data quality: uniform business office & the revenue cycle dha uniform business office program...
TRANSCRIPT
Data Quality:Uniform Business Office & The Revenue Cycle
DHA Uniform Business Office Program Manager
January 2015
.

2
Outline
• Uniform Business Office (UBO) Organization• UBO Cost Recovery Programs• MHS Billing Systems• MTF Revenue Cycle • Data Quality and How it Affects Each Phase of the
Revenue Cycle • UBO Success Factors• Resources
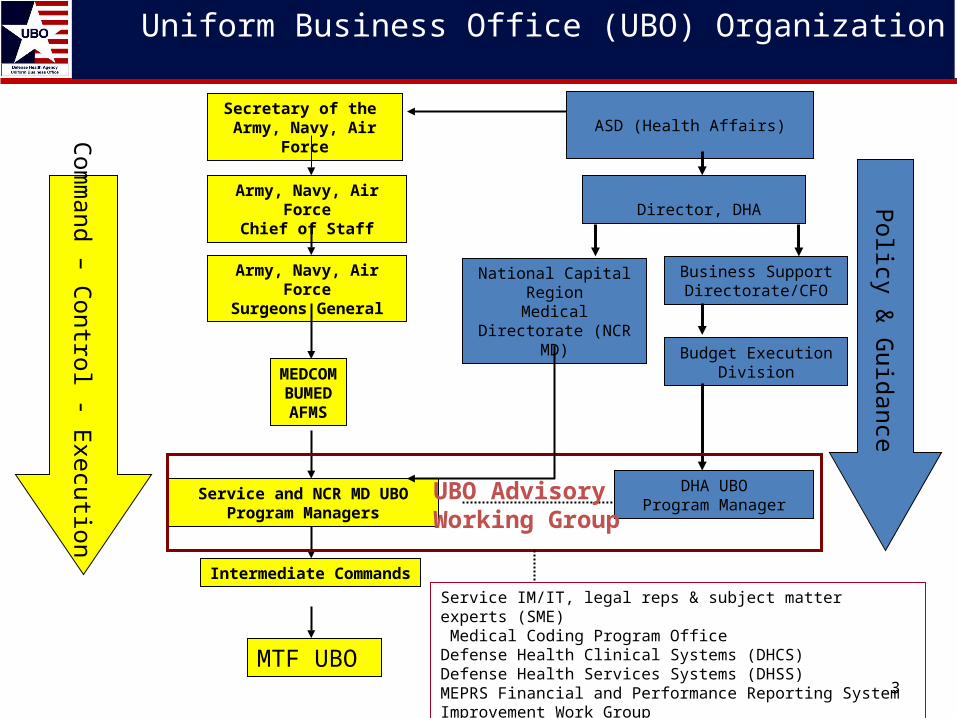
Uniform Business Office (UBO) Organization
3
Business Support Directorate/CFO
Budget Execution Division
DHA UBOProgram Manager
Service and NCR MD UBO Program Managers
ASD (Health Affairs)
Director, DHA
Intermediate Commands
MTF UBO
Army, Navy, Air ForceSurgeons General
Army, Navy, Air ForceChief of Staff
MEDCOMBUMEDAFMS
Com
mand – C
ontrol - Execution
Policy &
Guidance
Secretary of the Army, Navy, Air Force
UBO Advisory Working Group
Service IM/IT, legal reps & subject matter experts (SME) Medical Coding Program OfficeDefense Health Clinical Systems (DHCS)Defense Health Services Systems (DHSS)MEPRS Financial and Performance Reporting System Improvement Work Group Medical Coding Program Office (MCPO)
National Capital Region
Medical Directorate (NCR MD)

4
UBO Cost Recovery Programs
Third Party Collections Program (TPCP)
Medical ServicesAccount (MSA)
Medical AffirmativeClaims (MAC)
5
Who Gets Billed Under Which Cost Recovery Program?
• Third Party Collections Program– Bill insurers for care provided to eligible DoD beneficiaries
(excludes Active Duty) with other health insurance (excluding Medicare & TRICARE)
• Medical Services Account– Includes billing for care provided to eligible patients from
Veterans Affairs/Coast Guard /NOAA/ PHS/Civilian Emergencies/Foreign Military & their Family Members
• Medical Affirmative Claims– Bill for care provided to eligible DoD beneficiaries injured
by third parties

6
Collections by UBO Cost Recovery Program
• Third Party Collections Program (TPCP) – $135.3M (FY 2014)
• Medical Services Account (MSA) – $289.8M (FY 2014)
• Medical Affirmative Claims (MAC) – $12.9M (FY 2014)
• ALL funds collected are retained by your MTF– TPC funds are in addition to the MTFs O&M budget

7
*NOTE: Collected amount includes dollars for healthcare services provided in previous FYs and may exceed current FY billings .
On average, from FY10-FY13, 52% of total MHS uncollected dollars can be attributed to acceptable third party payer denials (co-pay, deductibles, out of network, non-covered benefits).
Data Source: MTF DD Form 2570 submissions to the DHA UBO Metrics Report A/O 1 Nov 2014
Service FY10 FY11 FY12 FY13 FY14
Billed Collected Billed Collected Billed Collected Billed Collected Billed Collected
Outpatient
Army $ 88.0 $ 58.0 $ 91.9 $ 51.5 $ 79.0 $ 42.2 $ 69.8 $ 39.2 $ 60.1 $ 32.5
Navy $ 40.2 $ 27.7 $ 36.7 $ 21.2 $ 35.0 $ 18.0 $ 31.7 $ 16.0 $ 31.3 $ 14.0
Air Force $ 159.9 $ 79.7 $ 145.0 $ 70.9 $ 135.9 $ 58.5 $ 124.0 $ 51.3 $ 110.3 $ 44.4
NCR MD $ 13.4 $ 9.2 $ 16.3 $ 9.0 $ 25.8 $ 12.0 $ 23.6 $ 12.0 $ 23.9 $ 10.8
Total $ 301.5 $ 174.6 $ 289.9 $ 152.6 $ 275.7 $ 130.7 $ 249.1 $ 118.5 $ 225.6 $ 101.7
Inpatient
Army $ 53.7 $ 26.3 $ 55.1 $ 22.5 $ 44.6 $ 22.7 $ 41.3 $ 21.0 $ 35.2 $ 16.8
Navy $ 12.5 $ 4.6 $ 11.8 $ 4.7 $ 12.4 $ 4.5 $ 10.9 $ 4.4 $ 14.3 $ 3.8
Air Force $ 26.6 $ 10.1 $ 17.3 $ 7.9 $ 16.2 $ 5.4 $ 16.0 $ 4.5 $ 15.9 $ 4.0
NCR MD $ 6.7 $ 4.5 $ 6.8 $ 2.9 $ 14.0 $ 4.8 $ 8.9 $ 6.2 $ 16.4 $ 9.0
Total $ 99.5 $ 45.5 $ 91.0 $ 38.0 $ 87.2 $ 37.4 $ 77.1 $ 36.1 $ 81.8 $ 33.6
Third Party Collections Program (TPCP) Inpatient and Outpatient Amounts Billed and Collected ($M) FY14 Q4

8
Current MHS Billing Systems
• Third Party Outpatient Collection System– Government developed system for billing outpatient TPCP
(includes outpatient visits, lab/rad/pharmacy prescriptions)
• CHCS Medical Services Account (MSA) Module– Government developed module used for billing TPCP
inpatient claims (both institutional & professional charges) & MSA
• Relationship to other systems– Provider Specialty Codes and other Provider Data– Collection of other health insurance (OHI) information in
CHCS– Centralized OHI Repository on DEERS– Coding Compliance Editor (CCE)

9
MSA ClaimsTPCP Inpatient Claims
FinancialPersonnelWorkload
LegendDatabase
Subsystem
Data
Documents
CHCS
DEERS
TPOCS TPCP OP ClaimsMAC Claims
EAS IV
MDR M-2
ADM
WAM PDTS
CCE
AHLTA
Existing MHS Systems
Billing/Collections
10
Data Quality Characteristics
• Accurate• Complete• Concise• Cost-effective• Relevant / Timely / Up-To-Date• Presentation• Consistent

11
MTF Revenue Cycle
Results are increased resourcing with reliable outcomes in the form of usable data
CHCS(Files &Tables)
PatientAccess
PayerEducation
Appeals
Payment Posting
Denial Management
AccountFollow-up
Claims Submissions
Coding
EncounterDocument
PatientRegistrationIns Verify &
Auth
Data Quality Management
CCE TPOCS
ElectronicBilling
Data Quality Management Controls are the driving force and conduit for ensuring effective and efficient operations.
Visual review for validating and streamlining major clinical business and resource management processes
Improved patient access, records documentation and coding accuracy
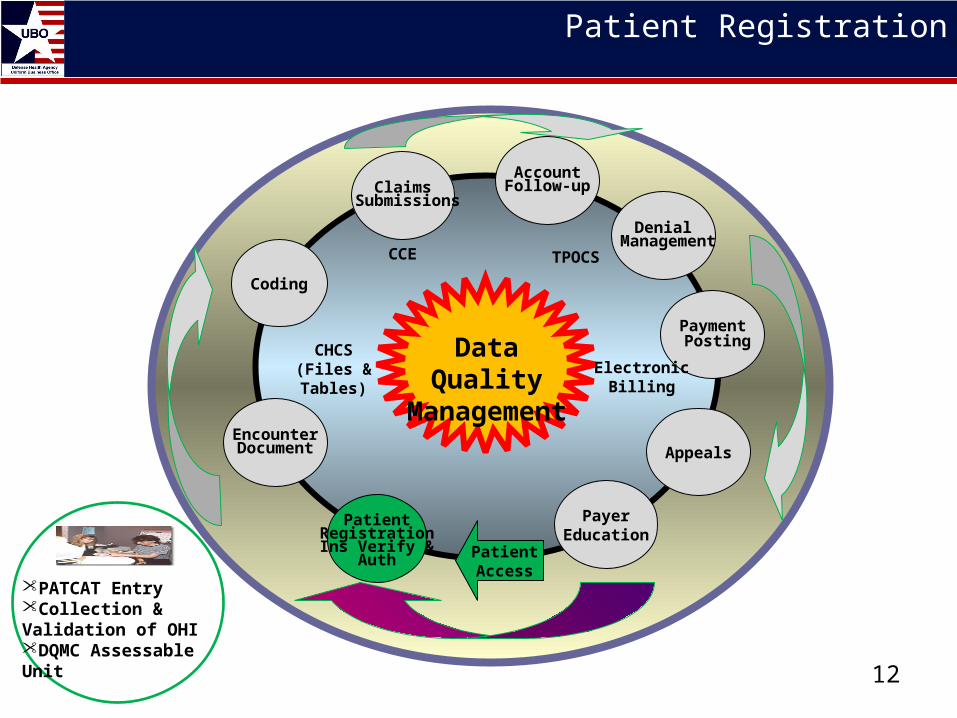
Patient Registration
12
CHCS(Files &Tables)
PatientAccess
PayerEducation
Appeals
Payment Posting
Denial Management
AccountFollow-upClaims
Submissions
Coding
EncounterDocument
PatientRegistrationIns Verify &
Auth
Data Quality Management
CCE TPOCS
ElectronicBilling
•PATCAT Entry•Collection & Validation of OHI•DQMC Assessable Unit

13
Importance of Accurate PATCAT Entry
• Patient Category (PAT) determines the reimbursable rate (if any) for healthcare– Over 300 PATCATs to select from
• Challenge of Patients with Multiple PATCATs– Spouse of AD Member who is a Reservist and employed
as a Federal Employee
• Who is responsible for training/accuracy?
14
Training for Selecting the Correct PATCAT
• PATCAT course now available via the DHA UBO website
• http://www.tricare.mil/ocfo/mcfs/ubo/patcat.cfm

15
Other Health Insurance (OHI) Information
• Use DD Form 2569 to capture OHI information about your patients– All Non-Active Duty Patients required to complete it every 12
months or if data changes– OHI needs to be entered into CHCS PII screen or it “doesn’t
exist” for billing purposes– Direct correlation between presence of a current DD Form
2569 in patient record and rate of TPC billing– Reported monthly in Commander’s DQ Statement

16
CHCS(Files &Tables)
PatientAccess
PayerEducation
Appeals
Payment Posting
Denial Management
AccountFollow-up
Claims Submissions
Coding
EncounterDocument
PatientRegistrationIns Verify &
Auth
Data Quality Management
CCE TPOCS
ElectronicBilling
•Medical Record Availability•Documentation
Encounter Documentation / Coding
17
CHCS Provider Specialty Codes (PSC)
• Set of codes unique to CHCS
• Current business rules preclude TPOCS from receiving ADM encounters with blank PSCs or PSCs > 900 – (exception of 901 – Physician Assistant)– 702 (Clinical Psychologist) versus 954 (Psychology)
• Site visit to large medical center found 20% of PSCs fields were blank– Billable ADM encounter never reach TPOCS
18
Correcting the CHCS Provider Specialty Codes (PSC)
• Get your site’s most current CHCS Provider Profile and review the PSC fields for accuracy– No blank fields– Billable providers have PSC under 900 (plus 901 – Physician
Assistant)
• Determine whose responsible for maintaining the PSC fields and TRAIN THEM!!!
• Periodically review the PSC fields to make sure the problem really has been permanently fixed

19
Type 1 National Provider Identifier (NPI)
• Every Provider who can bill for healthcare services is required to have a Type 1 NPI
• 23 May 07 was the deadline for MHS providers to obtain their own unique Type 1 NPIs
• Are all of your providers’ TYPE 1 NPIs in CHCS? – No NPI = No payment from Insurance Companies

20
CHCS(Files &Tables)
PatientAccess
PayerEducation
Appeals
Payment Posting
Denial Management
AccountFollow-up
Claims Submissions
Coding
EncounterDocument
PatientRegistrationIns Verify &
Auth
Data Quality Management
CCE TPOCS
ElectronicBilling
•Insurance Verification•Claim Form Data & Line Item Billing
•Account Follow-Up•Payment Posting•Denial Management
Type 1 National Provider Identifier (NPI)
Thank You
Questions?