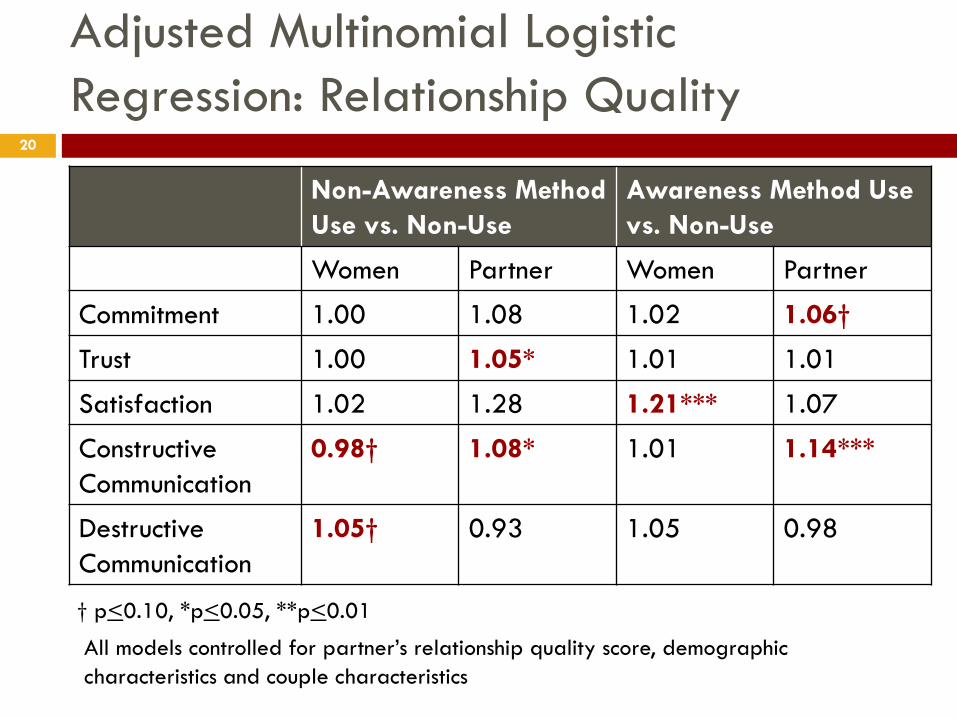
Adjusted Multinomial Logistic
Regression: Relationship Quality 20
Non-Awareness Method
Use vs. Non-Use
Awareness Method Use
vs. Non-Use
Women Partner Women Partner
Commitment 1.00 1.08 1.02 1.06†
Trust 1.00 1.05* 1.01 1.01
Satisfaction 1.02 1.28 1.21*** 1.07
Constructive
Communication
0.98† 1.08* 1.01 1.14***
Destructive
Communication
1.05† 0.93 1.05 0.98
† p<0.10, *p<0.05, **p<0.01
All models controlled for partner’s relationship quality score, demographic
characteristics and couple characteristics
Conclusion 21
Certain dimensions of relationship quality are important in contraceptive decision-making.
Male partner’s perception of relationship quality matters in contraceptive use.
Association between contraceptive use and relationship quality varies by dimension of relationship quality and type of contraception.
Relationship quality should be considered in reproductive health research and programs.

Limitations 22
Cross-sectional data
Challenges in measuring
relationship quality
Potential bias
Generalizability
Public Health Implications 23
Policy
Establish and enforce policies promoting harmonious relationships and access to quality family planning services
Ensure the individual right to contraception
Programmatic
Incorporate the promotion of positive relationship quality:
Mass media messages
Sexual education
Training curricula for family planning providers
Sexual and reproductive health programs

Next Steps in Research 24
Assess how relationship quality relates to other aspects of contraceptive decision-making:
Fertility desires, Unmet need, and Covert use
Further examine the validity of relationship quality measures in the West African context
Conduct qualitative research to better understand key findings and identify other dimensions of relationship quality important in contraceptive use

Acknowledgements
Co-authors: Michelle Hindin, Easmon Otupiri, and
Roderick Larsen-Reindorf
Gates Institute for Population and Reproductive
Health
Faculty and Staff at JHSPH
Research Team at KNUST
Study Participants
25

Questions?
26
Thank You!

Supplemental Slides
27
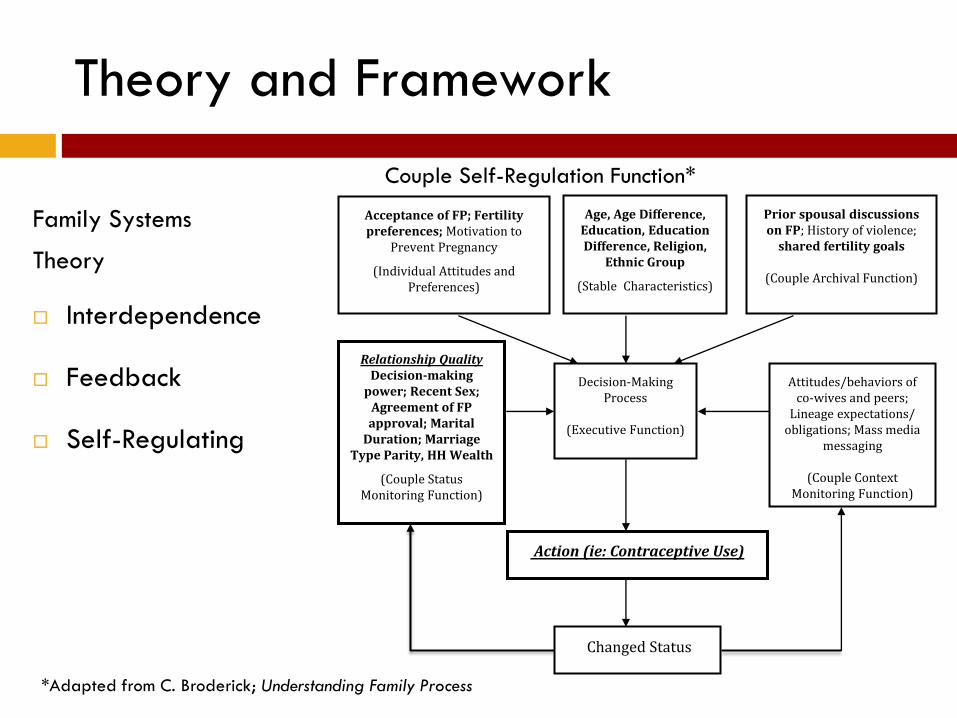
Theory and Framework
Family Systems
Theory
Interdependence
Feedback
Self-Regulating
Couple Self-Regulation Function*
*Adapted from C. Broderick; Understanding Family Process
Prior spousal discussions on FP; History of violence;
shared fertility goals
(Couple Archival Function)
Action (ie: Contraceptive Use)
Relationship Quality
Decision-making power; Recent Sex;
Agreement of FP approval; Marital
Duration; Marriage Type Parity, HH Wealth
(Couple Status Monitoring Function)
Decision-Making Process
(Executive Function)
Changed Status
Attitudes/behaviors of co-wives and peers;
Lineage expectations/ obligations; Mass media
messaging
(Couple Context Monitoring Function)
Age, Age Difference, Education, Education Difference, Religion,
Ethnic Group
(Stable Characteristics)
Acceptance of FP; Fertility preferences; Motivation to
Prevent Pregnancy
(Individual Attitudes and Preferences)

Assumptions of the Family Systems
Theory
An entire system must be considered as a whole rather than its individual parts.
The context in which things occur is essential to consider when interpreting interactions and outcomes of the system.
Systems are hierarchically organized and nested within each other.
All living systems are open, active systems that interact with their environment.
Human systems are self-reflexive implying that individuals are able to reflect on their behaviors and interactions within the system.
Reality is constructed by individuals through their own perspective.
*Jurich and Myers-Brown (1998)

Conceptual Framework
Fertility Preferences (Both Partners)
Individual-Level Variables: (Age, Education, Wealth, Urban/Rural, Religion, Parity, Ethnic Group)
Couple-Level Variables: (Difference in Age, Difference in Education, Marital Duration, Husband’s Absence, Marriage Type, Household Decision-Making Power)
Contraceptive Use
Community-Level Variables: (Gender Inequality, Cultural Norms, Health Facilities)
Family Planning Decision-Making Power
)
Knowledge of Family Planning
Spousal Discussion
on Family Planning
Relationship Quality
Coital Frequency
Acceptance of Contraception
Contraception-Related Health
Concerns
Access to Contraception
Motivation to Prevent
Pregnancy

Commitment Subscale 31
Retained in Final
Scale
Commitment Subscale Female Male
I expect my love for my current partner to last for the
rest of my life. Yes Yes
I can't imagine ending my relationship with my current
partner. Yes No
I view my relationship with my current partner as
permanent. Yes Yes
I am committed to maintaining my relationship with
my current partner. Yes Yes
I have confidence in the stability of my relationship
with my current partner. Yes Yes

Dyadic Trust Scale 32
Retained in Final Scale
Dyadic Trust Scale Female Male
My partner is primarily interested in his own welfare No No
There are times when my partner cannot be trusted No No
My partner is perfectly honest and truthful with me Yes Yes
I feel I can trust my partner completely Yes Yes
My partner is truly sincere in his promises Yes Yes
I feel that my partner does not show me enough
consideration No No
My partner treats me fairly and justly Yes Yes
I feel that my partner can be counted on to help me Yes Yes

Constructive Communication Subscale 33
Retained in Final Scale
Constructive Communication Factor Female Male
We try to discuss the problem Yes Yes
We express their feelings to each other Yes No
We suggest possible solutions and compromises Yes Yes
Destructive Communication Factor
We blame, accuse and criticize each other Yes No
We threaten each other with negative consequences Yes Yes
I call my partner names, swear at him, or attack his character Yes Yes
My partner calls me names, swears at me, or attacks my
character Yes Yes

Confirmatory factor analysis: Women 34
SRMR, standardized root mean square residual; RMSEA, the root-mean-square-error-of-
approximation; TLI, tucker-lewis fit index, CFI, comparative fit index

Confirmatory Factor Analysis: Men 35
SRMR, standardized root mean square residual; RMSEA, the root-mean-square-error-of-
approximation; TLI, tucker-lewis fit index, CFI, comparative fit index

Qualitative Results 36
Dimensions of relationship quality important in
contraceptive decision-making:
Communication
Necessary step
Facilitation of discussion
Communication style important for acceptance
Empathy
Emphatic concern for the well-being of one’s partner and the
family important