darnell - poly pharmacy - oregon pa · non-adherence use of potentially inappropriate medications...
TRANSCRIPT

10/16/2015
1
GERIATRIC PHARMACONSIDERATIONS
John C. Darnell PharmD, BCACP
Objectives
� Evaluate the safety and efficacy of various
medications in the older adult patient population
� Identify medications to be used cautiously or avoided altogether in older adult patients
� Recommend safer alternatives for specific conditions
Providence Health
3
Providence Health & Services- Large, integrated health system
Oregon Region• 8 acute care facilities (25-500 beds)
• Providence Portland Medical Center (483 beds)
• Providence St. Vincent Medical Center (523 beds)
• Over 100 medical clinics (Oregon, SW Washington)
• Specialty Pharmacy and Home Services
• Ambulatory Geriatrics clinics
• Providence Health Plan- >400,000 member lives

10/16/2015
2
PMG Clinical Pharmacy Department
• A non-distribution pharmacy service providing
clinical, educational and operational support to the PMG employed physician practices
• Employs a combination of centralized and de-centralized services
• Goal: To support high-quality, evidence-based, cost-effective medication therapy
Acknowledgements
� Kristy Butler, PharmD, BCPS, BCACP, FASHP
� Jonathan White, PharmD, BCACP
� Chelsea Mannebach, PharmD, BCPS
� Vickie Poremba, PharmD
� Johanna Thompson, PharmD,
Outline
� Background
� Metabolic changes in the elderly
� Beers List Updates:
� Pearls in Prescribing:
� Diabetes Mellitus
� Hypertension
� Hyperlipidemia
� Benzodiazepines
� Anticoagulants
� Anticholinergics
� Take Home Principles

10/16/2015
3
Polypharmacy
� Unclear definition as there is no “minimum number”
� 5 – 10?
� Any inappropriate, unnecessary, or excessive medication
� Leads to numerous potential problems
� Drug/drug inx, adverse effects, “prescribing cascade”…
Google image. Polypharmacy.
Aging Population
� Of patient’s 65 years of age or older:
� 20% have five or more chronic diseases
� 50% are on five or more medications
� Account for 34-40% of Rx and OTC meds
� Increasing number of providers
N Engl J Med 2004; 351(27):2870
So why is this a concern?

10/16/2015
4
Polypharmacy Problems in Older Adults
� Overuse of Medications
� Underuse of Medications
� Non-adherence
� Use of potentially inappropriate medications
� Adverse drug events
� Drug interactions
� Changing pharmacodynamics…
J Am Geriatr Soc 2015;1-20.
Physiologic Changes with Age
Elliot DP. Pharmacokinetics and pharmacodynamics in the elderly. In: Schumock G, Brundage D, et al., eds. Pharmacotherapy Self Assessment
Program, 5th ed. Lenexa, KS: American College of Clinical Pharmacy, 2004:115-130.
Organ
System
Resulting Effect on PK
GI ↓ absorption of drugs and nutrients
Skin ↓ drug reservoir formation with
transdermal formulations
Body
Composition
↑ Vd of lipid-soluble drugs
↓ Vd of water-soluble drugs
Liver ↓ clearance of drugs with a high first-
pass metabolism
Renal ↓ renal elimination of many
medications
Pharmacokinetic Changes
� Absorption� ↑ risk ulceration from ASA, NSAIDS
� Transdermal formulations require a subQ fat layer to form a drug reservoir for absorption – caution in thin, cachetic pts
� Distribution� Lipid-soluble benzodiazepines have ↑ half life
� Albumin-bound drugs have larger fraction of free drug
� Metabolism� Changes in metabolism through phase I (oxidative) and
cytochrome P450(CYP) enzymes are variable
� Elimination� Drugs eliminated through glomerular filtration must be dosed on
the basis of individual estimated renal function
Elliot DP. Pharmacokinetics and pharmacodynamics in the elderly. In: Schumock G, Brundage D, et al., eds. Pharmacotherapy Self Assessment Program,
5th ed. Lenexa, KS: American College of Clinical Pharmacy, 2004:115-130.

10/16/2015
5
BEERS Criteria
� Published in 1991 by Dr. Mark Beers
� Expert consensus developed through extensive literature review and questionnaire evaluations
� Adopted by the CMS in July 1999 for nursing home regulation
� 53 individual medications or classes to avoid in the
elderly
� Not “contraindicated” but “potentially inappropriate”
� Use could be justified by special circumstances
Slide courtesy of Kristy Butler, Polypharmacy:Too Much of a Good Thing. Accessed 2/6/2015.
BEERS Criteria
� Focus on “high(est) risk” medications
� Benzodiazepines
� Tertiary-amine TCAs (amitriptyline, imipramine, doxepin)
� Metoclopramide, chlorpromazine
� Anticholinergics/antihistamines
� Narrow Therapeutic Index
� Phenytoin, digoxin, lithium, theophylline
Slide courtesy of Kristy Butler, Polypharmacy:Too Much of a Good Thing. Accessed 2/6/2015.
Beers Criteria 2015 Update
� Use of nitrofurantoin has been extended to those with CrCl > 30 ml/min
� long term use still not recommended
� Z-drugs (zolpidem, et. al) are still bad
� risk of falls, fractures
� Avoid use of proton pump inhibitors beyond 8 weeks in the absence of justification

10/16/2015
6
Pearls in Prescribing: Diabetes
Pearls: Diabetes
� ADA goals do not specifically mention age
� Most adults A1c < 7%� Same for older patients that are functionally/cognitively intact
� Individualized goals are important
� Less stringent goals (A1c 7-8%) for those with:� History of severe hypoglycemia
� Limited life expectancy (<5 years)
� Advanced diabetes complications/extensive comorbid conditions
� Long duration of diabetes (>10 years)
� < 8.5% for “very complex/poor health”; limited life expectancy
Diabetes Care 2012; 35(12): 2650-2664
Diabetes Care 2015; 38(1)
Pearls: Diabetes
� Cohort study: all-cause mortality in age 50+
� “Happy place” = A1c 7.5%
Metformin plus sulfonylureas Insulin-based regimen
Lancet 2010;375(9713):481-9

10/16/2015
7
Pearls: Diabetes
Drug to Avoid Concerns Safer Alternatives
Glyburide
(Diabeta)
Prolonged hypoglycemia
(especially with renal
dysfunction)High “failure rate”
Glipizide, glimepiride
Other drugs: metformin,
sitagliptin, insulin
“Sliding-scale”
insulin
Risk of hypoglycemia
(dosing mistakes)
Poor efficacy
Fixed dose:
• Basal insulin +/- rapid-
acting meal-time insulin• Mixed insulin (70/30)
Pioglitazone
(Actos)
Edema, worsening HF Metformin, sitagliptin, insulin
What about the new drugs?
� SGLT-2 inhibitors (Invokana®, Farxiga®)
� GLP-1 agonists (Victoza®, Bydureon®)
� Generally:� Not good coverage � donut hole
� Not good candidates
� Stick to the basics � metformin, insulin, sitagliptan,
glipizide
Pearls in Prescribing: Hypertension
10/16/2015
8
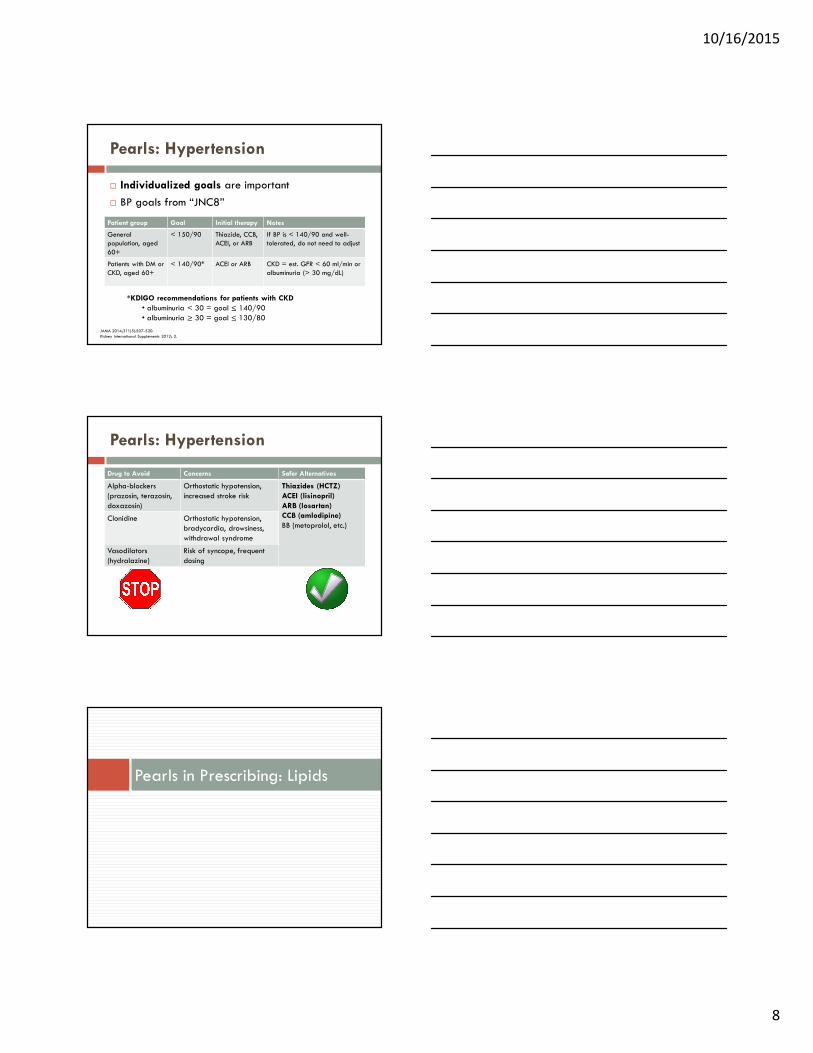
Pearls: Hypertension
� Individualized goals are important
� BP goals from “JNC8”
Patient group Goal Initial therapy Notes
General population, aged
60+
< 150/90 Thiazide, CCB,ACEI, or ARB
If BP is < 140/90 and well-tolerated, do not need to adjust
Patients with DM or CKD, aged 60+
< 140/90* ACEI or ARB CKD = est. GFR < 60 ml/min or albuminuria (> 30 mg/dL)
*KDIGO recommendations for patients with CKD
• albuminuria < 30 = goal ≤ 140/90
• albuminuria ≥ 30 = goal ≤ 130/80
JAMA 2014;311(5):507-520.
Kidney International Supplements 2012; 2.
Pearls: Hypertension
Drug to Avoid Concerns Safer Alternatives
Alpha-blockers
(prazosin, terazosin,
doxazosin)
Orthostatic hypotension,
increased stroke risk
Thiazides (HCTZ)
ACEI (lisinopril)
ARB (losartan)
CCB (amlodipine)
BB (metoprolol, etc.)Clonidine Orthostatic hypotension,
bradycardia, drowsiness,
withdrawal syndrome
Vasodilators
(hydralazine)
Risk of syncope, frequent
dosing
Pearls in Prescribing: Lipids

10/16/2015
9
Pearls: Lipids/Statins
� Recommendations for patients > 75
� Continue statin if already taking and tolerating
� Use moderate-intensity statin for secondary
prevention
� Data do not clearly support statins for primary prevention
� Consider comorbidities, safety, priorities of care
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic
Cardiovascular Risk in Adults. Circulation 2013.
Pearls: Lipids/Statins
� Secondary prevention trialsStudy Population Patient
age
Comparison Outcomes RRR NNT
PROSPER Vascular dx or high
risk
70-82 Prava 40 vs. placebo
Death/MI/CVA
CHD death/MI
15%
19%
4848
SAGE CHD 65-85 Atorva 80 vs. Prava 40
CV eventsMortality
29%77%
--37
HPS, elderly
CHD or risk equivalent
75-80 Simva 40 vs.placebo
CV events 20% 18
4S, elderly
CHD 65-70 Simva 20 vs. placebo
Mortality
CHD death
CV events
34%
43%
34%
1617
10
Bold text indicates statistically significant result
Circulation 2007;115:681-683.
Clin Interv Aging 2008 Jun; 3(2): 299–314.
Pearls: Lipids/Statins
� Primary Prevention Trials
Study Population Patient
age
Comparison Outcomes RRR NNT
CARDS, elderly
T2DM 65-75 Atorva 10 vs. placebo
MortalityCV events
Stroke
22%38%
49%
--21
--
ASCOT-LLA,
elderly
HTN 65-79 Atorva 10 vs. placebo
CHD death/MI 36% 83
Bold text indicates statistically significant result.
Circulation 2007;115:681-683.
Clin Interv Aging 2008 Jun; 3(2): 299–314.

10/16/2015
10
Pearls: Lipids/Statins
� Adverse effects: trial data in older patients
� AST/ALT >3x ULN: 0.03-4.8%
� Myalgias: 5-10%
� CK > 10x ULN: 0-1%
� Rhabdomyolysis: 0-0.06%
� Monitoring
� ALT/AST and CK levels should not be routinely monitored; check if symptoms are present
Circulation 2007;115:681-683.
Clin Interv Aging 2008 Jun; 3(2): 299–314.
Australian Prescriber 2013; 36:79–82.
Pearls: Lipids/Statins
� Adverse effects: other concerns
� Cognitive impairment
� Lacking data to support an association
� If occurs, appears reversible on discontinuation
� Diabetes
� Moderate evidence that statins are associated with increased risk of diabetes
� Higher risk with higher potency or higher dose?
Circulation 2007;115:681-683.
Clin Interv Aging 2008 Jun; 3(2): 299–314.
Australian Prescriber 2013; 36:79–82.
Pearls: Lipids/Statins
� In older adults (think age 75-82)
� Secondary prevention
� Moderate-intensity statin
� Good evidence supports decreased CV events (1-3 years)
and mortality (5 years)
� Primary prevention
� Some evidence supports decreased CV events, mortality
� Look for key comorbidities: DM, HTN

10/16/2015
11
Benzodiazepine Use in Older Adults
Benzodiazepines: Older Adults
� High prevalence of use among patients > 65 years
of age (13-23%)
� Frequently prescribed for institutionalized pts
� United States National Nursing Home Survey: Of all the psychotropic prescribed for patients > 65 years of age, 41% anti-anxiety agents
European Journal of Clinical Pharmacology 59:669–676, 2003.
Practical Geriatrics 55:233-235.
Benzodiazepines: Older Adults
� Age-related alterations in CNS receptors
� Increased sedation, unsteadiness, memory loss, disinhibition
� Increased risk of additive adverse effects
� Simultaneous use of multiple medications
� Greater risk of sedation
� Dementia
Greenblatt DJ, Shader RI: Benzodiazepines in the elderly: pharmacokinetics and drug sensitivity, in Anxiety in the Elderly. Edited by Salzman C,
Lebowitz BD. New York, Springer, 1991.

10/16/2015
12
Benzodiazepines:
BEERS Recommendation
� Avoid if possible
� SSRI’s 1st line for anxiety
� Risks of benzodiazepine use� Dementia and cognitive impairment
� Falls or fractures� Risk factors: ataxia, impaired psychomotor function,
syncope, falls
� Shorter-acting benzodiazepines are not safer than longer-acting benzodiazepines
Drug Safety 21:101–122, 1999
CNS Drugs 825–837, 2003
Benzodiazepines:
Comparative Properties
ACCP: Updates in Therapeutics: The Pharmacotherapy Preparatory Review and Recertification Course, 2014 Edition.
Brand
Name
Generic Name Approved
Dose Range
(<65 yo)
Elimination
half-life
(hours)
Active
metabolite
Xanax Alprazolam 0.5-10 mg/d 12-15 Not significant
Klonopin Clonazepam 0.5-4 mg/d 20-50 Not significant
Valium Diazepam 2-40 mg/d >100 N-DMDZ
Librium Chlordiazepoxide 15-100 mg/d >100 N-DMDZ
Ativan Lorazepam 1-10 mg/d 10-20 None
Serax Oxazepam 30-120 mg/d 5-14 None
Restoril Temazepam 7.5-30 mg/d 4-18 None
Benzodiazepines:
Comparative Properties
ACCP: Updates in Therapeutics: The Pharmacotherapy Preparatory Review and Recertification Course, 2014 Edition.
Brand
Name
Generic Name Approved
Dose Range
(<65 yo)
Elimination
half-life
(hours)
Active
metabolite
Xanax Alprazolam 0.5-10 mg/d 12-15 Not significant
Klonopin Clonazepam 0.5-4 mg/d 20-50 Not significant
Valium Diazepam 2-40 mg/d >100 N-DMDZ
Librium Chlordiazepoxide 15-100 mg/d >100 N-DMDZ
Ativan Lorazepam 1-10 mg/d 10-20 None
Serax Oxazepam 30-120 mg/d 5-14 None
Temazepam 7.5-30 mg/d 4-18 None

10/16/2015
13
Benzodiazepines: Tapering
� Taper can take months and should not be rushed
� Taper schedule should be individualized
� Sporadic or intermittent use may not require taper regimen
� Chronic daily use: Calculate the total daily dose and determine diazepam equivalent dosing, then:
� Taper by 10% total diazepam equivalent dose every 1-2 weeks until the dose is 10% of the original � then taper by 5% every 2-4 weeks
American Journal of Psychiatry 146:1242–1243, 1989
NEW ANTICOAGULANTS IN OLDER PATIENTS
Anticoagulation: Overview
� Warfarin has been the “gold standard” for many
years
� Since 2010, several new oral anticoagulants
(NOACs) have been approved:
� Dabigatran (Pradaxa)
� Rivaroxaban (Xarelto)
� Apixaban (Eliquis)
� Edoxaban (Savaysa) – approved 1/2015
CGS Journal of CME 2014; Vol 4, Issue 1: 18-20.
9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST Feb 2012.
10/16/2015
14
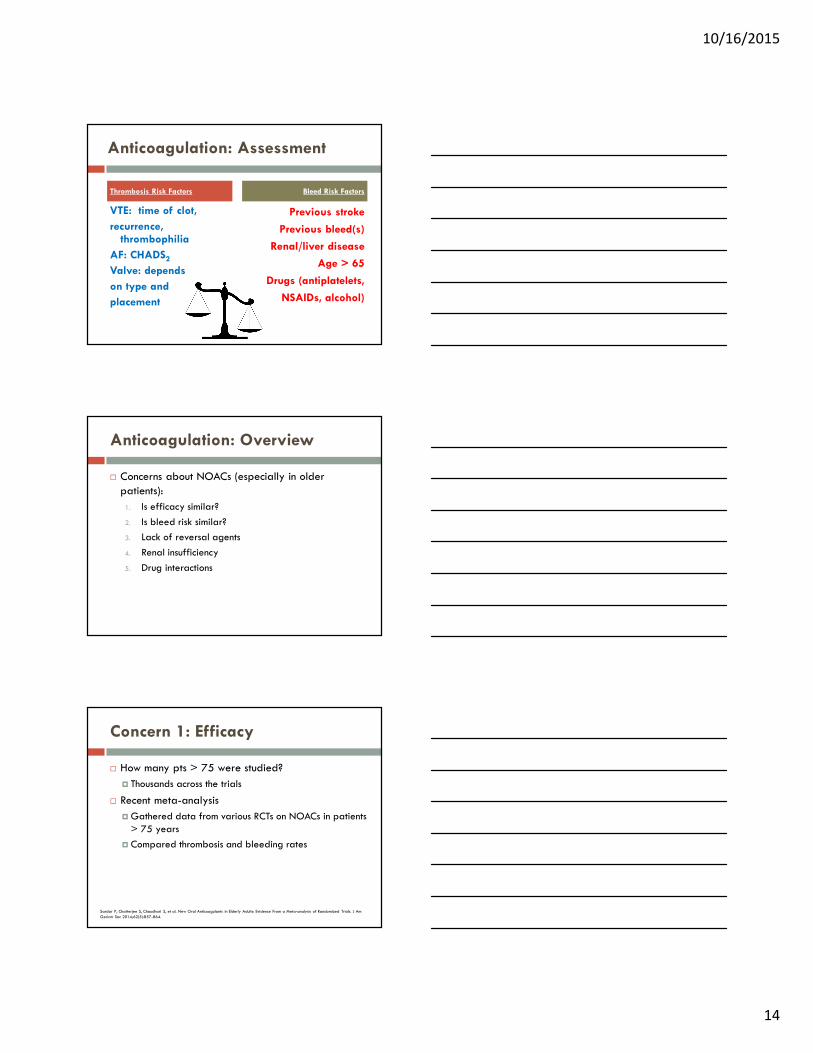
Anticoagulation: Assessment
Thrombosis Risk Factors
VTE: time of clot,
recurrence, thrombophilia
AF: CHADS2
Valve: depends
on type and
placement
Bleed Risk Factors
Previous stroke
Previous bleed(s)
Renal/liver disease
Age > 65
Drugs (antiplatelets,
NSAIDs, alcohol)
Anticoagulation: Overview
� Concerns about NOACs (especially in older
patients):
1. Is efficacy similar?
2. Is bleed risk similar?
3. Lack of reversal agents
4. Renal insufficiency
5. Drug interactions
Concern 1: Efficacy
� How many pts > 75 were studied?
� Thousands across the trials
� Recent meta-analysis
� Gathered data from various RCTs on NOACs in patients > 75 years
� Compared thrombosis and bleeding rates
Sardar P, Chatterjee S, Chaudhari S, et al. New Oral Anticoagulants in Elderly Adults: Evidence From a Meta-analysis of Randomized Trials. J Am
Geriatr Soc 2014;62(5):857-864.

10/16/2015
15
Concern 1: Efficacy
Trial Intervention Control Age > 75 on
NOAC, n
ROCKET-AF Rivaroxaban Warfarin 3,082
ARISTOTLE Apixaban Warfarin 2,743
RE-LY Dabigatran Warfarin 4,828
EINSTEIN Rivaroxaban Enoxaparin/warfarin 215
EINSTEIN-PE Rivaroxaban Enoxaparin/warfarin 441
AMPLIFY Apixaban Placebo 220
RE-MEDY Dabigatran Warfarin 140
Total 11,669
Sardar P, Chatterjee S, Chaudhari S, et al. New Oral Anticoagulants in Elderly Adults: Evidence From a Meta-analysis of Randomized Trials. J Am
Geriatr Soc 2014;62(5):857-864.
Concern 1: Efficacy
� Take Home Message:
� NOACs significantly reduced stroke and systemic embolism in AF versus conventional therapy (OR 0.65; 95% CI 0.48-0.87)
� NOACs significantly reduced VTE and VTE-related death versus conventional therapy (OR 0.45; 95% CI 0.27-0.77)
J Am Geriatr Soc 2014;62(5):857-864.
Concern 2: Bleed Risk
� Take Home Message:
� NOACs did not cause significantly more major or clinically relevant bleeding vs. conventional therapy (OR 1.02; 95% CI 0.73-1.43)
� Rivaroxaban and dabigatran “trended” toward more bleeding
� Apixaban appears to have lowest bleed rates
J Am Geriatr Soc 2014;62(5):857-864.

10/16/2015
16
Concern 2: Bleed Risk
� What about all those reports about more bleeding
with NOACs?
� Many included individuals with multiple comorbidities, like renal impairment
� Bleed risk may be more related to comorbidities (CKD, low weight, drug interactions) than age alone
J Am Geriatr Soc 2014;62(5):857-864.
Concern 3: Reversal
� Yes, there are no specific reversal agents
� However:
� NOACs have short half-lives
� Unclear whether hemorrhage on warfarin is less devastating
� Can rapidly reverse INR � but morbidity and mortality remain high
J Am Geriatr Soc 2014;62(5):857-864.
Concern 4: Renal Insufficiency
� All NOACs are renally cleared
� Renal function declines with age
� Dose must be adjusted based on CrCl
Drug CrCl > 50 CrCl 30-50 CrCl 15-29 CrCl < 15
Dabigatran(Pradaxa)
No adjustment
No adjustment US: 75 mg BIDOther: AVOID
AVOID
Apixaban(Eliquis)
No adjustment
No adjustment A-fib: see below*
AVOID AVOID
Rivaroxaban(Xarelto)
No adjustment
A-fib: 15 mg daily
AVOID AVOID
Edoxaban(Savaysa)
AF: do not
use if > 95
No adjustment 30 mg daily* AVOID
Lexi-Comp Drug Database. Accessed via Up-To-Date through PMG Intranet
9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST Feb 2012.
*If 2/3 present: Age > 80, SCr > 1.5 mg/dL, or BW < 60 kg, reduce to 2.5 mg BID

10/16/2015
17
Concern 4: Renal Insufficiency
� NOACs not studied in advanced CKD/ESRD
� Trials excluded patients with CrCl < 25-30 ml/min
� Anticoagulant levels can be markedly increased and elimination significantly prolonged
� Choose an alternate anticoagulant (e.g. warfarin) for
advanced CKD
Lexi-Comp Drug Database. Accessed via Up-To-Date through PMG Intranet
9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST Feb 2012.
Concern 5: Interactions
� Drug interactions
� Not as many as warfarin, but still problematic
� Increase: Amiodarone, ketoconazole, itraconazole, clarithromycin
� Decrease: rifampin, carbamazepine, St. John’s Wort
� Look them up; there are lots of nuances!
� Example: Renal insufficiency (CrCl 30-80 ml/min) + a drug that increases anticoagulant levels = may need to avoid
NOAC
Anticoagulants: Bottom Line
� Effective for preventing thrombosis
� Respect quality of life!
� Similar bleed risks vs. conventional therapy
� Apixaban appears to have lowest bleeding rates
� Dabigatran and rivaroxaban “trend” toward more bleeding
� More GI bleeding seen with both in pivotal trials
� Be wary of renal dysfunction
� Look up drug interactions!

10/16/2015
18
Anticholinergics in Elderly
Anticholinergics: Overview
� Retrospective review found almost 25% of all community dwelling patients > 65 were on a “clinically significant” anticholinergic drug
� Adverse effects associated with anticholinergic drugs include: � Memory impairment
� Confusion
� Hallucinations
� Dry mouth
� Blurred vision
� Constipation
� Nausea
� Urinary retention
� Tachycardia
Drugs Aging. 2013 Oct(10):837-44. Image from: http://sketchymedicine.com/2012/01/anticholinergic-mnemonic/
Indication Offending
Medication Class
Recommendation
Urinary incontinence
Antispasmodic Agents(ie: oxybutynin)
- Avoid in patients with hx of dementia or cognitive impairment
- Use more selective antispasmodic agents such as darifenacin, solifenacin, or trospium
- Avoid in males w/ BPH
Allergic rhinitis 1st generation antihistame
(diphenhydramine –Benadryl®)
- Intranasal saline flushes - Intranasal corticosteroid
- 2nd generation antihistamine (loratadine –Claritin®, certirizine – Zyrtec®, fexofenadine –
Allegra®)
Insomnia TricyclicAntidepressants (ie
amitriptyline, imipramine, doxepin)
- Non-pharmacologic therapy
- melatonin
- low dose trazodone- Low dose secondary amine tricyclic
antidepressant (nortriptyline, desipramine)
Skeletal muscle pain
Muscle relaxants - Short course NSAIDs (topical > oral) - Topical cream (capsaicin cream)
J Am Geriatr Soc 2015;1-20.

10/16/2015
19
Anticholinergics: Bottom Line
� Difficult to avoid as many medications in many
different classes have anticholinergic side effects
� More important to recognize possible medication side effects vs symptoms of a separate disorder
Take Home Points/Principles
Take Home Points
� Avoid > 1 med in same class
� Consider meds that treat more than 1 problem
� Start low, go slow
� But keep going� ACE-Is, beta-blockers, antidepressants
� Or stay low� Li, anticonvulsants, digoxin, opioids, BZDs

10/16/2015
20
Take Home Points
� Stop/taper meds if not indicated/effective
� Taper 25-50% every 5 half lives
� Change one medication at a time
� Schedule f/u for monitoring of adverse effects, withdrawal, improvement, worsening
� Summarize changes in writing
� Once daily meds or combination products
Take Home Principles
� ALWAYS assess the evidence for its use
� ALWAYS assess the risk
� ALWAYS factor in quality of life
References
1. Ferner RE, Aronson JK. Communicating information about drug safety. BMJ 2006;333(7559):143.
2. Tinetti ME, Bogardus ST Jr, et al. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 2004; 351(27):2870.
3. American Geriatrics Society 2015 updated Beers Criteria for potentially inappropriate medication use in older adults. American Geriatrics Society 2015 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2015;1-20.
4. Elliot DP. Pharmacokinetics and pharmacodynamics in the elderly. In: Schumock G, Brundage D, et al., eds. Pharmacotherapy Self Assessment Program, 5th ed. Lenexa, KS: American College of Clinical Pharmacy, 2004:115-130.
5. Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med 1991; 151:1825-32.
6. Kirkman MS, Briscoe VJ, Clark N et al. Diabetes in older adults. Diabetes Care 2012; 35(12): 2650-2664
7. Cefalu WT, Bakris G, Blonde L, et al. Standards of medical care in diabetes. Diabetes Care 2015; 38(1)
8. Currie CJ, Peters JR, Tynan A et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet 2010;375(9713):481-9
9. James PA, Oparil S, Carter BL, et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA 2014;311(5):507-520.
10. Eknoyan G, Eckardt K, Kasiske BL, et al. KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney International Supplements 2012; 2.
11. Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation 2013
12. Gotto AM. Statin therapy and the elderly: SAGE advice? Circulation 2007;115:681-683.
13. Acharjee S, Welty FK. Atorvastatin and cardiovascular risk in the elderly – patient considerations. Clin Interv Aging 2008 Jun; 3(2): 299–314.
14. Hilmer S, Gnjidic D. Statins in older adults. Australian Prescriber 2013; 36:79–82.

10/16/2015
21
References
15. Holmquist IB, Svensson B, Hoglund P: Psychotropic drugs in nursing and old age homes: relationships between needs of care and mental health status. European Journal of Clinical Pharmacology 59:669–676, 2003
16. Bogunovic OJ, Greenfield SF. Use of benzodiazepines among elderly patients. Practical Geriatrics 55:233-235.
17. Greenblatt DJ, Shader RI: Benzodiazepines in the elderly: pharmacokinetics and drug sensitivity, in Anxiety in the Elderly. Edited by Salzman C, Lebowitz BD. New York, Springer, 1991.
18. Gray S, Lai K, Larson E: Drug- induced cognition disorders in the elderly. Drug Safety 21:101–122, 1999
19. Cumming RG, Le Couter DG: Benzodiazepines and risk of hip fractures in older people: a review of the evidence. CNS Drugs 825–837, 2003
20. Schweizer E, Case WG, Rickels K: Benzodiazepine dependence and withdrawal in elderly patients. American Journal of Psychiatry 146:1242–1243, 1989
21. Budlovsky J, Wong RY. Novel Oral Anticoagulants in the Elderly. CGS Journal of CME 2014; Vol 4, Issue 1: 18-20.
22. Weitz JI, Eikelboom JW, Samama, MM. New Antithrombotic Drugs: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST Feb 2012.
23. Sura SD, Carnahan RM, et al. Prevalence and determinants of anticholinergic medication use in elderly dementia patients. Drugs Aging 2013 Oct;30(10):837-44.
24. Sardar P, Chatterjee S, Chaudhari S, et al. New Oral Anticoagulants in Elderly Adults: Evidence From a Meta-analysis of Randomized Trials. J Am Geriatr Soc 2014;62(5):857-864.
Images from: http://eastpennfoot.wordpress.com/2013/02/01/edema-how-to-avoid-swollen-feet-and-ankles/http://onhealthyliving.com/archives/2009/02/21/natural-remedies-of-constipation
Start calcium
channel blocker
Furosemide AND KCl
Stomach upset
Tx with antacids
Anti-diarrheals
Dry mouth
More fluid intake
Edema from CCB
?Constipation