current perspectives on medication development for methamphetamine dependence steve shoptaw january...
Post on 20-Dec-2015
218 views
TRANSCRIPT
Current Perspectives on Medication Development for Methamphetamine
Dependence
Steve ShoptawSteve Shoptaw
January 5, 2006January 5, 2006

Key Points
• Acute Symptoms vs Abuse/dependence
• Mechanism vs syndromic approach
• Medications with promise for other stimulants may work for methamphetamine
• New directions – bupropion
Acute Symptoms
• Intoxication and psychotic symptoms can be managed efficiently using current medications– Benzodiazepine +/- short and fast acting
antipsychotics
• Medical consequences present more challenging medical management
• Objective is resolution of symptoms; stabilize patient

Risperidone/Haloperidol• Controlled evaluation
of risperidone (.75mg) and haloperidol (3mg) among healthy volunteers
• Placebo-controlled, 2 (treatment agent) x 2 (meth 20mg or placebo) design
• Active drugs caused mild sedation compared to placebo
• Neither drug blocked subjective effects of methamphetamine
Wachtel et al., 2002Wachtel et al., 2002
Thus, acute meds unlikely to have long lasting effects for Rx!Thus, acute meds unlikely to have long lasting effects for Rx!

Abuse and Dependence
• Treatment targets– Instilling of abstinence– Prevention of relapse– Improve mood and cognition– Reduce craving
• Pharmacology of methamphetamine associated with use patterns complicates medication development

Prefrontal CortexPrefrontal Cortex
ThalamusThalamus
Nuc AccumbensNuc Accumbens
Substantia NigraSubstantia NigraSubthalamic NucleiSubthalamic Nuclei
Globus PallidusGlobus Pallidus
High High Affinity D2 Affinity D2 receptor loopreceptor loop
Low Low Affinity Affinity D1 D1 receptor receptor looploop

Important Neuropharm Considerations
• High dose (5-10mg/kg) – D2 mediated– Enters cell via passive diffusion– Reverse transporters (DAT, 5-HT, NE, VMAT-
2)– Affects transporter trafficking (DAT) by
entering vesicles • Leads to abnormal monoamine distribution
• Generates free radicals

High Dose Methamphetamine
• >10 fold presynaptic increase of monoamines• Activates D1 receptor and D2 receptors• Toxicity to some DA and 5HT pathways, but NOT NE
– Amphet damages DA; MA damages DA & 5-HT; MDMA damages 5-HT
• May damage some interneurons, NPY, somatostatin and is D-1 sensitive
• If dose starts low and escalates gradually, causes “tolerance”

Low Dose Methamphetamine
• Low dose (.5-1mg/kg) – D1 mediated and is within therapeutic dose – Enters cell by riding plasma-lemnal transporters– Reverses transporters, largely by blocking
uptake– Mostly D-1 effects, but some D2– Little or no metabolic problems, so no free
radicals

Pharmacology of Methamphetamine
• Targets (D1 or D2, 5-HT) may vary by use level and previous history
• Neuropeptide-related systems that may be affiliated with low dose, D1 effects– GABA (+/- glutamate)– Nicotinic receptor– VMAT-2 – CB-1 antagonist

Mechanistic Precursor Approach
• While not a Phase 2 trial, placebo-controlled double-blind cross-over evaluation of tyrosine-free amino acid mixture 4 h before methamphetamine challenge in 16 healthy volunteers
• Tyrosine-free mixture caused significant reductions in subjective and objective measures of stimulant effects of methamphetamine (McTavish et al., 2001)

Amlodipine
• Randomized, placebo-controlled, double-blind 8-week study
• Amlodipine – 10m/d (n=26)
– 5mg/d (n=25)
– Placebo (n=26)
• No differences between groups by urine drug screening, self-report of drug use, craving or severity of dependence
Batki et al., 2001 (unpublished data)Batki et al., 2001 (unpublished data)
Mechanism - Calcium Channel BlockerMechanism - Calcium Channel Blocker
This just in on mechanisms…
• 20 week trial of Concerta, aripiprazole, placebo in IV 53 methamphetamine abusers in Norway
• Concerta (methylphenidate SR) significantly better than placebo;
• Aripiprazole significantly worse than placebo
CTN Meth Menace Conference, 12/2005CTN Meth Menace Conference, 12/2005

A Syndrome Approach…
Enhanced Job FunctioningEnhanced Job Functioning
Euphoria/PartyingEuphoria/Partying Psychiatric/Cognitive Psychiatric/Cognitive EffectsEffects

Psychiatric Medications
• Fluoxetine
• Imipramine
• Sertraline
• Gabapentin
• Baclofen
Fluoxetine
• Randomized, placebo-controlled, double-blind, 8-week study
• Fluoxetine 40mg/d, n=32; placebo n=28
• No differences between groups by urine drug screen, self-report of drug use, craving
Batki et al., 2000 (CPDD abstract)Batki et al., 2000 (CPDD abstract)
Mechanism – SSRI; Mediate depressionMechanism – SSRI; Mediate depression
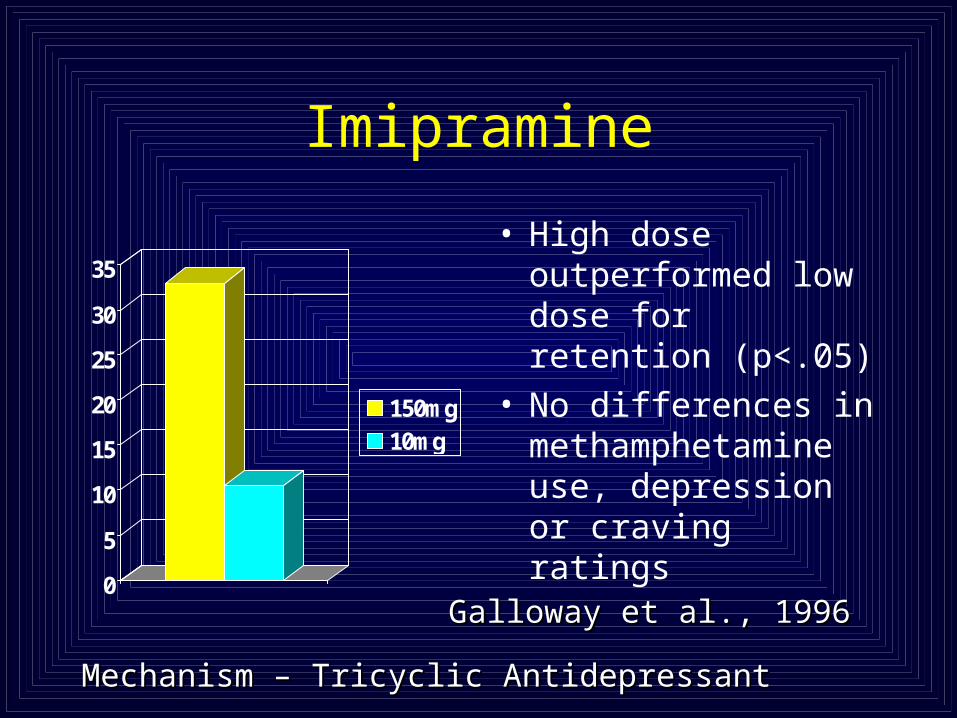
Imipramine
0
5
10
15
20
25
30
35
150mg10mg
• High dose outperformed low dose for retention (p<.05)
• No differences in methamphetamine use, depression or craving ratings
Galloway et al., 1996Galloway et al., 1996
Mechanism – Tricyclic AntidepressantMechanism – Tricyclic Antidepressant

Sertraline Study Design
• Randomized, double blind, placebo-controlled trial for 225 participants, using a 2x2 design
• Sertraline (Zoloft) - start at 50 mg/day; increase to 100 mg/day after 1 week [versus placebo]
• Contingency Management – Higgins’ high magnitude voucher reinforcement [versus no CM]
• 12 weeks, thrice weekly urine drug screening and group counseling sessions
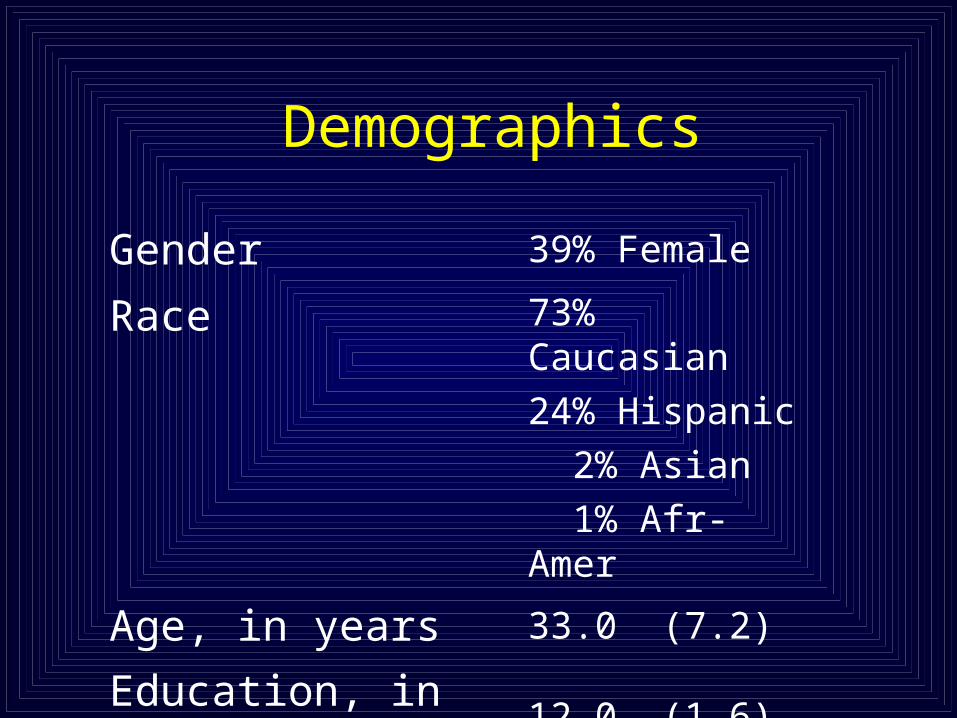
Demographics
Gender 39% Female
Race 73% Caucasian
24% Hispanic
2% Asian
1% Afr-Amer
Age, in years 33.0 (7.2)
Education, in years 12.0 (1.6)
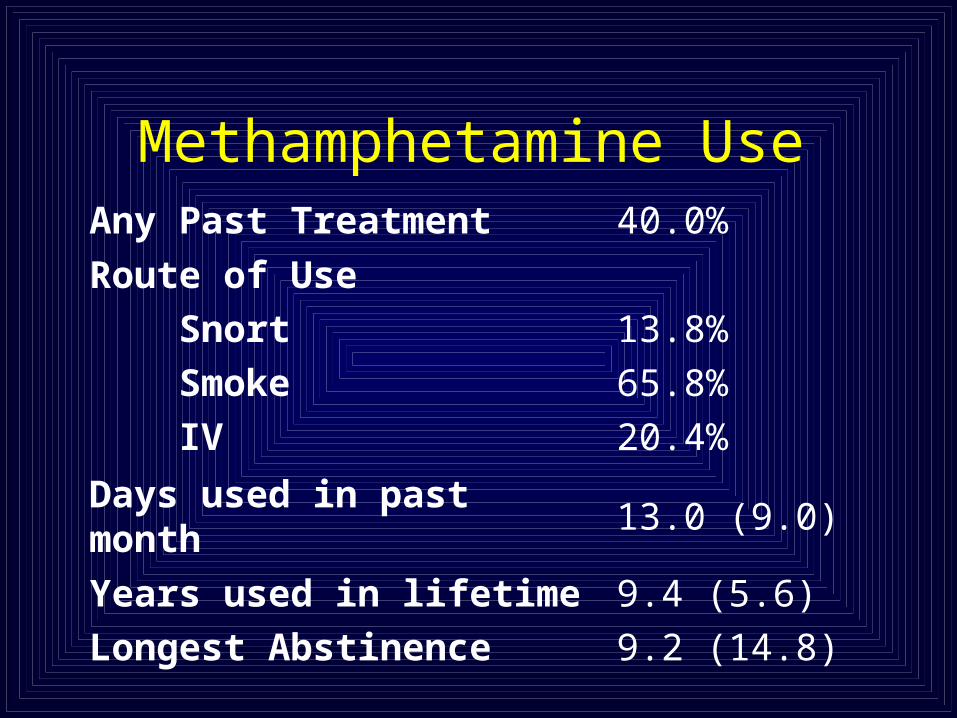
Methamphetamine UseAny Past Treatment 40.0%
Route of Use
Snort
Smoke
IV
13.8%
65.8%
20.4%
Days used in past month 13.0 (9.0)
Years used in lifetime
Longest Abstinence
9.4 (5.6)
9.2 (14.8)

Retention
0
10
20
30
40
50
60
70
Zoloft + CMPlacebo + CMZoloft + No CMPlacebo + No CM
n.s effects CM
n.s effects Med
Num
ber
of P
atie
nts
Sur
vivi
ngN
umbe
r of
Pat
ient
s S
urvi
ving

Treatment Effectiveness Scores
0
2
4
6
8
10
12
14
16
18
20
Zoloft & CMPlaceob & CMZoloft & No CMPlaceob & No CM
CM: F = 8.6 , df = 1 , p < 0.01Medication n.s.

Longest Abstinence
0
5
10
15
20
25
30
35
40
Zoloft & CMPlacebo & CMZoloft & No CMPlacebo & No CM
CM: F = 25.4 , df = 1, p < 0.001 Medication n.s.
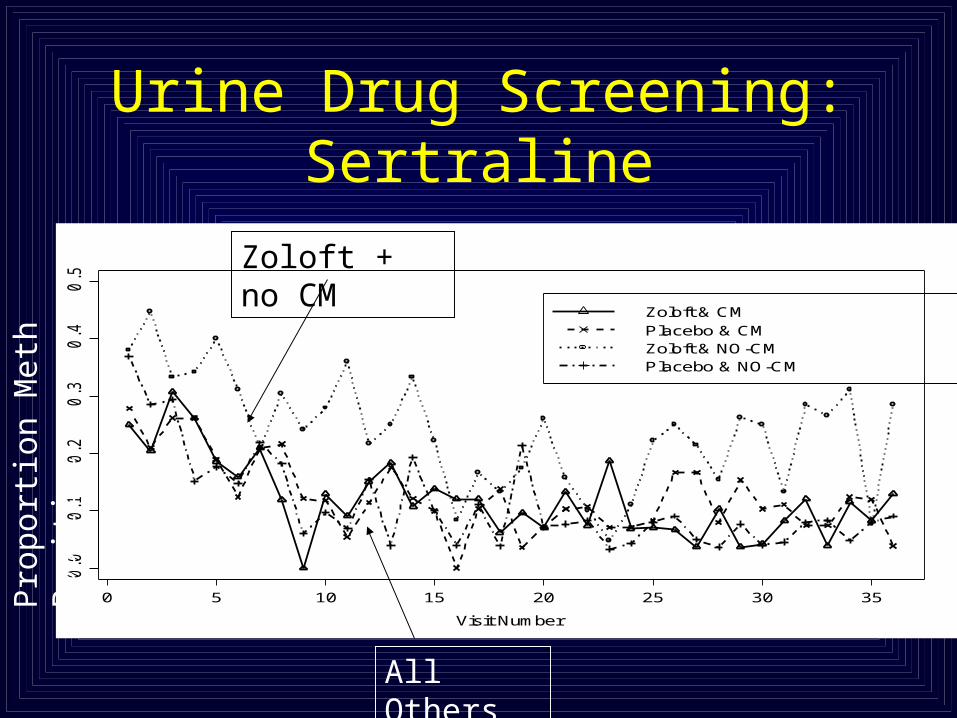
Urine Drug Screening: Sertraline
0 5 10 15 20 25 30 35
0.0
0.1
0.2
0.3
0.4
0.5
Visit Number
Pe
rce
nt
of
Co
ca
ine
Use
Zoloft & CMPlacebo & CMZoloft & NO-CMPlacebo & NO-CM
Pro
port
ion
Met
h P
osit
ive
Zoloft + no CM
All Others
Conclusions on Sertraline; SSRIs?
• CM effective at reducing methamphetamine abuse (longest abstinence; TES)
• Placebo effective over sertraline along abstinence variables
• No real effect of depression reduction– Implications on using SSRI medications for
methamphetamine abuse

Gabapentin Baclofen
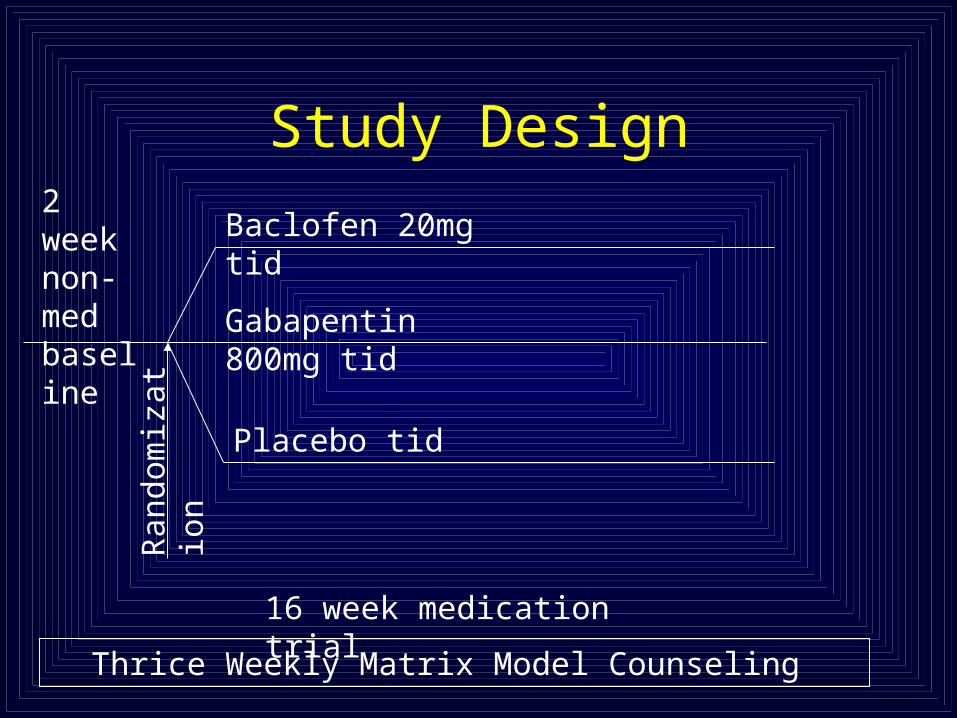
Study Design
Gabapentin 800mg tid
Baclofen 20mg tid
Placebo tid
Thrice Weekly Matrix Model Counseling
2 week non-med baseline
16 week medication trial
Ran
dom
izat
ion
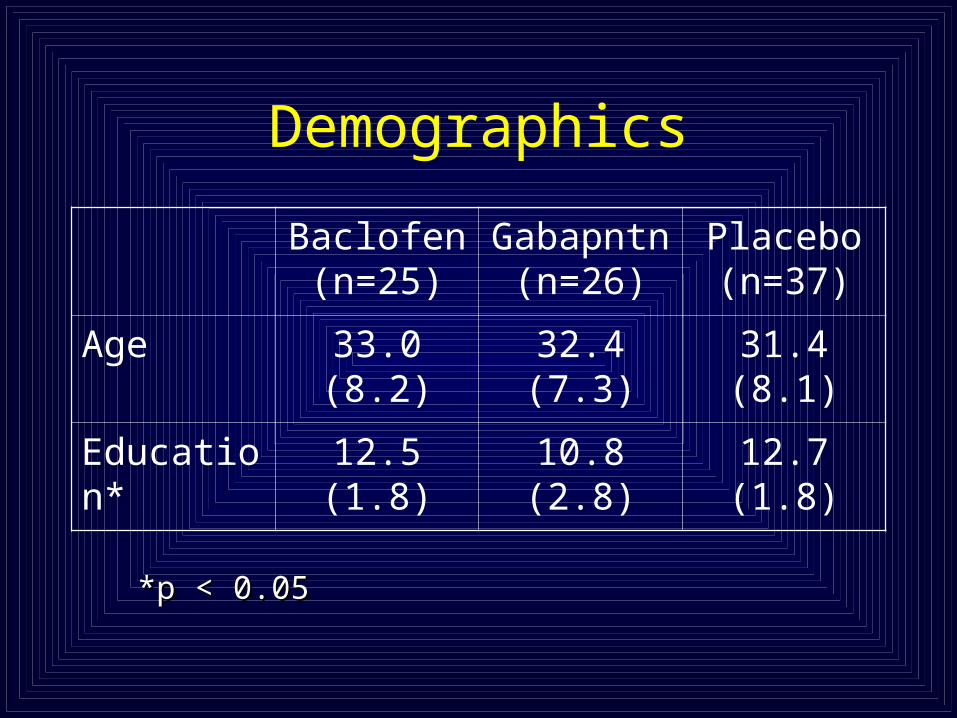
Demographics
Baclofen (n=25)
Gabapntn (n=26)
Placebo (n=37)
Age 33.0 (8.2) 32.4 (7.3) 31.4 (8.1)
Education* 12.5 (1.8) 10.8 (2.8) 12.7 (1.8)
*p < 0.05*p < 0.05

Demographics
Baclofen (n=25)
Gabapntn (n=26)
Placebo (n=37)
Gender
Female
Male
28%
72%
38%
62%
27%
73%
Ethnicity
White
Latino/a
Other
72%
20%
8%
54%
31%
15%
54%
38%
8%

Drug Use History
Baclofen (n=25)
Gabapntn (n=26)
Placebo (n=37)
30-Day Meth 13.8 (8.1)
16.6 (10.2)
14.4 (8.8)
Meth Lifetime 8.9 (7.4) 10.1 (6.3) 9.6 (5.9)
30-Day Cocaine 0.6 (3.0) 0.3 (1.2) 0.1 (0.5)
30-Day Marijuana* 8.9 (11.6) 2.4 (6.1) 3.3 (6.6)
P < 0.05P < 0.05

Route of Administration
0
10
20
30
40
50
60
70
80
90
Per
cent
Smoke Nasal IV
Bac (n=25)Gaba (n=26)Plac (n=37)

Survival Analysis
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47
Study Visits
Pro
po
rtio
n R
eta
ined
Baclofen Gabapentin Placebo
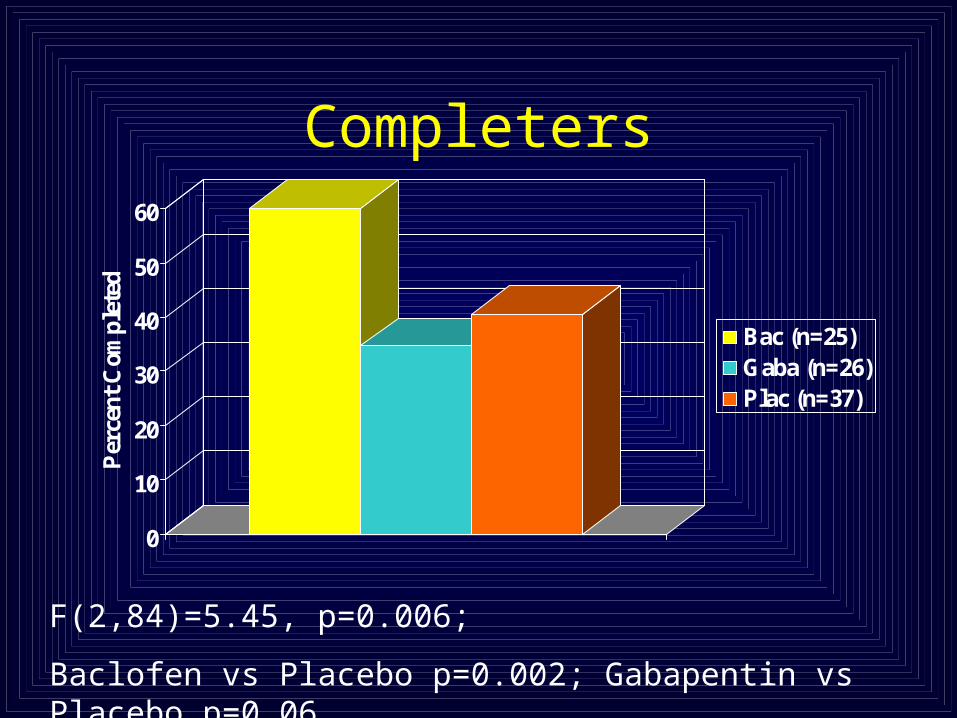
Completers
0
10
20
30
40
50
60
Per
cent
Com
plet
ed
Bac (n=25)Gaba (n=26)Plac (n=37)
F(2,84)=5.45, p=0.006;
Baclofen vs Placebo p=0.002; Gabapentin vs Placebo p=0.06
Medication Compliance
0102030405060708090
100
Per
cent Bac (n=25)
Gaba (n=26)Placebo (n=37)

Urine Drug Screening: Composites
0
10
20
30
40
50
60
2 weeks 3 weeks TES
Bac (n=25)Gaba (n=26)Plac (n=37)
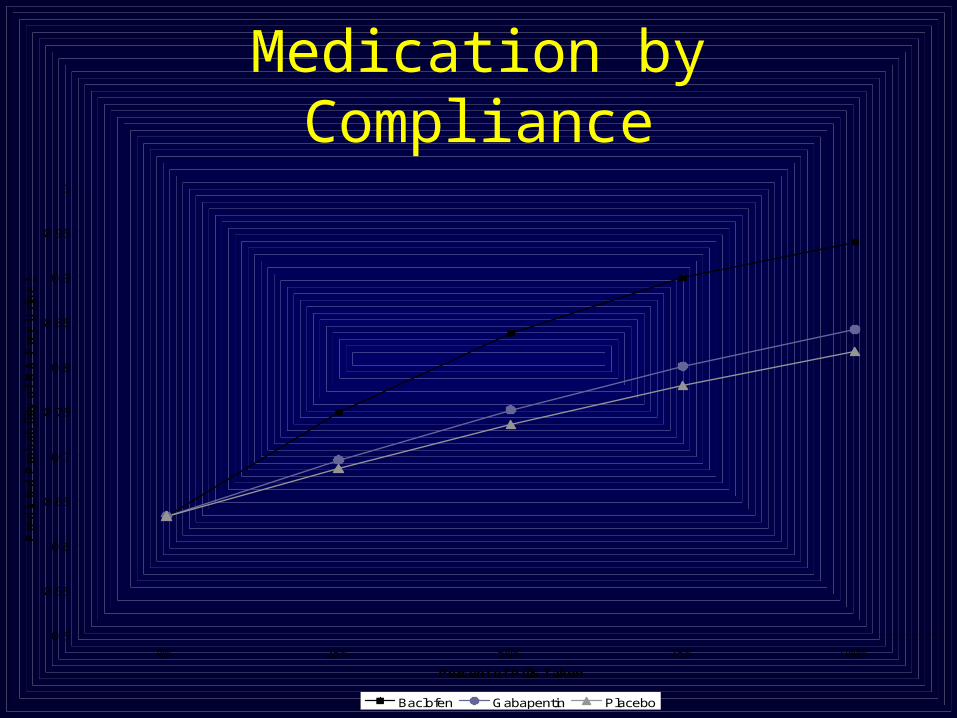
Medication by Compliance
0.5
0.55
0.6
0.65
0.7
0.75
0.8
0.85
0.9
0.95
1
0% 25% 50% 75% 100%
Percent of Pills Taken
Pre
dic
ted
Pro
ba
bil
ity
of
MA
-Fre
e U
rin
e S
am
ple
Baclofen Gabapentin Placebo

Depression
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
18.00
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Study Week
Mean
BD
I S
co
re
Baclofen Gabapentin Placebo
P = 0.057P = 0.057

Depression and Methamphetamine
Urine Screen -3 days -1 day +1 day +3 days
Chi Square 10.79 9.54 9.3 7.13P value 0.001 0.002 0.002 0.007
BDI Score

Baclofen/Gabapentin:Summary
• Education and Cannabis differences by assignment
• No significant main effects for treatment condition• Post hoc analyses suggests baclofen effects,
particularly with increased medication compliance• More evidence of a need for “super GABA” agent
– Open label trial of Brodie et al (2005)

Partying: Ondansetron
• 5-HT3 antagonist with evidence of efficacy for early-onset alcoholism (Johnson et al., 2004)
• MCTG study completed in 2004• 1,2,4,0mg/d • No evidence of any dose of ondansetron over
placebo as measured by methamphetamine use, retention, craving (Johnson et al., 2004 CPDD abstract)

What’s New in The Medication Cupboard?
• Recent Findings:– Bupropion
• Significant effect on urine, especially in low use group
• Planned Studies – Bupropion
– GVG
– Modafinil

Application of Advanced Biostatistics
Random Effect Markov Transition ModelsRandom Effect Markov Transition Models
Shoptaw, Yang et al., 2002Shoptaw, Yang et al., 2002
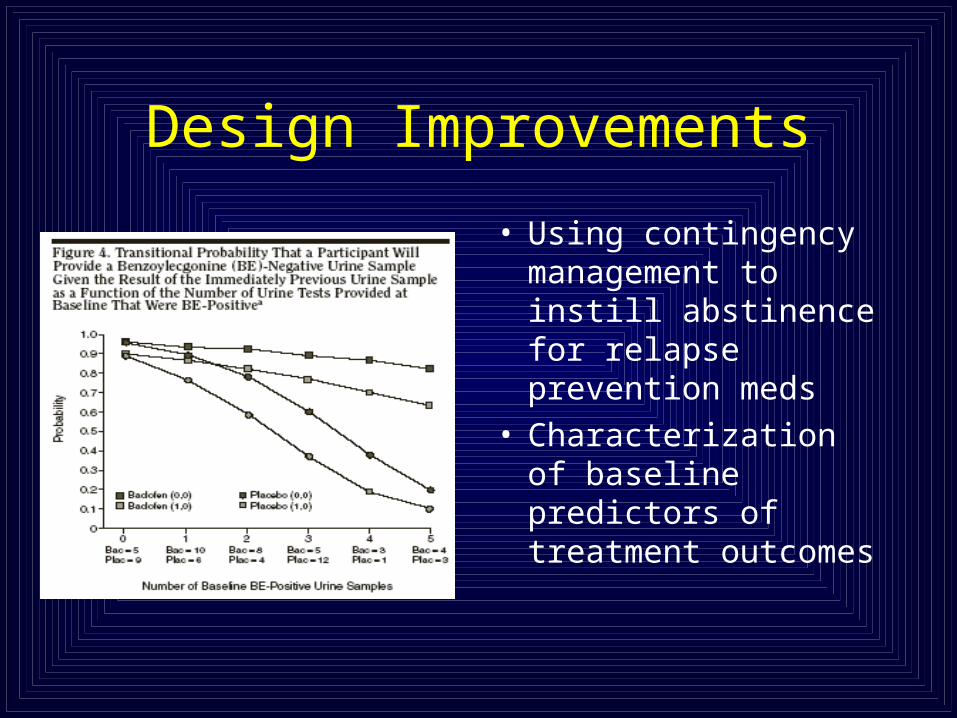
Design Improvements
• Using contingency management to instill abstinence for relapse prevention meds
• Characterization of baseline predictors of treatment outcomes