ct urographyfrom seeing to understanding
TRANSCRIPT

CT UROGRAPHYFROM SEEING TO UNDERSTANDING
Dr. Hazem Abu Zeid YousefLecturere of Radiodiagnosis
Faculty of MedicineAssiut University

Although all imaging modalities play an important role in imaging the urinary tract, CT urography represents the most comprehensive imaging examination of the urinary tract. It provides a single noninvasive examination of the kidneys, ureters, and bladder in one test. As a result, CT urography is the current modality of choice for evaluation of painless gross or microscopic hematuria. CT urography allows for identification of stones, renal parenchymal masses, and urothelial abnormalities.

APPROACHES TO CTU For a CT examination to allow for
comprehensive urinary tract imaging, it must be able to adequately detect urinary tract calculi, renal masses, and renal collecting system, bladder, and ureteral abnormalities.

TECHNIQUES OF CTU
• SINGLE BOLUS 3 OR 4 PHASES TECHNIQUE
• SPLIT BOLUS TECHNIQUE
• SALINE HYDRATION
• IV DIURETICS.

INDICATIONS FOR MDCTU

Due to the radiation intensive nature of MDCTU, some investigators have suggested that this study be performed only on patients who are preidentified by urologists as being at a high risk for having urinary tract pathology, especially transitional cell carcinoma. When these restrictions are enforced, MDCTU is generally performed on patients more than 40 years of age and patients with at least one of the following: a history of transitional cell carcinoma (and who are therefore likely to have recurrences or metachronous tumors), positive urine cytology, previous equivocal imaging studies, and persistent symptoms (e.g., ongoing hematuria).

In contrast, others suggest performing MDCTU as a screening test on any patient who presents with hematuria. According to these authors, MDCTU is already in a position to replace EU completely. Regardless of the differing recommendations as to when MDCTU should be performed, all investigators are extremely enthusiastic about its potential. Even those advocating limited use have stated that with a few additional radiation-restricting modifications in CT hardware and changes in CT technique, MDCTU is poised to make EU obsolete in the very near future.

NORMAL ANATOMY

NORMAL ANATOMY
FRONTAL (ANTERIOR) VIEW OF VR IMAGES

MIP IMAGE (POSTERIOR VIEW) VR DOUBLE DENSITY IMAGE (POSTERIOR VIEW)

NORMAL VARIANTS AND CONGENITAL ANOMALIES

NORMAL PAPILLARY BLUSH

PROMINENT RENAL PAPILLA

COMPOUND CALYX

PTOTIC KIDNEY

ECTOPIC KIDNEY

VR IMAGE MIP IMAGE

HORSESHOE KIDNEY

DOUPLEX LEFT COLLECTING SYSTEM WITH ECTOPIC UPPER MOIETY URETER


BENIGN TUBULAR ECTASIA

CROSSED FUSED ECTOPIA

UROLITHIASIS

CASE (1)
NON ENHANCED CT SHOWING BILATERAL RENAL PELVIS CALCULI WITH MARKED PYELITIS.
ENHANCED CT SHOWING GOOD ENHANCEMENT.

MIP; THE STONES ARE WELL-SEEN WITHIN THE OPACIFIED RENAL PELVIS.

CASE (2)
THICK SLAP MIPBILATERAL RENAL AND UB STONES
CORONAL IMAGESSHOWING MARKED PYELITIS OF THE LEFT KIDNEY

MIP; THE STONES ARE WELL-SEEN WITHIN THE OPACIFIED RENAL PELVIS. MULTIPLE UB STONES.

CASE (3)
PRE AND POST CONTRAST SCANS.MARKED STRANDING OF THE PERINEPHRIC FAT ON THE RIGHT SIDE.

SURFACE SHADED DISPLAY (SSD). THE LUMEN AND THE STONES COULD NOT BER SEEN

CASE (4)
ACUTELY OBSTRUCTEDLEFT KIDNEY WITH PERINEPHRIC COLLECTION (FORNICEAL RUPTURE).

CURVED REFORMATSSHOWING 3 LOWER URETERIC STONES.

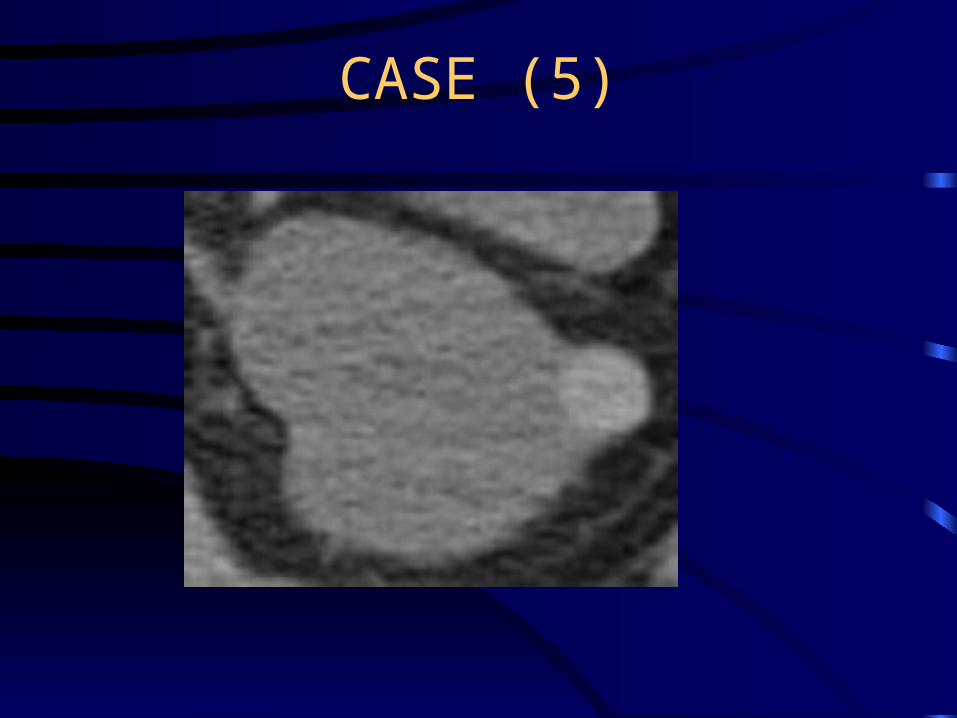
CASE (5)
CURVED REFORMATLOWER URETERIC STONE
CAUSING MILD HYDRONEPHROSIS
DOUBLE DENSITY VR IMAGETHE STONE IS DEMONSTRATED
AGAINST THE UNDERLYINGBONE

CASE (6)
BILHARZIAL CALCIFICATION OF THE LEFT LOWER URETER WITH LOWER URETERIC STONE.

CASE (9)
MEDULLARY NEPHROCALCINOSIS


RENAL INFECTIONS

CASE (1)
MULTIFOCAL NEPHRONIA

CASE (2)
OBSTRUCTED INFECTED KIDNEYENLARGED LEFT KIDNEY WITH MARKED STRANDING OF THE
PERINEPHRIC FAT AND OBSTRUCTING PELVIC CALCULUS

DOUBLE DENSITY VR IMAGE SHOWING THE OBSTRUCTING CALCULUS

CASE (3)
RIGHT UPPER POLAR ABSCESS

CASE (3)
RIGHT UPPER POLAR ABSCESS

DELAYED FILLING OF THE ABSCESS

RENAL SOLs

CASE (1)
NON ENHANCED CT ENHANCED CT

DELAYED FILLING OF CALYCEAL DIVERTICULUM

CASE (2)

SIMPLE (BOSNIAK TYPE I) RENAL CYST

CASE (3)

MULTILOCULAR PARAPELVIC CYST WITH STRETCHING OF THE MAJOR CALYCES

CASE (4)

BOSNIOAK TYPE II CYST WITH THIN CALCIFIED RIM AND INTRACYSTIC SEPTUM
(THANKS FOR THE SUBMILLEMETRIC SLICE THICKNESS)
CASE (5)

INITIALLY HYPERDENSE SIMPLE CYST (BOSNIAK TYPE II)

CASE (6)

BOSNIAK TYPE III CYSTTHICK ENHANCING INCOMPLETE
SEPTUM AND IRREGULAR OUTLINES

CASE (7)

BOSNIAK TYPE IV CYSTTHICK ENHANCING MURAL NODULE

CASE (8)

SOLID UPPER POLAR MASS CLEARLY DEMONSTRATED IN CORONAL IMAGES

CASE (9)


MALIGNANT LOWER POLAR LEFT RENAL MASS WITH ENHANCING MALIGNANT THROMBUS WITHIN THE IVC
AND SECONDARY VARICOSITIES OF THE LEFT TESTICULAR VEIN.

CASE (10)
MALIGNAT SUPRARENAL MASSWITH LIVER METASTASES


DISPLACED LEFT KIDNEY WITH DOUPLEX RIGHT COLLECTING SYSTEM

INTRARENAL COLLECTING SYSTEM

CASE (1)
PRE AND POST CONTRAST MIP IMAGESTUBULAR DILATATION WITH TINY
CALCULI WITHIN THE DILATED TUBULES(MEDULLARY SPONGE KIDNEY)


CASE (2)

ACUTE PAPILLARY NECROSISYOUNG FEMALE PATIENT WITH PAINLESS HEMATUREA AND HISTORY OF ANALGESIC ABUSE

CASE (3)

MALIGNANT UROTHELIAL NEOPLASM OF THE UPPERE CALYX IN A MIDDLE AGED MALE WITH PAINLESS HEMATUREA

CASE (4)

ANOTHER EXAMPLE OF MALIGNANT UROTHELIAL NEOPLASM OF THE UPPERE CALYX

URETERS
AS A RULE;MALIGNANT URETERIC NEOPLASMS CHARACTERISTICALLY CAUSE DILATATION OF THE URETER BOTH PROXIMAL AND DISTAL TO THE LESION.

CASE (1)


CASE (2)


CASE (3)


CASE (4)


CASE (5)


CASE (6)

FIBROVASCULAR POLYP OF THE URETER

URINARY BLADDER

CASE (1)


CASE (2)
EXTRAVESICAL PARARECTAL MASS


CASE (3)
URACHUS

RENAL ARTERY ASSESSMENT


THANK YOU