course: key competences background: curriculum elements … · pip peep drug chart emergency drug...
TRANSCRIPT

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Course: Key Competences Background: In 2007, the Royal College of Paediatrics and Child Health (RCPCH) published a new curriculum for postgraduate medical education, which has been approved by the Postgraduate Medical Education and Training Board 1. In addition, the RCPCH has devised an assessment strategy that uses multisource feedback tools to map specifically to assessment standards. By the completion of Level One training, all trainees are expected to be able to initiate therapy in a child presenting with Sepsis. This scenario/ workshop has been designed to assess competence in management of this key condition of childhood. Curriculum Elements Addressed: The commonest causes of septicaemia in children is meningococcal or pneumococcal, but other causes include Group B streptococcal in young infants, gram negative sepsis in relation to urinary tract or gut problems and group A streptococcal sepsis. Children may present with shock and non blanching rash (if meningococcal). The management of Sepsis can be separated into five distinct phases:
• Assessment • Recognition of the condition • Formulation of differential diagnoses • Investigation • Definitive therapy
Assessment (Expected) Brief history should be obtained (key features – fever, anorexia, sleepy, abdominal pain and vomiting (symptoms often nonspecific). The child should be examined thoroughly. Key features of examination:
• Tachycardia 140 beats.min-1; NIBP 80/50; • CRT 4-5 sec • Tachypnoea 35 breaths.min-1 • Temperature 39oC • Moaning.
Recognition of condition (Expected) Signs are of shock with metabolic acidosis.
1 A Framework of Competences for Level 1 Training in Paediatrics.
http://www.rcpch.ac.uk/Training/Competency-Frameworks
Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Formulation of differential diagnosis (Expected) Diagnostic possibilities include:
• Hypovolaemia, (acute abdomen, haemorrhage) • Acute cardiac (failure, cardiomyopathy, arrhythmia) • Distributive (anaphylaxis) • Obstructive (tension pneumothorax, cardiac tamponade) • Dissociative (carbon monoxide poisoning).
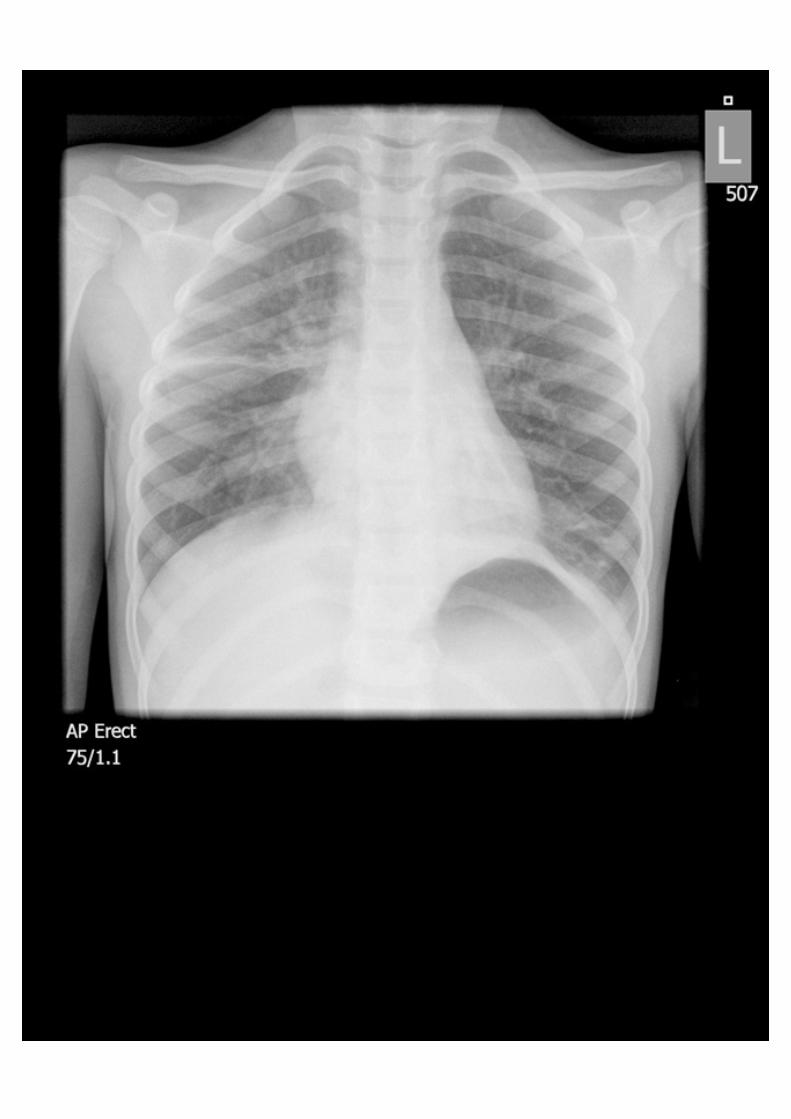
Investigations (Expected) Cardiovascular monitoring Pulse oximetry Blood gas, lactate, Glucose Septic screen (partial) [LP should not be performed in this under-resuscitated child] Laboratory investigations (to include U&Es, FBC, CRP, clotting, blood and urine cultures, cross match) Chest X-ray Blood gas reveals metabolic acidosis, lactic acidosis
Definitive Therapy (Expected) 1. Apply oxygen 2. Gain intravenous / intraosseous access 3. Reverse shock (40ml/kg [20ml/kg twice] of 0.9% saline) 4. Antibiotic (Cefotaxime/ Ceftriaxone) 5. Start peripheral inotrope (Dopamine) 6. Call for help (PICU/ anaesthesia) to get child intubated and transferred to PICU 7. Further volume resuscitation 20ml/kg 8. Consider adrenaline infusion 9. Appropriate monitoring, CVS, assess level of consciousness, glucose, potassium 10. Appropriately manage decreased level of consciousness 11. CT scan should not be undertaken unless patient is stabilised 12. Lumbar puncture is contraindicated due to shocked patient with decreased level
of consciousness and prolonged clotting.
Assessment Domains:
Level of Achievement RCPCH Standards Good Adequate Poor
Effective skills in paediatric assessment
Knowledge of common and serious paediatric conditions and their management
Effective initial management of ill-health and clinical conditions in paediatrics, seeking additional advice and opinion as appropriate
Safe practical skills in paediatrics
Advanced Neonatal and Paediatric Life Support Skills
Effective communication and interpersonal skills with colleagues

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Scenario: Septic Shock
Learning Objectives: At the end of the session candidates should be able to: 1. Recognise symptoms and signs of septic shock 2. Gain appropriate access (Intraosseous access if very shocked) 3. Appropriate fluid resuscitation 4. Early antibiotics 5. Profound shock may not respond to volume and need early inotropic
support and ICU assessment 6. Intubate early to allow definitive management to progress 7. Sepsis may present with mixed septicaemic & meningitic picture
Faculty Script: A six year old boy is brought to hospital A&E department by parents. He has had a cold for 3 days and was found in bed this morning very hot and confused. This boy has fluid resistant shock and though he will respond transiently to fluid boluses when administered, he will only stabilise once he has been commenced on peripheral inotropes and appropriate referral to PICU for definitive treatment has been made.
Patient Demographics: Name: Richard Peaky Gender: M Age: 6years Weight: 20 kg
Candidate Brief:
Presenting History (Candidate Storyboard): A six year old boy is brought to hospital A&E department by parents. He has had a cold for 3 days and was found in bed this morning very hot and confused.
Previous Medical History: Nil of note. Normally fit and healthy.
Family Medical History: Nil of note
Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
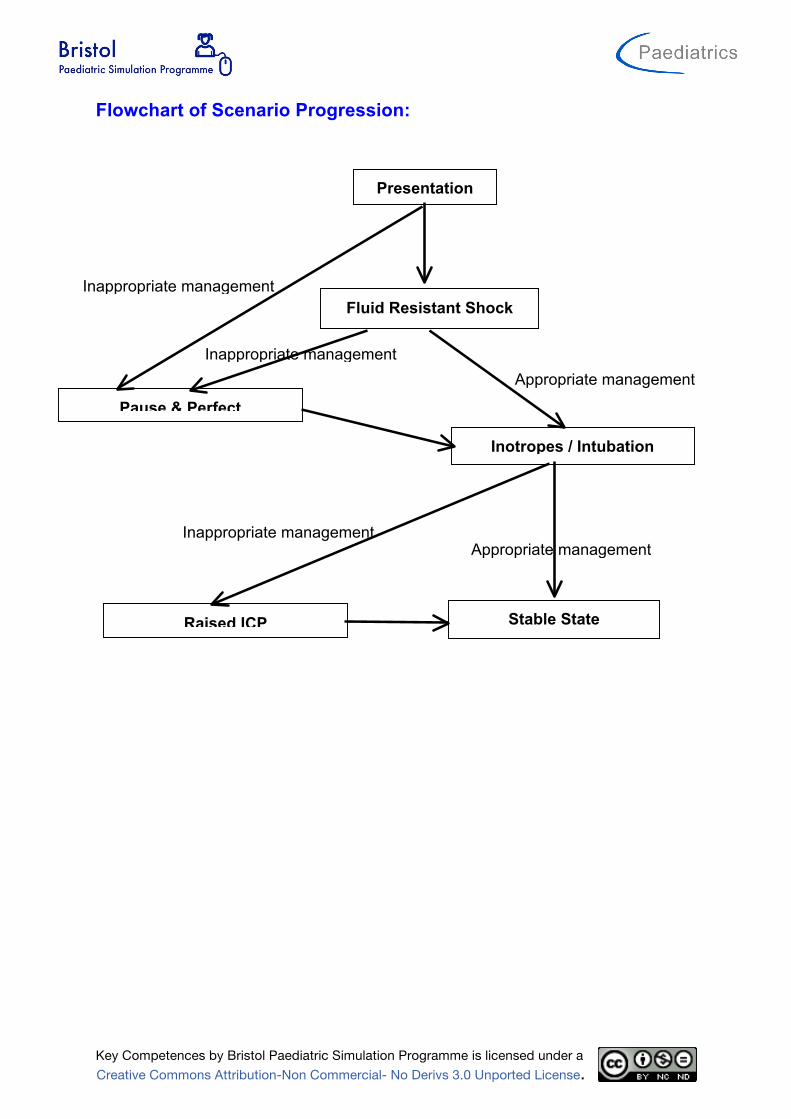
Flowchart of Scenario Progression:
Appropriate management
Inappropriate management
Presentation
Inotropes / Intubation
Fluid Resistant Shock
Stable State
Appropriate management
Raised ICP
Pause & Perfect
Inappropriate management
Inappropriate management

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Scenario setup and preparation:
Faculty Recommended: Director Control
Actor/Confederate(s) Roles: Parent Nursing Staff Anaesthetic/ICU Registrar
If you have a multiprofessional group of candidate then you should have a multiprofessional faculty.
Participants:
Medical Roles Nursing Roles AHP Roles Paediatric SHO
Location: Emergency Department
Simulator: Meti Paed ECS, Paediasim or SimJunior Monitor Setup: 3 wave format
Monitor Parameters Required:
ECG SaO2 RR EtCO2 NIBP ABP CVP PAP ICP CPP Temp (P) Temp (C) Other:
Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
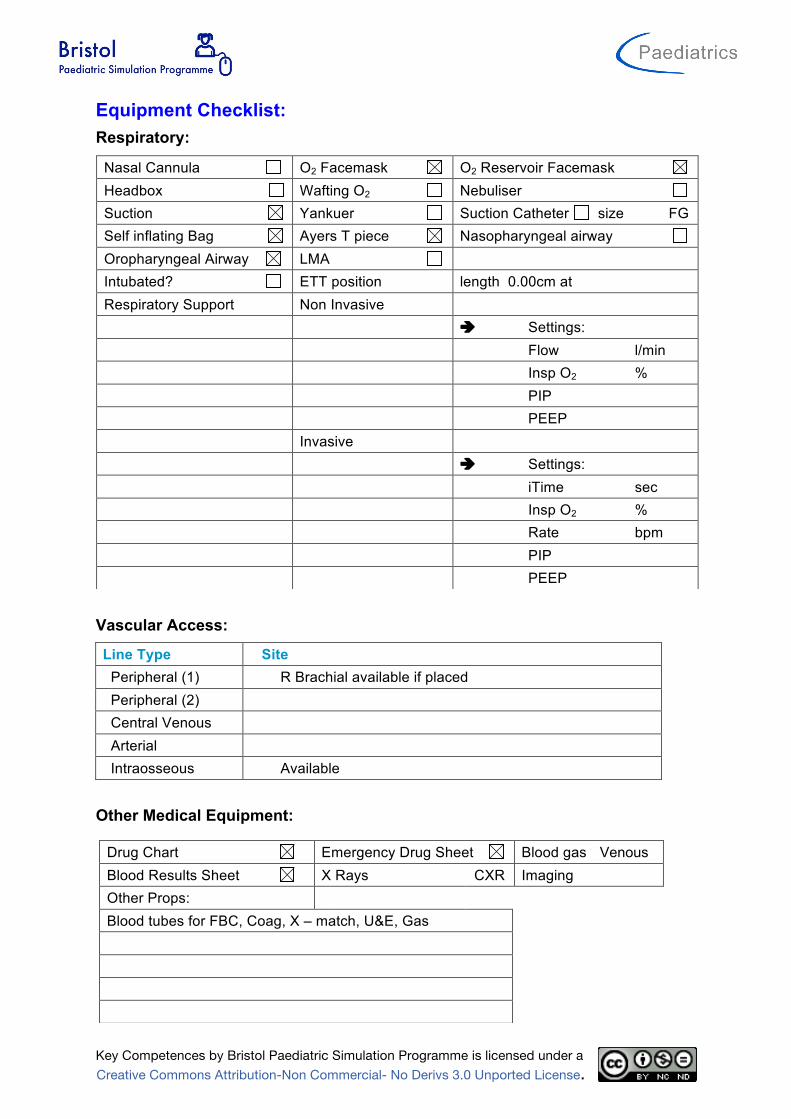
Equipment Checklist: Respiratory:
Vascular Access:
Line Type Site Peripheral (1) R Brachial available if placed Peripheral (2) Central Venous Arterial Intraosseous Available
Other Medical Equipment:
Nasal Cannula O2 Facemask O2 Reservoir Facemask Headbox Wafting O2 Nebuliser Suction Yankuer Suction Catheter size
FG Self inflating Bag Ayers T piece Nasopharyngeal airway Oropharyngeal Airway LMA Intubated? ETT position length 0.00cm at Respiratory Support Non Invasive è Settings: Flow
l/min Insp O2
% PIP
PEEP
Invasive è Settings: iTime
sec Insp O2
% Rate
bpm PIP
PEEP
Drug Chart Emergency Drug Sheet Blood gas Venous Blood Results Sheet X Rays CXR Imaging Other Props: Blood tubes for FBC, Coag, X – match, U&E, Gas

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
IV Fluids:
Setup Fluid Type Fluids Running Fluids Available (1) 0.9% Saline Fluids Available (2) Colloid: 4.5% HAS or Gelofucin or Starch Fluids Available (3) FFP Other Fluids Blood
Medications: (route, dose/rate)
Infusions (Running) Dose Running Rate (ml/hr) Nil
Infusions (Available) Dose Running Rate (ml/hr) Dopamine 5mcg/kg/ml 1 - 2 Adrenaline 0.05mcg/kg/ml 1 - 4 Nor-Adrenaline 0.05mcg/kg/ml 1 - 4
Bolus Drugs (Available) Dose Adrenaline 1:10 000 2ml Cefotaxime/Ceftriaxone Mannitol 0.5G/kg Ketamine 40mg Pancuronium 2mg

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Moulage: Effect needed
Draw relevant equipment needed on diagram e.g. cannula, wounds etc.
Page 1 of 2
DEPARTMENT/PROGRAM:
TOPIC:
SCENARIO TITLE:
LEARNING OBJECTIVES:
At the end of the session, trainees should be able
to:
1.
2.
3.
4.
5.
PATIENT DEMOGRAPHICS
Patient Name:
Age:
Gender:
Weight:
Allergies:
Dx:
Sx:
SET-UP
Simulator:
SimMan PediaSim
SimBaby
Task Trainer:
Access:
PIV size:
Location:
PIV size:
Location:
CVL#:
Location:
ART
PICC
Other:
Other Medical Equipment:
Monitor Parameters:
EKG RR CVP
SpO2 ABP PAP
NBP ICP Temp
Other:
IV Fluids:
NS LR
D5 ! NS D5 " NS
D5W D10W
Other:
Props:
Respiratory Equipment
Nasal Cannula
Face tent
Simple Face Mask
Non-rebreather
Self-inflating bag
Anesthesia Bag
SVN
MDI / Spacer
Suction
Intubated Ventilator
Vent Settings: Pressure Control PIP: PEEP:
IMV: TV:
FiO2:
Medications: (route; dose/rate)
1.
2.
3.
4.
5.
6.
Multi-Media (xrays, CT):
Please LABEL the body to indicate location of
dressings, access, chest tubes, etc.
22G Cannula if placed
Intraosseous available

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Scenario States:
Name of State Sepsis Presentation Duration Vital Signs Rhythm SR HR 140 SBP 80 DBP 40 CVP
Resp Rate 35 SaO2 90 ETCO2 Temp 39.5 Other
AVPU P GCS 12 Pupils 4 ERL ICP NIRS
Asessment
Periph Pulses weak Cap refil 5 sec Skin warm peripheries
ECG/Heart normal heart sounds Airway unobstructed Breathing shallow Air entry reduced bilateral Breath sounds Normal WOB grunting Recession Neuro Moaning Renal Hepatic Other
Results Hb 9.8 WCC 2 PLT 36 HCT 0.3 CRP 189 PH/ H+ 7.19 PaCO2 61/ 8.1 PaO2 44 / 5.8 HCO3 16.6 BE - 9.9 Lactate 6.7 Na2+ 135 K+ 4.6 Cl- 111 Ur 8.9 Cr 68 Glucose 14.6 Ca2+ 2.6 Mg2+ 0.5 PO4
- 1.0
Expected Outcomes: Participants should: Brief history should be obtained (key features – fever, anorexia, sleepy.
The child should be examined thoroughly. Establish monitoring • Cardiovascular monitoring • Pulse oximetry
Investigations • Blood gas, lactate, Glucose • Laboratory investigations (to include U&Es, FBC, CRP, clotting, blood
and urine cultures, cross match) • Septic screen (partial) [LP should not be performed in this under-
resuscitated child] • Chest X-ray
Early management • Facemask O2, • IV/IO access • Fluid resuscitation • Antibiotics
Facilitators should: Initial improvement in parameters with fluid resuss, but deteriorates requiring further fluid.

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Name of State Fluid Resistent shock Duration Vital Signs Rhythm SR HR 140 SBP 80 DBP 35 CVP Resp Rate 35 SaO2 93 ETCO2 Temp 39.5 Other AVPU U GCS 8 Pupils 4 ERL ICP NIRS
Asessment Periph Pulses weak Cap refil 5 Skin warm peripheries ECG/Heart Normal heart sounds Airway clear Breathing shallow Air entry reduced bilateral Breath sounds normal WOB normal Recession none Neuro Unresponsive Renal Hepatic Other
Results Hb WCC PLT HCT CRP PH/ H+ 7.16 PaCO2 54 /7.2 PaO2 55 / 7.3 HCO3 12.6 BE - 14 Lactate 7.1 Na2+ 137 K+ 4.4 Cl- 97 Ur Cr Glucose 16.1 Ca2+ Mg2+ PO4
-
Expected Outcomes:
Participants should: Re assess patient and identify that patient still shocked despite 40 ml/kg, Commence Inotropes – Dopamine /Adrenaline Call for anaesthetic/ICU help to intubate, place central and arterial lines
Facilitators should: If managed well progress to Post Inotrope/Intubation State If management not optimal, pause scenario and discuss lack of response and potential strategies to implement. Restart scenario allowing candidates to implement strategies
Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
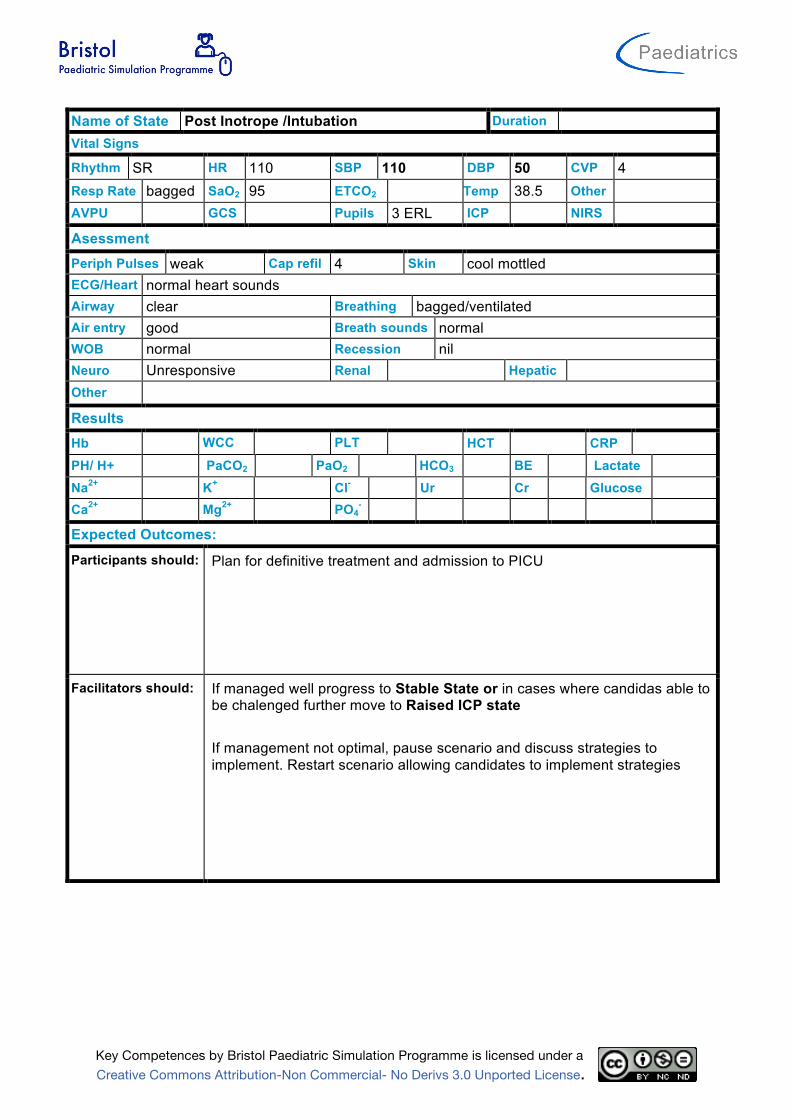
Name of State Post Inotrope /Intubation Duration Vital Signs Rhythm SR HR 110 SBP 110 DBP 50 CVP 4 Resp Rate bagged SaO2 95 ETCO2 Temp 38.5 Other AVPU GCS Pupils 3 ERL ICP NIRS
Asessment Periph Pulses weak Cap refil 4 Skin cool mottled ECG/Heart normal heart sounds Airway clear Breathing bagged/ventilated Air entry good Breath sounds normal WOB normal Recession nil Neuro Unresponsive Renal Hepatic Other
Results Hb WCC PLT HCT CRP PH/ H+ PaCO2 PaO2 HCO3 BE Lactate Na2+ K+ Cl- Ur Cr Glucose Ca2+ Mg2+ PO4
-
Expected Outcomes:
Participants should: Plan for definitive treatment and admission to PICU
Facilitators should: If managed well progress to Stable State or in cases where candidas able to be chalenged further move to Raised ICP state If management not optimal, pause scenario and discuss strategies to implement. Restart scenario allowing candidates to implement strategies

Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
Name of State Raised ICP Duration Vital Signs Rhythm SR HR 65 SBP 165 DBP 80 CVP 8 Resp Rate 15 SaO2 92 ETCO2 Temp 38.5 Other AVPU U GCS 6 Pupils 3 ERL ICP NIRS
Asessment Periph Pulses strong Cap refil 4 Skin cool mottled ECG/Heart normal heart sounds Airway clear Breathing bagged/ventilated Air entry good Breath sounds normal WOB normal Recession nil Neuro Unresponsive Renal Hepatic Other
Results Hb WCC PLT HCT CRP PH/ H+ PaCO2 PaO2 HCO3 BE Lactate Na2+ K+ Cl- Ur Cr Glucose Ca2+ Mg2+ PO4
-
Expected Outcomes:
Participants should: Recognise deteriorated neurological state Call for Help Initiate management cerebral oedema prior to CT scan Hand bag, check pupils, opiates, mannitol, anticonvulsants
Facilitators should: If managed well progress to Stable State If management not optimal, pause scenario and discuss lack of response and potential strategies to implement. Restart scenario allowing candidates to implement strategies
Key Competences by Bristol Paediatric Simulation Programme is licensed under a Creative Commons Attribution-Non Commercial- No Derivs 3.0 Unported License.
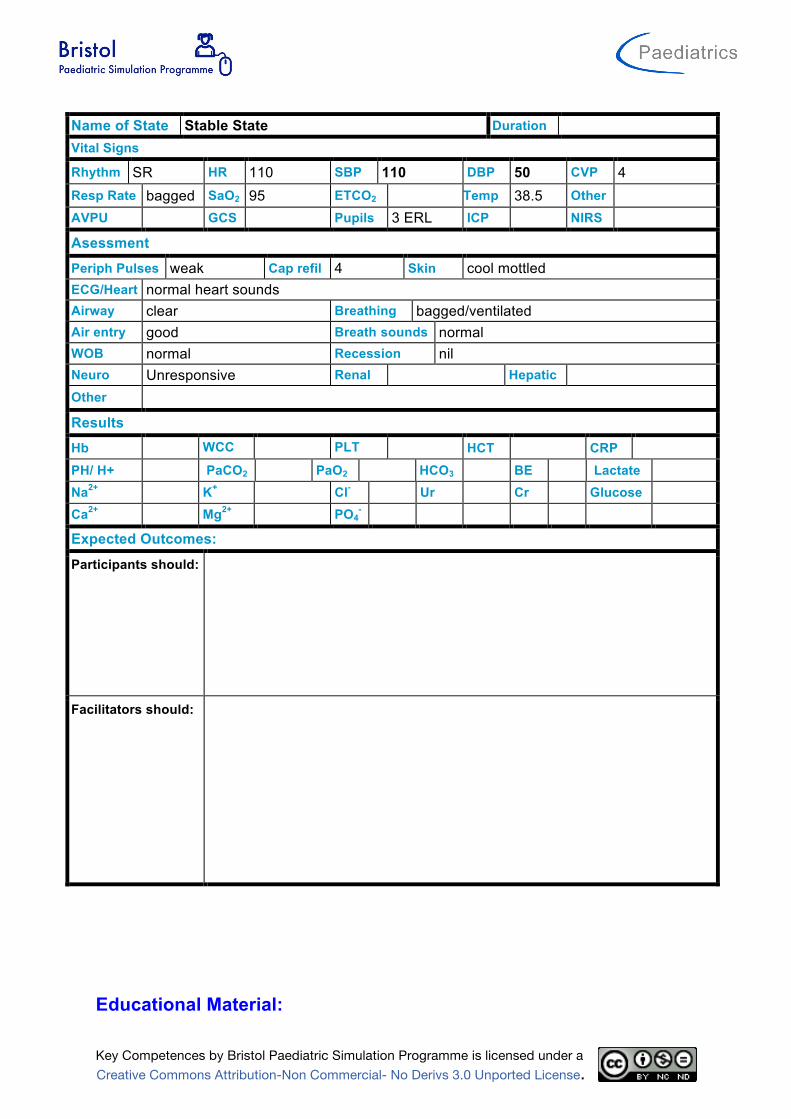
Name of State Stable State Duration Vital Signs Rhythm SR HR 110 SBP 110 DBP 50 CVP 4 Resp Rate bagged SaO2 95 ETCO2 Temp 38.5 Other AVPU GCS Pupils 3 ERL ICP NIRS
Asessment Periph Pulses weak Cap refil 4 Skin cool mottled ECG/Heart normal heart sounds Airway clear Breathing bagged/ventilated Air entry good Breath sounds normal WOB normal Recession nil Neuro Unresponsive Renal Hepatic Other
Results Hb WCC PLT HCT CRP PH/ H+ PaCO2 PaO2 HCO3 BE Lactate Na2+ K+ Cl- Ur Cr Glucose Ca2+ Mg2+ PO4
-
Expected Outcomes:
Participants should:
Facilitators should:
Educational Material:
Division of Women’s and Children’s Services Local Practice Guidelines
Author; G.Haythornthwaite
Yes
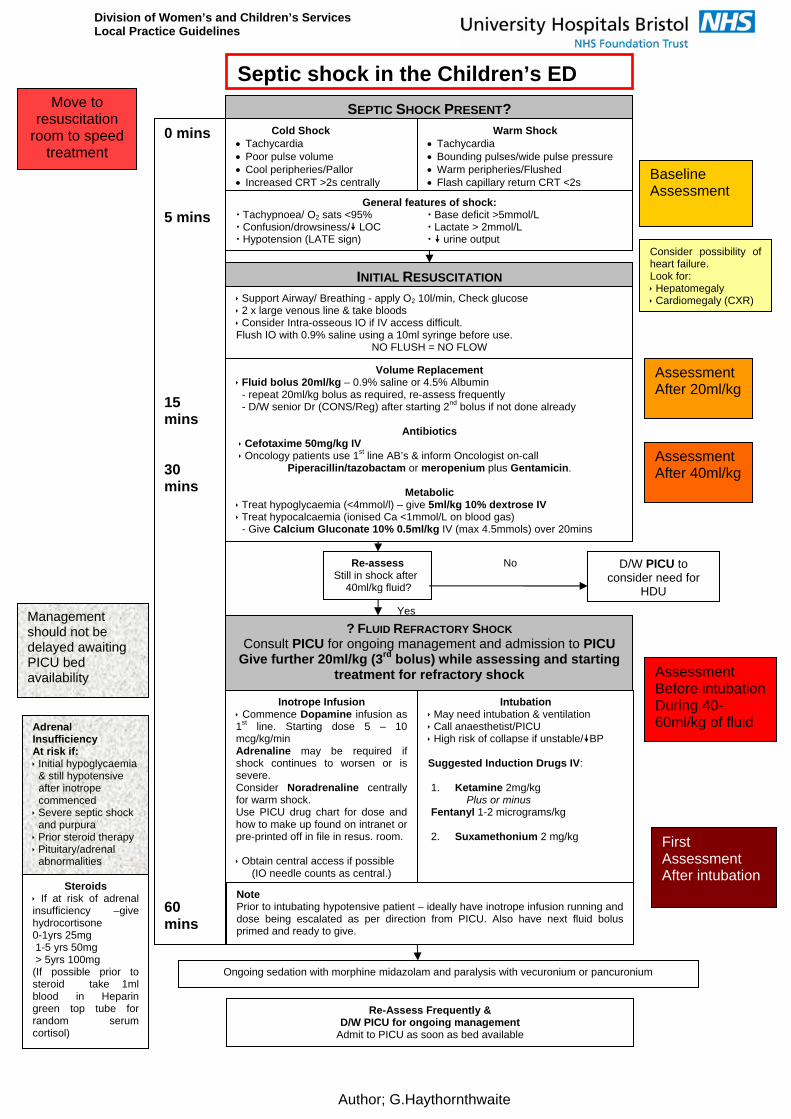
SEPTIC SHOCK PRESENT? Cold Shock Tachycardia Poor pulse volume Cool peripheries/Pallor Increased CRT >2s centrally
INITIAL RESUSCITATION
Support Airway/ Breathing - apply O2 10l/min, Check glucose 2 x large venous line & take bloods Consider Intra-osseous IO if IV access difficult. Flush IO with 0.9% saline using a 10ml syringe before use.
NO FLUSH = NO FLOW
Volume Replacement Fluid bolus 20ml/kg – 0.9% saline or 4.5% Albumin - repeat 20ml/kg bolus as required, re-assess frequently - D/W senior Dr (CONS/Reg) after starting 2nd bolus if not done already
Antibiotics
Cefotaxime 50mg/kg IV Oncology patients use 1st line AB’s & inform Oncologist on-call
Piperacillin/tazobactam or meropenium plus Gentamicin.
Metabolic Treat hypoglycaemia (<4mmol/l) – give 5ml/kg 10% dextrose IV Treat hypocalcaemia (ionised Ca <1mmol/L on blood gas) - Give Calcium Gluconate 10% 0.5ml/kg IV (max 4.5mmols) over 20mins
Warm Shock Tachycardia Bounding pulses/wide pulse pressure Warm peripheries/Flushed Flash capillary return CRT <2s
General features of shock: Tachypnoea/ O2 sats <95% Base deficit >5mmol/L Confusion/drowsiness/ LOC Lactate > 2mmol/L Hypotension (LATE sign) urine output
Re-assess Still in shock after 40ml/kg fluid?
Intubation May need intubation & ventilation Call anaesthetist/PICU High risk of collapse if unstable/BP Suggested Induction Drugs IV: 1. Ketamine 2mg/kg Plus or minus Fentanyl 1-2 micrograms/kg 2. Suxamethonium 2 mg/kg
? FLUID REFRACTORY SHOCK Consult PICU for ongoing management and admission to PICU
Give further 20ml/kg (3rd bolus) while assessing and starting treatment for refractory shock
Inotrope Infusion Commence Dopamine infusion as 1st line. Starting dose 5 – 10 mcg/kg/min Adrenaline may be required if shock continues to worsen or is severe. Consider Noradrenaline centrally for warm shock. Use PICU drug chart for dose and how to make up found on intranet or pre-printed off in file in resus. room. Obtain central access if possible
(IO needle counts as central.)
D/W PICU to consider need for
HDU
No
Note Prior to intubating hypotensive patient – ideally have inotrope infusion running and dose being escalated as per direction from PICU. Also have next fluid bolus primed and ready to give.
Consider possibility of heart failure. Look for: Hepatomegaly Cardiomegaly (CXR)
Baseline Assessment
Assessment After 20ml/kg
Assessment After 40ml/kg
Assessment Before intubation During 40-60ml/kg of fluid
Ongoing sedation with morphine midazolam and paralysis with vecuronium or pancuronium
0 mins 5 mins 15 mins 30 mins 60 mins
Adrenal Insufficiency At risk if: Initial hypoglycaemia & still hypotensive after inotrope commenced Severe septic shock and purpura Prior steroid therapy Pituitary/adrenal abnormalities
Management should not be delayed awaiting PICU bed availability
Steroids If at risk of adrenal insufficiency –give hydrocortisone 0-1yrs 25mg 1-5 yrs 50mg > 5yrs 100mg (If possible prior to steroid take 1ml blood in Heparin green top tube for random serum cortisol)
Move to resuscitation
room to speed treatment
First Assessment After intubation
Septic shock in the Children’s ED
Re-Assess Frequently & D/W PICU for ongoing management
Admit to PICU as soon as bed available
Division of Women’s and Children’s Services Local Practice Guidelines
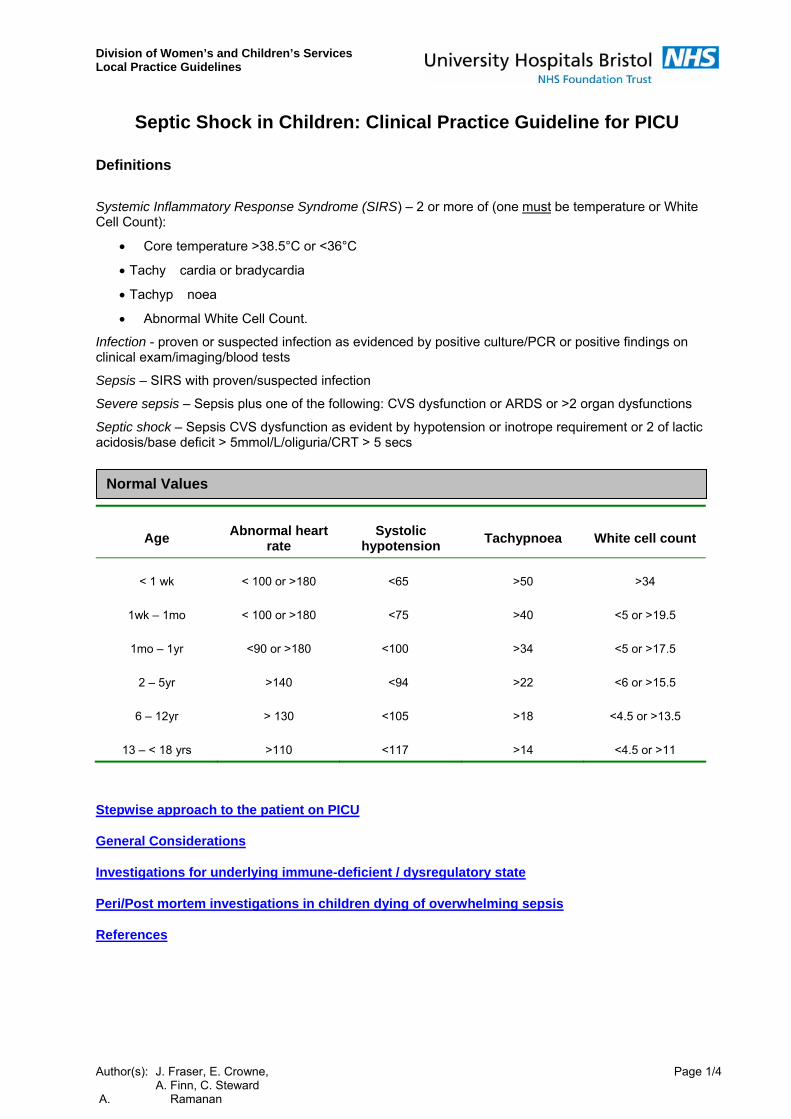
Septic Shock in Children: Clinical Practice Guideline for PICU
Definitions
Systemic Inflammatory Response Syndrome (SIRS) – 2 or more of (one must be temperature or White Cell Count):
• Core temperature >38.5°C or <36°C
• Tachy cardia or bradycardia
• Tachyp noea
• Abnormal White Cell Count.
Infection - proven or suspected infection as evidenced by positive culture/PCR or positive findings on clinical exam/imaging/blood tests
Sepsis – SIRS with proven/suspected infection
Severe sepsis – Sepsis plus one of the following: CVS dysfunction or ARDS or >2 organ dysfunctions
Septic shock – Sepsis CVS dysfunction as evident by hypotension or inotrope requirement or 2 of lactic acidosis/base deficit > 5mmol/L/oliguria/CRT > 5 secs Normal Values
Age Abnormal heart
rate Systolic
hypotension Tachypnoea White cell count
< 1 wk < 100 or >180 <65 >50 >34
1wk – 1mo < 100 or >180 <75 >40 <5 or >19.5
1mo – 1yr <90 or >180 <100 >34 <5 or >17.5
2 – 5yr >140 <94 >22 <6 or >15.5
6 – 12yr > 130 <105 >18 <4.5 or >13.5
13 – < 18 yrs >110 <117 >14 <4.5 or >11
Stepwise approach to the patient on PICU
General Considerations
Investigations for underlying immune-deficient / dysregulatory state
Peri/Post mortem investigations in children dying of overwhelming sepsis
References
Author(s): J. Fraser, E. Crowne, Page 1/4 A. Finn, C. Steward A. Ramanan

Division of Women’s and Children’s Services Local Practice Guidelines
Stepwise approach to the patient on PICU Index
Consider risk of adrenal insufficiency?• severe shock with Purpura • current or recent steroid treatment • known/possible adrenal/pituitary abnormalities
Yes No
InotropesEstablish central venous access and
arterial line Begin dopamine 5-10micrograms/kg/min
Regularly Reassess and treat:• ABC, Fluid Volume Status (may need >100ml/kg), Electrolyte Disturbances (esp iCa2+ and K+) • Aim for adequate BP and high-normal CVP • Request Echocardiogram to assess cardiac contractility
Fluid and Inotrope Refractory Shock (requiring >10mcg/kg/min Dopamine)
What type of shock?
Cold Shock (SvO2 < 70%)
o Reduced function with BP OK o Milrinone/Sodium Nitroprusside
with volume
Cold Shock (SvO2 < 70%)o Reduced function & BP o Adren aline with volume
Warm shock (SvO2 > 70%) o Vasodilated but function OK o Noradrenaline with volume
Draw baseline Cortisol level, then give stat IV Hydrocortisone:
• 0-1 yrs 25mg • 1-5 yrs 50mg • > 5yrs 100mg
Continue on Hydrocortisone 1-2 mg/kg/tds
Fluid refractory shock (60mls/kg administered in first 15 mins)
Calculator for Preparing Inotrope Infusions
Author(s): J. Fraser, E. Crowne, Page 2/4 A. Finn, C. Steward A. Ramanan

Division of Women’s and Children’s Services Local Practice Guidelines
General Considerations Indexo Goal-directed approach. This has been shown to reduce mortality in adult sepsis. Central venous Pressure
(CVP) should be kept 8-12 mmHg although this will be lower when measured through a femoral catheter. If < 8 mmHg give further colloid boluses, especially if evidence of impaired RV function in a child who is ventilated. Mixed venous saturations (SvO2) should ideally be measured in the right atrium. Normal is > 70%.
o Ventilation. It should be assumed that all patients with sepsis have an Acute Lung Injury and therefore be ventilated with a standard protective ventilatory strategy from the outset.
o Inotrope strategy. Although the above flow diagram describes a 3 model picture, it must be realised that haemodynamic states in children with sepsis may change over time. Constant vigilance and assessment with echo/transoesophageal Doppler is useful. A Cardiac Index (CI) of > 3.3 l/min should be aimed for.
o Steroids. Routine use of steroids should await the result of further randomised controlled trials. STEPS (steroids in sepsis) study due to start early 2008. Adrenal insufficiency in the case of cathecholamine resistant shock is assumed at a random total cortisol concentration < 18 mg/dl (500nmol/L). If AI suspected continue steroids for 5 days, and then wean over 2 days before consideration to stopping. If high level of suspicion re Adrenal Insufficiency, suggest contact endocrinology team relating to need for convalescent synacthen test.
o Granulocyte-Colony Stimulating Factor (G-CSF). Consider in children with neutropenic sepsis secondary to chemotherapy and/or primary WBC immunodeficiency.
o Intravenous Immunoglobulin (IVIG). Consider in patients with Toxic Shock Syndrome and in neonatal septic shock. Dose 1 g/kg/day for 3 days.
o Activated Protein C. No evidence.
o Antibiotic policy. See separate antibiotic guidelines. Remember use of Linezolid/Vancomycin in suspected PVL staphylococcal sepsis. NOTE: one may see
PVL +ve MRSA AND MSSA strains Clindamycin in Toxic Shock Syndrome Vancomycin or Teicoplanin if suspected MRSA sepsis
o Feed. As early as possible…using the enteral route by whatever means that are possible (i.e. early NJ tube placement if necessary)
o Renal replacement Therapy (RRT). CVVH useful in children with anuria/severe oliguria and fluid overload. If started consider using high-volume turnover. Consider peritoneal dialysis if concerns about Abdominal Compartment Syndrome.
o Sedation/Muscle relaxants. Aim for sedation alone, or intermittent pancuronium in context of LCOS and if permits patient-ventilator synchrony
Investigations for underlying immune-deficient / dysregulatory state Index 1. Stored serum for DNA studies as part of Community Acquired Infection study. This study applies to any child
admitted to PIC with a severe community-acquired infection. The PIC team are not expected to take the blood tests. Contact Natalie or Sheila in MCRN office ext 0211 and 0216; work mobile 07768817944 and 07768824276 respectively)
2. Children with recurrent or severe bacterial or fungal illness, bronchiectasis or chronic ENT problems may
have an underlying immune deficiency. However, there is no role for routine tests in children with sepsis syndrome, unless such features are present. Lymphocyte subsets, immunoglobulins, and neutrophil function tests might be considered in the convalescent phase but this should be discussed at the Thursday microbiology round.
3. Similarly, some patients with a Haemophagocytic disorder may present with multi-organ dysfunction
syndrome that may mimic severe sepsis. Consider in children who have a history of: • Multiple infections requiring antibiotics • Problems with warts/herpes virus • Prolonged ‘recovery’ following trivial infection • Atypical neonatal problems
Additionally, consider in children in whom routine investigations demonstrate: • Abnormalities of MCV (raised indicating bone marrow failure, reduced indicating gut pathology & iron
malabsorption) • Pancytopenia, and/or DIC out of proportion with the degree of Multi Organ Dysfunction Syndrome
Author(s): J. Fraser, E. Crowne, Page 3/4 A. Finn, C. Steward A. Ramanan

Division of Women’s and Children’s Services Local Practice Guidelines
Tests to be undertaken: • Serum ferritin • Fasting triglycerides • Lactate Dehydrogenase (LDH) • Ebstein Barr Virus (EBV) & Cytomegalovirus (CMV) PCR (esp when hepatosplenomegaly present ) (1 ml serum sample in a yellow-topped bottle sent to biochemistry is required for ferritin, TG and LDH tests; a separate 1 ml yellow-topped bottle to virology is required for PCR studies)
Peri/Post mortem investigations in children dying of overwhelming sepsis Index
1. Peripheral blood for lymphocyte subsets and neutrophil function tests (looking for evidence of chronic granulomatous disease)
(1 ml EDTA sample in a red-topped bottle is required for LSs; a 1 ml heparin sample in an orange-topped bottle is required for NFTs. Please discuss with immunology lab, Southmead, before sending; on-call via NBT switchboard out of hours)
2. Request pathologist to look for:
• Anatomical clues of immunodeficiency e.g. small/absent spleen, presence of large numbers of lymph
glands, total absence of lymphoid tissue
• Evidence of haemophagocytosis in the spleen, liver, lymph node and marrow
References Index
1. Carcillo J et al. Clinical practise parameters …. Crit care Med 2002 (30) 6: 1365-1374 2. Dellinger P et al. Surviving Sepsis campaign guidelines…. Crit care med 2004; 32(3): 858-69 3. Goldstein B. International pediatric Sepsis Consensus conference…. Ped Crit care med 2005; 6(1): 1-8. 4. Hayden M, Schibler A. QPICS Septic Shock Practise Guideline. March 2005.
Author(s): J. Fraser, E. Crowne, Page 4/4 A. Finn, C. Steward A. Ramanan
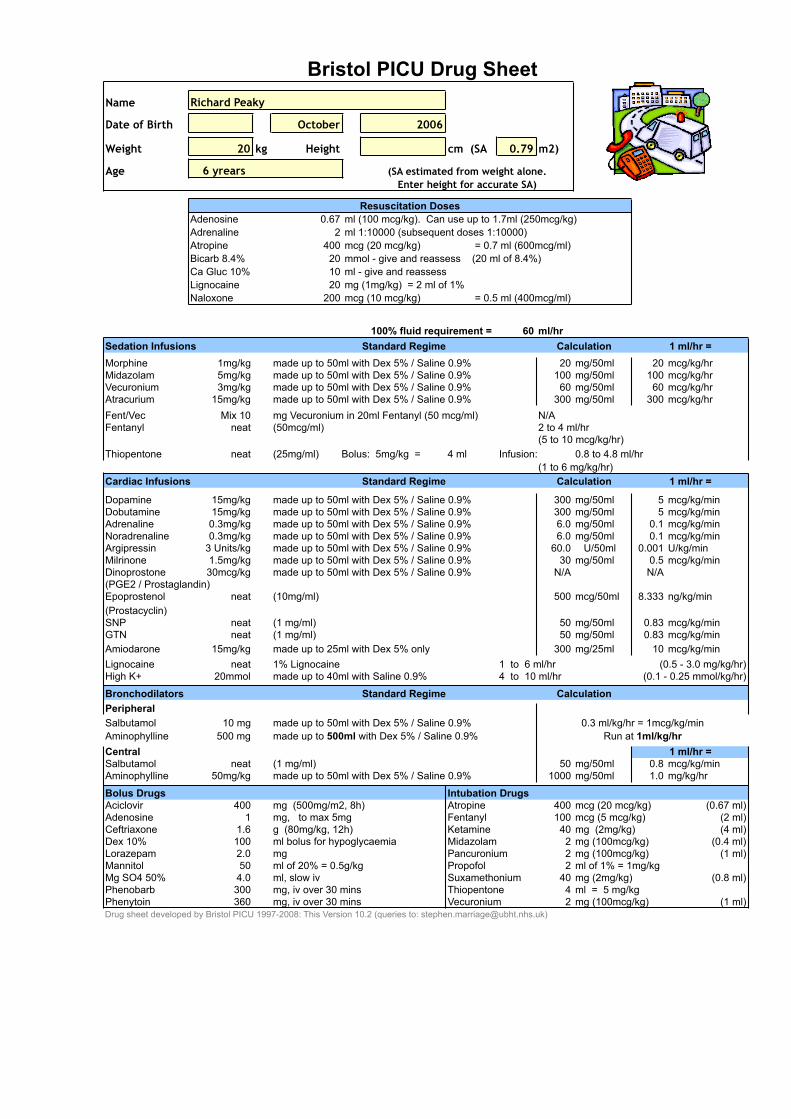
Name
Date of Birth October 2006
Weight 20 kg Height cm (SA 0.79 m2)
Age
Adenosine 0.67 ml (100 mcg/kg). Can use up to 1.7ml (250mcg/kg)Adrenaline 2 ml 1:10000 (subsequent doses 1:10000)Atropine 400 mcg (20 mcg/kg) = 0.7 ml (600mcg/ml)Bicarb 8.4% 20 mmol - give and reassess (20 ml of 8.4%)
10 ml - give and reassessLignocaine 20 mg (1mg/kg) = 2 ml of 1%Naloxone 200 mcg (10 mcg/kg) = 0.5 ml (400mcg/ml)
100% fluid requirement = 60 ml/hrSedation InfusionsMorphine 1mg/kg made up to 50ml with Dex 5% / Saline 0.9% 20 mg/50ml 20 mcg/kg/hrMidazolam 5mg/kg made up to 50ml with Dex 5% / Saline 0.9% 100 mg/50ml 100 mcg/kg/hrVecuronium 3mg/kg made up to 50ml with Dex 5% / Saline 0.9% 60 mg/50ml 60 mcg/kg/hrAtracurium 15mg/kg made up to 50ml with Dex 5% / Saline 0.9% 300 mg/50ml 300 mcg/kg/hrFent/Vec Mix 10 mg Vecuronium in 20ml Fentanyl (50 mcg/ml) N/A Fentanyl neat (50mcg/ml) 2 to 4 ml/hr
(5 to 10 mcg/kg/hr)Thiopentone neat 4 ml Infusion: 0.8 to 4.8 ml/hr
(1 to 6 mg/kg/hr)Cardiac Infusions
Dopamine 15mg/kg made up to 50ml with Dex 5% / Saline 0.9% 300 mg/50ml 5 mcg/kg/minDobutamine 15mg/kg made up to 50ml with Dex 5% / Saline 0.9% 300 mg/50ml 5 mcg/kg/minAdrenaline 0.3mg/kg made up to 50ml with Dex 5% / Saline 0.9% 6.0 mg/50ml 0.1 mcg/kg/minNoradrenaline 0.3mg/kg made up to 50ml with Dex 5% / Saline 0.9% 6.0 mg/50ml 0.1 mcg/kg/minArgipressin 3 Units/kg made up to 50ml with Dex 5% / Saline 0.9% 60.0 U/50ml 0.001 U/kg/minMilrinone 1.5mg/kg made up to 50ml with Dex 5% / Saline 0.9% 30 mg/50ml 0.5 mcg/kg/minDinoprostone 30mcg/kg made up to 50ml with Dex 5% / Saline 0.9% N/A N/A(PGE2 / Prostaglandin)Epoprostenol neat (10mg/ml) 500 mcg/50ml 8.333 ng/kg/min(Prostacyclin)SNP neat (1 mg/ml) 50 mg/50ml 0.83 mcg/kg/minGTN neat (1 mg/ml) 50 mg/50ml 0.83 mcg/kg/minAmiodarone 15mg/kg made up to 25ml with Dex 5% only 300 mg/25ml 10 mcg/kg/minLignocaine neat 1% Lignocaine 1 to 6 ml/hr (0.5 - 3.0 mg/kg/hr)High K+ 20mmol made up to 40ml with Saline 0.9% 4 to 10 ml/hr (0.1 - 0.25 mmol/kg/hr)
BronchodilatorsPeripheralSalbutamol 10 mg made up to 50ml with Dex 5% / Saline 0.9%Aminophylline 500 mg made up to 500ml with Dex 5% / Saline 0.9%CentralSalbutamol neat (1 mg/ml) 50 mg/50ml 0.8 mcg/kg/minAminophylline 50mg/kg made up to 50ml with Dex 5% / Saline 0.9% 1000 mg/50ml 1.0 mg/kg/hr
Bolus Drugs Intubation DrugsAciclovir 400 mg (500mg/m2, 8h) Atropine 400 mcg (20 mcg/kg) (0.67 ml)Adenosine 1 mg, to max 5mg Fentanyl 100 mcg (5 mcg/kg) (2 ml)Ceftriaxone 1.6 g (80mg/kg, 12h) Ketamine 40 mg (2mg/kg) (4 ml)Dex 10% 100 ml bolus for hypoglycaemia Midazolam 2 mg (100mcg/kg) (0.4 ml)Lorazepam 2.0 mg Pancuronium 2 mg (100mcg/kg) (1 ml)Mannitol 50 ml of 20% = 0.5g/kg Propofol 2 ml of 1% = 1mg/kgMg SO4 50% 4.0 ml, slow iv Suxamethonium 40 mg (2mg/kg) (0.8 ml)Phenobarb 300 mg, iv over 30 mins Thiopentone 4 ml = 5 mg/kgPhenytoin 360 mg, iv over 30 mins Vecuronium 2 mg (100mcg/kg) (1 ml)Drug sheet developed by Bristol PICU 1997-2008: This Version 10.2 (queries to: [email protected])
1 ml/hr =
Enter height for accurate SA)
1 ml/hr =
0.3 ml/kg/hr = 1mcg/kg/minRun at 1ml/kg/hr
Calculation
(25mg/ml) Bolus: 5mg/kg =
Calculation
CalculationStandard Regime
Ca Gluc 10%
Standard Regime
Standard Regime 1 ml/hr =
Bristol PICU Drug SheetRichard Peaky
Resuscitation Doses
6 yrears (SA estimated from weight alone.

Name: Richard Peaky Request: 1235-3467
Serum/plasma Magnesium 0.50 mmol/L (0.70-1.00) Calcium 2.20 mmol/L (2.25-2.80) Calcium (corrected) 2.60 mmol/L (2.25-2.80) Phosphate 1.00 mmol/L (1.30-2.00) Bilirubin 12 umol/L (< 17) Alkaline phosphatise 175 IU/L (70-250) Alanine aminotransferase 35 IU/L (5-40) Total protein 46 g/L (62-80) Albumin 20 g/L (29-55) Globulin 26 g/L (22-36) Serum/plasma Creatinine 68 umol/L (28-60) Urea 8.90 mmol/L (1.4-5.4) Sodium 135 mmol/L (133-143) Potassium 4.60 mmol/L (3.7-5.2) Chloride 111 mmol/L (95-105) Bicarbonate 12 mmol/L (21-34) Anion gap 18 mmol/L (6-14) C-reactive protein 189 mg/L (< 10) COAGULATION SCREEN Prothrombin time 18.00 s (9.5-12.0) INR 1.50 Aptt time 63.00 s (20.0-45.0) Aptt ratio 1.60 Hb:9.80g/dL (11.5-16.5)Plt:36 10*9/L(150-400)Wbc: 2.00 10*9/L(5.00-19.00) Rbc 10*12/L : 4.60 (3.00-5.40) Neut 10*9/L : 0.80 (3.00-9.00) Hct 1/1 : 0.30 (0.33-0.53) Lymp 10*9/L : 1.20 (3.00-16.00) MCV fL : 98.0 (92.0-116.0) Mono 10*9/L : 0.00 (0.30-1.00) MCH pg : 32.0 (30.0-36.0) Eosi 10*9/L : 0.00 (0.20-1.00) MCHC g/dL : 35.0 (29.0-37.0) Baso 10*9/L : 0.00 (< 0.11) Hypo % : 2.00
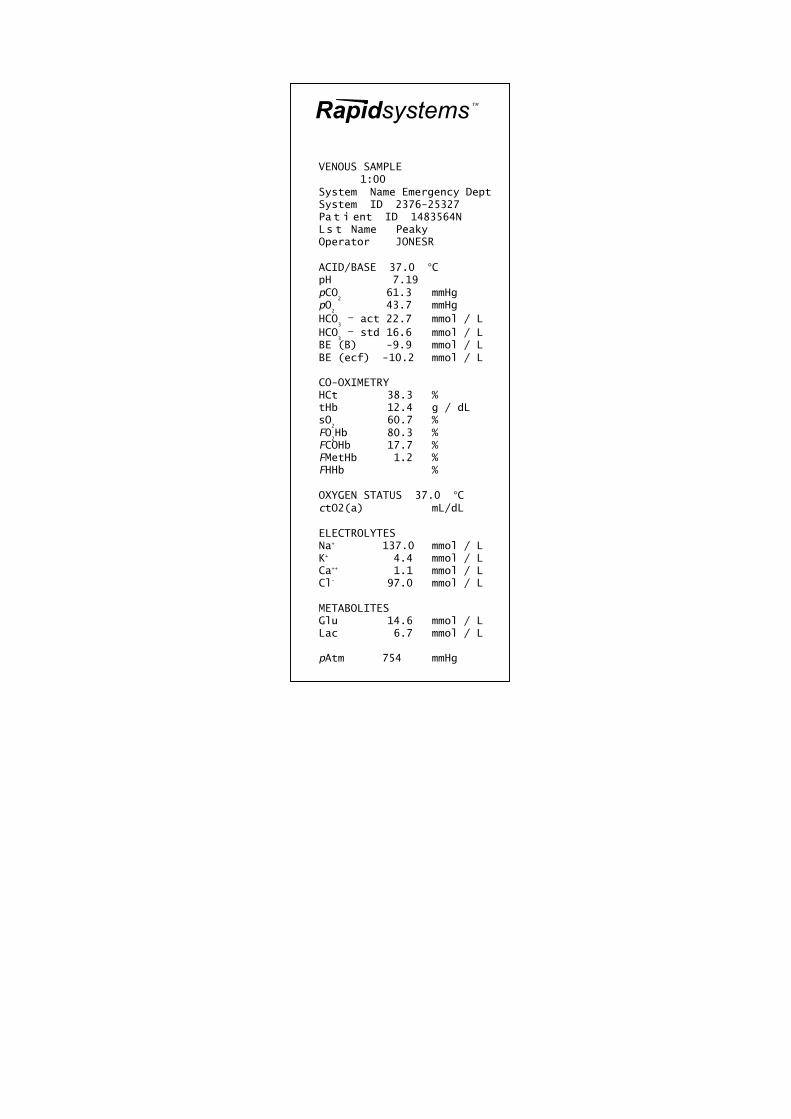
Rapidsystems
VENOUS SAMPLE
1:00 System Name Emergency Dept System ID 2376-25327 Pa t i ent ID 1483564N Ls t Name Peaky Operator JONESR ACID/BASE 37.0 °C pH 7.19 pCO
2 61.3 mmHg
pO2
43.7 mmHg HCO
3 – act 22.7 mmol / L
HCO3 – std 16.6 mmol / L
BE (B) -9.9 mmol / L BE (ecf) -10.2 mmol / L CO-OXIMETRY HCt 38.3 % tHb 12.4 g / dL sO
2 60.7 %
FO2Hb 80.3 %
FCOHb 17.7 % FMetHb 1.2 % FHHb
% OXYGEN STATUS 37.0 °C ctO2(a)
mL/dL ELECTROLYTES Na+ 137.0 mmol / L K+ 4.4 mmol / L Ca++ 1.1 mmol / L Cl- 97.0 mmol / L METABOLITES Glu 14.6 mmol / L Lac 6.7 mmol / L pAtm 754 mmHg

Rapidsystems
VENOUS SAMPLE 1:00 System Name Emergency Dept System ID 2376-25327 Pa t i ent ID 1483564N Ls t Name Peaky Operator JONESR ACID/BASE 37.0 °C pH 7.19 pCO
2 8.1 kPa
pO2
5.8 kPa HCO
3 – act 22.7 mmol / L
HCO3 – std 16.6 mmol / L
BE (B) -9.9 mmol / L BE (ecf) -10.2 mmol / L CO-OXIMETRY HCt 38.3 % tHb 12.4 g / dL sO
2 60.7 %
FO2Hb 80.3 %
FCOHb 17.7 % FMetHb 1.2 % FHHb % OXYGEN STATUS 37.0 °C ctO2(a) mL/dL ELECTROLYTES Na+ 137.0 mmol / L K+ 4.4 mmol / L Ca++ 1.1 mmol / L Cl- 97.0 mmol / L METABOLITES Glu 14.6 mmol / L Lac 6.7 mmol / L pAtm 754 mmHg

Rapidsystems
VENOUS SAMPLE
2 System Name Emergency Dept System ID 2376-25327 Pa t i ent ID 1483564N Ls t Name Peaky Operator JONESR ACID/BASE 37.0 °C pH 7.16 pCO
2 54.1 mmHg
pO2
55.3 mmHg HCO
3 – act 15.7 mmol / L
HCO3 – std 12.6 mmol / L
BE (B) -13.1 mmol / L BE (ecf) -14.1 mmol / L CO-OXIMETRY HCt 28.3 % tHb 8.4 g / dL sO
2 45.3 %
FO2Hb 80.3 %
FCOHb 19.7 % FMetHb 1.2 % FHHb
% OXYGEN STATUS 37.0 °C ctO2(a)
mL/dL ELECTROLYTES Na+ 137.0 mmol / L K+ 4.4 mmol / L Ca++ 0.8 mmol / L Cl- 97.0 mmol / L METABOLITES Glu 16.1 mmol / L Lac 7.1 mmol / L pAtm 754 mmHg

Rapidsystems
VENOUS SAMPLE 2 System Name Emergency Dept System ID 2376-25327 Pa t i ent ID 1483564N Ls t Name Peaky Operator JONESR ACID/BASE 37.0 °C pH 7.16 pCO
2 7.2 kPa
pO2
7.3 kPa HCO
3 – act 15.7 mmol / L
HCO3 – std 12.6 mmol / L
BE (B) -13.1 mmol / L BE (ecf) -14.1 mmol / L CO-OXIMETRY HCt 28.3 % tHb 8.4 g / dL sO
2 45.3 %
FO2Hb 80.3 %
FCOHb 19.7 % FMetHb 1.2 % FHHb % OXYGEN STATUS 37.0 °C ctO2(a) mL/dL ELECTROLYTES Na+ 137.0 mmol / L K+ 4.4 mmol / L Ca++ 0.8 mmol / L Cl- 97.0 mmol / L METABOLITES Glu 16.1 mmol / L Lac 7.1 mmol / L pAtm 754 mmHg