cpc 5 kelsey hultman ryan fader jeremy carey nichole boettcher steve aldrich marsha erickson suzanne...
TRANSCRIPT

CPC 5
Kelsey HultmanRyan FaderJeremy CareyNichole BoettcherSteve AldrichMarsha EricksonSuzanne EspensonMatthew Geeslin

Chief Complaint“My chest hurts and I can’t catch my breath”

Presenting Symptoms• A 68 yro woman brought to ER one night in Feb by her
daughter who is concerned b/c her mother is experiencing chest pain.
• The patient has been ill for the past 3 days with malaise, fever, and cough.
• The cough was initially non-productive, but over the past 2 days she is producing occasional green phlegm in scant amounts.
• She reports she has been feeling weak, with a fever "on and off" for the past 2 days.
• She denies rigors and chills. • During this time, she began taking acetaminophen for
pain and fever as well as an OTC cough medication

Past Medical History•Type 2 diabetes for 10 years with diabetic
retinopathy and diabetic nephropathy•Hyperlipidemia•Hypertension•Past cholecystectomy
Medications: •Glipizide 5 mg po bid•Atorvastatin 10 mg po qd•Lisinopril 10 mg po qd
Allergies: None

Habits•Smoking: quit 15 yrs ago after a 30 pk yr hx•Alcohol: none •Travel: returned from a trip to Quebec last
week with an 8 hour stopover in Toronto. •Family Hx: mother died of diabetes at age
83, father of an MI at age 45 •Social History: retired secretary, widowed
for three years. Lives alone in her own home.

ROS
Negative:• weight loss • HA• sinus congestion• Earache• sore throat• Hemoptysis• N/V• Arthralgia• Myalgia• rash
Positive:• poor appetite for the past
week
Additional:• no flu shot in past 2 yrs• never had a pneumovax
Physical Exam• Well-nourished female who is coughing & SOB• Vitals: BP: 130/80; HR: 112 & regular; RR: 28; T: 39 ⁰C • HEENT: PERRL, fundi showed soft exudates & old hemorrhages. TM's
clear, throat w/o exudates. No sinus tenderness. • Neck: Supple, trachea midline; thyroid normal size w/o nodules; no
bruits; no JVD • Chest: Bronchial breath sounds auscultated at right base,
otherwise clear to auscultation and percussion; right base has egophony and increased tactile fremitus; no wheezing
• Heart: S1 & S2 are normal, no S3, S4 or murmurs. PMI at MCL • Abdomen: Bowel sounds present, no organomegaly or tenderness, past
RUQ scar well healed. • Musculo-skeletal: No clubbing or edema • Skin: Neurological: Alert &oriented x 3, no lateralizing findings
What do you think?

Differential DiagnosisPulmonary:• PE• Bacterial Infection (Pneumonia)• Viral Infection (Influenza)• TB• Malignancy• Inhalation of Irritant/Chemical
Cardiovascular: • MI/CHF• Aortic Dissection
Others:• Anemia• Hypothyroid• Metabolic Acidosis• Anxiety & Hyperventilation

TESTS
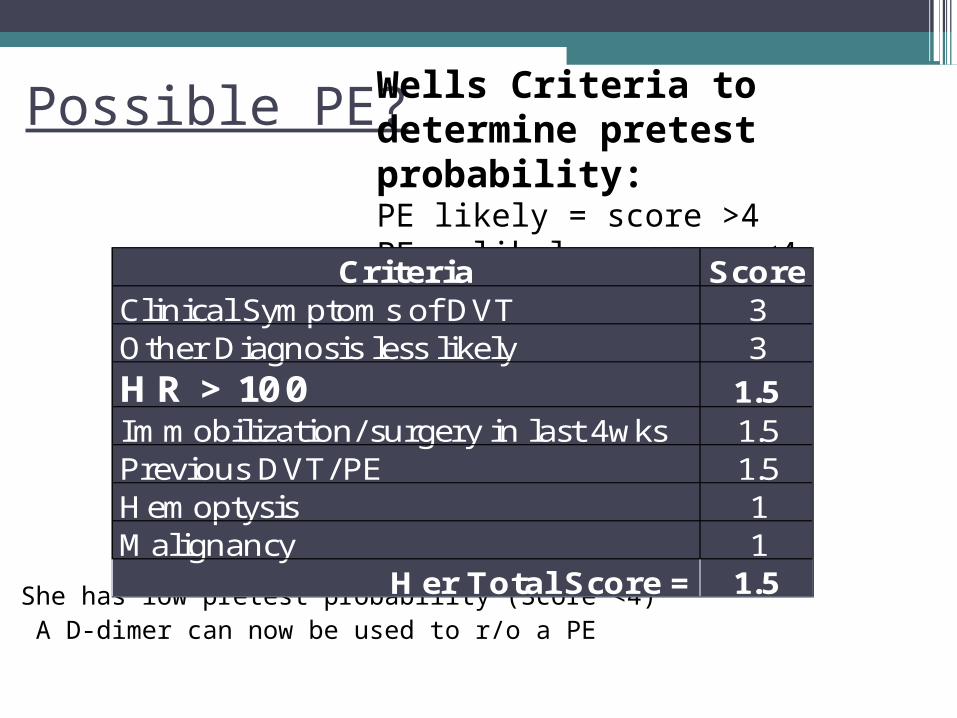
Possible PE?
She has low pretest probability (Score <4) A D-dimer can now be used to r/o a PE
Wells Criteria to determine pretest probability:PE likely = score >4 PE unlikely = score <4
Criteria ScoreClinical Symptoms of DVT 3Other Diagnosis less likely 3HR > 100 1.5Immobilization/ surgery in last 4wks 1.5Previous DVT/PE 1.5Hemoptysis 1Malignancy 1
Her Total Score = 1.5

D-Dimer - $109
•Fibrinogen split products: normal Neg at 1:4 dilution
•Low pretest probability + negative D Dimer = r/o PE

ECG - $78
CAD risk factors: - Diabetic- Family history of M I- Hx of smoking
ECG Test Results: NORMAL MI & CHF less likely; however, 1/3 of
patients who have an MI have a normal ECG. Keeping this in mind, we order a chest X-ray.
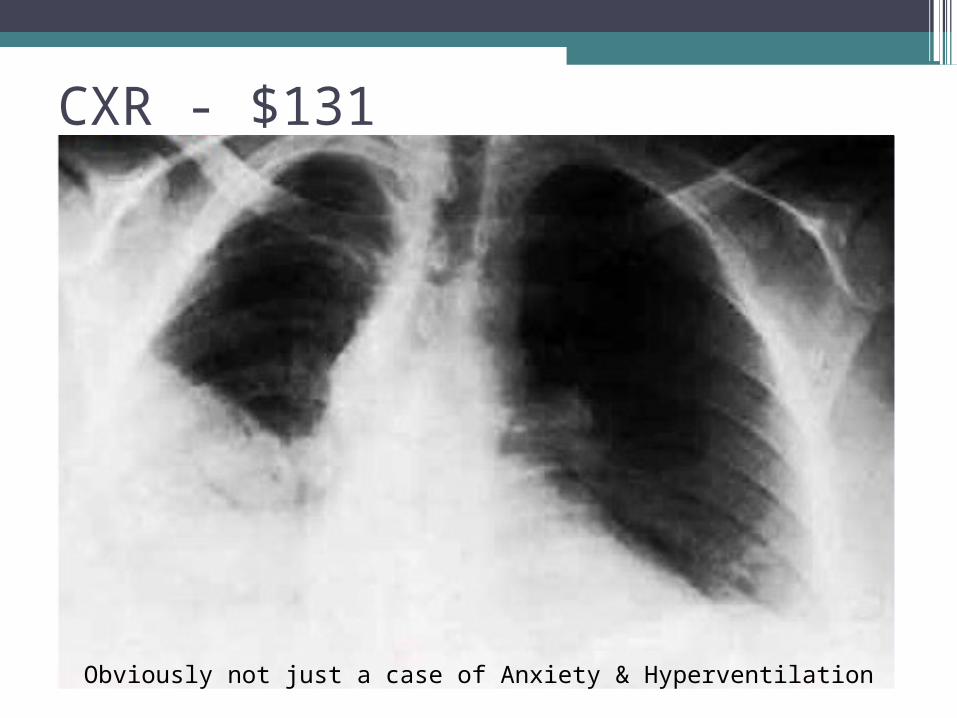
CXR - $131
Obviously not just a case of Anxiety & Hyperventilation
CT - $494
•Middle and lower lobe infiltrate•No mass present
Justification – not very good!•Daughter’s concern•hx of smoking•couldn’t tell if there was a mass on the xray•We should have treated first with an
antibiotic and then taken another xray

CBC (r/o infection) - $41
• Low MCV polycythemia, Pb, Fe deficiency, Thalassemia
Result NormalAuto Basophils 2.97% 0-1% highAuto Eosinophils 7.47% 1-3% highAuto Granulocytes 52.25% 40-76%Auto Lymphocytes 22.56% 22-44% lowAuto Monocytes 6.44% 3-7%Automated Differential %'s normalErythrocyte count (RBC) 4.39 10 2̂1/ l 4.15-4.87Hematocrit (HCT) 47.42% 37-47%Hemoglobin (HGB) 13.46 g/dl 12.2-14.7 r/o AnemiaLeukocyte count (WBC) 16.0 10 9̂/ l 4500-1100 highMean corpuscular volume 72.06 76-100 lowPlatelet count 282 10 9̂/ l 150-450RDW 11.93 11.5-14.5

ABG’s (Assess Ventilation) - $86
Tachypnic trying to get O2 & breathing off CO2
ABG'S RESULT NORM ANALYSIS
HCO3 22 mEq/L 22-26 Low normal
O2 Sat 89.00% 94-100 Hypoxic
pCO2 25mmHg 35-45 Hypocapnic
pH 7.50 7.35-7.45 Alkalotic
pO2 63 mmHg 75-100 Hypoxemia

Calculating A-a difference
PAO2 = PIO2 – (PACO2/R) = 150mmHg – (25mmHg/.8)
= 125.8 mmHg
A-a = PAO2 – PaO2 = 55.75mmHg – 63mmHg
= 55.75 mmHg
A-a difference > 10mmHg cannot just be due to hypoventilation

Possible causes of A-a difference• Shunt• V/Q mismatch•Diffusion Block seems most likely based on the infiltrate in the lung

Sputum Culture (What is the infiltrate?)- $43
•Candida albicans: normal •Gram stain: normal •Strep: normal
FYI: This is not a helpful testSensitivity of Sputum gram stain for
streptococcus pneumoniae is 50-60%

Electrolytes- check AB balance - $80
Electrolyte mEq/l Normal
Carbon Dioxide 22.99
Chloride 103.71 96-106
HCO3 30.64
Potassium 5.01 4.8
Sodium 144.08 135-145
•Serum HCO3 is more reliable than ABG HCO3.
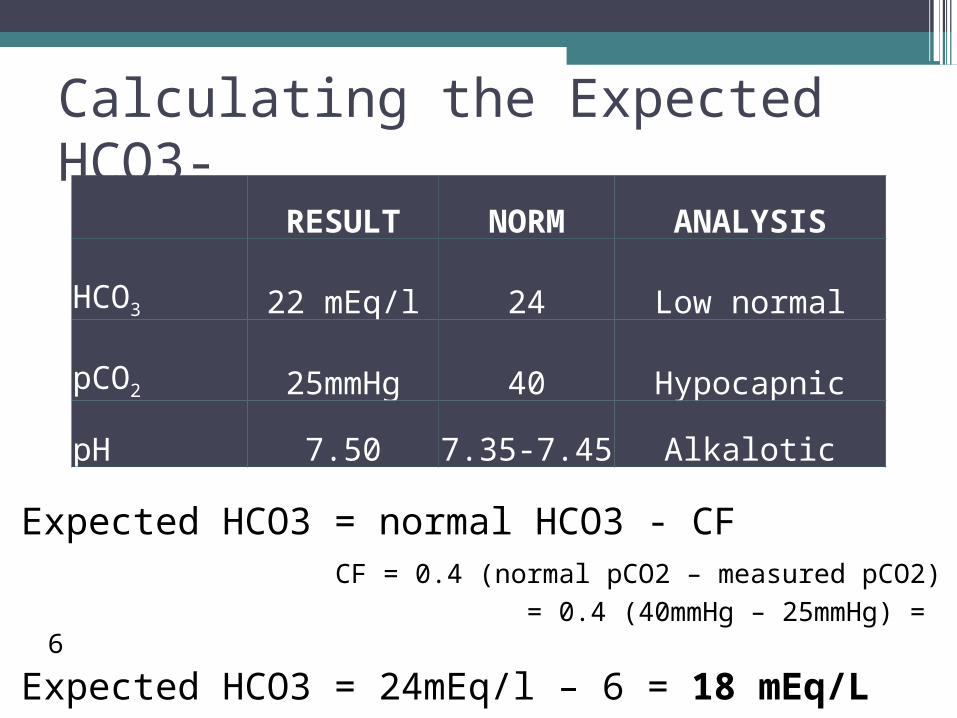
Calculating the Expected HCO3-
Expected HCO3 = normal HCO3 - CF CF = 0.4 (normal pCO2 – measured pCO2)
= 0.4 (40mmHg – 25mmHg) = 6
Expected HCO3 = 24mEq/l – 6 = 18 mEq/L
RESULT NORM ANALYSIS
HCO3 22 mEq/l 24 Low normal
pCO2 25mmHg 40 Hypocapnic
pH 7.50 7.35-7.45 Alkalotic
Creatinine – check kidney fx - $20•Creatinine - serum: 1.8 mg/dl
normal values for a female = 0.5 – 1.0
• This is abnormal but for someone with known diabetic nephropathy, is this baseline?
• Normally it’s filtered in the kidney; if filtering is deficient, creatinine levels rise in the blood.
• Creatinine levels can be used to calculate the creatinine clearance rate (CrCl), which is a good estimation of GFR.
Fasting Glucose - $20
•Glucose: 306 Fasting:mg/dl
Uncontrolled diabetes? Or a result of Infection? Stress?
Keep in mind High glucose = nice environment for bacteria


Community Acquired Pneumonia
• Most commonly caused by Streptococcus Pneumoniae• Other causes: H. Influenzae, Klebsiella pneumoniae, Staphylococcus aureus, Pseudomonas aeruginosa, Mycoplasma pneumoniae (Atypical)

Pneumonia outcomes
•Resolution: most common•Abscess formation•Empyema•Organization (scarring)•Bacteremia dissemination to kidneys,
spleen, heart and brain•Death

RISK FACTORS POINTS PATIENT'S PTSDemographic Factors
age for men age age for women age - 10 58nursing home resident 10 coexisting illnesses neoplastic disease (active) 30 chronic liver disease 20 CHF 10 cerebrovascular disease 10 chronic renal disease 10 10
physical exam findings altered mental status 20 RR >= 30/min 20 Systolic BP <90 mmHg 20 Temp < 35 C or >= 40C 15 Pulse >= 125 beats/min 20
Lab & radiographic findings arterial pH <7.35 30 BUN >=30mg/Dl 20 Na <130mmol/L 20 Glucose >= 250 mg/dL 10 10Hematocrit <30 % 10 partial pressure of arterial oxygen <60mmHg 10 10Pleural Effusion 10
Total Points = 88
Do we hospitalize?- Assess her risk

Stratification of Risk Score
Risk Class No. of points Mortality % RecommendationsI No predictors 0.1 OutpatientII ≤ 70 0.6 OutpatientIII 71-90 2.8 Inpatient (brief)IV 91-130 8.2 Inpatient V > 130 29.2 Inpatient

Patient with Productive Cough
Sputum Sample No sputum Sample
Rapid test IDs likely pathogen (s)
No Pathogen Identified Treat Empirically
Treat with Pathogen – appropriate agent
Treatment
•Hospitalize/Admit to medical floor•Oxygen (binasal cannula) – 2 Liters•Antibiotics• Insulin Management•Monitor Intake and Output to determine if
fluid is necessary. Currently no indications for fluid (negative for hypotension, N/V, weight loss).

Pharmacy Frame of Reference•68 y.o. Caucasian F admitted with CAP•Pertinent Labs: SCr: 1.8 (DM2 with
Nephropathy), wt. n/a, Glc 306•Admission Meds:
▫Glipizide 5 mg PO BID▫Atorvastatin 10 mg PO QD▫Lisinopril 10 mg PO QD
•Key issues: Antibiotic selection, glucose control
Basic Approach to ABx Selection•Obtain cultures prior to starting therapy•Empiric therapy based on likely
pathogens•Calculate CrCl•Review all concomitant drugs and
supplements•Narrowest spectrum of activity preferred

Creatinine Clearance
•Important consideration in drug dosing – CrCl ~ GFR
•Cockcroft Gault equation – preferred for drug dosing (need wt. to calculate)
•MDRD equation derived for CKD staging : 186 x SCr-1.154 x Age -0.203 x 0.742 = 30 mL/min/1.73m2
Antibiotic Therapy • Non-ICU hospitalized CAP
▫ Beta-lactam + macrolide OR▫ Fluoroquinolone alone
• Levofloxacin▫ Good Strept, Gram neg, atypical coverage▫ Less $ than 2-drug therapy▫ Drawback: limited Staph coverage (but low incidence for
CAP)▫ 750 mg IV q 48H (nl renal fxn allows q 24H)▫ Switch to po upon clinical improvement (same dose)▫ Duration of therapy:
Minimum of 5 days d/c when afebrile for 2-3 d, no supplemental O2, clinically stable

Monitoring ABx Therapy
•s/s initial improvement expected in 2-3 d (cough, sputum, tachypnea, malaise, fever,WBC,O2 dependence)
•If no resolution of sx in 2-3 d, reassess ABx therapy
•Culture results also help tailor therapy•Common adverse effects: GI, H/A,
insomnia, glycemic control

Diabetes Management•Glucose control important for Pneumonia
recovery•Options: SSI, Basal/Bolus insulin, oral agents•Selection: Glargine (basal) and Glulisine
(bolus)▫d/c glipizide
•Est. Insulin Requirements: 0.5 units/kg/day; give 50% basal, 50% bolus divided with meals.
•QID glucose monitoring with SSI for BG>140

Prior to Discharge
•Monitor BP control on lisinopril•Continue atorvastatin (check historical
lipid control)•Resume glipizide and d/c insulin•Influenza vaccine•Pneumonia vaccine

Quiz
What is the most common cause of CAP?
A. streptococcus pneumoniaeB. klebsiella pneumoniaeC. staphylococcus aureusD. pseudomonas aeruginosa
Recommended Antibiotic Therapy for a non ICU hospitalized patient with CAP?
A. Penicillin GB. ChloramphenicolC. VancomycinD. Beta lactam + macrolide E. Fluoroquinolone aloneF. D and E

Which X ray finding is most consistent with CAP?
A. Lobar infiltrateB. Spontaneous pneumothoraxC. Coin LesionD. Lacey Interstitial Pattern
Which fluorinated quinolone is the best choice for treatment of pneumonia?
A. LevofloxacinB. NorfloxacinC. MoxifloxacinD. CiprofloxacinE. Notafloxacin

What presenting symptom is not typical of bacterial CAP?
A. Productive CoughB. FeverC. Insidious OnsetD. Shortness of Breath

Most common outcome of CAP?A. EmpyemaB. ResolutionC. DeathD. Abscess formation

Any Questions?