david stultz, md, facc - drstultz.comdrstultz.com/presentations/2010 04 13 takotsubo...
TRANSCRIPT

© 2010 David Stultz, MD
TakotsuboTakotsubo CardiomyopathyCardiomyopathyApril 13, 2010April 13, 2010David Stultz, MD, FACCDavid Stultz, MD, FACC
Handout available at http://Handout available at http://www.drstultz.comwww.drstultz.com

© 2010 David Stultz, MD
Pronunciation is keyPronunciation is key……

© 2010 David Stultz, MD
…said of his mother’s dog. “Everything depends on him. If he’s OK, she’ll be OK.”

© 2010 David Stultz, MD
Case 1Case 1
House fires are hard on the heartHouse fires are hard on the heart
�� 76 year old female76 year old female
�� No prior historyNo prior history
�� Presented to ER 8 hours after firePresented to ER 8 hours after fire�� Looking for dog, possible smoke inhalation Looking for dog, possible smoke inhalation for 20 minutesfor 20 minutes
�� Acute shortness of breath and chest Acute shortness of breath and chest discomfortdiscomfort�� Lasted about 1 hourLasted about 1 hour
�� Fluctuating BP/Fluctuating BP/hypotensivehypotensive in the ERin the ER
© 2010 David Stultz, MD
Past Medical HistoryPast Medical History
�� No significant past medical history.No significant past medical history.
�� History of orthopedic procedures to History of orthopedic procedures to
femur and wristfemur and wrist
�� No medicationsNo medications
�� Lives alone with her dogLives alone with her dog
�� Smokes about Smokes about ½½ pack cigarettes a daypack cigarettes a day
�� Very infrequent alcohol use, none recentVery infrequent alcohol use, none recent

© 2010 David Stultz, MD
Physical ExamPhysical Exam
�� Initial VitalsInitial Vitals�� HR 88HR 88
�� BP 97/68BP 97/68
�� OO22 saturation 98% on 2 Liters NCsaturation 98% on 2 Liters NC
�� respsresps 22/min22/min
�� GENERAL: A&O x 3, no acute distressGENERAL: A&O x 3, no acute distress
�� Neck: No JVD, no bruitsNeck: No JVD, no bruits
�� Heart: regular, Heart: regular, occassionaloccassional PVC, no murmurPVC, no murmur
�� Lungs: decreased in basesLungs: decreased in bases
�� Extremities: no edema, distal pulses intact and equalExtremities: no edema, distal pulses intact and equal
�� NeuroNeuro: No focal deficits: No focal deficits

© 2010 David Stultz, MD
Laboratory DataLaboratory Data
�� CreatinineCreatinine, Sodium, Potassium normal, Sodium, Potassium normal
�� WBC 11.4, WBC 11.4, HgbHgb 14.1, platelets 205,00014.1, platelets 205,000
�� TroponinTroponin I 1.22 I 1.22 --> 4.03> 4.03
�� CKCK--MB 12.1 MB 12.1 --> 14.5> 14.5
�� Initial ABG (32% FiOInitial ABG (32% FiO22))�� CO level 2.4% (normal range 0CO level 2.4% (normal range 0--2%)2%)
�� FollowupFollowup ABG (32% FiOABG (32% FiO22))�� CO 1.6%CO 1.6%
�� pOpO22 91mmHg, pCO91mmHg, pCO22 37mmHg37mmHg

© 2010 David Stultz, MD
8 hours after the fire8 hours after the fire

© 2010 David Stultz, MD
Later that nightLater that night
© 2010 David Stultz, MD
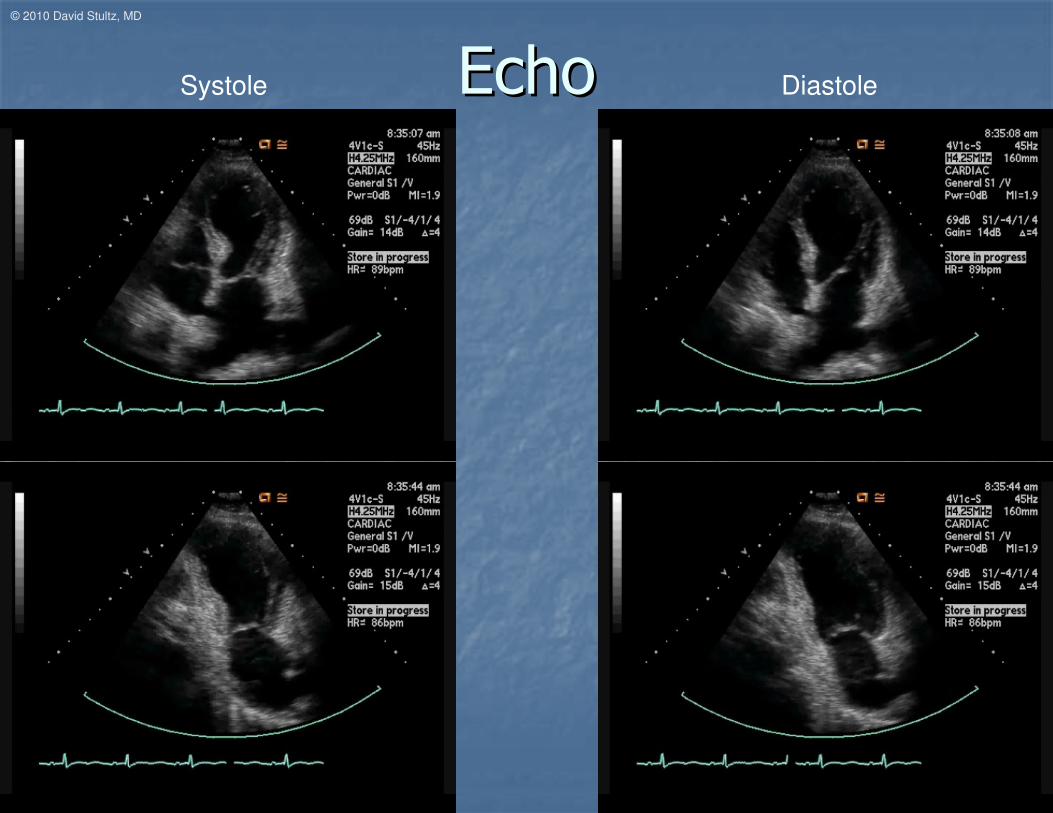
EchoEchoSystole Diastole

© 2010 David Stultz, MD
CathCath
Systole Diastole

© 2010 David Stultz, MD
Hospital CourseHospital Course
�� After catheterization, developed atrial After catheterization, developed atrial
fibrillation with rapid ventricular responsefibrillation with rapid ventricular response
�� Systolic blood pressures in the 80Systolic blood pressures in the 80’’ss
�� Attempted cardioversion, unsuccessfulAttempted cardioversion, unsuccessful
�� Treated with IV amiodaroneTreated with IV amiodarone

© 2010 David Stultz, MD
Day after fireDay after fire
�� Missing pet found, fine after fire Missing pet found, fine after fire �� …… police today confirmed that a 5police today confirmed that a 5--yearyear--old Terrier mix old Terrier mix
breed dog unaccounted for during a house fire breed dog unaccounted for during a house fire ……, is , is safe and back home with his owner.safe and back home with his owner.
�� "I'm very pleased to say that he was found yesterday"I'm very pleased to say that he was found yesterday……He turned up out running around in the neighborhood."He turned up out running around in the neighborhood."
�� Little Guy went missing after his ownerLittle Guy went missing after his owner…… returned returned home from taking him for a walk and found her home home from taking him for a walk and found her home …… ablaze.ablaze.

© 2010 David Stultz, MD
Discharge MedicationsDischarge Medications
�� AspirinAspirin 81 mg daily81 mg daily
�� CoumadinCoumadin
�� LipitorLipitor 80 mg daily80 mg daily
�� LisinoprilLisinopril 5 mg daily5 mg daily
�� MetoprololMetoprolol 12.5 mg 12.5 mg popo b.i.db.i.d..
�� AldactoneAldactone 25 mg daily25 mg daily
�� AmiodaroneAmiodarone 200 mg 200 mg popo b.i.db.i.d..
�� LasixLasix 40 mg 40 mg popo dailydaily
�� ProtonixProtonix 40 mg daily40 mg daily
�� AlbuterolAlbuterol 90 mcg INH q.2h. 90 mcg INH q.2h. prnprn
�� SpirivaSpiriva 18 mcg INH daily18 mcg INH daily
�� AdvairAdvair 250/50 INH 250/50 INH b.i.db.i.d..

© 2010 David Stultz, MD
4 months later4 months later
© 2010 David Stultz, MD
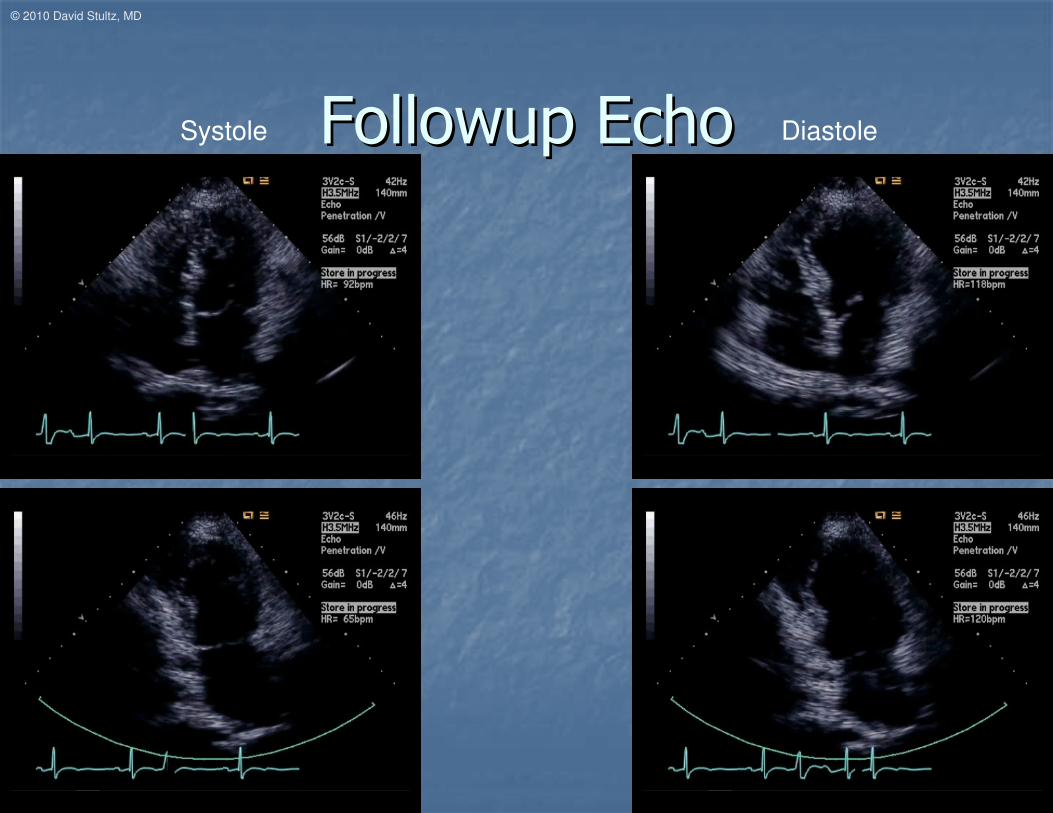
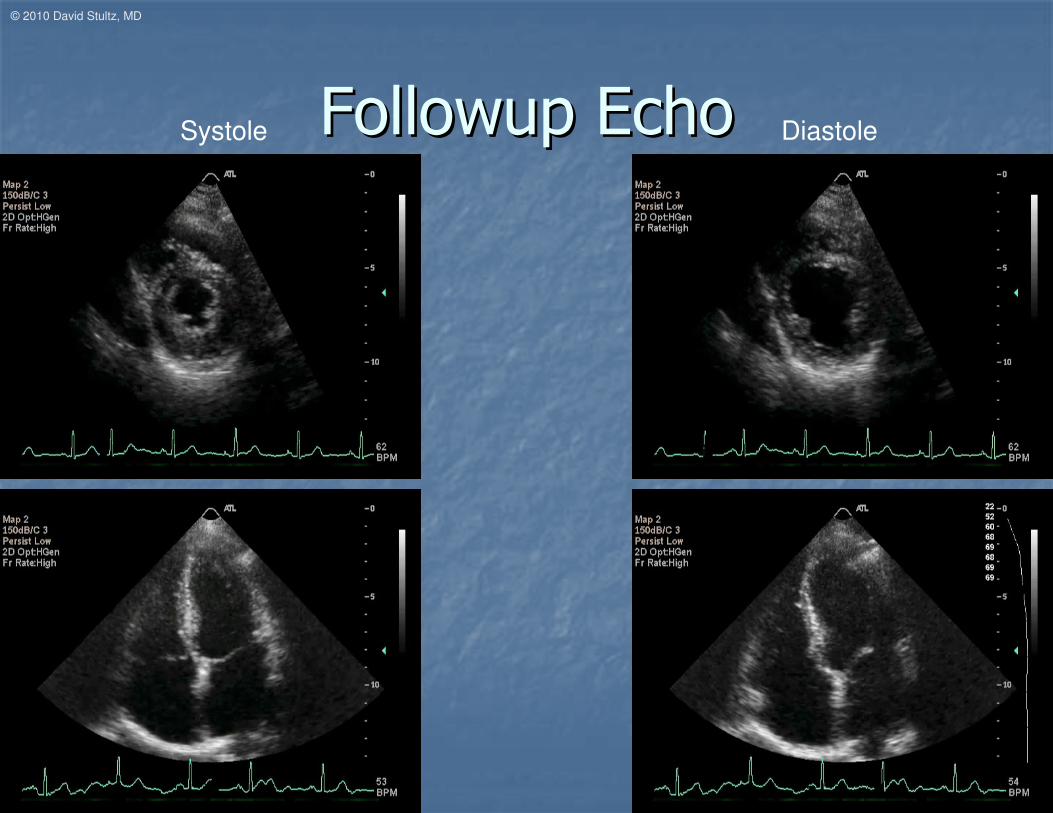
FollowupFollowup EchoEchoSystole Diastole
© 2010 David Stultz, MD
TakotsuboTakotsubo
Japanese Octopus PotJapanese Octopus Pot
�� Also known asAlso known as
�� Apical ballooning syndromeApical ballooning syndrome
�� Broken heart syndromeBroken heart syndrome
�� Stress induced cardiomyopathyStress induced cardiomyopathy
http://www.takotsubo.com/http://www.lifestylewellnesscoach.com/wellness/the-broken-heart-tako-tsubo/

© 2010 David Stultz, MD
Etiology and presentationEtiology and presentation
�� 11stst identified in 1991 in Japanidentified in 1991 in Japan
�� Significant increase in attention in 2002Significant increase in attention in 2002
�� Precipitated by a stressful eventPrecipitated by a stressful event�� Psychological or physicalPsychological or physical
�� Presentation consistent with acute myocardial infarctionPresentation consistent with acute myocardial infarction�� Chest painChest pain
�� Shortness of breathShortness of breath
�� EKG changes including ST ElevationEKG changes including ST Elevation
�� Abnormal cardiac enzymesAbnormal cardiac enzymes
�� Can have unstable Can have unstable hemodynamicshemodynamics
Brenner ZR, Powers J. Takotsubo cardiomyopathy. Heart Lung. 2008 Jan-Feb;37(1):1-7.

© 2010 David Stultz, MD
Features of Features of TakotsuboTakotsubo
CardiomyopathyCardiomyopathy
�� Significant left ventricular wall motion Significant left ventricular wall motion
abnormalityabnormality
�� Normal or Normal or hyperdynamichyperdynamic basal segmentsbasal segments
�� HypokineticHypokinetic, , akineticakinetic, or , or dyskineticdyskinetic apical apical
segmentssegments
�� No obstructive coronary atherosclerosis No obstructive coronary atherosclerosis
at cardiac catheterizationat cardiac catheterization
© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� Myocardial Oxygen DemandMyocardial Oxygen Demand--Supply Supply
DisproportionDisproportion
�� Aortic stenosisAortic stenosis
�� Prolonged hypotensionProlonged hypotension
�� TakotsuboTakotsubo cardiomyopathycardiomyopathy
�� Carbon monoxide poisoningCarbon monoxide poisoning
�� Incomplete differentiation of the aortic valveIncomplete differentiation of the aortic valve
�� Aortic insufficiencyAortic insufficiency
�� ThyrotoxicosisThyrotoxicosis
Braunwald, 8th ed.
© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� MiscellaneousMiscellaneous
�� Cocaine abuseCocaine abuse
�� MyocarditisMyocarditis
�� Myocardial contusionMyocardial contusion
�� Myocardial infarction with normal coronary Myocardial infarction with normal coronary
arteriesarteries
�� Complication of cardiac catheterizationComplication of cardiac catheterization
Braunwald, 8th ed.

© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� ArteritisArteritis�� LueticLuetic
�� Granulomatous (Takayasu disease)Granulomatous (Takayasu disease)
�� PolyarteritisPolyarteritis nodosanodosa
�� MucocutaneousMucocutaneous lymph node (Kawasaki) lymph node (Kawasaki) syndromesyndrome
�� Disseminated lupus Disseminated lupus erythematosuserythematosus
�� Rheumatoid Rheumatoid spondylitisspondylitis
�� AnkylosingAnkylosing spondylitisspondylitis
Braunwald, 8th ed.

© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� Trauma to coronary arteriesTrauma to coronary arteries
�� LacerationLaceration
�� ThrombosisThrombosis
�� IatrogenicIatrogenic
�� Radiation (radiation therapy for Radiation (radiation therapy for neoplasianeoplasia))
Braunwald, 8th ed.

© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� Coronary mural thickening with metabolic Coronary mural thickening with metabolic disease or intimal proliferative diseasedisease or intimal proliferative disease�� MucopolysaccharidosesMucopolysaccharidoses (Hurler disease)(Hurler disease)
�� HomocystinuriaHomocystinuria
�� FabryFabry diseasedisease
�� AmyloidosisAmyloidosis
�� Juvenile intimal sclerosis (idiopathic arterial Juvenile intimal sclerosis (idiopathic arterial calcification of infancy)calcification of infancy)
�� Intimal hyperplasia associated with contraceptive Intimal hyperplasia associated with contraceptive steroids or with the postpartum periodsteroids or with the postpartum period
�� PseudoxanthomaPseudoxanthoma elasticumelasticum
�� Coronary fibrosis caused by radiation therapyCoronary fibrosis caused by radiation therapy
Braunwald, 8th ed.
© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� Luminal narrowing by other mechanismsLuminal narrowing by other mechanisms
�� Spasm of coronary arteriesSpasm of coronary arteries ((PrinzmetalPrinzmetal
angina with normal coronary arteries)angina with normal coronary arteries)
�� Spasm after nitroglycerin withdrawalSpasm after nitroglycerin withdrawal
�� Dissection of the aortaDissection of the aorta
�� Dissection of the coronary arteryDissection of the coronary artery
Braunwald, 8th ed.

© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� Emboli to Coronary ArteriesEmboli to Coronary Arteries�� Infective endocarditisInfective endocarditis
�� Nonbacterial thrombotic endocarditisNonbacterial thrombotic endocarditis
�� ProlapseProlapse of mitral valveof mitral valve
�� Mural thrombus from left atrium, left ventricle, or pulmonary Mural thrombus from left atrium, left ventricle, or pulmonary veinsveins
�� Prosthetic valve emboliProsthetic valve emboli
�� Cardiac Cardiac myxomamyxoma
�� Associated with cardiopulmonary bypass surgery and coronary Associated with cardiopulmonary bypass surgery and coronary arteriographyarteriography
�� Paradoxical emboliParadoxical emboli
�� Papillary Papillary fibroelastomafibroelastoma of the aortic valve (of the aortic valve (““fixed embolusfixed embolus””))
�� Thrombi from Thrombi from intracardiacintracardiac catheters or catheters or guidewiresguidewires
Braunwald, 8th ed.

© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� Congenital Coronary Artery AnomaliesCongenital Coronary Artery Anomalies
�� Anomalous origin of left coronary from Anomalous origin of left coronary from
pulmonary arterypulmonary artery
�� Left coronary artery from anterior sinus of Left coronary artery from anterior sinus of
ValsalvaValsalva
�� Coronary Coronary arteriovenousarteriovenous and and arteriocameralarteriocameral
fistulasfistulas
�� Coronary artery aneurysmsCoronary artery aneurysms
Braunwald, 8th ed.

© 2010 David Stultz, MD
Differential diagnosis ofDifferential diagnosis of
““Acute MI with normal coronariesAcute MI with normal coronaries””
�� Hematological (in situ Thrombosis)Hematological (in situ Thrombosis)
�� PolycythemiaPolycythemia veravera
�� ThrombocytosisThrombocytosis
�� Disseminated intravascular coagulationDisseminated intravascular coagulation
�� HypercoagulabilityHypercoagulability, thrombosis, , thrombosis,
thrombocytopenic thrombocytopenic purpurapurpura
Braunwald, 8th ed.

© 2010 David Stultz, MD
Case 2Case 2
DonDon’’t argue with the nurset argue with the nurse
�� 7575--yearyear--old Female who was old Female who was
accompanying her husband at his accompanying her husband at his
ophthalmologist appointment. ophthalmologist appointment.
�� She suddenly became upset, short of She suddenly became upset, short of
breath, and she had an argument with breath, and she had an argument with
the nurse.the nurse.
�� Developed chest pain and diaphoresis.Developed chest pain and diaphoresis.

© 2010 David Stultz, MD
Past HistoryPast History
�� Past Medical HistoryPast Medical History
�� Poor historianPoor historian
�� DementiaDementia
�� No other significant history notedNo other significant history noted
�� Medications Medications –– NoneNone
�� Family History Family History –– Positive for CADPositive for CAD

© 2010 David Stultz, MD
Physical ExamPhysical Exam
�� Vitals Vitals –– HR 70, BP 140/70HR 70, BP 140/70
�� General General –– A&O x 3, initially no distressA&O x 3, initially no distress
�� Lungs: Clear to auscultationLungs: Clear to auscultation
�� Heart: Regular with S4 gallop.Heart: Regular with S4 gallop.
�� Neurologic: Symmetric facial Neurologic: Symmetric facial
expressions. No focal deficits.expressions. No focal deficits.

© 2010 David Stultz, MD
Baseline EKG Baseline EKG –– 3 months prior3 months prior

© 2010 David Stultz, MD
Presenting EKG 1Presenting EKG 1
Chest pain subsidedChest pain subsided
© 2010 David Stultz, MD
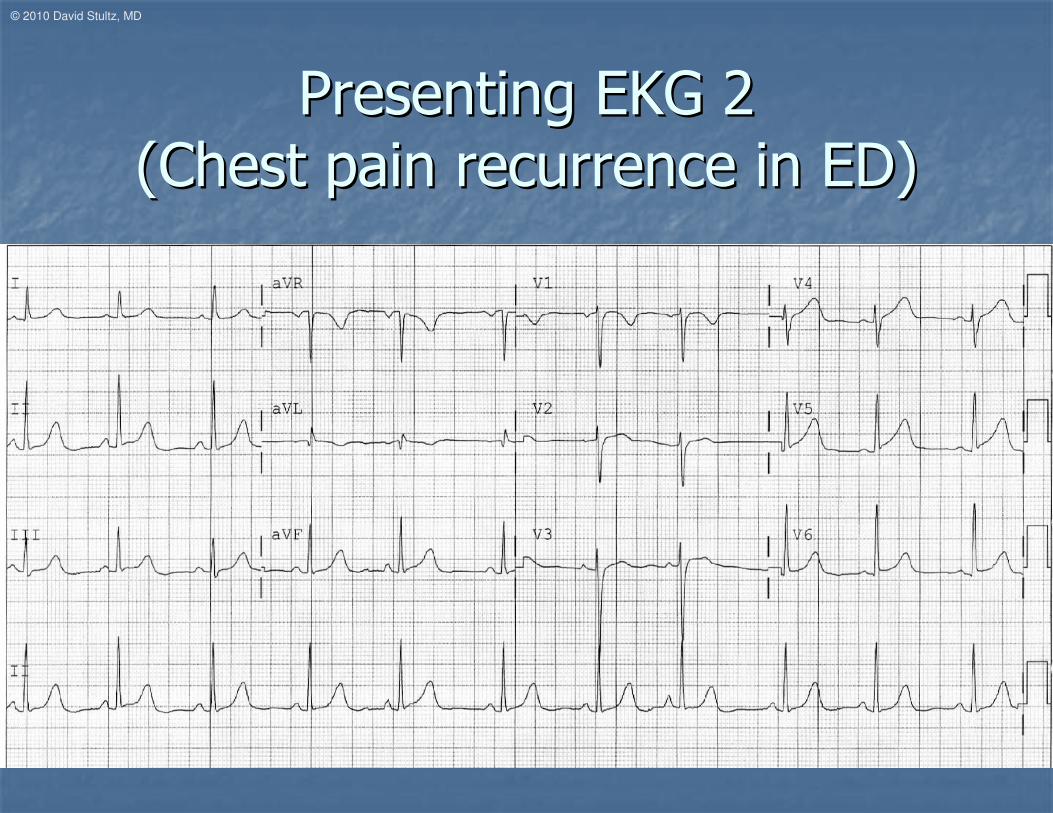
Presenting EKG 2Presenting EKG 2
(Chest pain recurrence in ED)(Chest pain recurrence in ED)
© 2010 David Stultz, MD
Inferior/Inferior/AnterolateralAnterolateral ST changes ST changes
with ongoing chest painwith ongoing chest pain
�� Taken to cardiac Taken to cardiac cathcath lab urgentlylab urgently
© 2010 David Stultz, MD
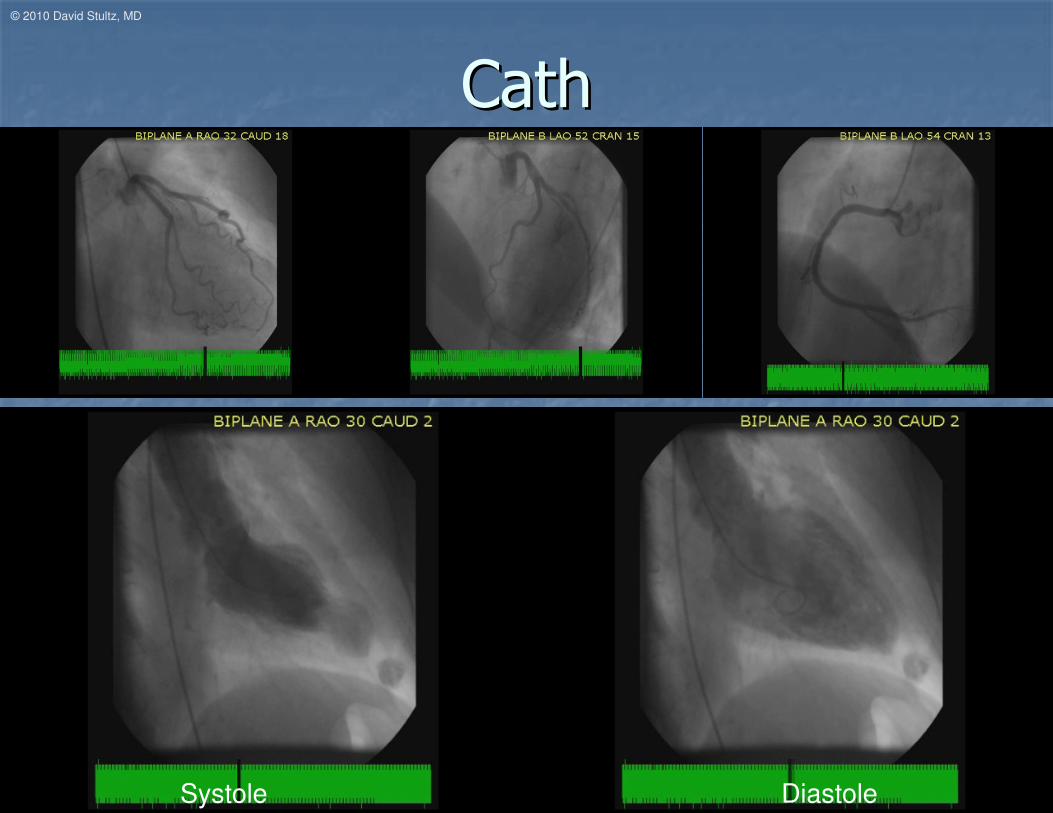
CathCath
Systole Diastole
© 2010 David Stultz, MD
LabsLabs
�� TroponinTroponin I peak 0.57ng/mL (0I peak 0.57ng/mL (0--0.49 0.49
normal)normal)

© 2010 David Stultz, MD
EKG day 2EKG day 2

© 2010 David Stultz, MD
EKG day 3EKG day 3
© 2010 David Stultz, MD
Discharge MedicationsDischarge Medications
�� AspirinAspirin 81 mg daily81 mg daily
�� ToprolToprol--XLXL 25 mg daily25 mg daily
�� LisinoprilLisinopril 10 mg daily10 mg daily
�� LipitorLipitor 40 mg daily40 mg daily
�� PlavixPlavix 75 mg daily75 mg daily
�� ProtonixProtonix 40 mg daily40 mg daily
�� Aricept daily Aricept daily

© 2010 David Stultz, MD
6 month 6 month followupfollowup
�� Overall doing wellOverall doing well
�� Still some intermittent episodes of chest Still some intermittent episodes of chest
pain well controlled with sublingual pain well controlled with sublingual
nitroglycerin as needednitroglycerin as needed

© 2010 David Stultz, MD
EKG 6 months laterEKG 6 months later
© 2010 David Stultz, MD
FollowupFollowup EchoEchoSystole Diastole

© 2010 David Stultz, MD
Profile of the typical patientProfile of the typical patient136 patients from 2001136 patients from 2001--2008, Minneapolis2008, Minneapolis
�� Mean age 68 Mean age 68 ±± 13 years13 years
�� 96% female96% female
�� 89% could identify a stressor within 12 89% could identify a stressor within 12
hours of presentationhours of presentation
�� 47% emotional (personal or family life crisis)47% emotional (personal or family life crisis)
�� 42% physical (medical illness or diagnostic 42% physical (medical illness or diagnostic
test)test)
�� Physical stressors more common in menPhysical stressors more common in menKurisu S, Inoue I, Kawagoe T, Ishihara M, Shimatani Y, Nakama Y, Kagawa E, Dai K, Ikenaga H. Presentation of Tako-tsubo
cardiomyopathy in men and women. Clin Cardiol. 2010 Jan;33(1):42-5.
Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and
expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010 Jan 26;55(4):333-41.

© 2010 David Stultz, MD
Acute ComplicationsAcute Complications
�� 3/136 died in acute phase3/136 died in acute phase�� CardiogenicCardiogenic shockshock
�� Anoxic brain injuryAnoxic brain injury
�� Traumatic Traumatic intracerebralintracerebral hemorrhagehemorrhage
�� 5/136 had apical thrombus5/136 had apical thrombus�� 2 had embolic events2 had embolic events
�� 13/136 developed LV outflow tract 13/136 developed LV outflow tract obstruction due to systolic motion of obstruction due to systolic motion of anterior mitral leafletanterior mitral leaflet
Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and
expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010 Jan 26;55(4):333-41.

© 2010 David Stultz, MD
Ejection fractionEjection fraction
�� Average EF at admission 32% Average EF at admission 32% ±± 11%11%
�� 126/136 had eventual return of EF 126/136 had eventual return of EF ≥≥50%50%
�� 94 had normal EF by 194 had normal EF by 1stst followupfollowup (51 (51 ±± 52 52
days)days)
�� 26 more had normal EF by 76 26 more had normal EF by 76 ±± 137 days137 days
Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and
expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010 Jan 26;55(4):333-41.

© 2010 David Stultz, MD
SurvivalSurvival
�� 5% had recurrence of 5% had recurrence of TakotsuboTakotsubo
Cardiomyopathy within 4.4 years of initial eventCardiomyopathy within 4.4 years of initial event
Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and
expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010 Jan 26;55(4):333-41.
© 2010 David Stultz, MD
Case 3Case 3Pain and back surgery can stress the heartPain and back surgery can stress the heart
�� 74 year old female74 year old female
�� 2 days post2 days post--op op laminectomylaminectomy for back painfor back pain
�� Extensive pain preExtensive pain pre--op and post opop and post op
�� Very anxious about hospitalizationVery anxious about hospitalization
�� Acute respiratory distressAcute respiratory distress
© 2010 David Stultz, MD
Past Medical HistoryPast Medical History
�� HypertensionHypertension
�� HyperlipidemiaHyperlipidemia
�� Coronary artery diseaseCoronary artery disease�� MI with 2 LAD stents 11 years agoMI with 2 LAD stents 11 years ago
�� Peripheral vascular diseasePeripheral vascular disease�� PTA/stents 12 years agoPTA/stents 12 years ago
�� AortofemoralAortofemoral bypass 11 years agobypass 11 years ago
�� Smokes < Smokes < ½½ pack cigarettes a daypack cigarettes a day

© 2010 David Stultz, MD
Outpatient medicationsOutpatient medications
�� AspirinAspirin 81 mg daily81 mg daily
�� AtenololAtenolol 25 mg daily25 mg daily
�� SimvastatinSimvastatin 40 mg daily40 mg daily
�� LisinoprilLisinopril 20 mg daily20 mg daily
�� HydrochlorothiazideHydrochlorothiazide 25 mg daily25 mg daily
�� AlprazolamAlprazolam 0.5 mg daily0.5 mg daily
�� FosamaxFosamax 70 mg daily70 mg daily
�� LevothyroxineLevothyroxine 25 mcg daily25 mcg daily
�� OmeprazoleOmeprazole 20 mg daily20 mg daily
�� PremarinPremarin 1.25 mg daily1.25 mg daily
�� Zoloft 50 mg dailyZoloft 50 mg daily
�� UltracetUltracet 325 mg 325 mg prnprn

© 2010 David Stultz, MD
Physical ExamPhysical Exam
�� PulePule 94, BP 92/6694, BP 92/66
�� Respirations 26, ORespirations 26, O22 saturation 98% on saturation 98% on nonrebreathernonrebreather face mask face mask
�� General: Mild respiratory distress General: Mild respiratory distress
�� Neck: Supple, No JVD notedNeck: Supple, No JVD noted
�� Lungs: ClearLungs: Clear
�� Heart: Regular, no murmursHeart: Regular, no murmurs
�� Extremities: No edema, no cyanosisExtremities: No edema, no cyanosis

© 2010 David Stultz, MD
LabsLabs
�� HgbHgb 11.7, WBW 12.3, Platelets 271,00011.7, WBW 12.3, Platelets 271,000
�� CreatinineCreatinine 1.1, Na 133, K+ 4.2, glucose 1.1, Na 133, K+ 4.2, glucose
144144
�� CKCK--MB 5.1 MB 5.1 --> 9.4> 9.4
�� TroponinTroponin I 0.03 I 0.03 --> 0.79> 0.79
�� CT Chest (PE protocol) negative for PECT Chest (PE protocol) negative for PE
© 2010 David Stultz, MD
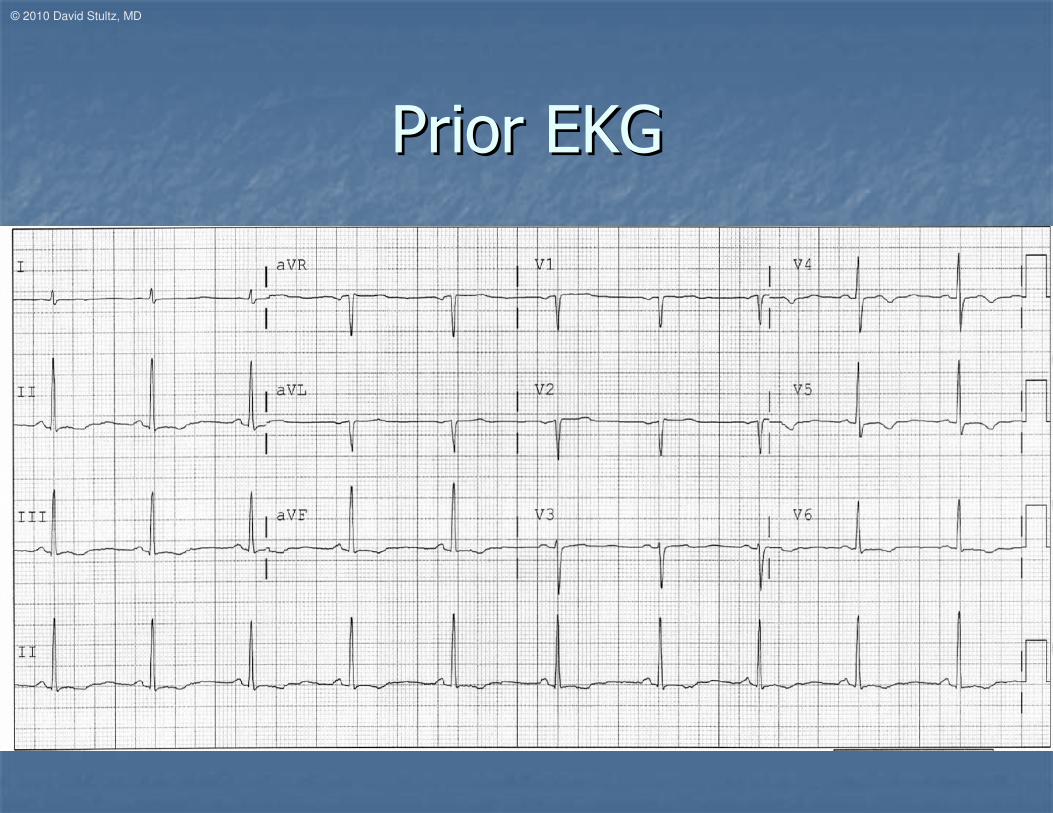
Prior EKGPrior EKG

© 2010 David Stultz, MD
Current EKGCurrent EKG

© 2010 David Stultz, MD
EchoEchoSystole Diastole

© 2010 David Stultz, MD
CathCath
Systole Diastole
© 2010 David Stultz, MD
Hospital CourseHospital Course
�� Supportive therapySupportive therapy
�� Changed to Changed to metoprololmetoprolol succinatesuccinate ((ToprolToprol
XL)XL)
�� Continued Continued lisinoprillisinopril, Aspirin, , Aspirin, simvastatinsimvastatin
© 2010 David Stultz, MD
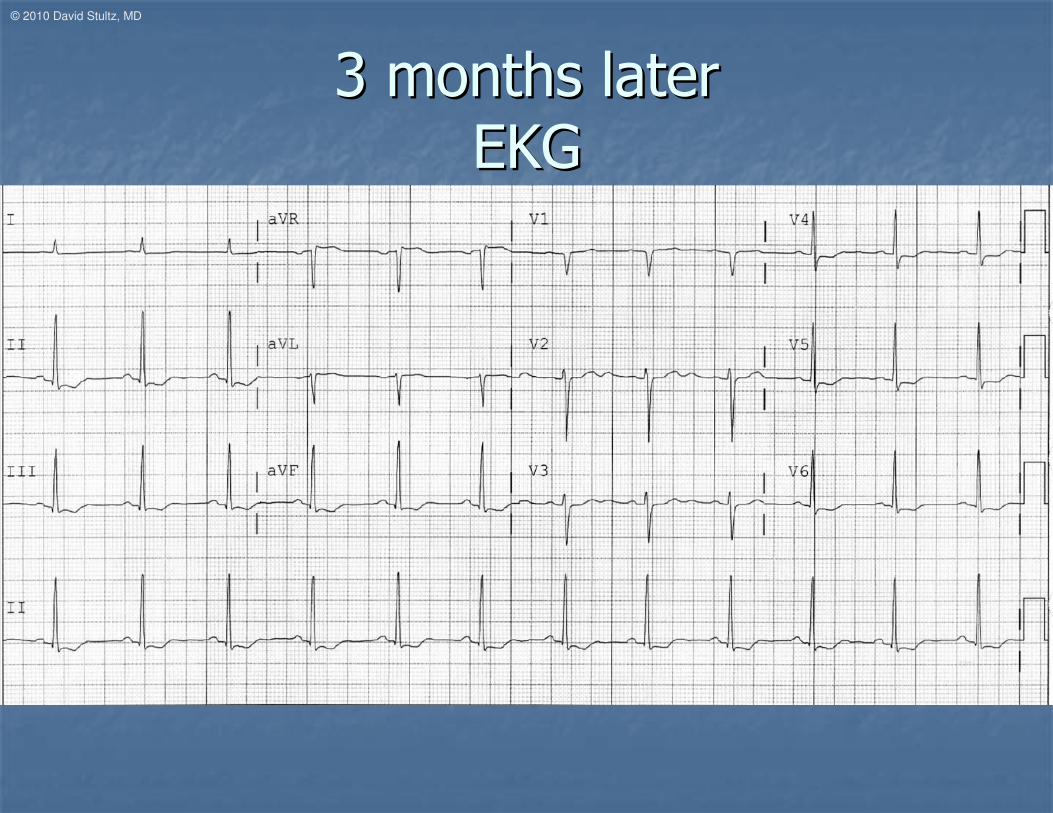
3 months later3 months later
EKGEKG

© 2010 David Stultz, MD
FollowupFollowup EchoEchoSystole Diastole

© 2010 David Stultz, MD
Role of Role of CatecholaminesCatecholamines
�� Can causeCan cause�� Acute Acute myocarditismyocarditis
�� CardiomyopathyCardiomyopathy
�� TachycardiaTachycardia
�� ArryhthmiasArryhthmias
�� MechanismsMechanisms�� Direct toxic effect on myocardiumDirect toxic effect on myocardium
�� Calcium overloadCalcium overload
�� Free radical productionFree radical production
�� Increased Increased sarcolemmalsarcolemmal permeabilitypermeability
�� Damage secondary to increased myocardial oxygen demandsDamage secondary to increased myocardial oxygen demands
�� Or decreased supply due to vasoconstrictionOr decreased supply due to vasoconstriction
Braunwald, 8th ed.

© 2010 David Stultz, MD
Variants of Variants of TakotsuboTakotsubo
CardiomyopathyCardiomyopathy
�� Reverse Reverse TakotsuboTakotsubo
�� Basal and Basal and midventricularmidventricular hypokinesishypokinesis with with
preserved apical wall motionpreserved apical wall motion
�� MidventricularMidventricular TakotsuboTakotsubo
�� MidventricularMidventricular akinesisakinesis with normal wall with normal wall
motion of basal and apical segmentsmotion of basal and apical segments
Braunwald, 8th ed.
•Davis M, Hardebeck C. Reverse Takotsubo syndrome diagnosed with Tc-99m SPECT perfusion study. J Nucl Cardiol. 2009 Nov-
Dec;16(6):999-1002.
© 2010 David Stultz, MD
Treatment of Treatment of TakotsuboTakotsubo
CardiomyopathyCardiomyopathy
�� No specific therapyNo specific therapy
�� General treatment for heart failure and NSTEMIGeneral treatment for heart failure and NSTEMI
�� Beta blockers, Ace inhibitorsBeta blockers, Ace inhibitors
�� Aspirin, statinAspirin, statin
�� LasixLasix as neededas needed
�� ? Digoxin, nitrates? Digoxin, nitrates
�� Specific treatment for complicationsSpecific treatment for complications
�� Anticoagulation for emboli, atrial fibrillationAnticoagulation for emboli, atrial fibrillation
�� Hemodynamic support as neededHemodynamic support as needed

© 2010 David Stultz, MD
ConclusionConclusion
�� TakotsuboTakotsubo cardiomyopathy mimics acute cardiomyopathy mimics acute
myocardial infarctionmyocardial infarction
�� Precipitated by emotional or physical Precipitated by emotional or physical
stressstress
�� Characteristic left ventricular wall motion Characteristic left ventricular wall motion
abnormalitiesabnormalities
�� Supportive therapySupportive therapy
�� Can have acute complicationsCan have acute complications
�� Often left ventricular function recovers Often left ventricular function recovers
© 2010 David Stultz, MD
ReferencesReferences
�� BraunwaldBraunwald E, E, ZipesZipes DP, Libby P: Heart Disease 8DP, Libby P: Heart Disease 8thth ed. Philadelphia, WB ed. Philadelphia, WB
Saunders, 2007.Saunders, 2007.
�� Brenner ZR, Powers J. Brenner ZR, Powers J. TakotsuboTakotsubo cardiomyopathy. Heart Lung. 2008 Jancardiomyopathy. Heart Lung. 2008 Jan--
Feb;37(1):1Feb;37(1):1--7.7.
�� Davis M, Davis M, HardebeckHardebeck C. Reverse C. Reverse TakotsuboTakotsubo syndrome diagnosed with Tcsyndrome diagnosed with Tc--
99m SPECT perfusion study. J 99m SPECT perfusion study. J NuclNucl CardiolCardiol. 2009 Nov. 2009 Nov--Dec;16(6):999Dec;16(6):999--1002.1002.
�� KurisuKurisu S, Inoue I, Kawagoe T, Ishihara M, S, Inoue I, Kawagoe T, Ishihara M, ShimataniShimatani Y, Y, NakamaNakama Y, Kagawa Y, Kagawa
E, Dai K, E, Dai K, IkenagaIkenaga H. Presentation of H. Presentation of TakoTako--tsubotsubo cardiomyopathy in men cardiomyopathy in men
and women. and women. ClinClin CardiolCardiol. 2010 Jan;33(1):42. 2010 Jan;33(1):42--5.5.
�� Sharkey SW, Sharkey SW, WindenburgWindenburg DC, Lesser JR, DC, Lesser JR, MaronMaron MS, Hauser RG, Lesser JN, MS, Hauser RG, Lesser JN,
Haas TS, Hodges JS, Haas TS, Hodges JS, MaronMaron BJ. Natural history and expansive clinical BJ. Natural history and expansive clinical
profile of stress (profile of stress (takotako--tsubotsubo) cardiomyopathy. J Am ) cardiomyopathy. J Am CollColl CardiolCardiol. 2010 Jan . 2010 Jan
26;55(4):33326;55(4):333--41.41.