creating and implementing a blenderized tube feeding1cb444df-77c3-4d94-82fa-e366d7d6ce04}/… ·...
TRANSCRIPT

Don’t Fear the Blender: creating and implementing a blenderized tube feeding
Objectives
• Review the benefits and challenges associated with blenderized
tube feeding (BTF)
• Provide a rubric for developing a new BTF recipe and plan for
transition
• Outline excellent available resources for clinicians and
caregivers
• Overall goal minimize apprehension around BTF
2
3
4
An Evolving Perspective?
4
• 2014 ASPEN survey involving 244 pediatric RDs regarding
experience in providing blended food via g-tube1
– 70% reported positive outcomes with BTF
– 58% recommend and use blended food via gtubes
– 12% don’t use BTF
– 70% attribute this to parent request
– 23% due to feeding intolerance with commercial formulas
• Older RDs were more familiar with BTF but less likely to use
them
The Benefits
• Physiologic
• May aid in transition to oral diet
• A natural product
– Consider: food components vs. whole foods
– Increased variety
• Improved GI symptoms2-4
– Decreases gagging/retching
– Decreases reflux symptoms
– Constipation or diarrhea
– Improve quality of life
5
The Benefits
• Prospective cross-sectional study in 54 enterally fed adults4
– 50% used BTF
– 80% expressed a desire to use BTF
• Motivation for using BTF
– Natural (43%)
– Eating what the family eats (33%)
– Better tolerance (30%)
6
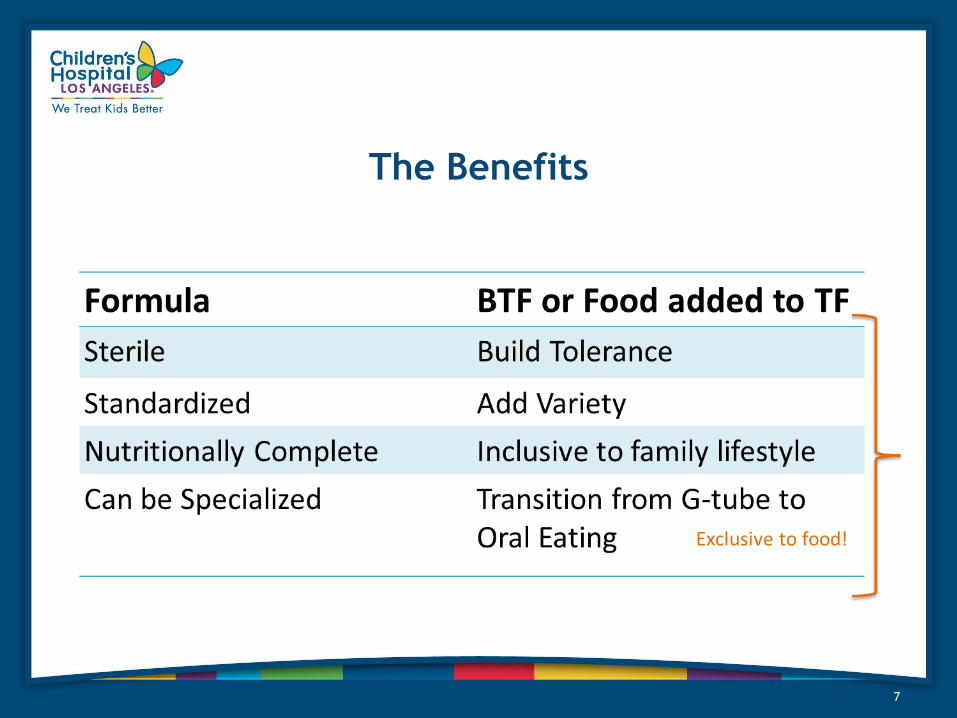
The Benefits
7
The Challenges
• Time commitment
– Caregiver: meal planning, daily/weekly preparation, follow-up
appointments
– Clinician: office visits, recipe analysis to ensure DRIs are met
• Sensitivity to volume, gastric dysmotility
• Small french size (< 14)
• Lack of support from medical team
• Acute illness or immunosupression
• Existing food allergies/intolerances
8
The Deal Breakers
• Patient age < 4-6 months
– AKA homemade infant formula (GROW 2016 topic?)
• Inadequate kitchen for safe prep and storage
• History of poor adherence/follow-up
• Post-pyloric feeding
9

Creating a recipe from scratch!
10
Start with PROTEIN
• Protein g/kg/cm goals from individualized assessment
• Compleat Pediatric is 15% protein with 38 g pro/1L
• Choose a solid and a liquid for viscosity and to meet 80-90% total
protein needs
• 10-20% max protein will come from cereals, legumes, nuts
– Solids: infant stage 2 chicken/turkey (7-8g per 2.5 oz jar), soft tofu
– Liquid: formula, 2% lactaid, yogurt, bone broth, alternative milks
11
Choose your CARBOHYDRATES
1. Fruits and vegetables: choose from both the Vit A & Vit C groups
– Vitamin A: squash, carrots, sweet potato, peaches, apricots
– Vitamin C: applesauce, pears, green peas, green beans, spinach
– Consider GI concerns: prunes, green beans
– Note: adds bulk without adding significantly to calorie delivery
2. Thickening agents: grains for additional kcal, cho, fiber
– Dry infant cereals: gerber oatmeal, other gerber cereals
– Whole grain based: soaked cheerios, steamed grains, white rice,
quinoa, barley, etc
12
Choose your FAT
• Important source of kcal
• Compleat Pediatric is 34% fat, in-pt recipes are ~30%
• Lower saturated fat vegetable oils: olive, canola, flax
• Consider avocado for added fiber
• Consider anti-inflammatory omega-3s
• Include sardines or salmon, 1x week
• Walnuts, hemp (hulled) and chia, caution with blending
• Also remember to choose other food items that are higher in fat to boost
kcal, ie whole fat greek yogurt or barley
13
14
Calculate Fluid
• If unable to use nutrient analysis software, free water can be
easily calculated if using infant purees, standard formulas or milks
• Calculate total ounces of pureed fluid-containing infant foods
(meats, fruits, vegetables, yogurt)
– Multiply by 0.75, most infant foods contain ~75% free water
• Add free water from formula and milk (typically ~85%)
15
16
17
Caregiver Education – getting started
• First, a great BLENDER
– Vitamix
– Blendtec
– Nutribullet
– Magic Bullet
– My Blend
• Measuring utensils or scale
• Thermometer
18
Caregiver Education
• Preparation
– Wash hands, sanitize work space
– Assemble equipment (utensils, measuring cups, blender, recipe)
– Cook meat, chicken, poultry, eggs to appropriate temperatures
– Cook grains, vegetables as appropriate
• Blending
– Cut up whole foods
– Blend solids first, gradually increase speed
– Add liquids gradually while evaluating consistency
– Some foods don’t blend well
19
Caregiver Education
• Storage
– Cover and store in the refrigerator
– Refrigerated blended feeds should be used within 24-48 hrs
– Freezer stored foods can be stored for up to 3 months
20
Caregiver Education
• Foods to use with caution:
– Low moisture content (dried fruit, chicken breast)
– High insoluble fibers (corn, nuts, seeds)
– Acidic foods (citrus, pineapple)
– Added sugars and supplements (increase osmotic load)
– High soluble fibers (can increase viscosity, clogging)
21
BTF - is it working?
• Growth monitoring
• Consider micronutrient needs
– Calcium, iron, sodium, zinc
– Can use software to analyze
– Consider MVI + variety offered
• GI symptoms
• Hydration status
22
Miscellany
• Consider the supplemental BTF when getting started
• It’s ok to not know – caregivers become your best resource
• Emergency Preparedness (in a pinch or for travel )
– Nestle Compleat line
– Liquid Hope + Real Food Blends
• Provide a letter of medical necessity
– Blendtech offers a free blender
– Vitamix offers a reduced-cost refurbished blender
23
Additional Resources
• Blenderized Tube Feeding: Suggested Guidelines to Clinicians5
• The Use of Blenderized Tube Feedings in Pediatric Patients6
• Foodfortubies.org
– Non-profit resource group: forum, recipe ideas, education
• Mealtimenotoins.com
– The Homemade Blended Formula Handbook by Marsha Dunn Klein,
MEd, OTR/L and Suzanne Evans Morris, PhD, CCC-SLP
• Seattle Children’s patient/family education materials
• Oley Foundation
24
References
25
1. Johnson, Teresa W., Amy Spurlock, and Leah Pierce. "Survey Study Assessing Attitudes and Experiences
of Pediatric Registered Dietitians Regarding Blended Food by Gastrostomy Tube Feeding." Nutrition in
Clinical Practice 30.3 (2015): 402-405.
2. Novak, Patricia, et al. "The use of blenderized tube feedings." ICAN: Infant, Child, & Adolescent
Nutrition 1.1 (2009): 21-23.
3. Bills, Hannah Bowman. USE OF HOMEMADE BLENDERIZED FORMULA IN GASTROSTOMY TUBE
DEPENDENT PEDIATRIC PATIENTS WITH FEEDING INTOLERANCE: A SERIES CASE STUDY. Diss. The Ohio
State University, 2015.
4. Hurt, Ryan T., et al. "Blenderized Tube Feeding Use in Adult Home Enteral Nutrition Patients A Cross-
Sectional Study." Nutrition in Clinical Practice(2015): 0884533615591602.
5. Escuro, Arlene A. "Blenderized Tube Feeding: Suggested Guidelines to Clinicians." PRACTICAL
GASTROENTEROLOGY (2014).
6. Schoenfeld, Laura. The Use of Blenderized Tube Feeding in Pediatric Patients: Evidence and Guidelines for
Dietetic Practice (Chapel Hill, North Carolina). Diss. University of North Carolina at Chapel Hill, 1913.