covers for hnp -...
TRANSCRIPT

Appendixes

An auxiliary nurse midwife speaking to slum dwellers about contraception and other sexual health matters in India. Photo by John Isaac,courtesy of the World Bank Photo Library.

1 0 3
APPENDIX A: WORLD BANK GROUP HNP TIMELINE

Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e
1 0 4
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
1952
1956
1961
1964
1968
Econ
omic
Sur
vey
mis
sion
to J
amai
ca to
stud
y th
e co
untry
’s de
velo
pmen
t req
uire
-m
ents
con
side
rs th
e ef
fect
s of
rapi
dpo
pula
tion
grow
th. (
Mar
ch) (
1)
IFC
is e
stab
lishe
d as
an
inst
itutio
n of
the
Wor
ld B
ank
Grou
p to
pro
mot
e su
stai
nabl
epr
ivat
e se
ctor
inve
stm
ent i
n de
velo
ping
coun
tries
.
Wor
ld B
ank
begi
ns le
ndin
g fo
r wat
ersu
pply
and
san
itatio
n pr
ojec
ts. (
2)
Robe
rt M
cNam
ara
beco
mes
Wor
ld B
ank
Pres
iden
t. (A
pril)
(1)
McN
amar
a ca
lls fo
r gov
ernm
ents
tode
velo
p st
rate
gies
to c
ontro
l pop
ulat
ion
grow
th. H
e ad
mits
that
ther
e is
no
alte
rnat
ive
to th
e W
orld
Ban
k’sin
volv
emen
t in
“thi
s cr
isis
.” (O
ctob
er) (
1)
Conc
ern
over
the
impa
ct o
f pop
ulat
ion
grow
th o
n de
velo
pmen
t is
disc
usse
d at
Seve
nth
Annu
al M
eetin
gs in
Mex
ico
City
.Ch
airm
an o
f the
Boa
rd o
f Gov
erno
rsar
gues
that
the
Wor
ld B
ank
is w
ell p
lace
dto
com
bine
sou
nd b
anki
ng p
rinci
ples
with
crea
tive
effo
rts to
add
ress
pop
ulat
ion
grow
th is
sues
. (Se
ptem
ber)
(1)
The
first
IFC
inve
stm
ent i
n ph
arm
aceu
ti-ca
ls, “
Huht
amak
i-Yht
yma
Oy”
of F
inla
nd,
is a
ppro
ved.
Econ
omic
s De
partm
ent’s
Spe
cial
Stu
dies
Divi
sion
is re
orga
nize
d to
cre
ate
aPo
pula
tion
Stud
ies
Divi
sion
hea
ded
byE.
K. H
awki
ns. (
3)
Popu
latio
n Pr
ojec
ts D
epar
tmen
t is
esta
blis
hed
unde
r the
Offi
ce o
f the
Dire
ctor
of P
roje
cts.
(Nov
embe
r) (4
)
K. K
anag
arat
nam
is a
sked
and
acc
epts
the
post
as h
ead
of th
e Po
pula
tion
Proj
ects
Depa
rtmen
t; ho
wev
er, h
e is
una
ble
tost
art i
mm
edia
tely,
and
in th
e in
terim
Geor
ge C
. Zai
dan
beco
mes
the
first
divi
sion
chi
ef o
f the
new
dep
artm
ent.
(3)

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 0 5
1969
1970
1971
1972
1973
McN
amar
a ca
lls fo
r em
phas
is o
n po
pula
-tio
n pl
anni
ng, e
duca
tiona
l adv
ance
s, a
ndag
ricul
tura
l gro
wth
in h
is A
nnua
l Mee
t-in
gs a
ddre
ss. H
e hi
ghlig
hts
the
need
for
deve
lopm
ent i
n nu
tritio
n, w
ater
sup
ply,
and
liter
acy.
(Sep
tem
ber)
(1)
In h
is An
nual
Mee
ting
addr
ess,
McN
amar
aem
phas
izes
the
impo
rtanc
e of
add
ress
ing
the
basi
c pr
oble
ms
affe
ctin
g th
e da
ilyliv
es o
f peo
ple
in d
evel
opin
g co
untri
es,
incl
udin
g nu
tritio
n, e
mpl
oym
ent,
and
inco
me
dist
ribut
ion,
am
ong
othe
rs. H
ede
scrib
es m
alnu
tritio
n as
a m
ajor
bar
rier
to h
uman
dev
elop
men
t. (S
epte
mbe
r) (1
)
A Ba
nk-w
ide
reor
gani
zatio
n cr
eate
s a
seni
or v
ice
pres
iden
t of o
pera
tions
with
five
Regi
onal
vic
e pr
esid
ents
and
a v
ice
pres
iden
t for
pro
ject
sta
ff. (A
ugus
t) (1
)
McN
amar
a us
es h
is a
ddre
ss a
t the
Annu
al M
eetin
gs to
em
phas
ize th
e ne
edto
inco
rpor
ate
popu
latio
n pl
anni
ng in
tode
velo
pmen
t stra
tegi
es. (
Sept
embe
r) (1
)
Firs
t pop
ulat
ion
loan
is a
ppro
ved
for
$2 m
illio
n to
sup
port
Jam
aica
’s fa
mily
plan
ning
pro
gram
. (Ju
ne) (
1)
As a
resu
lt of
the
reor
gani
zatio
n, a
Popu
latio
n an
d N
utrit
ion
Proj
ects
(PN
P)De
partm
ent a
nd s
ever
al o
ther
s w
ith to
ofe
w s
taff
for d
ecen
traliz
atio
n ar
e gr
oupe
din
the
Cent
ral O
pera
tion
Proj
ects
Depa
rtmen
t and
pro
vide
tech
nica
lse
rvic
es to
the
Regi
ons.
(4)
The
Boar
d of
Exe
cutiv
e Di
rect
ors
appr
oves
McN
amar
a’s p
ropo
sal f
or th
e Ba
nk to
take
the
lead
in m
obili
zing
inte
rnat
iona
l fun
dsfo
r an
onch
ocer
sias
is (r
iver
blin
dnes
s)co
ntro
l pro
gram
. (M
ay) (
1)
Poss
ible
Ban
k Act
ions
on
Mal
nutri
tion
Prob
lem
s is
rele
ased
. It i
s in
fluen
tial i
nca
lling
atte
ntio
n to
the
Bank
’s ro
le in
addr
essi
ng m
alnu
tritio
n. (J
anua
ry) (
5*)
Sect
oral
Pro
gram
s and
Pol
icies
Pap
erin
clud
es re
com
men
datio
ns o
n po
pula
tion
polic
ies.
It p
oint
s to
the
econ
omic
effe
cts
of p
opul
atio
n gr
owth
in d
evel
opin
gco
untri
es, d
escr
ibes
the
Bank
’s ef
forts
toas
sist
mem
ber c
ount
ries
to re
duce
popu
latio
n gr
owth
rate
s, a
nd o
utlin
es it
sfu
ture
pro
gram
in p
opul
atio
n as
sist
ance
.(M
arch
) (6*
)
A nu
tritio
n po
licy
pape
r mak
es th
e ca
sefo
r inv
estm
ent i
n nu
tritio
n an
d pr
opos
esth
at th
e Ba
nk “
assu
me
a m
ore
activ
e an
ddi
rect
role
in n
utrit
ion.
” (8
*)
Wor
ld B
ank/
WHO
Coo
pera
tive
Prog
ram
ises
tabl
ishe
d to
add
ress
wat
er s
uppl
y,w
aste
dis
posa
l, an
d st
orm
dra
inag
e.(S
epte
mbe
r) (1
)
Wor
ld B
ank
parti
cipa
tes
in a
n ad
viso
ryca
paci
ty in
WHO
’s Sp
ecia
l Pro
gram
of
Rese
arch
Dev
elop
men
t and
Trai
ning
inHu
man
Rep
rodu
ctio
n (H
RP).
(7)
Wor
ld B
ank
conv
enes
Mee
ting
ofOn
choc
ersi
asis
Con
trol P
rogr
am in
Par
isw
ith W
HO, t
he U
.N. F
ood
and
Agric
ultu
reOr
gani
zatio
n (FA
O), t
he U
nite
d N
atio
nsDe
velo
pmen
t Pro
gram
(UN
DP).
The
purp
ose
of th
e m
eetin
g is
to fo
rmul
ate
ast
rate
gy to
figh
t riv
er b
lindn
ess.
(Jun
e) (1
)
(Tabl
e co
ntin
ues n
ext p
age)
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
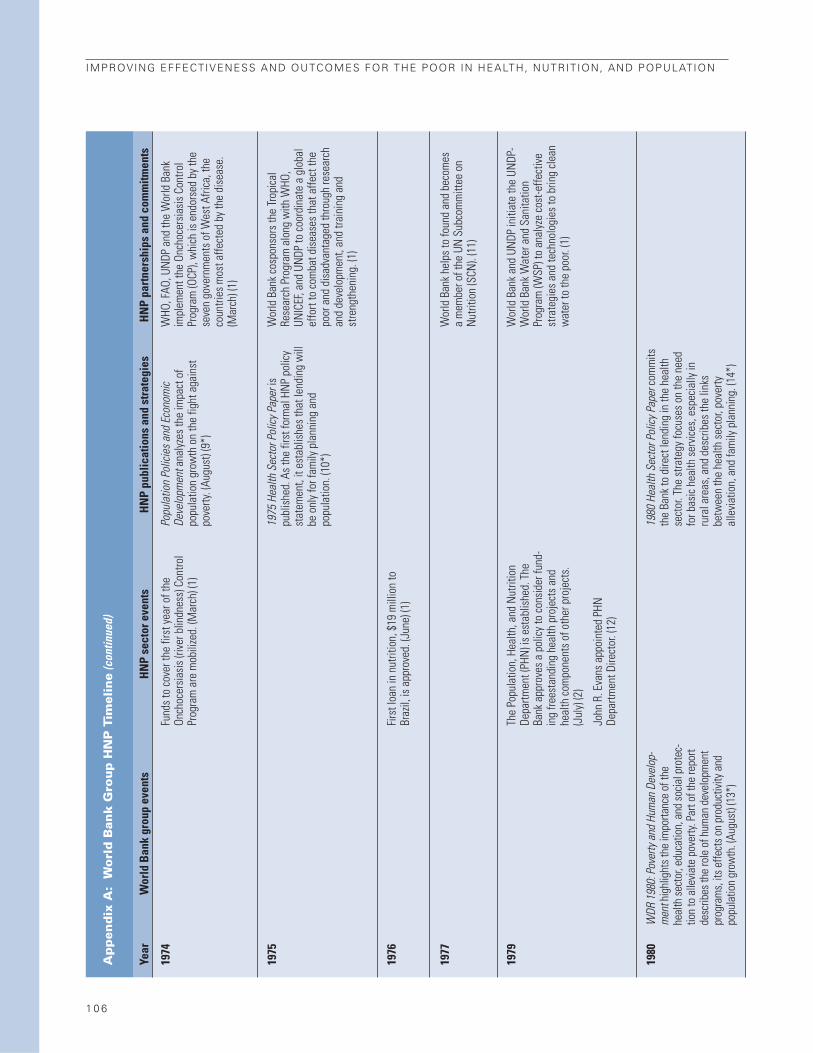
1974
1975
1976
1977
1979
1980
WDR
198
0: P
over
ty a
nd H
uman
Dev
elop
-m
ent h
ighl
ight
s the
impo
rtanc
e of
the
heal
th se
ctor
, edu
catio
n, a
nd so
cial p
rote
c-tio
n to
alle
viate
pov
erty.
Par
t of t
he re
port
desc
ribes
the
role
of h
uman
dev
elop
men
tpr
ogra
ms,
its e
ffect
s on
prod
uctiv
ity a
ndpo
pula
tion
grow
th. (
Augu
st) (
13*)
Fund
s to
cov
er th
e fir
st y
ear o
f the
Onch
ocer
sias
is (r
iver
blin
dnes
s) C
ontro
lPr
ogra
m a
re m
obili
zed.
(Mar
ch) (
1)
Firs
t loa
n in
nut
ritio
n, $
19 m
illio
n to
Braz
il, is
app
rove
d. (J
une)
(1)
The
Popu
latio
n, H
ealth
, and
Nut
ritio
nDe
partm
ent (
PHN
) is
esta
blis
hed.
The
Bank
app
rove
s a
polic
y to
con
side
r fun
d-in
g fre
esta
ndin
g he
alth
pro
ject
s an
dhe
alth
com
pone
nts
of o
ther
pro
ject
s.(J
uly)
(2)
John
R. E
vans
app
oint
ed P
HNDe
partm
ent D
irect
or. (
12)
Popu
latio
n Po
licie
s and
Eco
nom
icDe
velo
pmen
t ana
lyze
s th
e im
pact
of
popu
latio
n gr
owth
on
the
fight
aga
inst
pove
rty. (
Augu
st) (
9*)
1975
Hea
lth S
ecto
r Pol
icy P
aper
ispu
blis
hed.
As
the
first
form
al H
NP
polic
yst
atem
ent,
it es
tabl
ishe
s th
at le
ndin
g w
illbe
onl
y fo
r fam
ily p
lann
ing
and
popu
latio
n. (1
0*)
1980
Hea
lth S
ecto
r Pol
icy P
aper
com
mits
the
Bank
to d
irect
lend
ing
in th
e he
alth
sect
or. T
he s
trate
gy fo
cuse
s on
the
need
for b
asic
hea
lth s
ervi
ces,
esp
ecia
lly in
rura
l are
as, a
nd d
escr
ibes
the
links
betw
een
the
heal
th s
ecto
r, po
verty
alle
viat
ion,
and
fam
ily p
lann
ing.
(14*
)
WHO
, FAO
, UN
DP a
nd th
e W
orld
Ban
kim
plem
ent t
he O
ncho
cers
iasi
s Co
ntro
lPr
ogra
m (O
CP),
whi
ch is
end
orse
d by
the
seve
n go
vern
men
ts o
f Wes
t Afri
ca, t
heco
untri
es m
ost a
ffect
ed b
y th
e di
seas
e.(M
arch
) (1)
Wor
ld B
ank
cosp
onso
rs th
e Tr
opic
alRe
sear
ch P
rogr
am a
long
with
WHO
,UN
ICEF
, and
UN
DP to
coo
rdin
ate
a gl
obal
effo
rt to
com
bat d
isea
ses
that
affe
ct th
epo
or a
nd d
isad
vant
aged
thro
ugh
rese
arch
and
deve
lopm
ent,
and
train
ing
and
stre
ngth
enin
g. (1
)
Wor
ld B
ank
help
s to
foun
d an
d be
com
esa
mem
ber o
f the
UN
Sub
com
mitt
ee o
nN
utrit
ion
(SCN
). (1
1)
Wor
ld B
ank
and
UNDP
initi
ate
the
UNDP
-W
orld
Ban
k W
ater
and
San
itatio
nPr
ogra
m (W
SP) t
o an
alyz
e co
st-e
ffect
ive
stra
tegi
es a
nd te
chno
logi
es to
brin
g cl
ean
wat
er to
the
poor
. (1)
1 0 6
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 0 7
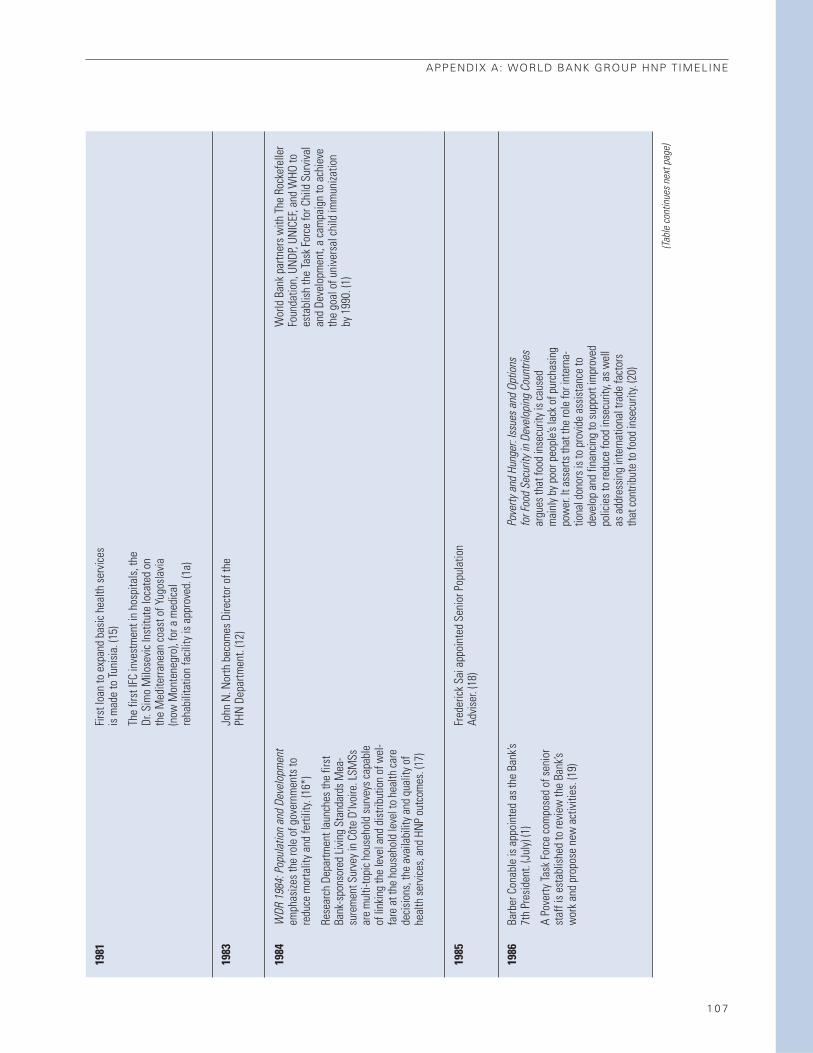
1981
1983
1984
1985
1986
WDR
198
4: P
opul
atio
n an
d De
velo
pmen
tem
phas
izes
the
role
of g
over
nmen
ts to
redu
ce m
orta
lity
and
ferti
lity.
(16*
)
Rese
arch
Dep
artm
ent l
aunc
hes
the
first
Bank
-spo
nsor
ed L
ivin
g St
anda
rds
Mea
-su
rem
ent S
urve
y in
Côt
e D’
Ivoi
re. L
SMSs
are
mul
ti-to
pic
hous
ehol
d su
rvey
s ca
pabl
eof
link
ing
the
leve
l and
dis
tribu
tion
of w
el-
fare
at t
he h
ouse
hold
leve
l to
heal
th c
are
deci
sion
s, th
e av
aila
bilit
y an
d qu
ality
of
heal
th s
ervi
ces,
and
HN
P ou
tcom
es. (
17)
Barb
er C
onab
le is
app
oint
ed a
s th
e Ba
nk’s
7th
Pres
iden
t. (J
uly)
(1)
A Po
verty
Task
For
ce c
ompo
sed
of s
enio
rst
aff i
s es
tabl
ishe
d to
revi
ew th
e Ba
nk’s
wor
k an
d pr
opos
e ne
w a
ctiv
ities
. (19
)
Firs
t loa
n to
exp
and
basi
c he
alth
ser
vice
sis
mad
e to
Tuni
sia.
(15)
The
first
IFC
inve
stm
ent i
n ho
spita
ls, t
heDr
. Sim
o M
ilose
vic
Inst
itute
loca
ted
onth
e M
edite
rrane
an c
oast
of Y
ugos
lavi
a(n
ow M
onte
negr
o), f
or a
med
ical
reha
bilit
atio
n fa
cilit
y is
app
rove
d. (1
a)
John
N. N
orth
bec
omes
Dire
ctor
of t
hePH
N D
epar
tmen
t. (1
2)
Fred
eric
k Sa
i app
oint
ed S
enio
r Pop
ulat
ion
Advi
ser.
(18)
Pove
rty a
nd H
unge
r: Iss
ues a
nd O
ptio
nsfo
r Foo
d Se
curit
y in
Deve
lopi
ng C
ount
ries
argu
es th
at fo
od in
secu
rity i
s cau
sed
mai
nly b
y poo
r peo
ple’s
lack
of p
urch
asin
gpo
wer
. It a
sser
ts th
at th
e ro
le fo
r int
erna
-tio
nal d
onor
s is t
o pr
ovid
e as
sista
nce
tode
velo
p an
d fin
ancin
g to
supp
ort i
mpr
oved
polic
ies t
o re
duce
food
inse
curit
y, as
wel
las
add
ress
ing
inte
rnat
iona
l tra
de fa
ctor
sth
at co
ntrib
ute
to fo
od in
secu
rity.
(20)
Wor
ld B
ank
partn
ers
with
The
Roc
kefe
ller
Foun
datio
n, U
NDP
, UN
ICEF
, and
WHO
toes
tabl
ish
the
Task
For
ce fo
r Chi
ld S
urvi
val
and
Deve
lopm
ent,
a ca
mpa
ign
to a
chie
veth
e go
al o
f uni
vers
al c
hild
imm
uniza
tion
by 1
990.
(1)
(Tabl
e co
ntin
ues n
ext p
age)

1 0 8
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
1987
1988
1989
1990
Pres
iden
t Con
able
ann
ounc
es a
n in
tern
alre
orga
niza
tion
to b
e co
mpl
eted
by
Sept
embe
r. (M
ay) (
1)
The
IDA
Debt
Red
uctio
n Fa
cilit
y is
esta
blis
hed
to re
duce
the
stoc
k of
deb
tow
ed to
com
mer
cial
cre
dito
rs b
y ID
A-on
lyco
untri
es. (
Augu
st) (
1)
Bank
fina
nces
the
first
free
stan
ding
nong
over
nmen
tal o
rgan
izatio
n-im
plem
ente
d pr
ojec
t for
gra
ssro
ots
deve
lopm
ent i
n To
go. (
19)
Firs
t soc
ial f
und
proj
ect i
s ap
prov
ed. (
1)
The
IBRD
app
rove
s th
e la
rges
t loa
n at
this
poi
nt in
its
hist
ory
(nom
inal
term
s) to
Mex
ico
to s
uppo
rt a
debt
-redu
ctio
npr
ogra
m, a
nd th
e De
bt-R
educ
tion
Faci
lity
for I
DA-o
nly
coun
tries
und
erta
kes
its fi
rst
oper
atio
n in
Bol
ivia
. (19
)
PHN
bec
omes
a d
ivis
ion
of th
e Po
pula
tion
and
Hum
an R
esou
rces
(PHR
) Dep
artm
ent.
Tech
nica
l dep
artm
ents
, inc
ludi
ng P
HNun
its, a
re c
reat
ed w
ithin
eac
h re
gion
, and
coun
try d
epar
tmen
ts a
re c
reat
ed w
ithin
Regi
ons,
com
bini
ng th
e fu
nctio
ns fo
rmer
lydi
vide
d be
twee
n pr
ogra
ms
and
proj
ects
depa
rtmen
ts. (
21)
Ann
O. H
amilt
on is
app
oint
ed P
HRDe
partm
ent D
irect
or. (
12)
Dean
T. J
amis
on is
app
oint
ed C
hief
Man
ager
of P
HN D
ivis
ion.
(12)
Firs
t fre
esta
ndin
g AI
DS p
roje
ct is
appr
oved
in Z
aire
. Thi
s is
als
o th
e fir
stap
prov
ed fr
eest
andi
ng B
ank
proj
ect f
or a
sing
le d
isea
se. (
21)
Anth
ony
Mea
sham
bec
omes
PHN
Chi
efM
anag
er. (
12)
Stev
en S
indi
ng b
ecom
es S
enio
rPo
pula
tion
Advi
ser.
(26)
Finan
cing
Heal
th S
ervic
es in
Dev
elop
ing
Coun
tries
: An
Agen
da fo
r Ref
orm
argu
esth
at g
over
nmen
t exp
endi
ture
s sh
ould
shift
tow
ard
prov
idin
g he
alth
ser
vice
s fo
rth
e po
or. T
he p
olic
y st
udy
addr
esse
sth
emes
of i
neffi
cien
t pub
lic s
pend
ing
onhe
alth
car
e an
d re
curre
nt c
ost f
inan
cing
.(M
ay) (
22*)
Acqu
ired
Imm
unod
efici
ency
Syn
drom
e(A
IDS)
: The
Ban
k’s A
gend
a fo
r Act
ion
ispr
epar
ed b
y th
e Af
rica
Tech
nica
l Dep
art-
men
t. It
was
not
form
ally
ado
pted
by
the
Bank
man
agem
ent a
s a
stra
tegy
but
rele
ased
as
a w
orki
ng p
aper
. (23
*)
Sub-
Saha
ran
Afric
a: Fr
om C
risis
to S
us-
tain
able
Dev
elop
men
t cal
ls fo
r a d
oubl
ing
of e
xpen
ditu
re o
n hu
man
reso
urce
dev
el-
opm
ent:
food
sec
urity
, prim
ary
educ
atio
n,an
d he
alth
car
e. (N
ovem
ber)
(25*
)
Wor
ld B
ank
cosp
onso
rs th
e Sa
fe M
othe
r-ho
od C
onfe
renc
e in
Nai
robi
, Ken
ya. T
heBa
nk p
ledg
es to
take
spe
cific
ste
ps to
addr
ess
issu
es a
ffect
ing
wom
en, a
nd th
eSa
fe M
othe
rhoo
d In
itiat
ive
is la
unch
ed.
(Feb
ruar
y) (1
)
Wor
ld B
ank
beco
mes
a fu
nder
of t
heW
HO’s
HRP.
(24)

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 0 9
(Tabl
e co
ntin
ues n
ext p
age)
1991
1992
1993
1994
Lew
is T.
Pre
ston
is a
ppoi
nted
as
the
8th
pres
iden
t of t
he W
orld
Ban
k. (S
epte
mbe
r)(2
1)
A re
port
of th
e Ta
sk F
orce
on
Portf
olio
Man
agem
ent (
the
“Wap
enha
ns R
epor
t”)
is tr
ansm
itted
to th
e Ex
ecut
ive
Dire
ctor
san
d is
a m
ajor
fact
or in
the
Bank
’sim
petu
s to
redo
uble
its
effo
rts to
war
def
fect
ive
impl
emen
tatio
n of
lend
ing
proj
ects
. (1)
WDR
199
3: In
vest
ing
in H
ealth
eval
uate
sth
e ro
les o
f gov
ernm
ents
and
mar
kets
inhe
alth
, as w
ell a
s ow
ners
hip
and
finan
cing
arra
ngem
ents
to im
prov
e he
alth
and
reac
hth
e po
or. I
t int
rodu
ces t
he d
isabi
lity-
adju
sted
life
year
(DAL
Y) to
calcu
late
the
Glob
al B
urde
n of
Dise
ase,
and
arg
ues t
hat
the
inte
rnat
iona
l com
mun
ity m
ust c
omm
itto
add
ress
ing
heal
th is
sues
. (Ju
ne) (
27*)
A po
licy
pape
r, W
ater
Res
ourc
es M
anag
e-m
ent ,
prop
oses
a n
ew a
ppro
ach
to m
an-
agin
g w
ater
reso
urce
s. T
he a
ppro
ach
advo
cate
s a
com
preh
ensi
ve p
olic
y fra
me-
wor
k an
d tre
atm
ent o
f wat
er a
s an
econ
omic
goo
d, a
long
with
dec
entra
lized
man
agem
ent a
nd d
eliv
ery
stru
ctur
es,
grea
ter r
elia
nce
on p
ricin
g, a
nd fu
ller p
ar-
ticip
atio
n by
sta
keho
lder
. (29
*)
Bank
issu
es a
sta
tem
ent t
hat a
borti
on
is a
n is
sue
coun
tries
them
selv
es m
ust
addr
ess
and
deni
es a
dvoc
atin
g th
ele
galiz
atio
n of
abo
rtion
in L
atin
Am
eric
a.(M
arch
) (1)
The
first
hea
lth-re
late
d ad
viso
ry s
ervi
cepr
ojec
t is
appr
oved
by
IFC
for t
heTh
aila
nd B
umru
ngra
d Ho
spita
l.
AIDS
in A
sia, t
he fi
rst R
egio
nal A
IDS
supp
ort u
nit,
is e
stab
lishe
d in
the
East
Asia
and
Pac
ific
Regi
on. (
21)
Jane
t de
Mer
ode
beco
mes
Dire
ctor
of t
hePH
N D
ivis
ion.
(12)
Davi
d de
Fer
rant
i bec
omes
Dire
ctor
of
PHN
Div
isio
n. (1
2)
Dise
ase
Cont
rol P
riorit
ies i
n De
velo
ping
Coun
tries
prov
ides
info
rmat
ion
on d
isea
seco
ntro
l int
erve
ntio
ns fo
r the
mos
t com
mon
dise
ases
and
inju
ries
in d
evel
opin
gco
untri
es to
hel
p th
em d
efin
e es
sent
ial
heal
th s
ervi
ce p
acka
ges.
The
pub
licat
ion
even
tual
ly le
ads
to in
crea
sed
Bank
lend
ing
for d
isea
se c
ontro
l. (O
ctob
er) (
28*)
Bette
r Hea
lth in
Afri
ca, d
irect
ed to
bot
hBa
nk a
nd e
xter
nal a
udie
nces
, arg
ues
that
beca
use
hous
ehol
ds a
nd c
omm
uniti
esha
ve th
e ca
paci
ty to
use
kno
wle
dge
and
reso
urce
s to
resp
ond
to h
ealth
pro
blem
s,po
licy
mak
ers
shou
ld m
ake
effo
rts to
cre
-at
e an
ena
blin
g en
viro
nmen
ts th
at s
timu-
late
“go
od”
deci
sion
mak
ing.
It a
lso
poin
ts o
ut th
at h
ealth
refo
rms
are
nece
s-sa
ry, t
hat c
ost-e
ffect
ive
pack
ages
of s
er-
vice
s ca
n m
eet n
eeds
, and
that
cha
nges
in d
omes
tic a
nd in
tern
atio
nal f
inan
cing
for h
ealth
are
nec
essa
ry. T
he p
ublic
atio
nw
as n
ever
app
rove
d as
an
offic
ial s
trat-
egy,
but t
he W
orld
Ban
k su
ppor
ted
an in
-de
pend
ent ‘
Bette
r Hea
lth in
Afri
ca’ E
xper
tPa
nel t
hat w
orke
d to
dis
sem
inat
e ke
ym
essa
ges
to A
frica
n po
licy
mak
ers.
(30*
)
Wor
ld B
ank
join
s w
ith U
NDP
, UN
ICEF
,W
HO, a
nd R
otar
y In
tern
atio
nal t
o fo
rmth
e Ch
ildre
n’s V
acci
ne In
itiat
ive
(CVI
).CV
I’s g
oal i
s to
vac
cina
te e
very
chi
ld in
the
wor
ld a
gain
st v
iral a
nd b
acte
rial
dise
ases
. (27
)
Wor
ld B
ank
parti
cipa
tes
in In
tern
atio
nal
Conf
eren
ce o
n N
utrit
ion
in R
ome.
(Dec
embe
r) (1
5)
Bank
par
ticip
ates
in In
tern
atio
nal
Conf
eren
ce o
n Po
pula
tion
and
Deve
lop-
men
t (IC
PD) i
n Ca
iro a
nd c
omm
its to
its
plan
of a
ctio
n. (3
1)

1 1 0
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
1995
1995
1996
Jam
es W
olfe
nsoh
n is
app
oint
ed a
s th
eni
nth
Wor
ld B
ank
pres
iden
t. (J
une)
(1)
The
Broa
d Se
ctor
App
roac
h to
Inve
stm
ent
Lend
ing:
Sec
tor I
nves
tmen
t Pro
gram
sde
fines
sec
tor i
nves
tmen
t pro
gram
s (S
IP),
anal
yzes
exp
erie
nce
with
the
new
lend
ing
inst
rum
ent a
nd a
dvoc
ates
for m
ore
lear
ning
and
sup
port
of S
IPs,
par
ticul
arly
in A
frica
. (32
)
Wor
ld B
ank P
artic
ipat
ion
Sour
cebo
okla
unch
ed. W
olfe
nsoh
n an
noun
ces
that
the
Bank
will
invo
lve
NGO
s, th
e pr
ivat
ese
ctor
, com
mun
ity g
roup
s, c
oope
rativ
es,
wom
en’s
orga
niza
tions
, and
the
poor
and
disa
dvan
tage
d in
dec
isio
n-m
akin
gpr
oces
ses.
(Feb
ruar
y) (3
3)
In h
is A
nnua
l Mee
tings
add
ress
, Wol
fen-
sohn
def
ines
the
key
elem
ents
of t
heSt
rate
gic
Com
pact
to re
new
the
Bank
Grou
p an
d im
prov
e de
velo
pmen
t effe
c-tiv
enes
s: im
prov
ing
reso
urce
mob
iliza
tion;
taki
ng m
ore
inte
grat
ed a
ppro
ache
s; b
uild
-in
g pa
rtner
ship
s an
d sh
arin
g kn
owle
dge;
and
rest
ruct
urin
g th
e Ba
nk to
be
clos
er
to c
lient
s th
roug
h re
spon
sive
and
hig
h-qu
ality
pro
duct
s. (O
ctob
er) (
33)
The
Bank
ann
ounc
es th
at th
ree
new
netw
orks
will
be
crea
ted:
Env
ironm
enta
llyan
d So
cial
ly S
usta
inab
le D
evel
opm
ent
(ESS
D), F
inan
ce, P
rivat
e Se
ctor
and
Infra
stru
ctur
e (F
PSI),
and
Pov
erty
The
Hum
an D
evel
opm
ent D
epar
tmen
t is
esta
blis
hed
and
Davi
d de
Fer
rant
i ser
ves
as D
epar
tmen
t Dire
ctor
. Ric
hard
Fea
chem
(Hea
lth),
Jorg
e Ba
rrien
tos
(Impl
emen
ta-
tion)
, Ala
n Be
rg (N
utrit
ion)
and
Tho
mas
Mer
rick
(Pop
ulat
ion)
are
app
oint
ed a
sm
anag
ers/
advi
sers
. (Ju
ly) (
4,12
)
Lear
ning
and
Lea
ders
hip
Cent
er-H
uman
Deve
lopm
ent N
etw
ork
train
ing
wee
kin
itiat
ed to
pro
vide
sta
ff w
ith in
tens
ive
train
ing
focu
sed
on to
pica
l iss
ues
in th
eHN
P se
ctor
. (15
)
Wor
ld B
ank
spon
sors
toba
cco-
rela
ted
and
non-
com
mun
icab
le d
isea
se c
onfe
renc
e in
Was
hing
ton,
DC.
(Jun
e) (1
)
The
Flag
ship
Pro
gram
on
Heal
th S
ecto
rRe
form
and
Sus
tain
able
Fin
anci
ng is
initi
ated
by
the
Econ
omic
Dev
elop
men
tIn
stitu
te (E
DI, n
ow W
orld
Ban
k In
stitu
te)
to p
rovi
de k
now
ledg
e an
d tra
inin
g on
optio
ns fo
r hea
lth s
ecto
r dev
elop
men
t,in
clud
ing
less
ons
lear
ned
and
best
pra
c-tic
es fr
om c
ount
ry e
xper
ienc
e. C
ours
e is
offe
red
at re
gion
al a
nd c
ount
ry le
vels
. (1)
IFC
laun
ches
a g
loba
l stu
dy o
n “P
rivat
eHo
spita
l Inv
estm
ent O
ppor
tuni
ties”
toid
entif
y ke
y su
cces
s fa
ctor
s fo
rin
vest
men
t in
hosp
itals
and
mor
ege
nera
lly in
hea
lth. (
2a)
The
Bank
hos
ts a
con
fere
nce
to la
unch
the
Afric
an P
rogr
am fo
r Onc
hoce
rsia
sis
Cont
rol,
a fo
llow
-up
to a
suc
cess
ful
proj
ect l
aunc
hed
in th
e 19
70s.
Spo
nsor
edby
gov
ernm
ents
, NGO
s, b
ilate
ral d
onor
san
d in
tern
atio
nal i
nstit
utio
ns, i
t im
ple-
men
ts c
omm
unity
-bas
ed d
rug-
treat
men
tpr
ogra
ms
in 1
6 Af
rican
cou
ntrie
s.(D
ecem
ber)
(1)
The
Bank
par
ticip
ates
in th
e Fo
urth
Wor
ldCo
nfer
ence
on
Wom
en in
Bei
jing
(FW
CW)
and
agre
es to
: red
uce
the
gend
er g
ap in
educ
atio
n an
d en
sure
that
wom
en h
ave
equi
tabl
e ac
cess
and
con
trol o
ver
econ
omic
reso
urce
s. (3
1)
Spec
ial U
N In
itiat
ive
for A
frica
laun
ched
;Ba
nk p
artn
ers
with
UN
to p
rom
ote
anex
pand
ed p
rogr
am o
f ass
ista
nce
to S
ub-
Saha
ran
Afric
a an
d im
prov
e co
oper
atio
nbe
twee
n th
e Ba
nk a
nd th
e UN
. Ban
kco
mm
its to
take
spe
cial
resp
onsi
bilit
y fo
rm
obili
zing
reso
urce
s fo
r bas
ic h
ealth
and
educ
atio
n re
form
s. (M
arch
) (1)
Wol
fens
ohn
anno
unce
s Ba
nk’s
supp
ort f
orth
e G-
7’s d
ecla
ratio
n an
d ob
ject
ive
ofpr
ovid
ing
an e
xit s
trate
gy fo
r hea
vily
inde
bted
cou
ntrie
s. B
ank
pled
ges
$500
mill
ion
to a
trus
t fun
d fo
r deb
t rel
ief a
s its
initi
al c
ontri
butio
n. (J
une)
(33)
Wor
ld B
ank
cosp
onso
rs th
e Jo
int U
NPr
ogra
m o
n HI
V/AI
DS (U
NAI
DS) w
ithUN
DP, U
NES
CO, U
NFP
A, U
NIC
EF, a
ndW
HO. (
21)

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 1 1
(Tabl
e co
ntin
ues n
ext p
age)
1997
Redu
ctio
n an
d Ec
onom
ic M
anag
emen
t(P
REM
). (D
ecem
ber)
(1)
Pove
rty R
educ
tion
and
the
Wor
ld B
ank:
Prog
ress
and
Cha
lleng
es in
the
1990
s is
rele
ased
and
vow
s to
redo
uble
Ban
k’sef
forts
to e
nsur
e su
cces
s in
its
man
date
to h
elp
coun
tries
redu
ce p
over
ty. T
heBa
nk s
ays
that
it w
ill ju
dge
itsel
f and
staf
f by
thei
r con
tribu
tions
to a
chie
ving
this
goa
l. (J
une)
(1)
The
Bank
and
Inte
rnat
iona
l Mon
etar
yFu
nd la
unch
the
High
ly In
debt
ed P
oor
Coun
try (H
IPC)
Initi
ativ
e, c
reat
ing
afra
mew
ork
for c
redi
tors
to p
rovi
de d
ebt
relie
f to
the
wor
ld’s
mos
t poo
r and
inde
bted
cou
ntrie
s. T
he H
IPC
Trus
t Fun
dan
d HI
PC Im
plem
enta
tion
Unit
are
esta
blis
hed.
(Nov
embe
r) (1
)
Qual
ity A
ssur
ance
Gro
up (Q
AG)
esta
blis
hed
with
the
expr
esse
d pu
rpos
eof
impr
ovin
g th
e qu
ality
of t
he B
ank’s
oper
atio
nal w
ork
with
in th
e br
oad
cont
ext
of re
duci
ng p
over
ty a
nd a
chie
ving
deve
lopm
ent i
mpa
cts.
(34)
Wor
ld D
evel
opm
ent I
ndica
tors
199
7, th
efir
st e
ditio
n, is
pub
lishe
d. W
olfe
nsoh
npo
ints
to th
e pu
blic
atio
n as
an
exam
ple
ofth
e W
orld
Ban
k’s ro
le in
dis
sem
inat
ing
know
ledg
e to
faci
litat
e de
cisi
on m
akin
g in
dev
elop
men
t. (A
pril)
(33)
The
Stra
tegi
c Co
mpa
ct p
erio
d, a
thre
e-ye
ar o
rgan
izatio
n re
new
al p
roce
ss, i
sla
unch
ed. (
April
) (1)
Bank
reor
gani
zatio
n le
ads
to th
e cr
eatio
nof
Ban
k-w
ide
“anc
hor”
uni
ts to
pro
vide
qual
ity s
uppo
rt to
the
Regi
ons.
The
reor
gani
zatio
n w
as d
esig
ned
to p
rom
ote
bala
nce
betw
een
“cou
ntry
focu
s” a
nd“s
ecto
ral e
xcel
lenc
e.”
(21)
The
Hum
an D
evel
opm
ent N
etw
ork
(HDN
)is
form
ed, a
long
with
the
HNP
Sect
orBo
ard,
whe
n Ba
nk re
orga
niza
tion
grou
psse
ctor
sta
ff in
to re
gion
al s
ecto
r uni
ts o
rde
partm
ents
. Sec
tor s
taff
wor
k w
ithco
unty
dep
artm
ents
in a
mat
rixre
latio
nshi
p. T
his
allo
ws
Regi
onal
man
ager
s w
orki
ng in
the
HNP
sect
or to
com
e to
geth
er. (
21)
Davi
d de
Fer
rant
i ser
ves
as V
ice
Pres
iden
tan
d He
ad o
f HDN
. Ric
hard
G.A
. Fea
chem
is n
amed
HN
P Di
rect
or a
nd s
erve
s as
Chai
r of t
he S
ecto
r Boa
rd. (
12)
Wor
ld B
ank
orga
nize
s an
d ho
sts
anIn
tern
atio
nal C
onfe
renc
e on
Inno
vatio
nsin
Hea
lth F
inan
cing
. (36
)
IFC
spon
sors
a g
loba
l con
fere
nce
on“I
nves
ting
in P
rivat
e Ho
spita
ls a
nd O
ther
The
1997
Hea
lth, N
utrit
ion,
and
Pop
ula-
tion
Sect
or S
trate
gy P
aper
emph
asize
sth
e im
porta
nce
of in
stitu
tiona
l and
sys
-te
mic
cha
nges
to im
prov
e he
alth
outc
omes
for t
he p
oor,
impr
ove
heal
thsy
stem
per
form
ance
, and
ach
ieve
sust
aina
ble
finan
cing
in th
e he
alth
sec
tor.
(Sep
tem
ber)
(15*
)
Conf
ront
ing
AIDS
: Pub
lic P
riorit
ies i
n a
Glob
al E
pide
mic
mak
es th
e ca
se fo
r gov
-er
nmen
t int
erve
ntio
n to
con
trol A
IDS
inde
velo
ping
cou
ntrie
s fro
m e
pide
mio
logi
-ca
l, pu
blic
hea
lth, a
nd p
ublic
eco
nom
ics
pers
pect
ives
. The
repo
rt ad
voca
tes
that
dono
rs b
ase
thei
r sup
port
on e
vide
nce
ofco
untry
-spe
cific
effe
ctiv
enes
s fo
r int
er-
vent
ions
, and
fina
nce
key
inte
rnat
iona
lpu
blic
goo
ds. (
Nov
embe
r) (3
7*)
Wor
ld B
ank
beco
mes
a d
onor
to th
ene
wly
form
ed In
tern
atio
nal A
IDS
Vacc
ine
Initi
ativ
e (IA
VI).
It is
est
ablis
hed
to e
nsur
eth
e de
velo
pmen
t of a
n HI
V va
ccin
e fo
rus
e ar
ound
the
wor
ld. (
35)
Wor
ld B
ank
colla
bora
tes
with
UN
Eco
-no
mic
Com
mis
sion
for A
frica
and
UN
ICEF
to o
rgan
ize th
e Fo
rum
on
Cost
Sha
ring
inth
e So
cial
Sec
tors
of S
ub-S
ahar
an A
frica
.Fi
fteen
prin
cipl
es fo
r cos
t sha
ring
inhe
alth
and
edu
catio
n ar
e ag
reed
upo
n at
the
Foru
m. (
38)
The
Wor
ld B
ank
and
The
Dani
sh M
inis
tryof
For
eign
Affa
irs c
ohos
t a m
eetin
g fo
rdo
nor a
genc
ies
in C
open
hage
n to
dis
cuss
sect
orw
ide
appr
oach
es. A
t the
mee
ting
the
term
SW
Ap is
coi
ned,
a S
WAp
gui
deis
com
mis
sion
ed, a
nd a
n In
ter-A
genc
yGr
oup
on S
WAp
is fo
rmed
. (32
)

1 1 2
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
1998
1999
Pres
iden
t Wol
fens
ohn’s
add
ress
at t
heAn
nual
Mee
tings
war
ns th
at fi
nanc
ial
refo
rms
are
not s
uffic
ient
, tha
t hum
anne
eds
and
soci
al ju
stic
e m
ust a
lso
beso
ught
. (1)
Asse
ssin
g Ai
d: W
hat W
orks
, Wha
tDo
esn’
t and
Why
conc
lude
s th
at th
ere
isa
role
for f
orei
gn a
id a
nd th
at p
rope
rlym
anag
ed a
id c
an c
ontri
bute
to im
prov
ing
peop
le’s
lives
. It a
rgue
s th
at in
stitu
tiona
lde
velo
pmen
t and
pol
icy
refo
rms
alon
gw
ith s
trong
thre
e-w
ay p
artn
ersh
ip a
mon
gre
cipi
ent c
ount
ries,
aid
age
ncie
s, a
nddo
nor c
ount
ries
can
impr
ove
the
impa
ctof
fore
ign
assi
stan
ce. (
39*)
IFC
intro
duce
s its
fron
tier c
ount
ry s
trate
gyto
ste
er re
sour
ces
tow
ard
“pio
neer
ing”
or
unde
rser
ved
sect
ors
in h
igh-
risk
and/
orlo
w-in
com
e co
untri
es. (
3a)
Wol
fens
ohn
calls
for d
evel
opm
ent p
art-
ners
to a
dopt
a C
ompr
ehen
sive
Dev
elop
-m
ent F
ram
ewor
k, w
hich
aim
s to
impr
ove
the
effe
ctiv
enes
s of
dev
elop
men
t act
ivi-
ties
and
mov
e be
yond
indi
vidu
al p
roje
cts,
prom
otin
g na
tiona
l lea
ders
hip
and
con-
sens
us, a
nd re
quiri
ng a
com
mitm
ent t
o
Heal
th D
eliv
ery
Syst
ems
in D
evel
opin
gCo
untri
es: O
ppor
tuni
ties
and
Risk
s,”
brin
ging
toge
ther
IFC
and
Wor
ld B
ank
staf
f and
oth
er m
ajor
priv
ate
heal
th c
are
play
ers
from
dev
elop
ing
and
deve
lope
dco
untri
es.
The
Wor
ld B
ank
laun
ches
AID
S Va
ccin
eTa
sk F
orce
to s
peed
up
depl
oym
ent o
fef
fect
ive
and
affo
rdab
le A
IDS
vacc
ine.
Itsu
ppor
ts h
igh-
leve
l dia
logu
e w
ith
polic
y m
aker
s an
d in
dust
ry, b
oth
“pus
h”an
d “p
ull”
stra
tegi
es to
gen
erat
ein
vest
men
ts in
rese
arch
and
deve
lopm
ent,
and
spon
sors
stu
dies
of
pote
ntia
l dem
and
for a
vac
cine
inde
velo
ping
cou
ntrie
s. (A
pril)
(1)
The
Wor
ld B
ank
Inst
itute
dev
elop
s a
cour
se a
nd le
arni
ng p
rogr
am ti
tled
“Ada
ptin
g to
Cha
nge”
as
a re
spon
se to
the
ICPD
. (40
)
Chris
toph
er L
ovel
ace
is a
ppoi
nted
Dire
ctor
of t
he H
NP
Sect
or. (
12)
The
Heal
th C
are
Best
Pra
ctic
e Gr
oup
isfo
rmed
in IF
C to
ana
lyze
pot
entia
lin
vest
men
ts in
hea
lth a
nd to
sha
re a
ndle
vera
ge k
now
ledg
e ab
out t
he h
ealth
care
indu
stry
that
was
dev
elop
ing
acro
ssIF
C de
partm
ents
. Nev
erth
eles
s, th
e gr
oup
has
no d
ecis
ion-
mak
ing
role
. (4a
)
The
AIDS
Cam
paig
n Te
am fo
r Afri
ca(A
CTaf
rica)
uni
t is
crea
ted
to h
elp
mai
nstre
am H
IV/A
IDS
activ
ities
in a
llse
ctor
s. (2
1)
Edua
rdo
A. D
orya
n is
app
oint
ed H
DN V
ice
Pres
iden
t. (1
2)
Popu
latio
n an
d th
e W
orld
Ban
k: Ad
aptin
gto
Cha
nge
is s
hape
d la
rgel
y by
its
com
mit-
men
t to
the
1994
ICPD
and
by a
n em
phas
ison
hea
lth s
ecto
r ref
orm
in th
e 19
90s.
Its
obje
ctiv
e is
to a
ddre
ss p
opul
atio
n is
sues
with
a p
eopl
e-ce
nter
ed a
nd m
ultis
ecto
ral
appr
oach
that
impr
oves
repr
oduc
tive
heal
th th
roug
h ac
cess
to in
form
atio
n an
d
The
Wor
ld B
ank
partn
ers
with
WHO
and
Smith
Klin
e Be
echa
m to
initi
ate
a Pr
ogra
mto
Elim
inat
e El
epha
ntia
sis
by d
istri
butin
gdr
ugs
free
of c
harg
e to
gov
ernm
ents
and
colla
bora
ting
orga
niza
tions
. (Ja
nuar
y) (1
)
The
Wor
ld B
ank,
WHO
, UN
DP, a
nd U
NIC
EFla
unch
Rol
l Bac
k M
alar
ia to
pro
vide
aco
ordi
nate
d gl
obal
app
roac
h to
hal
vem
alar
ia b
y 20
10. (
41)
The
Wor
ld B
ank
partn
ers
to e
stab
lish
The
Glob
al A
llian
ce fo
r Vac
cine
s an
dIm
mun
izatio
n (G
AVI),
a p
ublic
-priv
ate
partn
ersh
ip, t
o en
sure
fina
ncin
g to
sav
ech
ildre
n’s li
ves
and
peop
le’s
heal
thth
roug
h w
ides
prea
d va
ccin
atio
ns. (
46)

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 1 3
(Tabl
e co
ntin
ues n
ext p
age)
expa
nded
par
tner
ship
, tra
nspa
renc
y, an
dac
coun
tabi
lity.
(Jan
uary
) (33
)
Boliv
ia b
ecom
es th
e pi
lot c
ount
ry fo
r the
CDF
with
two
loan
s fo
r hea
lth a
ndin
stitu
tiona
l ref
orm
. (Ju
ne) (
1)
In p
repa
ratio
n fo
r WDR
200
0/20
01, t
heBa
nk la
unch
es th
e Vo
ices o
f the
Poo
rst
udy.
The
stud
y fo
cuse
d on
per
cept
ions
of a
qua
lity
of li
fe; p
ress
ing
prob
lem
s an
dpr
iorit
ies;
the
qual
ity o
f int
erac
tions
with
key
publ
ic, m
arke
t and
civ
il so
ciet
y in
sti-
tutio
ns in
thei
r liv
es; a
nd c
hang
es in
gen
-de
r and
soc
ial r
elat
ions
. (Se
ptem
ber)
(42*
)
Wol
fens
ohn
appo
inte
d fo
r sec
ond
term
as
Wor
ld B
ank
pres
iden
t. (S
epte
mbe
r) (3
3)
Wol
fens
ohn
links
cor
rupt
ion
and
pove
rtyat
Inte
rnat
iona
l Ant
i-Cor
rupt
ion
Conf
eren
ce in
Dur
ban.
He
stat
es th
at th
eBa
nk w
ill p
ositi
on c
orru
ptio
n as
a c
entra
lis
sue
to d
evel
opm
ent,
appl
y ex
tern
alpr
essu
res
for c
hang
e at
the
coun
try le
vel
whi
le e
ncou
ragi
ng in
tern
al p
ress
ures
for
chan
ge, a
nd c
reat
e pa
rtner
ship
s to
addr
ess
corru
ptio
n is
sues
. (Oc
tobe
r) (3
3)
The
Wor
ld B
ank
and
Inte
rnat
iona
lM
onet
ary
Fund
ann
ounc
e th
atco
nces
sion
ary
lend
ing
to 8
1 el
igib
le p
oor
coun
tries
will
be
base
d on
pov
erty
redu
ctio
n st
rate
gies
, ini
tiatin
g th
e Po
verty
Redu
ctio
n Su
ppor
t Pap
er p
roce
ss. (
43)
Enha
nced
HIP
C la
unch
ed. H
IPC
initi
ativ
eis
mod
ified
to p
rovi
de d
eepe
r and
bro
ader
relie
f, fa
ster
relie
f, an
d to
cre
ate
a m
ore
dire
ct li
nk b
etw
een
debt
relie
f and
pove
rty re
duct
ion
thro
ugh
Pove
rtyRe
duct
ion
Stra
tegy
Pap
ers.
(1)
IEG
rele
ases
an
eval
uatio
n of
the
HNP
sect
or th
at s
ugge
sts
that
the
Bank
impr
ove
know
ledg
e m
anag
emen
t,de
velo
p m
ore
flexi
ble
inst
rum
ents
, and
supp
ort i
ncre
ased
eco
nom
ic a
nd s
ecto
rw
ork
to h
elp
coun
tries
iden
tify
chal
leng
esan
d im
prov
e th
e ef
ficie
ncy,
effe
ctiv
enes
s,an
d eq
uity
of h
ealth
refo
rms.
It a
rgue
s
The
Heal
th a
nd E
duca
tion
Unit
ises
tabl
ishe
d in
IFC.
serv
ices
, and
reco
gnize
s th
e im
porta
nce
of c
onte
xtua
l fac
tors
suc
h as
gen
der
equi
ty a
nd h
uman
righ
ts. (
Janu
ary)
(31*
)
The
Bank
’s ne
w s
trate
gy to
figh
t HIV
/AID
Sin
Afri
ca in
par
tner
ship
with
Afri
can
gove
rnm
ent a
nd J
oint
UN
Pro
gram
on
HIV/
AIDS
(UN
AIDS
) app
rove
d by
Reg
iona
lLe
ader
ship
Team
. (M
ay) (
21)
A He
alth
Sec
tor S
trate
gy fo
r the
Eur
ope
and
Cent
ral A
sia R
egio
nre
spon
ds to
chan
ges
in th
e he
alth
car
e sy
stem
s,pa
rticu
larly
in tr
ansi
tion
coun
tries
, by
prov
idin
g a
guid
e to
sup
port
regi
onal
lyap
prop
riate
, int
erse
ctor
al h
ealth
sys
tem
refo
rms.
Key
prio
ritie
s ar
e id
entif
ied
as:
(i) p
rom
otin
g w
elln
ess
and
redu
cing
the
prev
alen
ce o
f avo
idab
le il
lnes
s; (i
i)cr
eatin
g af
ford
able
and
sus
tain
able
deliv
ery
syst
ems;
and
(iii)
mai
ntai
ning
func
tioni
ng h
ealth
sys
tem
s du
ring
the
refo
rm p
roce
ss. (
Sept
embe
r) (4
5*)
The
docu
men
t “In
vest
ing
in P
rivat
eHe
alth
Car
e: A
Not
e on
Stra
tegi
cDi
rect
ion
for I
FC”
is p
repa
red
by IF
C’s
Heal
th C
are
Best
Pra
ctic
e Gr
oup.
(5a)

1 1 4
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
2000
that
pro
ject
s ha
d be
en to
o co
mpl
ex, h
adne
glec
ted
inst
itutio
nal a
naly
sis
and
that
mon
itorin
g an
d ev
alua
tion
was
alm
ost
none
xist
ent.
It ur
ged
that
the
sect
or “
dobe
tter,
not m
ore,
” th
at is
, be
mor
ese
lect
ive
to d
o a
few
thin
gs b
ette
r rat
her
than
too
muc
h w
ith p
oor r
esul
ts. (
44)
Wor
ld B
ank
anno
unce
s a
plan
to w
ork
with
chu
rch
grou
ps in
Afri
ca to
figh
tpo
verty
and
AID
S. (M
arch
) (1)
Thou
sand
s of
dem
onst
rato
rs p
rote
st a
tth
e De
velo
pmen
t Com
mitt
ee’s
Sprin
gm
eetin
gs in
Was
hing
ton.
The
Dev
elop
-m
ent C
omm
ittee
rene
ws
its p
ledg
e to
spee
d up
deb
t rel
ief a
nd to
sup
port
the
fight
aga
inst
AID
S. (M
arch
) (1)
Wol
fens
ohn
addr
esse
s th
e UN
Sec
urity
Coun
cil a
nd c
alls
for i
ncre
ased
reso
urce
allo
catio
n to
figh
t a “
War
on
AIDS
,”no
ting
the
epid
emic
’s de
vast
atin
g ef
fect
son
the
deve
lopi
ng w
orld
, esp
ecia
llyAf
rica.
(Jan
uary
) (33
)
The
first
Mul
ticou
ntry
AID
S Pr
ogra
m(M
AP) i
s ap
prov
ed b
y th
e Bo
ard
and
prov
ides
a $
500
mill
ion
enve
lope
for
finan
cing
HIV
/AID
S pr
ojec
ts in
Afri
ca.
(Sep
tem
ber)
(21)
The
over
all o
bjec
tive
of th
e W
orld
Ban
kSt
rate
gy fo
r Hea
lth, N
utrit
ion,
and
Popu
latio
n in
Eas
t Asia
and
the
Pacif
icRe
gion
is to
impr
ove
the
Bank
’sef
fect
iven
ess
in h
ealth
, nut
ritio
n, a
ndpo
pula
tion
in th
e re
gion
. The
stra
tegy
urge
s se
lect
ivity
and
flex
ibili
ty to
dev
elop
new
app
roac
hes,
as
nece
ssar
y, ba
sed
onle
sson
s le
arne
d an
d ex
perie
nce
in th
ere
gion
. It p
riorit
izes:
impr
ovin
g ou
tcom
esfo
r the
poo
r, en
hanc
ing
the
perfo
rman
ceof
hea
lth c
are
syst
ems,
and
sec
urin
gsu
stai
nabl
e fin
anci
ng. (
June
) (47
*)
Wor
ld B
ank
and
WHO
issu
e a
publ
icat
ion,
Toba
cco
Cont
rol i
n De
velo
ping
Cou
ntrie
s.It
argu
es th
at a
redu
ctio
n in
toba
cco
use
is e
ssen
tial t
o im
prov
e gl
obal
hea
lth.
(Aug
ust)
(48*
)
Inte
nsify
ing
Actio
n Ag
ains
t AID
S in
Afri
caem
phas
izes
the
impo
rtanc
e of
incr
ease
dad
voca
cy to
stre
ngth
en p
oliti
cal c
omm
it-m
ent t
o fig
htin
g HI
V/AI
DS, m
obili
zatio
nof
reso
urce
s, a
nd s
treng
then
ing
the
know
ledg
e ba
se. I
t adv
ocat
es a
lloca
tion
of in
crea
sed
reso
urce
s an
d te
chni
cal s
up-
port
to a
ssis
t Afri
can
partn
ers
and
the
Wor
ld B
ank
to m
ains
tream
HIV
/AID
S in
toal
l sec
tors
. (Au
gust
) (49
*)
Wor
ld B
ank
rele
ases
44
coun
try re
ports
on S
ocio
-Eco
nom
ic D
iffer
ence
s in
Hea
lth,
Nut
ritio
n an
d Po
pula
tion.
The
repo
rtsst
ress
that
the
poor
est s
ecto
rs o
f the
popu
latio
n m
ust r
ecei
ve a
dequ
ate
heal
thca
re. (
Nov
embe
r) (5
0*)
At th
e W
orld
Eco
nom
ic F
orum
,W
olfe
nsoh
n ur
ges
wor
ld le
ader
s to
supp
ort G
AVI a
nd it
s ca
mpa
ign
for
child
ren.
(Jan
uary
) (33
)
At th
e Se
cond
Wor
ld W
ater
For
um,
Wol
fens
ohn
pled
ges
the
Bank
’s su
ppor
tto
ens
ure
that
eve
ryon
e ha
s w
ater
serv
ices
for h
ealth
, foo
d, e
nerg
y, an
d th
een
viro
nmen
t. Th
e ap
proa
ch h
e ou
tline
sem
phas
izes
parti
cipa
tory
inst
itutio
ns a
sw
ell a
s te
chno
logi
cal a
nd fi
nanc
ial
inno
vatio
n. (M
arch
) (1)
At th
e XI
IIth
Inte
rnat
iona
l AID
S Co
nfer
-en
ce, t
he W
orld
Ban
k pl
edge
s $5
00 m
il-lio
n. T
he M
ultic
ount
ry A
IDS
Prog
ram
,de
velo
ped
with
UN
AIDS
, hel
ps c
ount
ries
to im
plem
ent n
atio
nal H
IV/A
IDS
pro-
gram
s. (J
uly)
(1)
The
Bank
-Net
herla
nds
Wat
er P
artn
er-
ship
Pro
gram
(BN
WPP
) is
esta
blis
hed
toim
prov
e w
ater
sec
urity
by
prom
otin
gin
nova
tive
appr
oach
es to
Inte
grat
edW
ater
Res
ourc
es M
anag
emen
t (IW
RM),
and
ther
eby
cont
ribut
e to
pov
erty
redu
ctio
n. (5
1)

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 1 5
(Tabl
e co
ntin
ues n
ext p
age)
2001
WDR
200
0/20
01: A
ttack
ing
Pove
rtyem
phas
izes
that
inse
curit
y, in
inco
me
orhe
alth
ser
vice
s, is
one
of m
any
depr
ivat
ions
suf
fere
d by
the
poor
. (52
*)
The
Wor
ld B
ank
anno
unce
s th
at it
will
join
the
UN a
s a
full
partn
er to
impl
emen
tth
e M
illen
nium
Dev
elop
men
t Goa
ls a
ndto
put
thes
e go
als
at th
e ce
nter
of t
hede
velo
pmen
t age
nda.
(Sep
tem
ber)
(1)
Wor
ld B
ank
mak
es a
Dec
lara
tion
ofCo
mm
itmen
t at S
peci
al S
essi
on o
f the
UN G
ener
al A
ssem
bly,
reaf
firm
ing
pled
ges
mad
e by
wor
ld le
ader
s to
hal
tan
d re
vers
e th
e sp
read
of H
IV/A
IDS
by20
15. (
June
) (33
)
The
Wat
er S
uppl
y an
d Sa
nita
tion
Pro-
gram
(WSP
) Cou
ncil
is c
reat
ed to
ove
rsee
prog
ram
act
iviti
es a
nd g
uide
stra
tegi
cde
velo
pmen
t in
wat
er a
nd s
anita
tion.
(53)
Boar
d of
Exe
cutiv
e Di
rect
ors
appr
oves
age
nder
and
dev
elop
men
t mai
nstre
amin
gst
rate
gy. (
54)
Firs
t pov
erty
redu
ctio
n su
ppor
t cre
dit
(PRS
C) a
ppro
ved.
(1)
Bank
ann
ounc
es it
will
bui
ld u
pon
curre
ntpr
ogra
ms
and
follo
w th
e Ca
ribbe
anRe
gion
al S
trate
gic
Plan
of A
ctio
n fo
rHI
V/AI
DS, d
evot
ing
up to
$15
0 m
illio
n to
the
fight
aga
inst
HIV
/AID
S in
the
Carib
bean
. (Ap
ril) (
21)
Jose
ph R
itzen
app
oint
ed H
DN V
ice
Pres
iden
t. (J
une)
(1)
Lead
ersh
ip P
rogr
am o
n AI
DS la
unch
ed b
yth
e W
orld
Ban
k In
stitu
te (W
BI) t
o bu
ildca
paci
ty fo
r acc
eler
ated
impl
emen
tatio
nof
HIV
/AID
S pr
ogra
ms.
(21)
IFC A
gain
st A
IDS
is la
unch
ed w
ith th
e id
eaof
acc
eler
atin
g th
e in
volve
men
t of t
he p
ri-va
te se
ctor
in th
e fig
ht a
gain
st H
IV/ A
IDS
thro
ugh
risk m
anag
emen
t and
impl
emen
-ta
tion
of w
orkp
lace
pro
gram
s. (6
a)
The
Heal
th a
nd E
duca
tion
Unit
beco
mes
aDe
partm
ent w
ithin
IFC.
(7a)
Sub-
regi
onal
HIV
/AID
S st
rate
gy fo
r Car
ib-
bean
. HIV
/AID
S in
the
Carib
bean
: Iss
ues
and
Optio
nsre
leas
ed. (
Janu
ary)
(55*
)
The
Bank
and
par
tner
s ga
ther
in W
ash-
ingt
on, t
o fu
rther
com
mit
to o
pera
tiona
lize
the
Amst
erda
m D
ecla
ratio
n. T
he G
loba
lPl
an to
Sto
p TB
cal
ls fo
r exp
ansi
on o
fac
cess
to D
OTS
and
incr
ease
d fin
anci
alba
ckin
g fo
r the
pro
gram
from
gove
rnm
ents
thro
ugho
ut th
e w
orld
.(O
ctob
er) (
56)
The
Bank
’s W
ater
and
San
itatio
n Pr
ogra
mfo
rms
the
Priv
ate-
Publ
ic P
artn
ersh
ip fo
rHa
ndw
ashi
ng w
ith th
e Lo
ndon
Sch
ool o
fHy
gien
e an
d Tr
opic
al M
edic
ine,
the
Acad
-em
y fo
r Edu
catio
nal D
evel
opm
ent,
USAI
D,UN
ICEF
, the
Ban
k-N
ethe
rland
s W
ater
Partn
ersh
ip, a
nd th
e pr
ivat
e se
ctor
. (57
)
The
Bank
bec
omes
a tr
uste
e of
the
Glob
alFu
nd to
Figh
t HIV
/AID
S, T
B, a
nd M
alar
ia(G
FATM
), a
finan
cing
mec
hani
sm e
stab
-lis
hed
to fo
ster
par
tner
ship
s bet
wee
n go
v-er
nmen
ts, c
ivil s
ocie
ty, th
e pr
ivate
sect
or,
and
affe
cted
com
mun
ities
to in
crea
se re
-so
urce
s and
dire
ct fi
nanc
ing
tow
ard
effo
rtsto
figh
t HIV
/AID
S, T
B, a
nd m
alar
ia. (
58)
In c
oope
ratio
n w
ith th
e Ga
tes
Foun
datio
nan
d Du
tch
and
Swed
ish
gove
rnm
ents
, the
Wor
ld B
ank
Heal
th a
nd P
over
ty T
hem
atic
Grou
p in
itiat
es th
e Re
achi
ng th
e Po
orPr
ogra
m (R
PP).
RPP
is a
n ef
fort
to fi
ndbe
tter w
ays
to e
nsur
e th
at th
e be
nefit
s of
HNP
prog
ram
s flo
w to
dis
adva
ntag
edpo
pula
tion
grou
ps th
roug
h re
sear
ch,
polic
y gu
idan
ce, a
nd a
dvoc
acy.
(1)
The
Bank
join
s th
e Ro
ckef
elle
r Fou
nda-
tion,
Sid
a/SA
REC,
and
Wel
lcom
e Tr
ust t
ola
unch
the
INDE
PTH
Net
wor
k, a
n in
tern
a-tio
nal p
latfo
rm o
f sen
tinel
dem
ogra
phic
site
s th
at p
rovi
des
heal
th a
nd d
emo-
grap
hic
data
and
rese
arch
to e
nabl
e de
-ve
lopi
ng c
ount
ries
to s
et e
vide
nce-
base
dhe
alth
prio
ritie
s an
d po
licie
s. (5
9)
The
Bank
and
USA
ID c
ohos
t the
Ann
ual
Mee
tings
of t
he G
loba
l Par
tner
ship
toEl
imin
ate
Rive
rblin
dnes
s in
Was
hing
ton.
The
partn
ers
pled
ged
to e
limin
ate
river
blin
dnes
s in
Afri
ca b
y 20
10. (
1)

1 1 6
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
2002
2003
Wol
fens
ohn
pres
ents
a s
even
-poi
nt P
ost-
Mon
terre
y Ac
tion
Plan
to th
e De
velo
p-m
ent C
omm
ittee
on
how
to b
oost
dev
el-
opm
ent a
id a
nd e
ffect
iven
ess,
and
trans
late
Mon
terre
y co
mm
itmen
ts in
tore
sults
. (Ap
ril) (
33)
From
this
poin
t, Co
untry
Ass
istan
ce S
trate
-gi
es (C
ASs),
the
mai
n ve
hicle
for m
akin
gst
rate
gic c
hoice
s abo
ut p
rogr
am d
esig
nan
d re
sour
ce a
lloca
tions
for i
ndivi
dual
coun
tries
, wer
e ba
sed
on P
over
ty R
educ
-tio
n Su
ppor
t Pap
ers i
n lo
w-in
com
e co
un-
tries
. (Ju
ly) (6
0)
IDA
anno
unce
s th
at 1
8–21
per
cent
of
IDA
wou
ld b
e in
gra
nts
and
avai
labl
e fo
rsp
ecifi
c ac
tiviti
es a
nd fo
r the
deb
t-vu
lner
able
poo
rest
cou
ntrie
s. (J
uly)
(1)
Wor
ld B
ank A
nnua
l Rep
ortd
escr
ibes
the
Bank
’s co
mm
itmen
t to
mee
ting
the
MDG
san
d em
phas
izes
its c
omm
itmen
t to
four
prio
rity
sect
ors
incl
udin
g HI
V/AI
DS, w
ater
and
sani
tatio
n, h
ealth
, and
edu
catio
n fo
ral
l. (S
epte
mbe
r) (1
)
$500
mill
ion
is a
ppro
ved
for t
he s
econ
dst
age
of it
s M
ultic
ount
ry H
IV/A
IDS
Prog
ram
for A
frica
(MAP
). (F
ebru
ary)
(1)
WBI
’s co
urse
“Ad
aptin
g to
Cha
nge”
beco
mes
“Ac
hiev
ing
the
MDG
s: R
epro
-du
ctiv
e He
alth
, Pov
erty
Red
uctio
n, a
ndHe
alth
Sec
tor R
efor
m.”
(40)
Jean
-Lou
is S
arbi
b as
sum
es H
DN V
ice
Pres
iden
cy. (
July
) (12
)
Boar
d ap
prov
es fi
rst p
ilots
of b
uy-d
own
mec
hani
sm in
sev
eral
pol
io e
radi
catio
npr
ojec
ts in
Pak
ista
n an
d N
iger
ia. P
roje
cts
wer
e fin
ance
d by
Gat
es F
ound
atio
n, U
NF,
Rota
ry In
tern
atio
nal,
and
the
Cent
ers
for
Dise
ase
Cont
rol a
nd P
reve
ntio
n. (6
3)
Rom
ania
Dia
lysi
s is
the
first
pub
lic-
priv
ate
partn
ersh
ip (P
PP) p
roje
ct in
hea
lthap
prov
ed b
y IF
C.
The
HNP
Sect
or B
oard
pre
sent
s an
HN
Pst
rate
gy u
pdat
e to
the
Boar
d. T
he p
rese
n-ta
tion
revi
ews
trend
s in
pro
ject
lend
ing
and
obje
ctiv
es, a
naly
tic a
nd a
dvis
ory
ser-
vice
s, Q
AG ra
tings
, IFC
lend
ing
for H
NP,
and
staf
fing.
The
upd
ate
reco
nfirm
s th
ese
ctor
’s co
mm
itmen
t to
the
obje
ctiv
es in
the
1997
stra
tegy
. It a
lso
emph
asize
s th
atgr
eate
r cou
ntry
sel
ectiv
ity a
nd d
iver
sity
inle
ndin
g in
stru
men
ts w
ill b
e pu
rsue
d al
ong
with
effo
rts to
sha
rpen
the
focu
s on
qua
l-ity
and
effe
ctiv
enes
s, w
ork
mor
e cl
osel
yw
ith c
lient
s an
d co
mm
uniti
es, a
nd im
-pr
ove
train
ing
for s
taff
and
thei
r allo
ca-
tion
to e
nsur
e th
e ap
prop
riate
ski
lls m
ix.
(Mar
ch) (
61)
The
2002
IFC
Heal
th S
trate
gy is
pres
ente
d to
the
Boar
d of
Dire
ctor
s.
Regi
onal
AID
S st
rate
gy fo
r ECA
pub
lishe
d:Av
ertin
g AI
DS C
rises
in E
aste
rn E
urop
ean
d Ce
ntra
l Asia
(Sep
tem
ber)
(64*
)
The
Glob
al/H
IV A
IDS
prog
ram
is c
reat
edal
ong
with
the
Glob
al M
onito
ring
and
Eval
uatio
n Te
am (G
AMET
). GA
MET
isho
used
at t
he W
orld
Ban
k an
d su
ppor
tsef
forts
with
UN
AIDS
to b
uild
cou
ntry
-le
vel m
onito
ring
and
eval
uatio
n ca
paci
ties
as w
ell a
s co
ordi
nate
tech
nica
l sup
port.
(Jun
e) (2
1)
Firs
t pha
se o
f Ban
k-N
ethe
rland
s W
ater
Partn
ersh
ip-W
ater
Sup
ply
and
Sani
tatio
nin
itiat
ed. (
51)
Glob
al A
llian
ce fo
r Im
prov
ed N
utrit
ion
(GAI
N) c
reat
ed a
t a s
peci
al U
N s
essi
onfo
r chi
ldre
n. T
he W
orld
Ban
k is
a k
eypa
rtner
, mai
nly
man
agin
g tru
st fu
nds
and
prog
ram
impl
emen
tatio
n. (6
2)
The
Bank
and
the
Pan-
Amer
ican
Hea
lthOr
gani
zatio
n (P
AHO)
inau
gura
te th
e“H
ealth
Par
tner
ship
for K
now
ledg
e Sh
ar-
ing
and
Lear
ning
in th
e Am
eric
as.”
The
initi
ativ
e pr
omot
es th
e us
e of
tech
nolo
gyto
sha
re e
xper
tise
in o
rder
to m
eet t
heM
DGs
acro
ss th
e re
gion
. (Oc
tobe
r) (1
)

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 1 7
2004
Wat
er R
esou
rces
Sec
tor S
trate
gy: S
trate
-gi
c Dire
ctio
ns fo
r Wor
ld B
ank E
ngag
e-m
ent i
s pu
blis
hed.
The
stra
tegy
hig
hlig
hts
the
cent
ralit
y of
wat
er re
sour
ce m
anag
e-m
ent a
nd d
evel
opm
ent t
o su
stai
nabl
egr
owth
and
pov
erty
redu
ctio
n. It
arg
ues
that
the
Wor
ld B
ank
is p
erce
ived
to h
ave
aco
mpa
rativ
e ad
vant
age
in th
e ar
ea. I
t em
-ph
asize
s th
e ne
ed to
tailo
r Cou
ntry
Wat
erAs
sist
ance
Stra
tegi
es to
be
cons
iste
ntw
ith c
ount
ry c
onte
xt, C
ASs,
and
Pov
erty
Redu
ctio
n Su
ppor
t Pap
ers.
(Jan
uary
) (65
)
Reac
hing
the
Poor
Pro
gram
spo
nsor
sgl
obal
con
fere
nce
for r
esea
rche
rs to
diss
emin
ate
evid
ence
of h
ow w
ell h
ealth
and
othe
r soc
ial p
rogr
ams
reac
h th
e po
oran
d to
pro
duce
pol
icy
guid
elin
es b
ased
upon
the
evid
ence
. (Fe
brua
ry) (
66)
The
Bank
spo
nsor
s an
eve
nt fo
r 35
Afric
anam
bass
ador
s, H
arm
onizi
ng A
ppro
ache
s to
Heal
th in
Afri
ca, t
o in
tens
ify e
fforts
toim
prov
e w
omen
’s he
alth
in A
frica
and
plan
follo
w-u
p ac
tiviti
es. (
April
) (1)
IEG
rele
ases
an
eval
uatio
n of
the
Bank
’sap
proa
ch to
glo
bal p
rogr
ams,
Add
ress
ing
the
Chal
leng
es o
f Glo
baliz
atio
n . T
he e
val-
uatio
n re
com
men
ds th
at th
e Ba
nk s
epa-
rate
ove
rsig
ht o
f glo
bal p
rogr
ams
from
man
agem
ent,
impr
ove
stan
dard
s of
gov
-er
nanc
e an
d m
anag
emen
t of i
ndiv
idua
lpr
ogra
ms,
reev
alua
te s
elec
tion
and
exit
crite
ria, s
treng
then
link
s be
twee
n gl
obal
prog
ram
s an
d co
untry
stra
tegi
es, a
ndst
reng
then
eva
luat
ions
and
revi
ew o
fgl
obal
pro
gram
s w
ithin
the
Bank
. (67
*)
WDR
200
4: M
akin
g Se
rvice
s Wor
k for
Poor
Peo
ple
iden
tifie
s go
od g
over
nanc
ean
d ac
coun
tabi
lity
mec
hani
sms
as k
eyde
term
inan
ts o
f hea
lth s
yste
mpe
rform
ance
. (68
*)
Regi
onal
HIV
/AID
S st
rate
gy fo
r Eas
t As
ia a
nd P
acifi
c pu
blis
hed
Addr
essin
gHI
V/AI
DS in
Eas
t Asia
and
the
Pacif
ic .(J
anua
ry) (
69*)
Impr
ovin
g He
alth
, Nut
ritio
n, a
nd P
opul
a-tio
n Ou
tcom
es in
Sub
-Sah
aran
Afri
ca-—
The
Role
of t
he W
orld
Ban
k not
es th
atpo
sitiv
e tre
nds
in h
ealth
indi
cato
rs h
ave
slow
ed o
r rev
erse
d in
Sub
-Sah
aran
Afri
ca.
It ar
gues
that
the
Bank
mus
t use
its
com
-pa
rativ
e ad
vant
age
to w
ork
with
gov
ern-
men
ts a
nd p
artn
ers
to s
treng
then
the
capa
city
of c
ount
ries
to im
prov
e he
alth
outc
omes
. Nut
ritio
n an
d po
pula
tion
mus
tre
mai
n ce
ntra
l iss
ues
in d
evel
opm
ent i
nSu
b-Sa
hara
n Af
rica
and
acco
rdin
gly,
the
repo
rt pr
esen
ts a
regi
onal
gui
de to
sha
pest
rate
gy fo
rmul
atio
n at
the
coun
try o
r sub
-re
gion
al le
vel.
(Dec
embe
r) (7
0*)
IFC
clar
ifies
five
stra
tegi
c pr
iorit
ies,
of
whi
ch h
ealth
and
edu
catio
n ar
e on
e. (8
a)
WHO
and
the
Bank
cos
pons
or th
e Fi
rst
High
-Lev
el F
orum
on
the
Heal
th M
DGs.
Head
s of
dev
elop
men
t age
ncie
s, b
ilate
ral
agen
cies
, glo
bal h
ealth
initi
ativ
es, a
ndhe
alth
and
fina
nce
min
iste
rs a
gree
on
four
act
ion
area
s: re
sour
ces
for h
ealth
and
pove
rty re
duct
ion
pape
rs; a
idef
fect
iven
ess
and
harm
oniza
tion;
hum
anre
sour
ces;
mon
itorin
g pe
rform
ance
.(J
anua
ry) (
1)
(Tabl
e co
ntin
ues n
ext p
age)

1 1 8
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
2005
Paul
Wol
fow
itz is
app
rove
d by
the
Boar
dof
Exe
cutiv
e Di
rect
ors
as th
e W
orld
Bank
’s 10
th P
resi
dent
. (M
arch
) (1)
In h
is s
peec
h at
the
Annu
al M
eetin
gs,
Wol
fow
itz e
mph
asize
s th
e im
porta
nce
ofle
ader
ship
and
acc
ount
abili
ty, c
ivil
soci
ety
and
wom
en, a
nd th
e ru
le o
f law
as w
ell a
s fo
cusi
ng o
n re
sults
. Whe
nsp
eaki
ng o
n th
e im
porta
nce
of h
ealth
on
the
deve
lopm
ent a
gend
a, h
e em
phas
izes
the
Wor
ld B
ank’s
com
mitm
ent t
o fig
htm
alar
ia w
ith th
e sa
me
inte
nsity
as
HIV/
AIDS
. (Se
ptem
ber)
(71)
An IE
G ev
alua
tion
of th
e Ba
nk’s
HIV/
AIDS
Assis
tanc
e, C
omm
ittin
g to
Res
ults
:Im
prov
ing
the
Effe
ctive
ness
of H
IV/A
IDS
Assis
tanc
e , is
rele
ased
. It f
inds
that
the
Bank
’s su
ppor
t has
raise
d co
mm
itmen
t and
acce
ss to
serv
ices,
but t
he e
ffect
on
the
spre
ad o
f HIV
and
surv
ival i
s unc
lear
. It
reco
mm
ends
that
the
Bank
: hel
p go
vern
-m
ents
to b
e st
rate
gic a
nd se
lect
ive, a
ndpr
iorit
ize h
igh-
impa
ct a
ctivi
ties a
nd th
ehi
ghes
t-risk
beh
avio
rs; s
treng
then
nat
iona
lin
stitu
tions
to m
anag
e an
d im
plem
ent
long
-run
resp
onse
s; an
d im
prov
e m
onito
r-in
g an
d ev
alua
tion
to st
reng
then
the
loca
lev
iden
ce b
ase
for d
ecisi
on m
akin
g. (2
1*)
Whe
n th
e Ad
vise
r for
Pop
ulat
ion
and
Repr
oduc
tive,
Mat
erna
l and
Chi
ld H
ealth
(Eliz
abet
h Lu
le) i
s ap
poin
ted
as m
anag
erof
ACT
Afric
a, th
e Ad
vise
r pos
ition
isel
imin
ated
. (Ja
nuar
y) (7
2)
The
Life
Sci
ence
s Gr
oup
is e
stab
lishe
dw
ithin
IFC’
s Gl
obal
Man
ufac
turin
gDe
partm
ent.
Rolli
ng B
ack M
alar
ia: T
he W
orld
Ban
kGl
obal
Stra
tegy
and
Boo
ster
Pro
gram
prov
ides
the
basi
s an
d ra
tiona
le fo
rin
itiat
ing
the
five-
year
Boo
ster
Pro
gram
for M
alar
ia C
ontro
l. Its
obj
ectiv
es a
re to
incr
ease
cov
erag
e, im
prov
e ou
tcom
es,
and
build
cap
acity
. Des
crib
ed a
s a
“new
busi
ness
mod
el,”
it p
riorit
izes
flexi
ble,
coun
try-d
riven
, and
resu
lts-fo
cuse
dap
proa
ches
. (Ja
nuar
y) (4
1*)
Wor
ld B
ank
partn
ers
laun
ch th
e He
alth
Met
rics
Net
wor
k, a
glo
bal p
artn
ersh
ip to
impr
ove
the
qual
ity, a
vaila
bilit
y, an
ddi
ssem
inat
ion
of d
ata
for d
ecis
ion
mak
ing
in h
ealth
. (Ju
ne) (
73)

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 1 9
2006
2007
Task
For
ce o
n Av
ian
Flu
for A
frica
esta
blis
hed
to m
anag
e th
e in
form
atio
n,co
mm
unic
atio
n, a
nd c
oord
inat
ion
aspe
cts
of th
e re
spon
se to
avi
an in
fluen
za. I
tsu
ppor
ts c
ount
ry te
ams
to p
repa
rein
divi
dual
cou
ntry
ope
ratio
ns; h
elps
coor
dina
te th
e re
gion
’s re
spon
se w
ith th
egl
obal
and
Ban
k-w
ide
fund
ing
prog
ram
s,w
ith d
onor
s, a
nd m
obili
ze a
dditi
onal
fund
ing
as n
eces
sary
. (74
)
Paul
Wol
fow
itz re
sign
s as
Wor
ld B
ank
Pres
iden
t. (J
une)
(79)
Robe
rt Zo
ellic
k be
com
es 1
1th
Wor
ld B
ank
Pres
iden
t. (J
uly)
(80)
Cris
tian
Baez
a ap
poin
ted
as A
ctin
g HN
PDi
rect
or (F
ebru
ary)
(75)
Joy
Phum
aphi
bec
omes
Vic
e Pr
esid
ent o
fth
e Hu
man
Dev
elop
men
t Net
wor
k.(F
ebru
ary)
(81)
Julia
n Sc
hwei
tzer
bec
omes
HN
P Se
ctor
Dire
ctor
. (Oc
tobe
r) (8
2)
IFC
Agai
nst A
IDS
is in
tegr
ated
into
the
Smal
l and
Med
ium
Ent
erpr
ises
Depa
rtmen
t.
Repo
sitio
ning
Nut
ritio
n as
Cen
tral t
o De
-ve
lopm
ent:
A St
rate
gy fo
r Lar
ge-S
cale
Ac-
tion
aim
s to
pos
ition
nut
ritio
n as
a p
riorit
yon
the
deve
lopm
ent a
gend
a at
bot
h th
eco
untry
and
inte
rnat
iona
l lev
els
to b
olst
erin
crea
sed
com
mitm
ents
and
inve
stm
ent t
ofig
ht m
alnu
tritio
n. It
prio
ritize
s: a
p-pr
oach
es th
at re
ach
the
poor
and
mos
tvu
lner
able
at s
trate
gic
stag
es in
thei
r de-
velo
pmen
t; sc
alin
g-up
pro
ven
and
cost
-ef
fect
ive
prog
ram
s; re
orie
ntin
g in
effe
ctiv
epr
ogra
ms;
impr
ovin
g nu
tritio
n th
roug
h de
-lib
erat
e ac
tiviti
es in
oth
er s
ecto
rs; s
up-
porti
ng a
ctio
n re
sear
ch a
nd le
arni
ng b
ydo
ing;
and
mai
nstre
amin
g nu
tritio
n in
tode
velo
pmen
t stra
tegi
es. (
Janu
ary)
(76*
)
Heal
th Fi
nanc
ing
Revis
ited:
A P
ract
i-tio
ner’s
Gui
de re
view
s th
e po
licy
optio
nsan
d to
ols
avai
labl
e fo
r hea
lth fi
nanc
e in
low
- and
mid
dle-
inco
me
coun
tries
. Key
prio
ritie
s in
clud
e: (i
) mob
ilizin
g in
crea
sed
and
sust
aina
ble
gove
rnm
ent h
ealth
spen
ding
; (ii)
impr
ovin
g go
vern
ance
and
regu
latio
n to
stre
ngth
en th
e ca
paci
ty o
fhe
alth
sys
tem
s an
d en
sure
that
inve
st-
men
ts a
re e
quita
ble
and
effic
ient
; and
(iii)
coor
dina
ting
dono
rs to
mak
e m
ore
flexi
-bl
e an
d lo
nger
-term
com
mitm
ents
that
are
alig
ned
with
the
deve
lopm
ent g
oals
of a
cou
ntry
. (M
ay) (
77*)
The
obje
ctiv
e of
the
2007
Wor
ld B
ank
Stra
tegy
for H
ealth
, Nut
ritio
n, a
ndPo
pula
tion
Resu
lts is
to u
se a
sel
ectiv
ean
d di
scip
lined
fram
ewor
k to
redo
uble
effo
rts to
sup
port
clie
nt c
ount
ries
to:
impr
ove
HNP
outc
omes
, esp
ecia
lly fo
r the
poor
; pro
tect
hou
seho
lds
from
illn
ess;
ensu
re s
usta
inab
le fi
nanc
ing;
and
impr
ove
sect
or g
over
nanc
e an
d re
duce
corru
ptio
n. (A
pril)
(63*
)
Wor
ld B
ank
cosp
onso
rs th
e In
tern
atio
nal
Pled
ging
Con
fere
nce
on A
vian
and
Hum
anIn
fluen
za in
Bei
jing
to a
sses
s fin
anci
ngne
eds
at c
ount
ry, r
egio
nal a
nd g
loba
lle
vels
. (Ja
nuar
y) (7
4)
Wor
ld B
ank
join
s th
e In
tern
atio
nal M
one-
tary
Fun
d an
d th
e Af
rican
Dev
elop
men
tBa
nk in
impl
emen
ting
the
Mul
tilat
eral
Debt
Rel
ief I
nitia
tive
(MDR
I), fo
rgiv
ing
100
perc
ent o
f elig
ible
out
stan
ding
deb
tow
ed to
thes
e th
ree
inst
itutio
ns b
y al
lco
untri
es re
achi
ng th
e co
mpl
etio
n po
int
of th
e HI
PC In
itiat
ive.
The
MDR
I will
ef-
fect
ivel
y do
uble
the
volu
me
of d
ebt r
elie
fal
read
y ex
pect
ed fr
om th
e en
hanc
ed H
IPC
Initi
ativ
e. (7
8)
Wor
ld B
ank
sign
s ag
reem
ent t
o jo
in th
eIn
tern
atio
nal H
ealth
Par
tner
ship
. The
Partn
ersh
ip a
ims
to im
prov
e th
e w
ork
ofdo
nor a
nd d
evel
opin
g co
untri
es a
ndin
tern
atio
nal a
genc
ies
to c
reat
e an
dim
plem
ent p
lans
and
ser
vice
s th
atim
prov
e he
alth
out
com
es fo
r the
poo
r.(S
epte
mbe
r) (8
4) (Ta
ble
cont
inue
s nex
t pag
e)
1 2 0
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
A:
Wo
rld
Ban
k G
rou
p H
NP
Tim
elin
e(c
ontin
ued)
Year
Wor
ld B
ank
grou
p ev
ents
HN
Pse
ctor
eve
nts
HN
P pu
blic
atio
ns a
nd s
trat
egie
sH
NP
part
ners
hips
and
com
mitm
ents
Popu
latio
n Iss
ues i
n th
e 21
st C
entu
ry:
The
Role
of t
he W
orld
Ban
k foc
uses
on
leve
ls a
nd tr
ends
in b
irths
, dea
ths,
mig
ratio
n an
d po
pula
tion
grow
th, a
ndre
late
d ch
alle
nges
. Afte
r ana
lyzin
g gl
obal
and
regi
onal
tren
ds, a
s w
ell a
s th
ose
for
lend
ing
for p
opul
atio
n, th
e re
port
outli
nes
the
Bank
’s ar
eas
of c
ompa
rativ
e ad
van-
tage
. It c
oncl
udes
that
the
Bank
mus
tfo
cus
anal
ytic
al w
ork
on p
opul
atio
nis
sues
, and
col
labo
rate
with
the
priv
ate
sect
or a
nd g
loba
l par
tner
s to
dev
elop
and
mai
nstre
am m
ultis
ecto
ral p
opul
atio
npo
licie
s ap
prop
riate
for l
ow-,
mid
dle-
, and
high
-ferti
lity
coun
tries
. (Ap
ril) (
83*)
The
IFC
Afric
a He
alth
Stra
tegy
is p
re-
sent
ed to
the
Boar
d of
Dire
ctor
s. (9
a)
Sour
ces:
The
Wor
ld B
ank p
art o
f thi
s tim
elin
e w
as co
mpi
led
by M
ollie
Fair,
and
isex
tract
ed fr
om a
ppen
dix
C of
“Fr
om P
opul
atio
n Le
ndin
g to
HN
P Re
sults
: The
Evo
-lu
tion
of th
e W
orld
Ban
k’s S
trate
gies
in H
ealth
, Nut
ritio
n, a
nd P
opul
atio
n,” I
EG W
ork-
ing
Pape
r, no
. 200
8/3,
Feb
ruar
y 20
08.
1.W
orld
Ban
k Gr
oup
Arch
ives
200
5.2.
Wor
ld B
ank
Web
site
. “W
ater
Sup
ply
and
Sani
tatio
n Pr
ojec
ts th
e Ba
nk’s
Ex-
perie
nce:
196
7–19
89.”
(http
://go
.wor
ldba
nk.o
rg/8
LRM
SA15
20)
3.Ki
ng 2
007.
4.W
orld
Ban
k Gr
oup
Arch
ives
, “Se
ctor
Dep
artm
ent C
hart.
”5.
Wor
ld B
ank
1972
a.6.
Wor
ld B
ank
1972
b.7.
Golla
day
and
Lies
e 19
80.
8.W
orld
Ban
k 19
73.
9.W
orld
Ban
k 19
74.
10.
Wor
ld B
ank
1975
.11
.Un
ited
Nat
ions
Sys
tem
Web
site
. “St
andi
ng C
omm
ittee
on
Nut
ritio
n.”
(http
://w
ww
.uns
yste
m.o
rg/S
CN/P
ublic
atio
ns/h
tml/m
anda
te.h
tml).
12
.W
orld
Ban
k Gr
oup
Arch
ives
, Wor
ld B
ank
Grou
p St
aff D
irect
orie
s.13
.W
orld
Ban
k 19
80b.
14.
Wor
ld B
ank
1980
a.15
.W
orld
Ban
k 19
97b.
16.
Wor
ld B
ank
1984
.17
.Gr
osh
and
Muñ
oz 1
996.
18.
Harv
ard
Scho
ol o
f Pu
blic
Hea
lth W
eb s
ite. (
http
://w
ww
.hsp
h.ha
rvar
d.ed
u/re
view
/fel
low
.sht
ml).
19.
Kapu
r and
oth
ers
1997
.20
.W
orld
Ban
k 19
86b.
21.
IEG
2005
a.22
.W
orld
Ban
k 19
86a.
23.
Wor
ld B
ank
1988
.24
.N
assi
m 1
991.
25.
Wor
ld B
ank
1989
.26
.Pe
ople
and
Pla
net.
Net
Web
site
. (h
ttp://
ww
w.p
eopl
eand
plan
et.n
et/
doc.
php?
id=1
740)
.27
.W
orld
Ban
k 19
93c.
28.
Jam
ison
and
oth
ers
1993
.29
.W
orld
Ban
k. 1
993b
. 30
.W
orld
Ban
k 19
94a.
31.
Wor
ld B
ank
1999
c.32
.Va
illan
cour
t 200
9.33
.W
orld
Ban
k Gr
oup
Arch
ives
. “Ja
mes
D. W
olfe
nsoh
n Ti
mel
ine
of M
ajor
Deve
lopm
ents
.”
34.
Wor
ld B
ank
Web
site
. “Qu
ality
Ass
uran
ce G
roup
.” (h
ttp://
web
.wor
ldba
nk.
org/
WBS
ITE/
EXTE
RNAL
/PRO
JECT
S/QA
G/0,
,con
tent
MDK
:200
6712
6~m
enu
PK:1
1486
5~pa
gePK
:109
617~
piPK
:109
636~
theS
itePK
:109
609,
00.h
tml).
35
.IA
VI W
eb S
ite (h
ttp://
ww
w.ia
vi.o
rg/v
iew
page
.cfm
?aid
=24)
.36
.Sc
hieb
er 1
997.
37.
Wor
ld B
ank
1997
a.38
.UN
ECA,
UN
ICEF
, and
Wor
ld B
ank.
199
8.
39.
Wor
ld B
ank
1998
a.40
.W
hite
, Mer
rick,
and
Yaz
beck
200
6.41
.W
orld
Ban
k 20
05b.
42.
Nar
ayan
and
Pet
esch
200
2.43
.W
agst
aff a
nd C
laes
on 2
004.
44.
IEG
1999
.
45.
Wor
ld B
ank
1999
a.46
.W
alt a
nd B
use
2006
.47
.W
orld
Ban
k 20
00b.
48.
Jha
and
Chal
oupk
a 20
00.
49.
Wor
ld B
ank
2000
a.50
.Gw
atki
n an
d ot
hers
200
0.51
.Ba
nk-N
ethe
rland
s W
ater
Par
tner
ship
Pro
gram
Web
site
(http
://w
ww
-esd
.w
orld
bank
.org
/bnw
pp/).
52.
Wor
ld B
ank
2001
c.53
.W
SP W
eb s
ite (h
ttp://
ww
w.w
sp.o
rg).
54.
Wor
ld B
ank
Web
site
. “Ge
nder
and
Dev
elop
men
t.” (h
ttp://
web
.wor
ldba
nk.
org/
WBS
ITE/
EXTE
RNAL
/TOP
ICS/
EXTG
ENDE
R/0,
,men
uPK:
3368
74~p
ageP
K:14
9018
~piP
K:14
9093
~the
Site
PK:3
3686
8,00
.htm
l).55
.W
orld
Ban
k 20
01a.
56.
Stop
TB
Partn
ersh
ip W
eb s
ite (h
ttp://
ww
w.s
topt
b.or
g/st
op_t
b_in
itiat
ive/
).57
.Gl
obal
Pub
lic-P
rivat
e Pa
rtner
ship
for H
andw
ashi
ng w
ith S
oap
Web
site
(http
://w
ww
.glo
balh
andw
ashi
ng.o
rg/).
58.
Kais
er F
amily
Fou
ndat
ion
Web
site
(ww
w.k
ff.or
g/hi
vaid
s/tim
elin
e).
59.
INDE
PTH
Web
site
(http
://w
ww
.inde
pth-
netw
ork.
org/
core
_doc
umen
ts/
visi
on.h
tm).
60.
Wor
ld B
ank
Web
site
. “St
rate
gies
.” (h
ttp://
intra
net.w
orld
bank
.org
/WBS
ITE/
INTR
ANET
/SEC
TORS
/HEA
LTHN
UTRI
TION
ANDP
OPUL
ATIO
N/IN
THIV
AIDS
/0,
,con
tent
MDK
:201
2070
2~m
enuP
K:37
5837
~pag
ePK:
2100
82~p
iPK:
2100
98~
theS
itePK
:375
799,
00.h
tml).
61.
HNP
Sect
or B
oard
. (dr
aft,
Feb
ruar
y 7,
200
2). “
Heal
th, N
utrit
ion
and
Popu
la-
tion
Sect
or S
trate
gy B
riefin
g.”
62.
GAIN
Web
site
(ht
tp://
ww
w.g
ainh
ealth
.org
/gai
n/ch
/en-
en/in
dex.
cfm
?pa
ge=/
gain
/hom
e/ab
out_
gain
/his
tory
).

APPENDIX A: WORLD BANK GROUP HNP TIMELINE
1 2 1
63.
Wor
ld B
ank
2007
a.64
.W
orld
Ban
k 20
03b.
65.
Wor
ld B
ank
2004
d.66
.W
orld
Ban
k Web
site
. (http
://w
eb.w
orld
bank
.org
/WBS
ITE/
EXTE
RNAL
/TOP
ICS/
EXTH
EALT
HNUT
RITI
ONAN
DPOP
ULAT
ION/
EXTP
AH/0
,,con
tent
MDK
:207
4433
4~pa
gePK
:210
058~
piPK
:210
062~
theS
itePK
:400
476,
00.h
tml?
).67
.IE
G 20
04a.
68.
Wor
ld B
ank
2003
b.69
.W
orld
Ban
k 20
04a.
70.
Wor
ld B
ank
2004
c.71
.W
orld
Ban
k W
eb s
ite. N
ews
and
Broa
dcas
t. “A
nnua
l Mee
tings
200
5 Op
en-
ing
Pres
s Co
nfer
ence
with
Pau
l Wol
fow
itz.”
(http
://w
eb.w
orld
bank
.org
/W
BSIT
E/ E
XTER
NAL
/NEW
S/0,
,con
tent
MDK
:206
5690
3~pa
gePK
:642
5704
3~pi
PK:4
3737
6~th
eSite
PK:4
607,
00.h
tml).
72.
Wor
ld B
ank
Web
site
. “N
ews
and
Broa
dcas
ts>“
http
://w
eb.w
orld
bank
.org
/W
BSIT
E/EX
TERN
AL/N
EWS/
0,,c
onte
ntM
DK:2
0138
122~
page
PK:6
4257
043~
piPK
:437
376~
theS
itePK
:460
7,00
.htm
l73
.W
HO W
eb si
te. “
Wha
t is H
MN
?” (h
ttp://
ww
w.w
ho.in
t/he
alth
met
rics/
abou
t/w
hatis
hmn/
en/in
dex.
htm
l).74
.W
orld
Ban
k W
eb s
ite. “
Avia
n an
d Pa
ndem
ic In
fluen
za.”
(http
://w
eb.w
orld
bank
.org
/WBS
ITE/
EXTE
RNA
L/TO
PICS
/EXT
HEA
LTH
NU
TRIT
ION
AN
D
POPU
LATI
ON/E
XTTO
PAVI
FLU/
0,,m
enuP
K:17
9360
5~pa
gePK
:641
6842
7~pi
PK:6
416
8435
~the
Site
PK:1
7935
93,0
0.ht
ml).
75.
Wor
ld B
ank
Web
site
. “Ac
ting
Assi
gnm
ents
in H
NP.”
(http
://in
trane
t.wor
ldba
nk.o
rg/W
BSIT
E/IN
TRAN
ET/S
ECTO
RS/H
EALT
HNUT
RITI
ONAN
DPOP
ULAT
ION/
0,,c
onte
ntM
DK:
2013
1131
~pag
ePK:
2100
82~p
iPK:
2100
98~t
heSi
tePK
:28
1628
,00.
htm
l) 76
.W
orld
Ban
k 20
06c.
77.
Gottr
et a
nd S
chie
ber 2
006.
78.
Wor
ld B
ank
Web
site
. “De
bt is
sues
.” (h
ttp://
web
.wor
ldba
nk.o
rg/W
BSIT
E/EX
TERN
AL/T
OPIC
S/EX
TDEB
TDEP
T/0,
,men
uPK:
6416
6739
~pag
ePK:
6416
6681
~piP
K:64
1667
25~t
heSi
tePK
:469
043,
00.h
tml).
79.
Wor
ld B
ank
Web
site
. “St
atem
ents
of
Exec
utiv
e Di
rect
or a
nd P
resi
dent
Wol
fow
itz.”
(http
://in
trane
t.wor
ldba
nk.o
rg/W
BSIT
E/IN
TRAN
ET/U
NIT
S/IN
TPR
ESID
ENT2
007/
INTP
ASTP
RESI
DEN
TS/IN
TPRE
SIDE
NTS
TAFC
ONN
/0,,c
onte
ntM
DK:2
1339
650~
men
uPK:
6432
4835
~pag
ePK:
6425
9040
~piP
K:64
2588
64~
theS
itePK
:101
4519
,00.
htm
l).80
.W
orld
Ban
k W
eb s
ite. “
Pres
iden
t’s S
taff
Conn
ectio
n.”
http
://in
trane
t.wor
ldba
nk.o
rg/W
BSIT
E/IN
TRAN
ET/U
NIT
S/IN
TPRE
SIDE
NT2
007/
0,,c
onte
ntM
DK:
2147
7815
~men
uPK:
6482
1535
~pag
ePK:
6482
1348
~piP
K:64
8213
41~t
heSi
tePK
:39
1504
5,00
.htm
l81
.W
orld
Ban
k Web
site
. Jan
uary
30,
200
7. “I
nter
view
with
Joy
Phu
map
hi, N
ewHD
Vic
e Pr
esid
ent.”
(http
://in
trane
t.wor
ldba
nk.o
rg/W
BSIT
E/IN
TRAN
ET/
UNIT
S/IN
THDN
ETW
ORK/
0,,co
nten
tMDK
:211
9908
7~m
enuP
K:51
4396
~pag
ePK:
6415
6298
~piP
K:64
1522
76~t
heSi
tePK
:514
373,
00.h
tml).
82.
Wor
ld B
ank W
eb si
te. “
Julia
n Sc
hwei
tzer
, Sec
tor D
irect
or, H
NP,
Hum
an D
evel
-op
men
t Net
wor
k.” h
ttp://
intra
net.w
orld
bank
.org
/WBS
ITE/
INTR
ANET
/ KIO
SK/
0,,co
nten
tMDK
:214
7306
3~m
enuP
K:34
897~
page
PK:3
7626
~piP
K:37
631~
theS
itePK
:366
4,00
.htm
l83
.W
orld
Ban
k 20
07g.
84.
Depa
rtmen
t for
Inte
rnat
iona
l Dev
elop
men
t Web
Site
. “In
tern
atio
nal H
ealth
Par
t-ne
rshi
p la
unch
ed to
day.”
(http
://w
ww
.dfid
.gov
.uk/
new
s/fil
es/ih
p/ d
efau
lt.as
p).
1aIF
C 19
82.
2aIF
C 20
02, p
. 24.
3aIF
C 19
98.
4aIF
C 20
02, p
. 24.
5aIF
C 19
99.
6aLu
talo
200
6.7a
IFC
2002
, p. 2
4.8a
IFC
2004
.9a
IFC
2007
a.No
te:*
indi
cate
s th
e pu
blic
atio
n its
elf,
othe
rwis
e, fa
cts
are
repo
rted
in th
e ci
ted
refe
renc
e.

A show of hands among Nepalese children who wash their hands after using their new latrine. Photo courtesy of George T. Keith Pitman.

1 2 3
World Bank HNP Project Portfolio
ProjectsThe review of the portfolio managed by the HNP
sector that is presented in chapters 2–4 included
all 220 active and closed projects approved from
fiscal 1997 to 2006 (table B.1). The 220 projects
are listed in appendix C. Approvals of supple-
mental allocations for active projects are attributed
to the original project; they are not considered
separate operations. The count of projects in
other sectors with HNP components included
any project with HNP commitments, as defined
below.
HNP CommitmentsUp to five sector codes are assigned to every
World Bank lending operation, and the percent-
age of the loan to be dedicated to each sector code
was noted in the project design documents. HNP
commitments include the amounts committed
under sector codes JA (health), BK (compulsory
health finance), FB (noncompulsory health fi-
nance) and other historic codes used for the
health sector (HB, HC, HE, HH, HP, HR, HT, HY).
Total commitments to HNP were calculated by tak-
ing the total amount of each project allocated to
these codes.1 Because there is often more than
one sector code, even for HNP-managed proj-
ects, it means that less than 100 percent of the cost
of a loan or credit is actually being counted. Note,
too, that for multisectoral Development Policy
Loans that are essentially direct budget support
to the government, the allocation across sector
codes is entirely notional and does not reflect
earmarked funds for any sector.
World Bank Water Supply and SanitationProject PortfolioThe water supply and sanitation projects reviewed
in chapter 4 include all 117 active and closed proj-
ects approved from fiscal 1997 to 2006 (table B.2)
with financial commitments to sector codes WA
(sanitation), WC (water supply), WS (sewerage),
and WZ (general water, sanitation, and flood pro-
tection), and managed by the Water Supply and San-
itation Sector Board. Projects that are solely aimed
at flood protection (WD) and solid waste man-
agement (WB) are not included. Supplemental
credits and projects approved under emergency
APPENDIX B: DEFINITION OF THE SAMPLES USED FOR PORTFOLIO REVIEWS AND WORLD BANK HNP STAFF ANALYSIS
Table B.1: Projects Managed by the HNP Sector by Fiscal Year of Approval andProject Status
Fiscal years
1997–2001 2002–06 1997–2006
Project status Projects Percent Projects Percent Projects Percent
Active 9 9 101 83 110 50
Closed 90 91 20 17 110a 50
Total 99 100 121 100 220 100a. Of these, 99 had been reviewed and rated by IEG as of September 30, 2008. In addition, 2 projects were cancelled before they were implemented and thusdid not receive an outcome rating.

1 2 4
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
procedures were also excluded. Greater detail and
the list of projects can be found in Overbey (2008).
World Bank Transport Project PortfolioThe transport projects reviewed in chapter 4 in-
clude all 229 active and closed projects approved
from fiscal 1997 to 2006 (table B.3). Only projects
managed by the Transport Sector Board and that
had financial commitments under the sector
codes TA (roads and highways), TP (ports, wa-
terways, and shipping), TV (aviation), TW (rail-
ways), and TZ (general transportation, which
includes urban transport) were included. Sup-
plemental credits and projects approved under
emergency procedures are excluded. Transport
projects managed by other sector boards were ex-
cluded because the resources needed to track
down the relatively small number of such projects
were not warranted.2 Thus, transport projects re-
lated to improvements of air quality that fell either
under the Environment Sector Board or were
funded through the Global Environment Facility
(GEF) have not been reviewed.
World Bank HNP StaffingThe analysis of HNP staffing in chapter 2 uses
four sets of data on World Bank staff in the HNP
sector provided by the Bank’s Human Resources
Department:
1. Master dataset of HNP staff. This is a mas-
ter dataset of all Bank staff at levels GF and
higher as of the end of every fiscal year (June
30), from fiscal 1997 to 2007, who were mapped
to the HNP sector. Staff members below level
GF are not systematically mapped to a sector,
so are excluded from the analysis. The datasets
included the following data for each individual:
fiscal year; UPI (staff identification) number; pri-
mary managing unit (PMU); unit of assignment;
entry on duty (EOD); appointment type; level;
job title; age; gender; whether Part I or II; years
in the Bank; years in the PMU; whether posted
at headquarters or in the field; duty country;
whether a coterminous appointment;3 pro-
gram name; whether a manager; and whether
a former Young Professional. The information
Table B.2: Water Supply and Sanitation Projects Included in the Portfolio Review
Fiscal years
1997–2001 2002–06 1997–2006
Project status Projects Percent Projects Percent Projects Percent
Active 33 53 55 100 88 75
Closeda 29 47 0 0 29 25
Total 62 100 55 100 117 100a. As of October 31, 2007. Implementation Completion Reports had not been received by IEG for 3 of the 29 projects at the time of the review, reducing to 26the number of completed projects reviewed.
Table B.3: Transport Projects Included in the Portfolio Review
Fiscal years
1997–2001 2002–06 1997–2006
Project status Projects Percent Projects Percent Projects Percent
Active 28 22 96 93 124 54
Closeda 98 78 7 7 105 46
Total 126 100 103 100 229 100a. As of June 25, 2007.

A P P E N D I X B : D E F I N I T I O N O F T H E S A M P L E S U S E D F O R P O R T F O L I O R E V I E W S A N D W O R L D B A N K H N P S TA F F A N A LY S I S
1 2 5
was provided separately for each fiscal year
and merged by IEG. This provided the basis for
a master panel dataset from which it is possi-
ble to track the movement of staff into and out
of the sector, using the UPI number as the
identifier.
2. Hub dataset. This is a dataset of all Bank staff
and consultants level GE and higher assigned
to the “hub” or “anchor,” for the period fiscal
1997–2007. The “hub” was defined as includ-
ing the units HDDHE and its successor HDNHE
(the HNP hub), and HDNGA (the central unit
for the AIDS program, established in 2004).
The data and variables assembled for hub staff
levels GF and higher are identical to those for
the master HNP staff dataset. However, this
dataset also includes staff at level GE and in
other categories, such as junior professional as-
sociates, junior professional officers, cotermi-
nous staff, and special assignments, who were
working in those units.
3. New hires. A dataset of all new hires of indi-
viduals directly into the World Bank HNP sec-
tor. The variables available included all of the
variables in the master HNP staff dataset, plus
the effective date of the hire.
4. Exits. A dataset of all terminations of individ-
uals from the World Bank who were mapped
to the HNP sector at the time that they left. This
includes, for example, resignations, retirements,
and deaths of HNP staff. The variables avail-
able for analysis included all of the variables
in the master HNP staff dataset, plus the effec-
tive date that of the hire and the reason for
termination.
Only a few corrections were made to the original
data for the analysis. First, the original data in-
cluded several individuals mapped to units in IFC
who were dropped. No other individuals were
dropped, though in a number of instances the unit
codes did not seem to pertain to health (for ex-
ample, the Board, Staff Association, External Af-
fairs, Commodity Risk Group). Second, in the
new hire and exit datasets there were often du-
plicates associated with conversions from one
type of assignment to another—for example, the
person appears as a new hire, then an exit, then
a new hire shortly thereafter in another assign-
ment type. In those instances, the first time that
the individual appears was used for the purposes
of counting the number of new hires and their age,
and in the exit dataset instances were excluded
of those who had been converted to a new as-
signment type. The last observation was used if
there was more than one appearance and the
person was no longer at the Bank (or at least no
longer in the HNP sector at the Bank).
Country Assistance StrategiesThe desk review of CASs included a sample of the
211 CASs approved from fiscal 1997 to 2006. In
light of the large number of countries in three Re-
gions, the study reviewed: (a) all CASs for East Asia,
the Middle East and North Africa, and South Asia;
and (b) a random sample consisting of roughly half
of all CASs for Europe and Central Asia, Latin
America and the Caribbean, and Africa (table B.4).
The results reported in chapters 2 and 4 have
been weighted to take the stratification of the
sample into account. A list of the CASs actually re-
viewed can be found in Sinha and Gaubatz 2009.
IFC Portfolio of Investment Projects and Advisory ServicesThe portfolio of 52 IFC health projects reviewed
in chapter 5 includes 35 active and 17 closed proj-
ects approved from fiscal 1997 to 2007 (appendix
D). Active projects are those for which IFC has fi-
nancial exposure; closed projects are those with
which IFC no longer has a financial relationship.
Health sector projects included those with the
health and pharmaceuticals sector code and ad-
ditional projects with business objectives related
to health (for example, a medical training project
with an education sector code). Dropped projects,
cancellations, rights issues, reschedulings, re-
structurings, supplementary investments made in
the context of previously approved projects, in-
vestments through the Africa Enterprise Fund
and Small Enterprise Fund, and individual in-
vestments under agency lines were excluded.4
Chapter 5 assesses the performance of IFC proj-
ects that reached “early operating maturity.”5 The
performance of mature projects was assessed
through either detailed Expanded Project Super-
vision Reports (XPSRs) prepared by the investment

1 2 6
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
departments and validated by IEG, or by IEG’s desk
review of project information for those not cov-
ered by an Expanded Project Supervision Report.
For projects that had not yet reached early oper-
ating maturity, IEG gathered information about
each project’s characteristics and design, as well
as information on implementation status in the su-
pervision reports. Field visits supplemented the
information gathered by the desk review. The ob-
jective of the field visits was to conduct in-depth
validation and interviews linked to ongoing and
completed investments and Advisory Services.
The five countries visited were selected to achieve
Regional balance, to have more than one current
or past IFC health investment, to include invest-
ments in different time periods, and to include dif-
ferent types of investments (for example, hospitals
and pharmaceuticals). During field visits, IFC
clients, government agency officials, health-
related professional and business associations,
relevant multilateral and/or bilateral development
organizations with private sector portfolios, and
other stakeholders were interviewed.
For Advisory Service projects, the monitoring and
evaluation system was still in a pilot phase. IEG
reviewed all health projects covered by the pre-
vious rounds of project completion report (PCR)
pilots, as well as desk review of approval and su-
pervision documents for projects not covered by
the PCR. Interviews were conducted with IFC
and World Bank managers, sector specialists, in-
vestment officers, and project task managers.
Table B.4: Country Assistance Strategies Issued in Fiscal Years 1997–2006, by Region and Year, and the IEG Sample for Review
ReviewedRegion 1997–2001 2002–06 Total sample
Sub-Saharan Africa 29 26 55 31
Europe and Central Asia 31 29 60 29
Latin America and the Caribbean 20 20 40 21
East Asia & Pacific 12 11 23 23
Middle East and North Africa 9 10 19 19
South Asia 7 7 14 14
Total 108 103 211 137

1 2 7
APPENDIX C: WORLD BANK HNP SECTOR PROJECTS APPROVED INFISCAL YEARS 1996–2007
Appendix C: World Bank HNP Sector Projects Approved in Fiscal Years 1996–2007
HNP commitment ($US millions)
Fiscal year Project Total Totalapproved ID Project name Country IBRD IDA HNP commitment
1997 P006059 Maternal and Child Health and Nutrition II Argentina 95.0 0.0 95.0 100.01997 P043418 AIDS and STD Control Argentina 11.9 0.0 11.9 15.01997 P044522 Essential Hospital Services Bosnia-Herzegovina 0.0 14.4 14.4 15.01997 P004034 Disease Control and Health Development Cambodia 0.0 27.7 27.7 30.41997 P010473 Tuberculosis Control India 0.0 129.6 129.6 142.41997 P010511 Malaria Control India 0.0 159.9 159.9 164.81997 P010531 Reproductive Health India 0.0 223.5 223.5 248.31997 P042540 Iodine Deficiency Control Indonesia 19.1 0.0 19.1 28.51997 P001999 Health Sector Development Program Niger 0.0 37.6 37.6 40.01997 P007927 Maternal Health/Child Development Paraguay 19.2 0.0 19.2 21.81997 P008814 Health Reform Pilot Russian Federation 66.0 0.0 66.0 66.01997 P041567 Endemic Disease Senegal 0.0 13.9 13.9 14.91997 P010526 Health Services Sri Lanka 0.0 17.5 17.5 18.81997 P009095 Primary Health Care Services Turkey 13.3 0.0 13.3 14.51998 P045312 Health Recovery Albania 0.0 13.9 13.9 17.01998 P050140 Health Armenia 0.0 8.4 8.4 10.01998 P037857 Health and Population Program Bangladesh 0.0 242.5 242.5 250.01998 P003566 Basic Health (Health VIII) China 0.0 78.2 78.2 85.01998 P052887 Health Comoros 0.0 6.7 6.7 8.41998 P007015 Provincial Health Services Dominican Republic 28.2 0.0 28.2 30.01998 P039084 Health Services Modernization Ecuador 40.5 0.0 40.5 45.01998 P045175 Health Sector Egypt, Arab Rep. of 0.0 90.0 90.0 90.01998 P043124 Health Eritrea 0.0 17.2 17.2 18.31998 P000825 Participatory HNP Gambia 0.0 17.8 17.8 18.01998 P000949 Health Sector Support Ghana 0.0 33.6 33.6 35.01998 P035688 National Health Development Program Guinea-Bissau 0.0 10.8 10.8 11.71998 P010496 Orissa Health Systems India 0.0 69.5 69.5 76.41998 P049385 Economic Restructuring India 72.3 58.1 130.4 543.21998 P035827 Women and Child Development India 0.0 273.0 273.0 300.01998 P036956 Safe Motherhood Indonesia 41.2 0.0 41.2 42.5
(Table continues next page)

1 2 8
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Appendix C: World Bank HNP Sector Projects Approved in Fiscal Years 1996–2007 (continued)
HNP commitment($US millions)
Fiscal year Project Total Totalapproved ID Project name Country IBRD IDA HNP commitment
1998 P001568 Community Nutrition II Madagascar 0.0 19.3 19.3 27.61998 P035689 Health Sector Investment Program Mauritania 0.0 23.8 23.8 24.01998 P007720 Health System Reform - SAL Mexico 700.0 0.0 700.0 700.01998 P055061 Health System Reform TA Mexico 21.5 0.0 21.5 25.01998 P035753 Health Sector II Nicaragua 0.0 18.2 18.2 24.01998 P004566 Early Childhood Development Philippines 17.1 0.0 17.1 19.01998 P002369 Integrated Health Sector Development Senegal 0.0 42.0 42.0 50.01998 P005746 Health Sector Tunisia 48.5 0.0 48.5 50.01998 P040551 Nutrition and Early Childhood Development Uganda 0.0 22.1 22.1 34.0
SIL 1999 P060392 Health Reform-APL I Bolivia 0.0 20.5 20.5 25.01999 P044523 Basic Health Bosnia-Herzegovina 0.0 8.2 8.2 10.01999 P043874 Disease Surveillance - VIGISUS Brazil 94.0 0.0 94.0 100.01999 P054120 AIDS and STD Control II Brazil 165.0 0.0 165.0 165.01999 P036953 Health IX China 9.4 47.0 56.4 60.01999 P000756 Health Sector Development Ethiopia 0.0 99.0 99.0 100.01999 P052154 Structural Reform Support Georgia 0.0 8.3 8.3 16.51999 P041568 Population and Reproductive Health Guinea 0.0 9.9 9.9 11.31999 P045051 HIV/AIDS II India 0.0 183.4 183.4 191.01999 P050651 Maharashtra Health System India 0.0 123.3 123.3 134.01999 P003967 Health V Indonesia 38.0 0.0 38.0 44.71999 P039749 Health Sector Reform Jordan 34.0 0.0 34.0 35.01999 P046499 Health Restructuring Kazakhstan 39.5 0.0 39.5 42.51999 P058520 Health Latvia 10.8 0.0 10.8 12.01999 P036038 Population/Family Planning Malawi 0.0 5.0 5.0 5.01999 P040652 Health Sector Development Program Mali 0.0 40.0 40.0 40.0
(PRODESS)1999 P055003 Nutrition, Food Security and Social Mauritania 0.0 1.9 1.9 4.9
Mobilization LIL1999 P005525 Health Management Morocco 64.0 0.0 64.0 66.01999 P040179 Health Pilot Panama 2.2 0.0 2.2 4.31999 P009125 Health Uzbekistan 26.7 0.0 26.7 30.02000 P055482 Public Health Surveillance and Disease Control Argentina 50.4 0.0 50.4 52.52000 P063388 Health Insurance for the Uninsured Argentina 3.3 0.0 3.3 4.92000 P050751 National Nutrition Program Bangladesh 0.0 82.8 82.8 92.02000 P055157 Health Sector Reform Bulgaria 51.3 0.0 51.3 63.32000 P055122 Health Sector Support Chad 0.0 33.6 33.6 41.52000 P051273 Health System Croatia 27.3 0.0 27.3 29.02000 P067330 Immunization Strengthening India 0.0 129.8 129.8 142.62000 P050657 Health Systems Development India 0.0 95.7 95.7 110.0

A P P E N D I X C : W O R L D B A N K H N P S E C T O R P R O J E C T S , F I S C A L Y E A R S 1 9 9 6 – 2 0 0 7
1 2 9
Appendix C: World Bank HNP Sector Projects Approved in Fiscal Years 1996–2007 (continued)
HNP commitment($US millions)
Fiscal year Project Total Totalapproved ID Project name Country IBRD IDA HNP commitment
2000 P049545 Provincial Health I Indonesia 0.0 33.8 33.8 38.02000 P059477 Water and Sanitation for Low Income Indonesia 0.0 24.0 24.0 77.4
Communities II2000 P069943 Primary Health Care and Nutrition II Iran 82.7 0.0 82.7 87.02000 P053200 Health Sector Reform Lesotho 0.0 4.5 4.5 6.52000 P035780 Health Lithuania 18.7 0.0 18.7 21.22000 P051741 Health Sector Support II Madagascar 0.0 38.4 38.4 40.02000 P062932 Health Reform Program Peru 77.6 0.0 77.6 80.02000 P008797 Health Sector Reform Romania 37.6 0.0 37.6 40.02000 P051418 Health Sector Management Slovenia 5.9 0.0 5.9 9.52000 P058358 Health Sector Development Project Solomon Islands 0.0 3.5 3.5 4.02000 P049894 Primary Health Care Tajikistan 0.0 4.8 4.8 5.42000 P058627 Health Sector Development Program Tanzania 0.0 20.5 20.5 22.02001 P069293 Health Reform LIL Azerbaijan 0.0 4.0 4.0 5.02001 P069933 HIV/AIDS Prevention Bangladesh 0.0 39.2 39.2 40.02001 P075220 HIV/AIDS I Barbados 14.4 0.0 14.4 15.22001 P074212 Health Sector Reform APL II Bolivia 0.0 32.2 32.2 35.02001 P073065 Multisectoral HIV/AIDS Cameroon 0.0 20.0 20.0 50.02001 P071505 HIV/AIDS Prevention & Control Project Dominican Republic 21.8 0.0 21.8 25.02001 P065713 HIV/AIDS, Malaria, STD, and TB Control Eritrea 0.0 33.2 33.2 40.02001 P069886 MAP Ethiopia 0.0 47.8 47.8 59.72001 P060329 HIV/AIDS Rapid Response Gambia 0.0 11.0 11.0 15.02001 P071617 AIDS Response Project (GARFUND) Ghana 0.0 21.3 21.3 25.02001 P067543 Leprosy II India 0.0 27.3 27.3 30.02001 P049539 Provincial Health II Indonesia 58.8 37.2 96.0 103.22001 P070920 HIV/AIDS Disaster Response Kenya 0.0 31.5 31.5 50.02001 P066486 Decentralized Reproductive Health and Kenya 0.0 46.0 46.0 50.0
HIV/AIDS 2001 P051372 Health II Kyrgyz Republic 0.0 12.5 12.5 15.02001 P066321 Basic Health Care III Mexico 343.0 0.0 343.0 350.02001 P051174 Health Investment Fund Moldova 0.0 9.5 9.5 10.02001 P064926 Health Sector Management Samoa 0.0 3.9 3.9 5.02001 P072482 HIV/AIDS Control Uganda 0.0 36.6 36.6 47.52001 P050495 Caracas Metropolitan Health Venezuela, R. B. de 28.8 0.0 28.8 30.32002 P073118 Multisectoral HIV/AIDS Benin 0.0 13.6 13.6 23.02002 P057665 Family Health Extension Project I Brazil 64.6 0.0 64.6 68.02002 P071433 HIV/AIDS Disaster Response Burkina Faso 0.0 16.3 16.3 22.02002 P071371 Multisectoral HIV/AIDS Control and Orphans Burundi 0.0 10.8 10.8 36.02002 P073525 HIV/AIDS Central African Rep. 0.0 8.0 8.0 17.02002 P074249 HIV/AIDS Cape Verde 0.0 6.5 6.5 9.0
(Table continues next page)

1 3 0
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Appendix C: World Bank HNP Sector Projects Approved in Fiscal Years 1996–2007 (continued)
HNP commitment($US millions)
Fiscal year Project Total Totalapproved ID Project name Country IBRD IDA HNP commitment
2002 P072226 Population and AIDS II Chad 0.0 16.5 16.5 24.62002 P071147 Tuberculosis Control China 96.7 0.0 96.7 104.02002 P073892 Health Sector Strengthening and Modernization Costa Rica 16.2 0.0 16.2 17.02002 P071062 Health Sector Development Djibouti 0.0 15.0 15.0 15.02002 P067986 Earthquake Emergency Reconstruction and El Salvador 135.5 0.0 135.5 142.6
Health Services Extension2002 P053575 Health System Reform Honduras 0.0 26.6 26.6 27.12002 P074641 HIV/AIDS Prevention and Control II Jamaica 13.5 0.0 13.5 15.02002 P072987 Multisectoral STI/HIV/AIDS Prevention I Madagascar 0.0 15.4 15.4 20.02002 P070290 Health System Development II Nigeria 0.0 111.8 111.8 127.02002 P070291 HIV/AIDS Program Development Nigeria 0.0 82.2 82.2 90.32002 P069916 Social Expenditure Management II Philippines 20.0 0.0 20.0 100.02002 P074059 HIV/AIDS Prevention and Control Senegal 0.0 25.8 25.8 30.02002 P070541 Nutrition Enhancement Program Senegal 0.0 11.3 11.3 14.72002 P073883 HIV/AIDS Response Sierra Leone 0.0 13.1 13.1 15.02002 P073305 Regional Blood Transfusion Centers Vietnam 0.0 38.2 38.2 38.22002 P043254 Health Reform Support Yemen 0.0 25.1 25.1 27.52003 P078324 Health Sector Emergency Rehabilitation Afghanistan 0.0 53.0 53.0 59.62003 P071004 Social Insurance TA Bosnia-Herzegovina 0.0 4.6 4.6 7.02003 P080400 AIDS and STD Control III Brazil 100.0 0.0 100.0 100.02003 P054119 Bahia Development (Health) Brazil 9.0 0.0 9.0 30.02003 P070542 Health Sector Support Cambodia 0.0 24.3 24.3 27.02003 P073603 HIV/AIDS, Malaria and TB Control Djibouti 0.0 3.6 3.6 12.02003 P076802 Health Reform Support Dominican Republic 30.0 0.0 30.0 30.02003 P082395 First Programmatic Human Dev. Reform Ecuador 14.0 0.0 14.0 50.02003 P040555 Primary Health Care Development Georgia 0.0 17.3 17.3 20.32003 P073649 Health Sector Program Support II Ghana 0.0 89.6 89.6 89.62003 P076715 HIV/AIDS Prevention and Control II Grenada 1.5 1.5 3.0 6.02003 P073378 Multi-Sectoral AIDS Guinea 0.0 7.1 7.1 20.32003 P075056 Food and Drugs Capacity Building India 0.0 54.0 54.0 54.02003 P073772 Health Workforce and Services (PHP III) Indonesia 21.8 52.2 73.9 105.62003 P074122 AIDS Control Moldova 0.0 5.5 5.5 5.52003 P078053 HIV/AIDS Response Mozambique 0.0 22.0 22.0 55.02003 P071612 Multisectoral STI/HIV/AIDS II Niger 0.0 10.0 10.0 25.02003 P080295 Polio Eradication Nigeria 0.0 28.7 28.7 28.72003 P074856 HIV/AIDS Prevention Project Pakistan 0.0 37.1 37.1 37.12003 P081909 Partnership For Polio Eradication Pakistan 0.0 20.0 20.0 20.02003 P064237 TB/AIDS Control Russia 150.0 0.0 150.0 150.02003 P046497 Health Reform Implementation Russia 24.0 0.0 24.0 30.02003 P071374 Multisectoral HIV/AIDS Rwanda 0.0 10.7 10.7 30.5

A P P E N D I X C : W O R L D B A N K H N P S E C T O R P R O J E C T S , F I S C A L Y E A R S 1 9 9 6 – 2 0 0 7
1 3 1
Appendix C: World Bank HNP Sector Projects Approved in Fiscal Years 1996–2007 (continued)
HNP commitment($US millions)
Fiscal year Project Total Totalapproved ID Project name Country IBRD IDA HNP commitment
2003 P077675 Health Serbia 0.0 20.0 20.0 20.02003 P074128 Health Sector Reconstruction and Development Sierra Leone 0.0 14.0 14.0 20.02003 P074730 National HIV/AIDS Prevention Sri Lanka 0.0 6.3 6.3 12.62003 P076798 HIV/AIDS Prevention and Control Project St . Kitts & Nevis 2.9 0.0 2.9 4.12003 P075528 HIV/AIDS Prevention and Control Trinidad & Tobago 20.0 0.0 20.0 20.02003 P069857 TB/AIDS Control Ukraine 45.0 0.0 45.0 60.02003 P003248 Zanara HIV/AIDS APL Zambia 0.0 16.8 16.8 42.02004 P082613 Regional HIVAIDS Treatment Acceleration Africa 0.0 38.9 38.9 59.82004 P074850 HIV/AIDS Project for Abidjan Lagos Transport Africa 0.0 6.8 6.8 16.6
Corridor2004 P071025 Provincial Maternal-Child Health Argentina 115.4 0.0 115.4 135.82004 P072637 Provincial Maternal-Child Health Sector Argentina 675.0 0.0 675.0 750.0
Adjustment2004 P073974 Health Systems Modernization Armenia 0.0 17.9 17.9 19.02004 P083169 HIV/AIDS and STI Prevention and Control Bhutan 0.0 2.6 2.6 5.82004 P087841 Social Sector Programmatic Credit Bolivia 0.0 6.3 6.3 25.02004 P083013 Disease Surveillance and Control II Brazil 57.0 0.0 57.0 100.02004 P080721 HIV/AIDS Prevention and Control Caribbean Region 0.0 2.3 2.3 9.02004 P077513 HIV/AIDS & Health Congo, Rep. of 0.0 4.6 4.6 19.02004 P073442 HIV/AIDS Global Mitigation Support Guinea-Bissau 0.0 1.4 1.4 7.02004 P076722 HIV/AIDS Prevention and Control Guyana 0.0 4.7 4.7 10.02004 P050655 Rajasthan Health Systems Development India 0.0 71.2 71.2 89.02004 P086670 Health Sector Management Macedonia, FYR 9.0 0.0 9.0 10.02004 P073821 Multi-Sectoral AIDS Malawi 0.0 3.5 3.5 35.02004 P078368 Multisectoral HIV/AIDS Control Mauritania 0.0 4.2 4.2 21.02004 P082223 Health System (Montenegro) Montenegro 0.0 4.9 4.9 7.02004 P075979 Social Sector Support São Tomé & Principe 0.0 1.7 1.7 6.52004 P082879 Health TA Slovak Republic 4.3 0.0 4.3 12.42004 P065954 Health Reform - SECAL Slovak Republic 50.3 0.0 50.3 62.92004 P050740 Health Sector Development Sri Lanka 0.0 26.4 26.4 60.02004 P082335 Health Sector Development II Tanzania 0.0 58.5 58.5 65.02004 P071014 HIV/AIDS Tanzania 0.0 10.5 10.5 70.02004 P075230 Health Sector Support Tonga 0.0 10.6 10.6 10.92004 P074053 Health Transition Turkey 24.2 0.0 24.2 60.62005 P080406 African Regional Capacity Building Network Africa 0.0 8.5 8.5 10.0
for HIV/AIDS Prevention, Treatment, & Care2005 P080413 HIV/AIDS Great Lakes Initiative APL Africa 0.0 11.0 11.0 20.02005 P083180 HAMSET SIL Angola 0.0 1.9 1.9 21.02005 P074841 HNP Sector Program Bangladesh 0.0 120.0 120.0 300.02005 P091365 Social Sector Programmatic Credit II Bolivia 0.0 3.8 3.8 15.0
(Table continues next page)

1 3 2
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Appendix C: World Bank HNP Sector Projects Approved in Fiscal Years 1996–2007 (continued)
HNP commitment($US millions)
Fiscal year Project Total Totalapproved ID Project name Country IBRD IDA HNP commitment
2005 P088663 Health Sector Enhancement Bosnia-Herzegovina 0.0 9.4 9.4 17.02005 P082243 HIV/AIDS Central America 0.0 6.0 6.0 8.02005 P087003 AIDS Control Central Asia 0.0 16.3 16.3 25.02005 P094694 HIV/AIDS/STI/TB/Malaria/Reproductive Eritrea 0.0 12.0 12.0 24.0
Health2005 P065126 Health Sector Support Guinea 0.0 17.5 17.5 25.02005 P073651 Disease Surveillance India 0.0 37.4 37.4 68.02005 P075058 Health Systems India 0.0 88.7 88.7 110.82005 P087843 HIV/AIDS Capacity Building TAL Lesotho 0.0 3.0 3.0 5.02005 P083401 Health Sector Support Malawi 0.0 12.0 12.0 15.02005 P040613 Health Sector Program Project Nepal 0.0 43.5 43.5 50.02005 P078991 Health Sector II (APL 2) Nicaragua 0.0 10.2 10.2 11.02005 P079628 Women’s Health and Safe Motherhood II Philippines 12.5 0.0 12.5 16.02005 P078971 Health Sector Reform II Romania 76.8 0.0 76.8 80.02005 P076795 HIV/AIDS Prevention and Control St Lucia 0.8 0.8 1.7 6.42005 P076799 HIV/AIDS Prevention and Control St. Vincent & 1.0 1.0 2.0 7.0
the Grenadines2005 P051370 Health II Uzbekistan 0.0 40.0 40.0 40.02005 P082604 HIV/AIDS Prevention Vietnam 0.0 24.5 24.5 35.02006 P082814 Health System Modernization Albania 0.0 13.1 13.1 15.42006 P094220 Health Sector Reform Azerbaijan 0.0 43.0 43.0 50.02006 P096482 Malaria Control Booster Program Benin 0.0 18.6 18.6 31.02006 P093987 Health Sector Support and AIDS Burkina Faso 0.0 35.3 35.3 47.72006 P088751 Health Sector Rehabilitation Support Congo, Dem. Rep. 0.0 135.0 135.0 150.0
(Zaire)2006 P088575 Health Insurance Strategy Ecuador 90.0 0.0 90.0 90.02006 P088797 Multisectoral HIV/AIDS Ghana 0.0 6.2 6.2 20.02006 P077756 Maternal and Infant Health and Nutrition Guatemala 31.9 0.0 31.9 49.02006 P085375 Water Supply and Sanitation for Low-Income Indonesia 0.0 6.9 6.9 137.5
Communities III2006 P084977 Health and Social Protection Kyrgyz Republic 0.0 10.8 10.8 15.02006 P100081 Avian and Human Influenza Control Lao, PDR 0.0 1.2 1.2 4.02006 P074027 Health Services Improvement Project Lao, PDR 0.0 14.3 14.3 15.02006 P076658 Health Sector Reform Phase II Lesotho 0.0 4.6 4.6 6.52006 P090615 Multisectoral STI/HIV/AIDS Prevention II Madagascar 0.0 10.5 10.5 30.02006 P094278 Health and Nutrition Support Mauritania 0.0 7.3 7.3 10.02006 P083350 Institutional Strengthening & Health Sector Niger 0.0 22.8 22.8 35.0
Support Program2006 P097402 Second Partnership For Polio Eradication Pakistan 0.0 46.7 46.7 46.72006 P082056 Mother and Child Basic Health Insurance Paraguay 12.1 0.0 12.1 22.02006 P075464 National Sector Support For Health Reform Philippines 99.0 0.0 99.0 110.02006 P078978 Community and Basic Health Tajikistan 0.0 8.0 8.0 10.02006 P079663 Mekong Regional Health Support Vietnam 0.0 69.3 69.3 70.02006 P096131 Malaria Health Booster Zambia 0.0 5.8 5.8 20.0

1 3 3
APPENDIX D: IFC HEALTH INVESTMENTS, FISCAL YEARS 1997–2007

1 3 4
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Ap
pen
dix
D:
IFC
Hea
lth
In
vest
men
ts A
pp
rove
d in
Fis
cal Yea
rs 1
99
7–2
00
7
Proj
ect
IFC
IFC
Tota
l IFC
App
rova
lCo
mm
itmen
tsi
zelo
ans
equi
tyco
mm
itmen
tCo
untr
yPr
ojec
t nam
eda
teda
te(U
S$ 0
00)
Prim
ary
sect
or
Seco
ndar
y se
ctor
($
000
)($
000
)(n
et, U
S$ 0
00)
Uzbe
kist
anCo
re P
harm
30-J
un-9
701
-Oct
-97
12,2
00Ch
emic
als
Phar
mac
eutic
als
3,35
050
03,
850
Indi
aDu
ncan
Hos
pita
l30
-Jun
-97
31-O
ct-9
729
,300
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er7,
000
877,
087
Latin
Am
eric
a Re
gion
MSF
Hol
ding
20-N
ov-9
727
-Apr
-98
90,0
00Fi
nanc
e &
Insu
ranc
eRe
ntal
& L
easi
ng S
ervi
ces
15,0
002,
000
17,0
00
Arge
ntin
aHo
spita
l Priv
ado
30-A
pr-9
831
-Aug
-98
21,2
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
9,60
00
9,60
0
Sri L
anka
Apol
lo L
anka
06-M
ay-9
820
-Jun
-01
32,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
5,35
01,
096
6,44
7
Mex
ico
CIM
A M
exic
o30
-Jun
-98
04-N
ov-9
811
,200
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er0
4,80
04,
800
Mex
ico
CIM
A Pu
ebla
30-J
un-9
806
-Jan
-99
32,5
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
3,50
00
3,50
0
Cost
a Ri
caCI
MA
Cost
a Ri
ca30
-Jun
-98
04-N
ov-9
82,
800
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er0
1,20
01,
200
Braz
ilIta
bera
ba04
-Mar
-99
24-F
eb-0
025
,000
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er0
5,34
05,
340
Cent
ral E
urop
e Re
gion
Med
icov
er15
-Apr
-99
14-M
ay-9
922
,000
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er7,
000
07,
000
Mac
edon
ia, F
YRAl
kalo
id30
-Jun
-99
20-J
ul-9
938
,200
Chem
ical
sPh
arm
aceu
tical
s4,
473
04,
473
Dom
inic
an R
epub
licHo
spita
l16
-Jul
-99
07-A
pr-0
045
,900
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er2,
000
02,
000
Braz
ilFl
eury
17-A
ug-9
908
-May
-00
58,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
15,0
000
15,0
00
Phili
ppin
esAs
ian
Hosp
ital
14-F
eb-0
019
-Dec
-00
88,4
75He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
5,00
00
5,00
0
Mex
ico
Hosp
ital A
BC02
-May
-00
07-F
eb-0
181
,800
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er10
,294
010
,294
Chin
aW
an J
ie H
ospi
tal
26-J
un-0
028
-Nov
-01
57,3
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
15,0
000
15,0
00
Croa
tiaPl
iva
09-N
ov-0
017
-Nov
-00
113,
000
Chem
ical
sPh
arm
aceu
tical
s35
,000
035
,000
Russ
ian
Fede
ratio
nN
MC
27-D
ec-0
011
-Apr
-01
9,00
0He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
2,10
00
2,10
0
Indi
aOr
chid
01-M
ar-0
119
-May
-01
116,
000
Chem
ical
sPh
arm
aceu
tical
s20
,000
020
,000
Phili
ppin
esAE
I07
-Jun
-01
20-M
ay-0
34,
200
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er1,
000
01,
000
Latin
Am
eric
a Re
gion
Salu
tia12
-Jul
-01
04-J
an-0
210
,000
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er0
2,50
02,
500
East
ern
Euro
pe R
egio
nEu
rom
edic
09-O
ct-0
114
-Nov
-01
33,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
12,9
760
12,9
76
Viet
nam
F-V
Hosp
ital
11-O
ct-0
130
-Nov
-01
40,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
8,00
00
8,00
0
Egyp
t, Ar
ab R
ep. o
fSE
KEM
28-M
ar-0
216
-Jan
-03
13,3
00Ch
emic
als
Phar
mac
eutic
als
5,00
00
5,00
0
Cost
a Ri
caGu
tis24
-Jun
-02
10-J
an-0
315
,800
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er6,
000
06,
000
Indi
aM
ax H
ealth
care
04-A
pr-0
303
-Sep
-03
84,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
128
012
8

A P P E N D I X D : I F C H E A LT H I N V E S T M E N T S , F I S C A L Y E A R S 1 9 9 6 – 2 0 0 7
1 3 5
Latin
Am
eric
a Re
gion
Hosp
ital I
I09
-Apr
-03
26-M
ay-0
342
,200
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er12
,000
012
,000
Jord
anHi
kma
19-J
un-0
327
-Jun
-03
32,0
00Ch
emic
als
Phar
mac
eutic
als
14,8
660
14,8
66
Turk
eyM
ESA
Hosp
ital
23-J
un-0
322
-Jul
-03
45,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
11,0
000
11,0
00
Sout
hern
Eur
ope
Regi
onEu
rom
edic
II04
-Mar
-04
12-M
ar-0
425
,800
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er12
,644
012
,644
Turk
eyAc
ibad
em29
-Oct
-04
11-N
ov-0
440
,900
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er20
,000
020
,000
Indi
aBh
arat
Bio
tech
16-F
eb-0
526
-May
-05
4,50
0Ch
emic
als
Phar
mac
eutic
als
04,
500
4,50
0
Chin
aBi
oChi
na11
-Apr
-05
10-M
ay-0
525
,000
Colle
ctiv
e In
vest
men
t Pr
ivat
e Eq
uity
Fun
ds0
4,65
04,
650
Vehi
cles
Mex
ico
Cent
roM
edic
o PD
H27
-Apr
-05
10-J
un-0
569
,000
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er14
,500
014
,500
Bosn
ia a
nd H
erze
govi
naBo
snal
ijek
expa
n16
-May
-05
13-J
un-0
524
,273
Chem
ical
sPh
arm
aceu
tical
s9,
403
09,
403
Indi
aDa
bur P
harm
a03
-Jun
-05
07-J
un-0
569
,000
Chem
ical
sPh
arm
aceu
tical
s0
15,0
6415
,064
Mex
ico
Cent
ro E
span
ol07
-Jun
-05
27-A
pr-0
615
,000
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er5,
000
05,
000
Indi
aAp
ollo
equ
ity08
-Aug
-05
10-A
ug-0
5N
AHe
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
05,
085
5,08
5
Chin
aUn
ited
Fam
ily16
-Sep
-05
13-O
ct-0
516
,000
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er8,
018
08,
018
Chin
aSA
C04
-Nov
-05
22-N
ov-0
513
,000
Educ
atio
n Se
rvic
esEd
ucat
ion
3,00
01,
600
4,60
0
Ukra
ine
Bioc
on G
roup
31-J
an-0
615
-May
-06
7,22
3Ch
emic
als
Phar
mac
eutic
als
3,50
00
3,50
0
Turk
eyAc
ibad
em II
24-F
eb-0
614
-Mar
-06
112,
894
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er40
,000
040
,000
Keny
aAd
v Bi
o-Ex
tract
s23
-Jun
-06
18-J
an-0
729
,300
Chem
ical
sPh
arm
aceu
tical
s9,
000
09,
000
Egyp
t, Ar
ab R
ep. o
fDa
r Al F
ouad
01-A
ug-0
629
-Apr
-07
31,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
04,
000
4,00
0
Rom
ania
Med
Life
13-O
ct-0
616
-Oct
-06
30,0
00He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
6,34
85,
000
11,3
48
Chin
aAi
er E
ye25
-Oct
-06
06-N
ov-0
629
,825
Heal
th C
are
Hosp
itals
, Clin
ics,
Lab
orat
orie
s &
Oth
er8,
112
08,
112
Indi
aOc
imum
Bio
01-N
ov-0
603
-Nov
-06
19,7
60He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
2,60
03,
900
6,50
0
Chin
aFo
sun
Phar
ma
08-N
ov-0
608
-Nov
-06
104,
000
Chem
ical
sPh
arm
aceu
tical
s40
,560
040
,560
Nig
eria
Hyge
ia E
xpan
sion
25-J
an-0
730
-Jan
-07
6,23
0He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
3,03
30
3,03
3
Chin
aW
eiga
o23
-Feb
-07
02-M
ar-0
720
,000
Chem
ical
sPh
arm
aceu
tical
s20
,000
020
,000
Indi
aM
ax P
hase
II24
-May
-07
29-J
un-0
714
6,86
1He
alth
Car
eHo
spita
ls, C
linic
s, L
abor
ator
ies
& O
ther
067
,144
67,1
44
Indi
aGr
anul
es07
-Jun
-07
08-J
un-0
731
,900
Chem
ical
sPh
arm
aceu
tical
s9,
000
6,00
015
,000

Indian woman with her children, who help her run her business. Photo by Curt Carnemark, courtesy of the World Bank Photo Library.

1 3 7
The World Bank’s population strategies andlending over the past decade took place inthe context of a shifting international con-sensus on approaches to population controland reproductive health and a number ofcompeting agendas.1 The Bank’s initial in-
volvement in the HNP sector in the 1970s arose
primarily over concern for the adverse impacts of
rapid population growth and high fertility.
However, the 1994 International Conference on
Population and Development (ICPD) in Cairo
shifted the focus of population programs away
from fertility reduction and family planning and
toward women’s health, economic and social fac-
tors affecting the demand for children, and the
right to reproductive health care (Robinson and
Ross 2007). Shortly thereafter, the international
community’s attention was drawn to addressing
the rising threat of HIV/AIDS; sectorwide ap-
proaches in health; and, following the recom-
mendations of the World Development Report
1993, delivery of a package of basic or essential
health services for the poor.
The Bank’s 1999 population strategy (World Bank
1999c) committed to assist countries to link pop-
ulation to poverty reduction and human devel-
opment; advocate for cost-effective policies that
reflect country context; build on analysis and di-
alogue; provide sustained support; and strengthen
skills and partnerships. A year later, the MDGs
were adopted with no explicit family planning or
reproductive health goal, even though both are
key to achieving many of the other MDGs.
The focus of the Bank’s support for reducingfertility and population growth declined overthe decade, and family planning became one
of many components of an essential packageof health or reproductive health services.Over the period fiscal 1997 to 2006, the Bank ap-
proved only 14 population projects, defined for the
purposes of the review as those with population
in the title and/or including an objective to reduce
fertility, or with a population or family planning com-
ponent or subcomponent.2 Population projects
thus defined represented about 6 percent of the
HNP lending portfolio, declining from 11 to 2 per-
cent of the portfolio over the decade. The popu-
lation projects approved in three-quarters of the
countries were preceded by population projects.
Those in Bangladesh, India, Indonesia, and Kenya
represented the last in a long series stretching
back to the 1970s. However, the series ended dur-
ing the period under review, replaced by operations
focusing on reproductive health or sectorwide
activities.
The Bank’s population support was directedto only about a quarter of the 35 countrieswith high fertility. Among the 13 countries that
received Bank support, 8 had a total fertility rate
of 5.0 or greater. Only one freestanding popula-
tion project was approved—the Population and
Family Planning Learning and Innovation Loan
in Malawi, which implemented community-based
distribution of family planning in rural areas on a
pilot basis. Two of the projects packaged popu-
lation and AIDS activities, three were linked to ma-
ternal and child health or reproductive health, and
eight were part of a health or HNP sector project.
The main activities financed by these projects in-
cluded: training health workers; information, ed-
ucation, and communication on family planning
and the benefits of smaller families; contraceptives,
including social marketing; civil works; commu-
nity funds; policy reform; and economic activities
APPENDIX E: WORLD BANK SUPPORT FOR POPULATION

for women and youth. Almost all of the support
was to low-income countries.
None of the projects with explicit fertility orpopulation objectives achieved them. Thethree projects with population or familyplanning components but no explicit fertilityobjective3 at least partially achieved their ob-jectives. Eleven of the population projects ap-
proved from fiscal 1997 to 2006 have closed; only
3 had satisfactory outcomes. In Guinea, India,
Kenya, and Mali, modern contraceptive use and
fertility were scarcely affected.4 In Russia, the
abortion rate declined in project areas at the
same rate as in nonproject areas, while modern
contraceptive use was stagnant. In Bangladesh,
Gambia, and Senegal, fertility declined some-
what, but there is significant doubt about links to
the support of the Bank, other donors, or public
policy more generally.5 Bangladesh had experi-
enced a spectacular decline in fertility—from 7
children per woman in the 1970s to 3.3 by 1999—
in large part because of a highly successful fam-
ily planning program supported by the Bank and
other donors (IEG 2005b). From 1999 to 2004, fer-
tility continued to decline to 3.0 and the contra-
ceptive prevalence rate rose from about 50 to 60
percent, but it is unlikely that this is primarily at-
tributable to the family planning program sup-
ported by the Health and Population Sector
Program, given the disruption in service delivery
caused by the controversy in attempting (without
success) to absorb the vertical family planning
program into other health services.
Shortcomings in project preparation con-tributed to poor outcomes.6 According to com-
pletion reports and IEG fieldwork, project designs
were often excessively complex, driven by partic-
ipatory or sectorwide approaches. This often re-
sulted in a failure to prioritize activities, which
reduced the project’s feasibility and ultimate im-
pact in the face of low implementation capacity.
Also frequently noted was a lack of up-front risk
analysis, risk mitigation actions, and institutional
analysis. An IEG field evaluation of the Vietnam
Population and Family Health Project (1996–2003)
(IEG 2006d), for example, found very little in-
crease in oral contraceptive use, partly because the
existing incentives for two-child families within
the family planning delivery structure were not
taken into account. This is something that insti-
tutional analysis in advance of the project should
have been able to anticipate.
The absorption of population and familyplanning into sectorwide programs—be theySWAps or health reform projects—may havecontributed to the lack of results. There were
significant improvements in the modern contra-
ceptive prevalence rate and a reduction in the total
fertility rate during Ghana’s Second Population
and Family Health Project (1991–97). However,
under the subsequent Health Sector Support
Project (1998–2002), which supported a sector-
wide approach, there was no progress on either
of these outcomes (IEG 2005b, 2007d). A similar
situation occurred in Bangladesh, between the
Fourth Population and Health Project (1991–98)
and the subsequent Health and Family Planning
Program (1998–2005) (IEG 2006b). In both cases,
the transition to a SWAp increased the emphasis
on process, but did not ensure the achievement
of health-service performance and output tar-
gets, including those for population (IEG 2007d).
Field visits in Egypt underscored the findings
of a recent study that family planning and repro-
ductive health services are diluted within the
basic package of services delivered through new
family health facilities supported by the Health Re-
form Project (1998–present) (IEG 2008b). Clients
report that there are no longer special rooms in
facilities for family planning clients; female physi-
cians or specialists to discuss the topic are not
available; and family physicians have less special-
ized training and less time to devote to the clients
(Zaky 2007 as reported in IEG 2008b).
Nevertheless, there were some importantsuccesses in raising contraceptive use andsupport for fertility decline in high-fertilityenvironments, particularly with respect touse of family planning. The Egypt Population
Project (1996–2005) contributed to raising con-
traceptive use and lowering fertility in rural Upper
Egypt, while the Malawi Population and Family
Planning Project was able to raise modern con-
traceptive use in rural areas through community-
1 3 8
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION

based distributors. Both of these projects in-
cluded important demand-generation activities.
The Madagascar Second Health Program Support
Project financed training and contraceptives, with
a particular focus on a new, long-duration im-
plantable contraceptive that is easily inserted and
especially convenient in rural and remote areas.
The number of locations offering family planning
services increased by 45 percent from 2003 to
2007, and the contraceptive prevalence rate rose
from 9.7 to 24 percent (World Bank 2008e). Un-
fortunately, the successful investment in pilot
family planning activities in Malawi was not repli-
cated nationally, and contraceptive use remains
low, with little change (figure E.1). There has
been virtually no improvement in Ghana despite
support by the Bank and other donors for a health
SWAp over the past decade, and there has been
modest improvement in Bangladesh, despite the
disruption in family planning services by the
unpopular and ultimately failed attempt to unify
the delivery of health and family planning services.
The problems of high fertility and rapidpopulation growth have regained promi-nence internationally and in the Bank’spopulation strategy. There is greater recogni-
tion that lowering fertility and population growth
through demand-side activities alone will take a
very long time, while simply providing family
planning as part of a package of basic services is
unlikely to raise contraceptive prevalence dra-
matically in high-fertility countries or to lower
fertility among the very poor. Both demand- and
supply-side activities are important. Universal
access to reproductive health was added as an
MDG in 2007.7 The Bank’s 2007 population strat-
egy (World Bank 2007g) differentiates between re-
productive, maternal, and sexual health and the
services that address them and factors that affect
demographic outcomes. It links population, eco-
nomic growth, and poverty reduction and advo-
cates targeting assistance to the 35 countries with
total fertility rates exceeding 5.0, many of which
are also among the poorest countries in the world.
A P P E N D I X E : W O R L D B A N K S U P P O R T F O R P O P U L AT I O N
1 3 9
Figure E.1: Trends in Modern Contraceptive UseRates, Case Study Countries
70
60
50
40
30
20
10
0
0 10 20 30 40 50 60 70
Mod
ern
cont
race
ptio
n ra
te in
ear
liest
sur
vey
Malawi (2000–2004)
Ghana (1998–2003)
Eritrea (1995–2002)
Bangladesh (1996–2004)
Nepal (1996–2006)
Egypt (1995–2005)
Vietnam (1997–2002)
45 degree line
Peru (1996–2004)
Modern contraception rate in latest survey
Source: Nankhuni forthcoming, based on demographic and health survey reports (www.measuredhs.com) Note: Solid circle indicates that the change is statistically significant at 5 or 10 percent level, hollow circleindicates that the change is not statistically significant, and solid triangle indicates that it was not possibleto determine statistical significance. Countries below the 45-degree line experienced improvements in up-take of modern contraception rates.

Woman in Burkina Faso cooking a typical meal over a wood fire. Photo by Ray Witlin, courtesy of the World Bank Photo Library.

1 4 1
The 2006 World Bank publication, Reposi-tioning Nutrition as Central to Develop-ment: A Strategy for Large Scale Action(World Bank 2006c), argues that malnutri-tion is one of the world’s most serious healthproblems and the largest contributor tochild mortality. About a third of children in de-
veloping countries are underweight (low weight
for age) or stunted (low height for age), and
about 30 percent of the population of those coun-
tries suffers from deficiencies in micronutrients
such as vitamin A, iodine, or iron.1 Women and
children are particularly affected, and nutritional
deficiencies in children while they are still in the
womb and up to age 2 can have lifelong conse-
quences. Malnutrition among children is highest
in South Asia and is high and increasing in Sub-
Saharan Africa. It affects both the poor and the
non-poor, but is greater among the poor: in 39 out
of 46 countries with recent household surveys,
more than half of children are stunted, and stunt-
ing is as much as eight times higher among the
poorest wealth quintile than among the richest.2
Tackling malnutrition not only contributesto the MDG of halving the share of peoplewho suffer from hunger, but also to otherMDGs that deal with reducing child mor-tality, improving maternal health, raisingschool achievement, and reducing incomepoverty.
The causes of malnutrition are diverse and in-
clude inadequate breastfeeding, poor child feed-
ing practices, diarrheal disease and other illness,
intestinal parasites, frequent and closely spaced
childbearing, inadequate diet, low access to health
care, unsafe water, poor sanitation, low purchas-
ing power, and in some cases inadequate food pro-
duction. However, the fact that the non-poor also
have significant levels of malnutrition indicates that
knowledge and behavior are often key.
World Bank support is in countries withhigh malnutrition, but coverage of the worst-affected countries is low. IEG undertook an in-
depth desk review of the 21 projects approved
from fiscal 1997 to 2006 with nutrition objectives
(10 percent of the HNP lending portfolio),3 plus
6 additional projects with nutrition in the title or
nutrition components or subcomponents, for a
total of 27 projects, henceforth called “nutrition
projects.”4 About half of them are general health
or HNP projects, five are freestanding nutrition
projects, four are mother and/or child health proj-
ects, and the remaining five are emergency or
multisectoral programmatic lending.5 While about
two-thirds of the nutrition projects were in coun-
tries with average child stunting of 30 percent or
more, only about a quarter of countries with such
high levels of malnutrition were receiving World
Bank nutrition support.6 Two-thirds of nutrition
projects were in low-income countries. While
Africa had the largest number of nutrition projects
(9), South Asia had the highest share of nutrition
projects relative to the rest of the Regional port-
folio (29 percent).7 The share of projects with
nutrition objectives declined from 12 to 7 percent
between the first and second half of the decade.
The types of interventions supported by these op-
erations included growth monitoring and nutri-
tional surveillance (100 percent), micronutrient
supplements (52 percent), behavior change (nu-
trition education, promotion of growth moni-
toring, breastfeeding, specific dietary changes,
and hygiene, 48 percent), and feeding supple-
ments or rehabilitation of malnourished children
(41 percent). The projects also supported ca-
APPENDIX F: WORLD BANK SUPPORT FOR NUTRITION

pacity building in the form of nutrition policy de-
velopment, training, and data collection. However,
4 of the 27 projects had an explicit objective to im-
prove nutrition, with no nutrition components or
subcomponents in the appraisal document.8
The diverse causes of malnutrition madenutrition projects organizationally com-plex—about half were multisectoral in imple-
mentation and in half of the multisectoral projects,
the executing agency was outside of the Ministry
of Health. The projects were managed by the
Ministry of Health or by the Ministry of Finance/
Economy/ Plan (four projects each); jointly exe-
cuted by multiple ministries, one of which was the
Ministry of Health (three projects); by a non-
health ministry (two projects); or by the Office of
the President or Prime Minister (one project).
The number of implementing agencies was often
greater, with six projects relying on three imple-
menting ministries and two projects on four im-
plementing agencies.
Several of the case study countries suffered from
high levels of child malnutrition, overall and
among the poor, and in most cases there was lit-
tle improvement (figure F.1). A 2005 IEG impact
evaluation found that, although nutritional status
in Bangladesh has improved over time, the link
between the interventions and outcomes was
weak (box F.1). Although the interventions pro-
duced some modest improvements, most nutri-
tion improvements over the period were brought
about by better food availability and lower prices
linked to the increase in rice yields since the late
1990s. The case study teams pointed to malnu-
trition as particularly neglected in the Bank’s sup-
port over the past decade in Nepal, Peru, and (at
least until recently) Malawi. The observed im-
provements in rural Nepal could also have been
affected through interventions in other sectors,
such as water supply and sanitation.9 Ghana has
had no specific nutrition support from the Bank,
but experienced an increase in rural stunting
over the course of sectorwide Bank support.
The overall performance of the nutritionprojects was weak. Fifteen of the nutrition proj-
ects had closed and been reviewed by IEG; 64
percent had satisfactory outcomes—about the
same as the rest of the portfolio. But this statistic
is deceptive, since nutrition is often only one of sev-
eral objectives, and in some cases only a small
component of a larger project.10 Only two proj-
ects—Indonesia Iodine Deficiency Control and
Senegal Nutrition—demonstrated substantial ef-
ficacy in meeting their objectives, with resulting
changes in nutritional outcomes. In Indonesia, in-
creased consumption of iodized salt and targeted
distribution of iodine capsules helped reduce the
total goiter rate by 35 percent in highly endemic
provinces and by more than 50 percent in a few
others.11 The Senegal project surpassed almost
all of its targets in terms of outputs (training, chil-
dren and mothers reached, health posts equipped)
and demonstrated improvements in some nutri-
tion indicators (exclusive breastfeeding), though
for a few indicators, only by slightly more than in
control areas (World Bank 2007c). Among the re-
maining 12 projects, the completion reports for 4
suggested little or no impact,12 and for 8 projects
1 4 2
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Figure F.1: Trends in Stunting in the Rural Areas ofCase Study Countries, 1995–2006
80
70
60
50
40
30
20
20 30 40
Percent stunted in latest survey
50 60 70 80
Perc
ent s
tunt
ed in
ear
liest
sur
vey
45 degree line
Malawi (2000–2004)
Ghana (1998–2003)
Egypt (1995–2000)
Eritrea (1995–2002)
Bangladesh (1996–2004)
Peru (1996–2000)
Nepal (1996–2001)
Source: Nankhuni forthcoming, based on demographic and health survey reports.Note: Solid circle indicates statistically significant change at p<.05 or p<.10; empty circle indicates that thechange is not statistically significant; solid diamond indicates that it was not possible to determine statis-tical significance. Countries above the 45-degree line experienced reductions in stunting levels, those belowthe line experienced increases, and those along the line experienced no change.

the impact was unclear, often due to the failure to
collect data or report on nutrition outcomes.
Complexity was cited as contributing to theshortcomings in more than half of the weak-performing projects. Projects in Bangladesh,
Indonesia, Nicaragua, and Sri Lanka had to be
scaled back and the efforts prioritized to include
fewer activities or a smaller geographic area. The
Food Security and Social Mobilization Project in
Mauritania suffered from the inexperience and
institutional weaknesses of the Executive State
Secretariat for Promotion of Women, in addition
to high project complexity. The Uganda Nutrition
and Child Development Project was designed as
a pilot intended for only a few districts; expansion
of its geographical coverage without additional
resources greatly increased its complexity.
M&E were particularly weak for both proj-ects with nutrition components and thefreestanding nutrition projects. Nutrition out-
comes are affected by many factors beyond the
interventions in these projects; it is thus very im-
portant to attempt to monitor other important fac-
tors that could be affecting outcomes, a lesson of
the project in Senegal. However, these projects
failed even to collect basic data on nutrition out-
comes, such as micronutrient consumption (Gam-
bia, Mauritania, Sri Lanka) or the projects’ main
outputs (Sri Lanka). The Bangladesh project did
not collect baseline data until two years before the
end of the project; the Indonesia project pro-
duced baseline and final data from different groups
of people; the India Women and Child Develop-
ment Project collected data on children aged 0–3
when the target group was aged 0–6. The com-
pletion report for the Nicaragua project reported
no outcomes at all.
This experience nevertheless presents someimportant lessons for future nutrition proj-ects. Several projects reported success in the
use of community volunteers to mobilize com-
munities or deliver services (Gambia, Senegal,
Nicaragua), while one of the reasons for poor
performance in Mauritania was the limited ca-
pacity of communities to undertake growth-pro-
motion activities. The experience also highlighted
the importance of demand generation for nutri-
A P P E N D I X F : W O R L D B A N K S U P P O R T F O R N U T R I T I O N
1 4 3
The Bank has supported improved nutrition in Bangladeshthrough two freestanding nutrition projects—the Bangla-desh Integrated Nutrition Project (BINP, 1995–2002) andthe National Nutrition Project (2000–07)—and as part oftwo projects supporting sectorwide approaches in HNP.In 2005, IEG evaluated the impact of the BINP, whichwas based on a community-based approach that providednutrition counseling to bring about behavior change andsupplementary feeding for pregnant women and youngchildren.
The evaluation found that coverage of the interven-tion was high in project areas in general, but that thecausal link between the interventions and nutrition out-comes was weakened by targeting deficiencies; largeshares of mothers and children receiving supplementalfeeding but no counseling; and the focus of behavior
change almost exclusively on mothers, who are often notthe main decision makers on nutrition-related practices(both husbands and mothers-in-law have an important in-fluence). Supplementary feeding had some impact amongthe most malnourished, but was a costly part of the pro-gram and not sustainable in the long run.
The follow-on National Nutrition Program revised thetargeting criteria and attempted to reach out to men withbehavior-change messages. The program was delayedand scaled back, but was able to maintain the achieve-ments of micronutrient coverage and to promote adop-tion of new behaviors. It was unable to demonstratesustainable improvements in birth weights and nutritionstatus of vulnerable groups; however, the baseline wascollected only two years before the end of the project andmonitoring data were not collected.
Box F.1: Reductions in Malnutrition in Bangladesh: Lessons from the IntegratedNutrition Project
Source: IEG 2005c, World Bank 2007e.

tion services and behavior change communication
for success in Senegal: lack of demand was a fac-
tor in weak results in India and Mauritania. Mul-
tisectoral coordination and the engagement of
sectors outside of health was lacking in India and
Mauritania. Two early child development proj-
ects pointed to the need for better targeting of
children in a more appropriate age range (Uganda)
or with more education and counseling (India).
Finally, a number of projects cited the need to de-
velop simpler indicators for use by grassroots
groups, to adopt more realistic and measurable
targets (Bangladesh), and to identify monitoring
indicators for improved supervision (Sri Lanka).
To summarize, the need to address malnutrition
in client countries is great, and the coverage of
Bank support for the hardest-hit countries is low.
However, the multidimensional determinants of
nutrition tend to lead to complex projects that
involve multiple sectors. While there have been
demonstrable results in a few cases, the overall re-
sults for the HNP-managed nutrition portfolio
were thin.
1 4 4
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION

1 4 5
The Bank’s analytic work in HNP includes both the
products of the lending part of the institution
and research products and other publications of
Bank staff. Official economic and sector work
(ESW) financed directly from the Bank budget for
country, Regional, or global-level HNP analysis is
tracked in an internal database.1
Between fiscal 2000 and 2008 the Bankspent $43 million of its own budget andtrust funds on a total of 218 ESW tasks that
generated reports, policy notes, conferences,
workshops, consultations, and country dialogue
on HNP. 2 This amounts to about 4 percent of
ESW Bank-wide for those years, whether measured
in costs or number of activities.
However, the true amount of HNP analyticwork undertaken by the Bank far exceedswhat is in the official database. The tracking
system excludes the work of the Bank’s Research
Department and major undertakings, such as
the World Development Report 2004: Making
Services Work for the Poor and the multiyear re-
search on Reaching the Poor with Health, Nu-
trition, and Population Services (World Bank
2005a).3 An exhaustive search for all individual ar-
ticles, working papers, studies, toolkits, reports,
and research published by the Bank or Bank staff
on HNP topics counted a total of 1,457 pieces is-
sued over fiscal 1997–2006—six times more than
implied by the official ESW database.4
ESW on HNP tripled over fiscal 2001–05,then dropped to half its previous levels infiscal 2006–08 (figure G.1). About two-thirds of
these activities were conducted at the country
level, about a quarter at the Regional level, and 7
percent at the global level.5 The largest shares of
these ESW activities were country-level HNP sec-
tor studies (42 percent), studies of health finance
(33 percent), HIV/AIDS studies (31 percent), or
health strategies or policies (29 percent). The in-
crease in ESW in fiscal 2002 and 2004–05 is mostly
attributable to an increase in country-level sector
studies or reviews in those years; there followed
a large drop in fiscal 2007–08.
Prominent among the country-level studies was
a series of more than a dozen HNP Country Sta-
tus Reports launched by the Africa Region in 2003,
with the purpose of informing the HNP discussion
in Poverty Reduction Strategies. Most used the an-
alytic framework proposed in the HNP chapter of
the Sourcebook for Poverty Reduction Strategies
(Claeson and others 2002), linking health out-
comes, household and community characteristics
and behaviors, health care delivery and financing,
and other sectors affecting health. All focused on
the relationship between health and poverty to dif-
fering degrees and included a chapter on public
expenditures in health and health financing.
Nearly two-thirds of all ESW tasks since2002 that stated an objective were intendedto inform government policy, while onlyhalf aimed to inform lending.6 Other main ob-
jectives of the HNP ESW portfolio were to inform
public debate (42 percent), inform the devel-
opment community (32 percent), and build ca-
pacity (25 percent). Not surprisingly, country and
Regional ESW were more likely intended to inform
government policy, and country-level ESW was the
most likely to have an objective to inform lend-
ing (55 percent), while all—or nearly all—global
HNP ESW intended to inform public debate or the
APPENDIX G: WORLD BANK SUPPORT FOR ANALYTIC WORK ON HNP
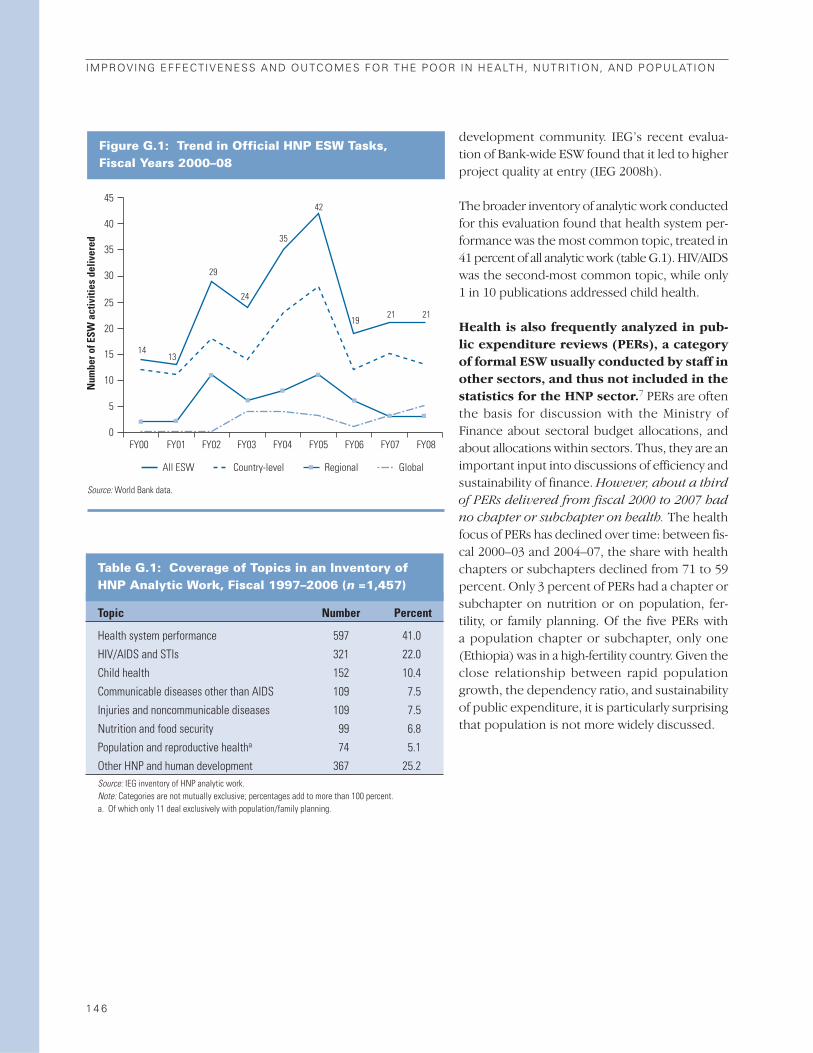
development community. IEG’s recent evalua-
tion of Bank-wide ESW found that it led to higher
project quality at entry (IEG 2008h).
The broader inventory of analytic work conducted
for this evaluation found that health system per-
formance was the most common topic, treated in
41 percent of all analytic work (table G.1). HIV/AIDS
was the second-most common topic, while only
1 in 10 publications addressed child health.
Health is also frequently analyzed in pub-lic expenditure reviews (PERs), a categoryof formal ESW usually conducted by staff inother sectors, and thus not included in thestatistics for the HNP sector.7 PERs are often
the basis for discussion with the Ministry of
Finance about sectoral budget allocations, and
about allocations within sectors. Thus, they are an
important input into discussions of efficiency and
sustainability of finance. However, about a third
of PERs delivered from fiscal 2000 to 2007 had
no chapter or subchapter on health. The health
focus of PERs has declined over time: between fis-
cal 2000–03 and 2004–07, the share with health
chapters or subchapters declined from 71 to 59
percent. Only 3 percent of PERs had a chapter or
subchapter on nutrition or on population, fer-
tility, or family planning. Of the five PERs with
a population chapter or subchapter, only one
(Ethiopia) was in a high-fertility country. Given the
close relationship between rapid population
growth, the dependency ratio, and sustainability
of public expenditure, it is particularly surprising
that population is not more widely discussed.
1 4 6
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Figure G.1: Trend in Official HNP ESW Tasks, Fiscal Years 2000–08
45
40
35
30
25
20
15
10
5
0
Num
ber o
f ESW
act
iviti
es d
eliv
ered
1413
29
24
35
21 2119
42
FY00 FY01 FY02 FY03 FY04 FY05 FY06 FY07 FY08
All ESW Country-level Regional Global
Source: World Bank data.
Table G.1: Coverage of Topics in an Inventory of HNP Analytic Work, Fiscal 1997–2006 (n =1,457)
Topic Number Percent
Health system performance 597 41.0
HIV/AIDS and STIs 321 22.0
Child health 152 10.4
Communicable diseases other than AIDS 109 7.5
Injuries and noncommunicable diseases 109 7.5
Nutrition and food security 99 6.8
Population and reproductive healtha 74 5.1
Other HNP and human development 367 25.2Source: IEG inventory of HNP analytic work. Note: Categories are not mutually exclusive; percentages add to more than 100 percent. a. Of which only 11 deal exclusively with population/family planning.

1 4 7
APPENDIX H: ADDITIONAL FIGURES ON WORLD BANK HNPLENDING, ANALYTIC WORK, AND STAFFING

1 4 8
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Figure H.1: IEG Ratings for Closed HNP Projects Approved in Fiscal 1997–2006, byYear of Approval
Perc
ent o
f pro
ject
s ra
ted
mod
erat
ely
satis
fact
ory
or h
ighe
r 100
80
60
40
20
0 Outcome Quality at entry
Rating category
Quality of supervision Bank performance Borrower performance
Fiscal years 1997–99 (n = 55) Fiscal years 2000–06 (n = 44)
56
64 66 63 64 59
71 66
70 73
Source: World Bank data.
Figure H.2: IEG Ratings for Closed HNP Projects Approved in Fiscal 1997–2006, by Year of Exit
Perc
ent o
f pro
ject
s ra
ted
mod
erat
ely
satis
fact
ory
or h
ighe
r
100
80
60
40
20
0 Outcome Quality at entry
Rating category
Quality of supervision Bank performance Borrower performance
Fiscal years 2001–05 (n = 47) Fiscal years 2006–08 (n = 52)
62 69 71
64 67
54
65 67 63
67
Source: World Bank data.

A P P E N D I X H : A D D I T I O N A L F I G U R E S O N W O R L D B A N K H N P
1 4 9
Figure H.3: IEG Bank Performance Ratings, by Sector Board and Fiscal Year of Exit
Perc
ent o
f pro
ject
s ra
ted
mod
erat
ely
satis
fact
ory
or h
ighe
r
100
80
60
40
20
0 1987–91 1992–96 1997–2001 2002–06
80
68
Other sectors HNP sector
Fiscal year project closed
Source: World Bank data.
Figure H.4: IEG Borrower PerformanceRatings, by Sector Board and Fiscal Year of Exit
Perc
ent o
f pro
ject
s ra
ted
mod
erat
ely
satis
fact
ory
or h
ighe
r
100
80
60
40
20
0 1987–91 1992–96 1997–2001 2002–06
76
71
Fiscal year project closed
Other sectors HNP sector
Source: World Bank data.
Figure H.5: IEG Sustainability Ratings, HNPand Other Sectors, by Fiscal Year of Exit
Perc
ent o
f pro
ject
s ra
ted
likel
y or
hig
h
100
80
60
40
20
01987–91 1992–96 1997–2001 2002–06
7874
(n = 14)
Fiscal year project closed
Other sectors HNP sector
Source: World Bank data.
Figure H.6: Mean and Median HNP ProjectPreparation Costs, by Fiscal Year of Approval (nominal dollars)
Fiscal year of approval
Mean Median
Thou
sand
s of
US
dolla
rs
450
400
350
300
250
200
150
100
50
0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Note: N = 220 projects.

1 5 0
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Figure H.7: Duration of HNP ProjectPreparation, by Fiscal Year of Approval
Fiscal year of approval
Mean Median
Mon
ths
25
20
15
10
5
01997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Note: N = 220 projects.
Figure H.8: Average Annual SupervisionCosts for Investment Projects Managed byHNP and Other Sectors
Cons
tant
200
6 U
S$ th
ousa
nds
120
80
100
60
20
40
0 2000 2001 2002 2003 2004
Fiscal year
2005 2006 2007 2008
Health Sector Board Other sectors
Source: World Bank data.
Figure H.10: HNP Operational Staff, byRegion and Fiscal Year
Num
ber o
f HN
P st
aff
60
50
40
30
20
10
0
Fiscal year
Africa South Asia Europe and Central Asia
Middle East and North Africa Latin America and the Caribbean East Asia and Pacific
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Source: Nankhuni and Modi 2008.
Figure H.9: Trends in HNP and Hub-MappedStaff of Level GF+ (excluding coterms), Fiscal 1997–2007
Num
ber o
f HN
P st
aff
200
150
100
50
0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Fiscal year
HNP mapped staff HDNHE & HDNGA (hub) mapped
158169
184
169
145136
178 174
165
183 185
1815 161722181918181312
Source: Nankhuni and Modi 2008.

A P P E N D I X H : A D D I T I O N A L F I G U R E S O N W O R L D B A N K H N P
1 5 1
Figure H.11: Trend in Population andNutrition Staff
Num
ber o
f pop
ulat
ion
or n
utri
tion
staf
f
25
20
15
10
5
0
Fiscal year
Total staff with population in title Total staff with nutrition in title
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Source: Nankhuni and Modi 2008.Note: If staff have both population and nutrition in their title, they are counted in bothcategories.
Table H.1: Frequency of Bank Performance Issues in Closed HNP Projects Approved in Fiscal 1997–2006, by Project Outcome
Projects with Projects withunsatisfactory satisfactory
outcome outcome
Bank performance issue Number Percent Number Percent
Inadequate risk assessment 17 (40) 2 (4) 10:1
Inadequate technical design 17 (40) 3 (5) 8:1
Inadequate supervision 18 (43) 5 (9) 5:1
Inadequate political or institutional analysis 17 (40) 8 (14) 3:1
Inadequate baseline data or unrealistic targets 17 (40) 8 (14) 3:1
Inadequate M&E framework, poor data quality 36 (86) 26 (46) 2:1
Overly complex design 12 (29) 8 (14) 2:1
Inadequate partner financing or coordination 5 (12) 4 (7) 2:1
Implementation disrupted by a crisis 7 (17) 8 (14) 1:1
Inadequate prior analytic work 5 (12) 0 (0) —
Number of projects 42 57
Source: IEG review of ICRs.
Ratio of percentunsatisfactory
to percentsatisfactory
outcome

1 5 2
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
Tab
le H
.2:
Pro
bit
Reg
ress
ion
s o
n t
he
Det
erm
inan
ts o
f P
roje
ct O
utc
om
e R
atin
gs
( n=
94 in
vest
men
t pro
ject
s ap
prov
ed fr
om fi
scal
199
7–20
06)
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
Vari
able
dP/d
xT
dP/d
xT
dP/d
xT
dP/d
xT
dP/d
xT
dP/d
xT
dP/d
xT
dP/d
xT
Satis
fact
ory
Bank
qua
lity
at e
ntry
0.30
91.
430.
325
1.36
0.30
81.
440.
537
3.02
0.58
03.
610.
549
3.12
Satis
fact
ory
Bank
sup
ervi
sion
0.18
70.
970.
225
0.98
0.20
91.
020.
341
1.89
0.33
92.
020.
337
1.89
Satis
fact
ory
borro
wer
per
form
ance
0.80
04.
040.
822
4.06
0.79
94.
10
IDA
–0.0
97–0
.05
0.05
50.
23–0
.054
–0.2
80.
224
0.86
0.05
60.
290.
219
0.84
0.08
90.
630.
369
1.90
Mul
tisec
tora
l0.
050
0.29
0.04
00.
230.
112
0.68
0.22
70.
680.
234
0.71
0.32
31.
450.
424
1.46
IDA*
mul
tisec
tora
l–0
.554
–2.6
9–0
.627
–2.9
6–0
.456
–1.9
0–0
.531
–1.4
6–0
.505
–1.3
4–0
.689
–3.1
4–0
.700
–2.4
7
Euro
pe a
nd C
entra
l Asi
a0.
518
2.93
0.49
52.
880.
510
2.75
0.44
22.
63M
iddl
e Ea
st a
nd N
orth
Afri
ca0.
479
2.58
0.48
62.
520.
481
2.54
0.44
22.
07Ea
st A
sia
and
Paci
fic0.
288
1.32
0.30
61.
440.
266
1.16
0.34
51.
74La
tin A
mer
ica
and
Carib
bean
0.41
71.
840.
355
1.52
0.40
21.
680.
500
2.82
Sout
h As
ia0.
580
3.65
0.57
83.
080.
572
3.38
0.46
83.
01
$10–
50 m
illio
n–0
.027
–0.1
7–0
.004
–0.0
20.
052
0.33
0.25
81.
050.
197
0.83
0.27
61.
110.
082
0.42
0.09
90.
42$5
0–10
0 m
illio
n0.
034
0.22
0.07
00.
380.
101
0.66
0.19
30.
740.
120
0.45
0.20
30.
780.
089
0.44
0.03
00.
12>
$100
mill
ion
0.37
91.
330.
399
1.29
0.36
50.
22–0
.118
–0.2
4–0
.194
–0.4
2–0
.093
–0.1
90.
113
0.31
–0.2
20–0
.50
Appr
oved
fisc
al 2
000–
060.
018
0.12
0.00
90.
060.
142
0.91
0.17
11.
160.
139
0.95
0.19
21.
230.
133
1.10
0.20
41.
64Su
ppor
t for
SW
Ap–0
.450
–2.3
0–0
.339
–1.9
8–0
.096
–0.4
7Af
rica
MAP
(HIV
) pro
ject
–0.4
5–2
.10
–0.3
03–1
.20
–0.1
500.
52
Pseu
do R
20.
6433
0.67
360.
6615
0.45
510.
4372
0.45
680.
1443
0.25
15
Join
t tes
ts (p
val
ue)
Qual
ity a
t ent
ry, B
ank
supe
rvis
ion,
borro
wer
per
form
ance
0.
0010
0.00
080.
0007
0.00
000.
0000
0.00
00Re
gion
s0.
0008
0.00
690.
0028
0.01
57Lo
an s
ize0.
6180
0.63
040.
6103
0.60
730.
6408
0.58
000.
9746
0.79
56ID
A, m
ultis
ecto
ral,
inte
ract
ion
0.00
320.
0006
0.15
050.
2701
0.44
360.
0017
0.03
33ID
A, m
ultis
ecto
ral,
Afric
a M
AP0.
0028
0.38
92a.
Figu
res
in b
old
are
sign
ifica
nt a
t p <
.01;
figu
res
unde
rline
dar
e si
gnifi
cant
at p
< .0
5; fi
gure
s in
ital
icsar
e si
gnifi
cant
at p
< .1
0.
b.Th
e co
mpa
rison
gro
ups
are:
Afri
ca R
egio
n; p
roje
cts
of le
ss th
an $
10 m
illio
n; a
ppro
ved
in fi
scal
yea
rs 1
997–
99.

1 5 3
The Medicines for Malaria Venture (MMV)
funds and manages the discovery, development,
and registration of new medicines for the treat-
ment of malaria in disease-endemic countries in
response to the increasing incidence of and mor-
tality from malaria, the declining efficiency of
first- and second-line treatments, and the limited
response of the pharmaceutical industry to dis-
cover and develop new antimalarial drugs. The
MMV has been highly successful at achieving its
initial objectives—to establish and manage a
portfolio of antimalarial drug candidates—and
the public sector target price of a full course
of treatment of a dollar or less appears within
reach.
The MMV’s mandate has been expanded to in-
clude improving access and delivery of antimalarial
drugs. It is less clear whether MMV has the orga-
nizational arrangement and institutional rela-
tionships (notably with countries) to deliver on
the highly demanding downstream access and
delivery activities and whether it will be able to rec-
oncile its private sector entrepreneurial style with
the public sector requirements for resolution of
policy and institutional issues in access and de-
livery (IEG 2007e).
The Population and Reproductive HealthCapacity Building Program (PRHCBP), estab-
lished in 1999, is a merger of three programs:
Population and Reproductive Health, Safe Mother-
hood, and the Program to Reduce the Practice of
Female Genital Mutilation and Improve Adolescent
Health. Its objective is to build the capacity of
civil society organizations to develop and imple-
ment culturally appropriate interventions in pop-
ulation and reproductive health. It does this by
providing grants to international intermediaries,
which then make grants to grassroots groups, and
supporting operations research and technology
and information transfer. It is financed entirely
by the Bank’s Development Grant Facility, man-
aged within the Bank structure, and with no steer-
ing committee or other structure that would
enable actors external to the Bank to participate
in decision making and oversight. To date, the
Bank has allocated $18.3 million of Development
Grant Facility funding to the PRHCBP. The evalu-
ation found that the objectives of the program
were highly relevant, but that both efficacy and ef-
ficiency were difficult to assess because there was
no systematic measurement of the achievement
of the program’s stated objectives. Grant deci-
sion making by the Review Committee was a very
informal process. It was only in 2006 that public
solicitation of proposals became practice, and in
2007 that criteria for evaluating proposals were
established. For almost a quarter of all grants
awarded through fiscal 2007, there was no writ-
ten record of review decisions. Under the opera-
tions research component, PRHCBP has supported
the International Partnership for Microbicides to
develop new technologies to prevent HIV/AIDS
and unwanted pregnancy. The consolidation of the
three programs did not lead to clear objectives and
the links to country-level Bank operations were
weak (IEG 2008e).
APPENDIX I: EVALUATION OF WORLD BANK PARTICIPATION IN TWO GLOBAL HNP PARTNERSHIPS

This mobile health education van covers rural areas in Sri Lanka. Photo by Dominic Sansoni, courtesy of the World Bank Photo Library.

1 5 5
APPENDIX J: MANAGEMENT RESPONSE
Management highly values IEG’s evaluation of
World Bank Group support in the health, nutri-
tion and population sector, an important assess-
ment after 10 years of implementation of the
1997 health, nutrition and population (HNP) strat-
egy.1 The evaluation is helpful in articulating some
of the contextual difficulties the Bank Group faces
as a key partner in the international health envi-
ronment. Management has some general com-
ments on the changing context for its support,
followed by comments on the evaluation’s main
findings and recommendations. Lastly, the Re-
sponse cites the International Finance Corpo-
ration’s (IFC) evolving role in the sector. The
Management Action Record (attached to the Man-
agement Response Summary at the front of this
volume) provides a Bank Group response to IEG’s
recommendations. As noted below, the 2007
Health Strategy (World Bank 2007a) found issues
similar to those raised by IEG, not surprising be-
cause there was regular interaction between HNP
staff and the IEG team in the process of prepar-
ing the new strategy. The recent health Strategy
Progress Report (World Bank 2009) lays out the
Bank’s actions to strengthen its support, includ-
ing taking into account all of the major IEG analy-
sis and recommendations. Annex 2 of the Progress
Report, the Management Action Plan, summa-
rizes how the actions being taken correspond to
IEG’s recommendations, including assigning re-
sponsibilities and setting benchmarks for mea-
suring progress. For reference it is appended to
this response.
Changing Context for WBG SupportThe context in which the Bank Group provides
support in this sector has changed dramatically
during the last decade. That context affects how
the World Bank Group works.
A Changing Global Environment RequiresMore from the Bank. The last 10 years have
seen the creation of new international health in-
stitutions and foundations, as well as the emer-
gence of many different innovative health fund-
ing mechanisms.2 The welcome result has been
sharply increased global funding for HNP. The
Bank’s role has undergone a similar paradigm
shift. Although lending investment remains sig-
nificant, we now play a much more nuanced role,
working with and through partners and new in-
ternational institutions.3 This changing role, an-
chored in the Paris and Accra Declarations, is
desirable from a development perspective, but it
also imposes significant additional challenges in
attributing development outcomes to Bank fi-
nance or technical contributions. The sector is
constantly adapting to this rapidly evolving envi-
ronment, using the full spectrum of the Bank’s
comparative advantages beyond traditional lend-
ing and economic and sector work (ESW). The
benefits are clear, as are the risks of working in a
complex development area, investing in complex
health systems while respecting the multiplicity
of synergies necessary for a continuum of care and
service delivery, essential for public health and dis-
ease control, and in some instances relying on
partners to deliver results.
A Mandate to Achieve Health Outcomesthrough Health in All Policies. The interna-
tional health community and the World Bank
Group have recognized that, in addition to stand-
alone interventions and sector-specific policies, we
must focus on more comprehensive “health in all
policies.” Given how the Bank Group is organized,
this is our comparative advantage—and the HNP
sector has been moving in this direction over the
past years. The 2007 HNP strategy (World Bank

1 5 6
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
2007a) included a critical self-assessment of the
sector’s performance since 1997. The IEG evalu-
ation reconfirms much of this self-assessment,
and many of IEG’s recommendations are helpful
in achieving greater effectiveness and impact.
Main Findings and RecommendationsManagement agrees with many of the findings, and
appreciates the recommendations. Management
has taken them into account in the Progress
Report and the Plan of Action (see the attached
Action Plan). While not detracting from the im-
portance that it gives to the evaluation and its use-
fulness for the Strategy Progress Report, manage-
ment has a set of observations on some of the
findings.
Health Status Has More than One Devel-opment Dimension. Management considers
better health a development outcome in and of
itself, irrespective of its contributions to other
goals. In addition to improving health status, the
HNP sector aims to cushion the financial shocks
of health costs, which can be substantial in many
client countries, where out-of-pocket payments
dominate. Thus, while we agree that investments
should focus on health outcomes for the poor, it
is also vital to protect those above the poverty line
from financial shocks from poor health that push
families into poverty.
The World Bank Group’s Global HNP En-gagements Go Beyond Projects and ESW.The evaluation emphasizes lending, with some
attention to policy dialogue and analytic work.
But the HNP sector has expanded the paradigm
over the past decade. The World Bank Group uses
a range of engagement instruments, such as ana-
lytic and advisory activities (including IFC Advisory
Services),4 just-in-time policy advice, policy-based
lending led by other sectors, subnational lending
without a sovereign guarantee (through IFC), and
working through international networks and part-
nerships, such as the Global Alliance for Vaccines
Initiative (GAVI), the Global Fund to Fight AIDS,
Tuberculosis and Malaria (GFATM), and the Euro-
pean Union (EU) Observatory. Working with part-
ners through pooled funding, country systems
and joint strategies and supervision (as opposed
to ring-fenced Bank operations) is also anchored
in international commitments and agreements
such as the Paris and Accra Declarations. The suc-
cess of the Joint United Nations Program on
HIV/AIDS (UNAIDS), GFATM, GAVI, Roll Back
Malaria, EU Observatory and other major inter-
national partnerships is also the shared success of
the Bank Group’s HNP work, as we exercise sub-
stantial technical and financial influence in these
networks and partnerships. Over the past decade,
we have also enhanced internal collaborations to
improve the Bank Group’s impact on global health:
Examples include work across units (notably with
Concessional Finance and Global Partnerships,
Operations Policy and Country Services, and Trea-
sury for innovative financing mechanisms—the
International Finance Facility for Immunization, Ad-
vance Market Commitment, and Treasury services)
and partnerships with GFATM, GAVI, UNAIDS,
and others. Harnessing the Bank’s broader de-
velopment expertise has significantly impacted
the structure of the global health architecture, in
addition to saving millions of lives.
The Evaluation Framework Does Not Assessthe World Bank Group’s Non-TraditionalContributions to Global Health and ClientSupport. The evaluation’s review of four ap-
proaches misses much of the work carried out in
support of global public health, including key
analytical pieces, the global work on core public
health functions, water and sanitation, surveil-
lance and vital statistics, indoor air pollution,
avian and human influenza, and so forth. The
evaluation does not evaluate performance-based
approaches, which we believe have delivered im-
pressive results. Regarding SWAPs, we note that
before reaching any conclusions on their effec-
tiveness we need to take into account elements
beyond the evaluation that reflect the Bank’s sup-
port for greater donor coordination and the use
of country systems as enshrined in the Paris and
Accra Declarations.
Coverage of Analytic Work. Much of the non-
traditional analytical work has a potentially large
or larger impact than the Bank’s lending, especially
since Bank financing is usually a small share of
overall health spending in middle-income coun-

APPENDIX J : MANAGEMENT RESPONSE
1 5 7
tries.5 Knowledge-product tasks are often pre-
ferred to ESW to get findings out more quickly or
provide just-in-time advice to clients and part-
ners. The evaluation does not sufficiently account
for the role of analytic and advisory activities in
engaging clients and advancing policy dialogue,
either as a stand-alone tool to support the client
(in particular in middle-income countries) or as
a parallel track dialogue to investment and policy-
based lending. The evaluation could also have
taken greater account of other knowledge prod-
ucts, such as a large portfolio of Japan Policy and
Human Resources Development Fund (PHRD)
grant-financed analytic and advisory activities in
support of project preparation, as well as non-
formal ESW and technical assistance.
Improving Poverty Targeting. Management
agrees with the need to ensure that project design
responds to the priorities and needs of the poor,
and to measure the full impact of improved health
services for the poor. Indeed, the 2007 HNP strat-
egy explicitly recognizes the need to focus not
only on levels of HNP outcomes but also on their
distribution, especially among the poor. This fo-
cus in the strategy drew heavily on HNP’s path-
breaking Reaching the Poor Program, active since
2001. Reaching the Poor has delivered global lead-
ership in the measurement of disparities in HNP
health-service coverage and outcome indicators
among the poor versus the non-poor, as well as of
the financial burden on households from seeking
care. In 2005, Reaching the Poor published a re-
view of interventions and programs that had been
successful in reaching the poor (Gwatkin, Wagstaff,
and Yazbeck 2005). A new report (Yazbeck 2009)
has been produced in the period since the adop-
tion of the 2007 HNP strategy and was launched
in January 2009. This volume lays out a policy
menu emphasizing pro-poor policy reform along
six dimensions, and a list of the analytical tools to
better understand the constraints to pro-poor tar-
geting of public health investments.6 Management
will use these findings to ensure a better pro-poor
focus in future lending operations.
Disease Control Programs and Targeting. As
opposed to specific income groups, disease con-
trol programs must focus on the prevailing epi-
demiology. For example, an AIDS program must
focus on high-risk groups—irrespective of income.
A malaria program focused solely on the poor
would fail to eliminate malaria. Polio could only be
eradicated from the Western Hemisphere by fo-
cusing on large, inclusive campaigns targeting all
income groups. Such investments in public health
and control of communicable diseases are global
public goods, generating positive externalities for
society, irrespective of income status.
Investments in Health Systems. The 2007 HNP
strategy underscores the need to focus on health
systems for delivering improved HNP results, par-
ticularly for the poorest and the most vulnerable,
and the Bank has emerged as a strategic leader in
advancing health systems strengthening for im-
proved HNP results. Over the past two years, proj-
ects with a primary focus on health systems have
increased twofold. In line with the strategy, 67
percent of Bank programs approved since fiscal
year 2007 that focus on priority disease areas also
include strong components on health systems
strengthening. A new Health Systems for the
Health MDGs initiative was launched in 2008 to
bring together the resources and efforts to fund
and implement coherent, country-led health sec-
tor programs in Africa and selected countries in
Asia.7 This program will improve the Bank’s abil-
ity to rapidly assist and advise HNP operations on
the ground, particularly in the areas of health fi-
nance and risk pooling mechanisms, human re-
sources for health, governance, supply chain
management, as well as infrastructure planning.
HNP in Poverty Assessments and CASs. Man-
agement notes the substantive improvements
over the past years in quantity and quality of HNP
involvement in the Poverty Reduction and Eco-
nomic Management Network–led analytical work,
and agrees that HNP must be fully included in all
Poverty Assessments and fully examined in the
preparation of CASs.
Cross-Sector Work. Management welcomes the
suggestion to expand cooperation and cross-
sector work with the Transport, Water and Sani-
tation sectors. More will be done to harness cross-
sectoral results along the notion of “health in all

1 5 8
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
policies.” The 2007 HNP strategy is a good con-
duit to foster improved collaboration across sec-
tors in support of health outcomes. We note the
recommendation that “when the benefits are po-
tentially great in relation to the marginal costs,”
health objectives should be incorporated into
non-health projects, but also note that clients un-
dertake such operations largely for non-health
objectives and it would be unrealistic within cur-
rent resources to burden all such projects with po-
tentially small (albeit cost effective) health impact
objectives, or to demonstrate and document em-
pirically such impact and outcomes in each case.
The Quality of the Bank HNP Portfolio. Man-
agement appreciates the concern for the quality
of the Bank HNP portfolio—in particular in Africa.
The current data on riskiness of the HNP port-
folio confirms the fact that the problems are
most acute in the Africa Region, and that HNP’s
performance across most other Regions is ap-
proaching other sectors’ performance. An addi-
tional area of concern is the underperformance
of projects that have a significant HIV/AIDS com-
ponent, a high percentage of which have received
unsatisfactory ratings from IEG8,9 (with a rela-
tively high disconnect—as management rated
the outcomes of several of these operations as sat-
isfactory) and which also constitute a dispropor-
tionate number of projects at risk in the current
portfolio.
The HNP Action Plan for the Portfolio. As out-
lined in the Strategy Progress Report, the HNP sec-
tor is making major efforts to improve the quality
of the existing portfolio and ensure the quality of
new operations entering the portfolio. These ef-
forts include increasing candor in reporting to
close the realism gap and improving other port-
folio indicators. The Africa Region has imple-
mented several changes aimed at improving HNP’s
portfolio in the Region. In March 2008, the Qual-
ity Assurance Group (QAG) was asked to review
the performance of HNP projects that were cat-
egorized as being at risk. The QAG panel indicated
important areas for urgent attention: strength-
ening sector management oversight; reviewing
current resources for preparation/supervision;
and addressing two key weaknesses: monitoring
and evaluation (M&E) and institutional analysis.
A detailed Portfolio Improvement Action Plan
that includes all at-risk projects, as well as proj-
ects needing additional management oversight to
avoid falling into at-risk status, has been developed
and is being monitored on a quarterly basis by the
HNP Sector Board.10 The Portfolio Improvement
Action Plan addresses some of the key concerns
raised by the various reviews, namely, intensify-
ing management oversight, targeting of resources
to projects most in need, strengthening project
implementation to focus on monitoring and eval-
uation, and matching project interventions to the
country’s institutional capacity. A comprehensive
approach has also been adopted to improve the
quality of HIV/AIDS projects, and this included
an umbrella restructuring package of 11 Multi-
Country HIV/AIDS Programs (MAP) for Africa
projects in fiscal year 2007. Additional technical
support is being provided to improve imple-
mentation, develop impact evaluation capacity,
and strengthen governance and accountability
within national AIDS programs.
Doing More in Population and Reproduc-tive Health. The Strategy Progress Report high-
lights plans for strengthening support for pop-
ulation and reproductive health in a health systems
approach. That strengthening is critical to im-
proving maternal and child survival rates.
Investing in Nutrition Support. We also agree
with the evaluation’s findings that nutrition has
played a less prominent role within HNP over
the past 10 years. The need for action is even
more important today in the context of the af-
termath of the crises in fuel, food, and fertilizers,
as well as the escalating effects of the financial cri-
sis. Management is therefore investing significant
resources in the next few years to ramp up the
Bank’s analytical and investment work and lever-
age resources from other donors. The agenda
for scaling-up nutrition is being catalyzed with
additional budget resources starting in 2009, and
continuing for three years. The increased alloca-
tions are being utilized principally in Africa and
South Asia, two Regions where the malnutrition
burden is highest. These funds will be comple-
mented by additional trust fund resources from

APPENDIX J : MANAGEMENT RESPONSE
1 5 9
Japan, and possibly from other donors that are cur-
rently engaged in discussions on this issue.
Needed Improvement in Monitoring andEvaluation. Management agrees that M&E needs
to be improved, and it is an important part of
Strategy implementation, as noted in the Strat-
egy Progress Report (including the work on retro-
fitting projects and improving the design of new
projects). The evaluation proposes a focus on
strengthening health information systems. How-
ever, in some cases, routine health monitoring
systems (including surveillance, facility reporting,
vital registration, census data, resource tracking,
and household surveys) first need to be strength-
ened to provide the data and indicators that are
needed. The Bank has deepened its collaboration
with the Health Metrics Network, a global part-
nership aimed at building statistical capacity in
countries to improve the collection and use of
health information. The Bank has produced a
toolkit on measuring health system governance to
better monitor accountability in the sector, and this
is being piloted in five countries with support of
the Governance and Anti-Corruption Trust Fund.
One of the largest impact evaluation trust funds at
the Bank, the Spanish Trust Fund for Impact Eval-
uation, is housed in the human development sec-
tor. The trust fund, which was initiated in 2007 and
will continue until 2010, finances rigorous impact
evaluations of interventions aimed at enhancing
human development as well as learning and dis-
semination activities to help promote knowledge
and awareness of “what works” in the human de-
velopment Sector. The Bank is also working with
partners, such as WHO, to develop better ways to
monitor the health MDGs, including the estima-
tion of trends in child and maternal mortality for
which updates have recently been issued.
The Problem of Attribution. The evaluation ar-
gues for a better attribution of health outcomes
to inputs financed by the World Bank Group.
Health outcomes are hard to evaluate within the
timeframe of a project and are influenced by mul-
tiple determinants. Also, the Paris and Accra De-
clarations emphasize the greater development
impact of pooled funding, use of country sys-
tems, and country-based M&E. The Bank’s policy
on M&E (OP 13.60) likewise emphasizes the use
of country-level M&E systems. Strictly speaking,
attribution is only possible in a tightly designed
randomized trial, which will rarely be feasible in
Bank-supported investment projects or sector
support. The standard should be that sufficient ev-
idence on outputs, intermediate outcomes, and
outcomes should be collected to establish a cred-
ible results chain regarding the link between
Bank-financed investments and sector progress.
Cost of M&E. Borrowing countries have many de-
velopment and poverty-reduction priorities and
worry about the opportunity cost of complex
M&E systems, especially those that are separate
from country systems. They see that large-scale
evaluations have an important global public good
aspect, justifying external (grant) financing in
most cases. This may delay the establishment of
appropriate baseline data and results frameworks
prior to project approval, notably with regard to
impact evaluations.
Operational Complexity. Management agrees
that we need to strive to reduce complexity in
Bank-financed HNP operations. However, HNP
operations can rarely be institutionally or techni-
cally simple, since the desired outcome usually de-
pends on a complex and interacting set of social,
cultural, and institutional factors. Investing in sim-
ple programs would not necessarily provide for last-
ing impact. Management acknowledges, however,
that complexity can be at least partially addressed
by some of the recommendations of the evaluation,
such as thorough technical preparation, including
solid analytical underpinning, political mapping,
high quality at entry including a good results frame-
work, and finally in-depth supervision and paral-
lel policy dialogue with client and partners.
The 2007 Health Sector Strategy and IEGRecommendations. The 2007 strategy actually
cited findings that were similar to the IEG findings,
as would be expected since IEG staff worked with
the strategy team to share preliminary results of
their work. Annex 2 of the Progress Report sum-
marizes how the overall actions being taken to
strengthen the Bank’s HNP support correspond
to IEG’s recommendations (see attached).

1 6 0
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
IFC’s HNP FootprintIFC has considerably increased its footprint in
HNP over the past decade and is prepared to in-
tensify collaboration within the World Bank Group.
During the period under review, much has oc-
curred, both in IFC’s health activities and in the
private health sector in developing countries.
There is a growing acknowledgement of the role
of the private sector in health care in developing
countries. Indeed, in many low-income coun-
tries, the private sector pays for a far larger part
of health care than the public one, and in many
more, it is at least of equal size. Furthermore,
joint research by the World Bank, IFC, and the U.S.
Agency for International Development (USAID)
conducted in Africa showed that very poor peo-
ple often obtain health care in the private sector
and that the public sector often subsidizes health
care for the rich. These findings have led to the
Bank and its partners designing innovative
consumer-focused approaches to addressing
major health financing challenges; such as the
AMFm (Affordable Medicines Facility for Malaria),
which will reduce the price of Artemisinin-based
Combination Therapy (ACT), and therefore out-
of-pocket payments.
In a world of growing, aging populations in de-
veloping countries that are likely to “get old be-
fore they get rich,” both public and private sector
resources are needed to tackle the health needs
of the population, as neither has the resources by
itself. Indeed, all countries’ health systems are fi-
nanced by both sectors; it is only the propor-
tions that vary.
IFC therefore has taken up the challenge to grow
its work to support the private health sector in
developing countries to complement the larger,
more established work done with the public sec-
tor by the World Bank. The period under review
has seen a marked increase in IFC’s activity in
health, the creation of a dedicated Health and
Education Department, and a specific focus on
pharmaceutical and life sciences activities within
IFC’s Global Manufacturing and Services De-
partment. During this time, many lessons have
been learned, specialist knowledge has deep-
ened, and performance has improved by any
measure applied. As in other sectors, IFC con-
tinues to strive for greater development impact,
and we therefore welcome all input that could
help us to do better.

IEG Recommendation Actions to Be Taken How Much & by When By Whom
APPENDIX J : MANAGEMENT RESPONSE
1 6 1
World Bank Management Action Plan
(a) Match project design to countrycontext and capacity and reducethe complexity of projects in low-capacity settings through greaterselectivity, prioritization, and se-quencing of activities, particularlyin Sub-Saharan Africa.
(b) Thoroughly and carefully assessthe risks of proposed HNP supportand strategies to mitigate them,particularly the political risks andthe interests of different stake-holders, and how they will beaddressed.
(c) Phase reforms to maximize theprobability of success.
(d) Undertake thorough institutionalanalysis, including an assessmentof alternatives, as an input intomore realistic project design.
(e) Support intensified supervision inthe field by the Bank and the bor-rower to ensure that civil works,equipment, and other outputs have been delivered as specified,are functioning, and are beingmaintained.
– 75% of all new HNP projects havean intensive Quality EnhancementReview focusing on technical prepa-ration, M&E, and institutional andrisk assessments and mitigationmeasures, starting fiscal year 2010.
– Quarterly reviews of HNP portfolioby HNP Sector Board ongoing.
– Of the Quality Enhancement Re-views conducted, 100% includefocus on risk, starting fiscal year2010.
– Develop and roll out course on proj-ect risk analysis for HNP teams, anddisseminate best practices and les-sons learned, starting fiscal 2010.
– 100% of new HNP projects focusingon health system strengthening orbroadly on health reform to bebased on analytical work, includingpolitical risks and the interests ofdifferent stakeholders, startingfiscal 2010.
– 80% of new HNP projects to bebased on institutional analysis,starting fiscal 2010.
– Training program designed anddelivered, starting fiscal 2010.
– All new HNP projects startingpreparation in fiscal 2010.
– All new HNP projects startingpreparation in fiscal 2010.
– Carry out Quality EnhancementReviews focusing on technicalpreparation, M&E, and institu-tional and risk assessmentsand mitigation measures.
– Reviews of HNP portfolio.
– Concentrate on risk manage-ment and mitigation duringQuality Enhancement Reviews.
– Expand learning on HNP sectorrisk assessments and mitiga-tion strategies.
– Increase analytical work focus-ing on reform for those HNP proj-ects focusing on health systemreform.
– Increase analytic and advisoryactivities for institutionalanalysis, with increasedattention through better policydialogue and analytical work,adapted to country context.
– Learning program focusing onHNP sector institutional andstakeholder analysis.
– Project design to specifyborrower responsibilities forcivil works and equipmentmaintenance.
– Project design to ensure ade-quate recurrent cost budgetingfor civil works and equipmentmaintenance.
HNP Sector Board, HNPHub, and Regional qualityteams.
HNP Sector Board, HNPHub, World Bank Institute.
HNP Sector Board, withtechnical support fromHNP Hub, as needed.
HNP Sector Board, HNP Hub.
HNP Sector Board, HNP Hub.
I. Intensify efforts to improve the performance of the World Bank’s health, nutrition, and population support.
(Table continues on next page)

1 6 2
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
IEG Recommendation Actions to Be Taken How Much & by When By Whom
World Bank Management Action Plan (continued)
(a) Boost population and family plan-ning support in the form of analyticwork, policy dialogue, and financ-ing to high-fertility countries andcountries with pockets of highfertility.
(b) Incorporate the poverty dimensioninto project objectives to increaseaccountability for health, nutrition,and population outcomes amongthe poor.
(c) Increase support to reducemalnutrition among the poor,whether originating in the HNPsector or other sectors.
(d) Monitoring health, nutrition, andpopulation outcomes among thepoor, however defined.
– By fiscal 2010.
– By fiscal 2010.
– 2 health system strengthening proj-ects in high-fertility countries in-clude strengthening of familyplanning delivery, by fiscal 2010.
– 50% of CASs for high-fertility coun-tries, starting fiscal 2010.
– 80% of all new HNP projects incor-porate the poverty dimension, whereappropriate, starting fiscal 2010.
– President’s Regional ReprioritizationFund to hire 6 additional Bank staff(US$4 million committed for fiscalyears 2009–11); Japan TF (US$2 mil-lion with potential for additionalUS$20 million); possibly funds fromother donors that are currently en-gaged in discussions on this issue.
– Global Action Plan designed andagreed with key partners, by fiscal2010.
– Six to 8 analytic and advisoryactivitiess or new investment innutrition by fiscal 2011.
– Annual review of health indicatorsamong the poor, starting fiscal 2010.
– Annual report, starting fiscal 2010.
– Develop guidelines and stan-dard specifications for civilworks and equipment andother health inputs, and theirmaintenance.
– Analytic and advisory activitypolicy note on reproductivehealth, including family planning.
– Incorporate family planninginto health-system strengthen-ing projects.
– In high-fertility countries, in-corporate population and fam-ily planning issue into CAS.
– Ensure adequate attention isgiven to poverty dimensions inproject design and supervision,particularly project develop-ment objectives and key per-formance indicators.
– Scale-up the Bank’s analyticaland investment work andleverage resources from otherdonors.
– Track health outcomes andintervention coverage amongthe poor.
– Publish report on health indica-tors of poor people.
HNP Sector Board, HNPHub.
HNP Sector Board, withtechnical support fromHNP Hub, as needed.
HNP Sector Board, HNP Hub.
HNP Hub
II. Renew the commitment to health, nutrition, and population outcomes among the poor.

APPENDIX J : MANAGEMENT RESPONSE
1 6 3
IEG Recommendation Actions to Be Taken How Much & by When By Whom
World Bank Management Action Plan (continued)
(e) Bring the health and nutrition ofthe poor and the links betweenhigh fertility, poor health, andpoverty back into poverty assess-ments in countries where this hasbeen neglected.
(a) Better define the efficiencyobjectives of its support and howefficiency improvements will beimproved and monitored.
(b) Carefully assess decisions tofinance additional earmarked communicable disease activities in countries where other donors are contributing large amounts ofearmarked disease funding andadditional funds could result indistortion in allocations and ineffi-ciencies in the rest of the healthsystem.
(c) Support improved health informa-tion systems and more frequentand vigorous evaluation of specificreforms or program innovations toprovide timely information for im-proving efficiency and efficacy.
– 90% of all poverty assessments andat least 40% of all CASs shouldassess the health status of the poor,starting fiscal 2010.
– 70% of HNP projects to includedefinition and analysis of improvingHNP sector efficiency, includingdiscussion of efficiency-equitytrade-off, starting fiscal 2010.
– Start fiscal 2010.
– 100% of HNP projects with signifi-cant priority-disease components tomap contributions from other donorsand ensure strengthening of healthsystems, starting fiscal 2010.
– 50% of new HNP projects includestrengthening of country M&Esystems, by fiscal 2010.
– Strategy for global monitoringarrangement designed (in collabora-tion with global partners), by fiscal2009.
– Country assessments in 10 countriesin fiscal 2010.
– Increase inclusion of HNP inpoverty assessments.
– Expanded PAD definition anddiscussion of efficiency objec-tives, measures and monitor-ing framework to be expandedand more explicit.
– Analytic and advisory activitiesto analyze and review experi-ence in improving healthsystem efficiency.
– Closely coordinate proposalsfor Bank support for newdisease-specific programs with other partners.
– Build statistical capacity forclient countries on priority HNPoutcome indicators directlythrough Bank operationsand/or supporting global partner’s country support (e.g., MDGs).
– Continue support of the Inter-national Health Partnership’s(IHP+) efforts to strengthenmonitoring and evaluation andhealth information systems incountries.
– Conduct country assessmentsof health information systems.
HNP Sector Board, withtechnical support fromHNP Hub and PREM, asneeded.
HNP Sector Board, HNP Hub.
HNP Sector Board, withtechnical support fromHNP Hub, as needed.
HNP Sector Board, HNP Hub.
III. Strengthen the World Bank Group’s ability to help countries to improve the efficiency of their health systems.
(Table continues on next page)
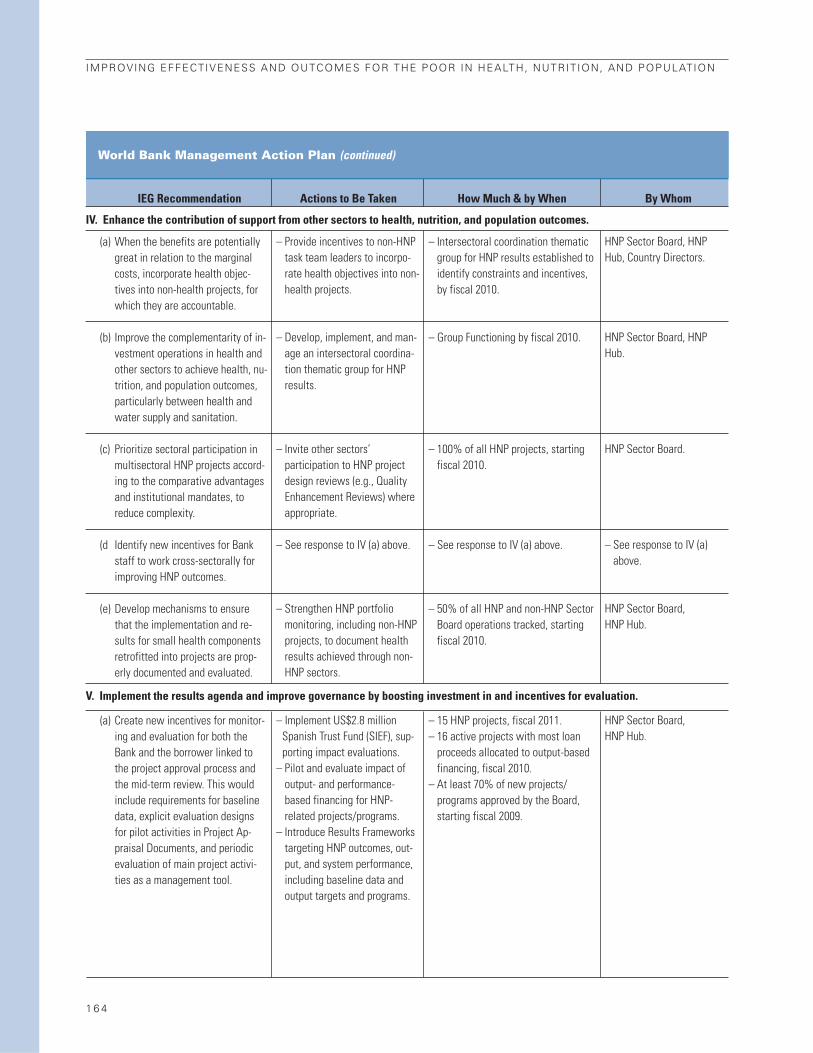
1 6 4
IMPROVING EFFECTIVENESS AND OUTCOMES FOR THE POOR IN HEALTH, NUTRITION, AND POPULATION
IEG Recommendation Actions to Be Taken How Much & by When By Whom
World Bank Management Action Plan (continued)
(a) When the benefits are potentiallygreat in relation to the marginalcosts, incorporate health objec-tives into non-health projects, forwhich they are accountable.
(b) Improve the complementarity of in-vestment operations in health andother sectors to achieve health, nu-trition, and population outcomes,particularly between health andwater supply and sanitation.
(c) Prioritize sectoral participation inmultisectoral HNP projects accord-ing to the comparative advantagesand institutional mandates, toreduce complexity.
(d Identify new incentives for Bankstaff to work cross-sectorally forimproving HNP outcomes.
(e) Develop mechanisms to ensurethat the implementation and re-sults for small health componentsretrofitted into projects are prop-erly documented and evaluated.
(a) Create new incentives for monitor-ing and evaluation for both theBank and the borrower linked tothe project approval process andthe mid-term review. This wouldinclude requirements for baselinedata, explicit evaluation designsfor pilot activities in Project Ap-praisal Documents, and periodicevaluation of main project activi-ties as a management tool.
– Intersectoral coordination thematicgroup for HNP results established toidentify constraints and incentives,by fiscal 2010.
– Group Functioning by fiscal 2010.
– 100% of all HNP projects, startingfiscal 2010.
– See response to IV (a) above.
– 50% of all HNP and non-HNP SectorBoard operations tracked, startingfiscal 2010.
– 15 HNP projects, fiscal 2011.– 16 active projects with most loan
proceeds allocated to output-basedfinancing, fiscal 2010.
– At least 70% of new projects/programs approved by the Board,starting fiscal 2009.
– Provide incentives to non-HNPtask team leaders to incorpo-rate health objectives into non-health projects.
– Develop, implement, and man-age an intersectoral coordina-tion thematic group for HNPresults.
– Invite other sectors’ participation to HNP projectdesign reviews (e.g., QualityEnhancement Reviews) whereappropriate.
– See response to IV (a) above.
– Strengthen HNP portfoliomonitoring, including non-HNPprojects, to document healthresults achieved through non-HNP sectors.
– Implement US$2.8 millionSpanish Trust Fund (SIEF), sup-porting impact evaluations.
– Pilot and evaluate impact ofoutput- and performance-based financing for HNP-related projects/programs.
– Introduce Results Frameworkstargeting HNP outcomes, out-put, and system performance,including baseline data andoutput targets and programs.
HNP Sector Board, HNPHub, Country Directors.
HNP Sector Board, HNPHub.
HNP Sector Board.
– See response to IV (a)above.
HNP Sector Board, HNP Hub.
HNP Sector Board, HNP Hub.
IV. Enhance the contribution of support from other sectors to health, nutrition, and population outcomes.
V. Implement the results agenda and improve governance by boosting investment in and incentives for evaluation.