debate risk stratification in hcm is feasible using a clinical score (con)
TRANSCRIPT

Barry J. Maron, MD Director, Hypertrophic Cardiomyopathy Center
Minneapolis Heart Institute Foundation Minneapolis, Minnesota
Disclosures: Medtronic (Grantee) GeneDx (Consultant)
Debate: Risk Stratification in HCM is Feasible
Using a Clinical Score (CON)


The ESC-HCM-Sudden death prediction formula is as follows: Probability SCD at 5 years = 1 – 0.998 exp (Prognostic index);
where Prognostic index = [0.15939858 x maximal LV wall thickness (mm)] – [0.00294271 x LV maximal wall thickness2 (mm2)] + [0.0259082 x left atrial diameter (mm)] + [0.00446131 x maximal (rest/Valsalva) LV outflow tract gradient (mm Hg)] + [0.4583082 x family history SCD] + [0.82639195 x NSVT] + [0.71650361 x unexplained syncope] – [0.01799934 x age at clinical evaluation (years)].
“When something is so complicated, you are forced to take a leap of faith”

I First Started Getting Angry Calls Right Away
Rome: “I have low risk symptomatic patient who is myectomy candidate with very high risk score because his gradient is high.”
Cleveland: “All my patients have low scores…even those who clearly seem high risk. This ESC thing doesn’t make any sense.”

DON’T USE IT
HERE IS WHY

Study Population
Minneapolis Heart Institute; Tufts Medical Center 1629 consecutive HCM patients ≥ 16 years
(1992-2014)
• Age: 47 ± 17 years
• Risk stratified by: ACC/AHA 2011; ACC/ESC 2003
• Sudden death events: 35
• Primary prevention appropriate ICD interventions: 46

% P
atie
nts
Wit
h/W
ith
ou
t IC
D In
terv
en
tio
n/S
ud
den
De
ath
Appropriate ICD
Intervention
No Appropriate ICD
Intervention
ESC Risk Score
<4% <4% 4-6% 4-6% >6% >6% Risk/5y Risk/5y
<4% 4-6% >6% Risk/5y
Sudden Death
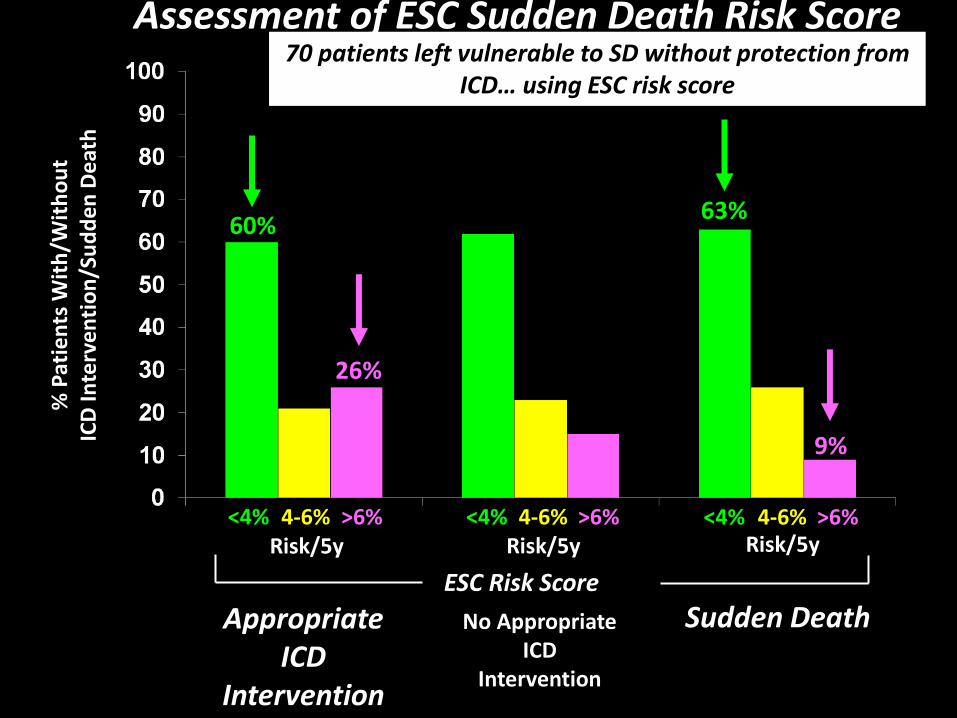
Assessment of ESC Sudden Death Risk Score (n = 1649)
60%
26%
63%
9%
70 patients left vulnerable to SD without protection from ICD… using ESC risk score

WHAT’S MISSING FROM ESC RISK MODEL?
• CMR and LGE • LV apical aneurysm • End stage (EF <50%)


LGE
LGE LGE
Extent of LGE vs. Sudden Death Risk in HCM
Follow-up (years)
Surv
ival
LGE (-) LGE < 10%
LGE 10-20%
LGE > 20%
Chan RH et. al. Circ 2014; 130(6): 484-95

QUESTIONABLE ADDITIONS TO ESC RISK MODEL
• Left atrial size • LV outflow gradient • Remote syncope
Mixed /no relation to SD risk

WHAT DOES WORK…?



Risk Stratification in HCM According to U.S. Guidelines

ICD Performance in High Risk Adults & Children with HCM
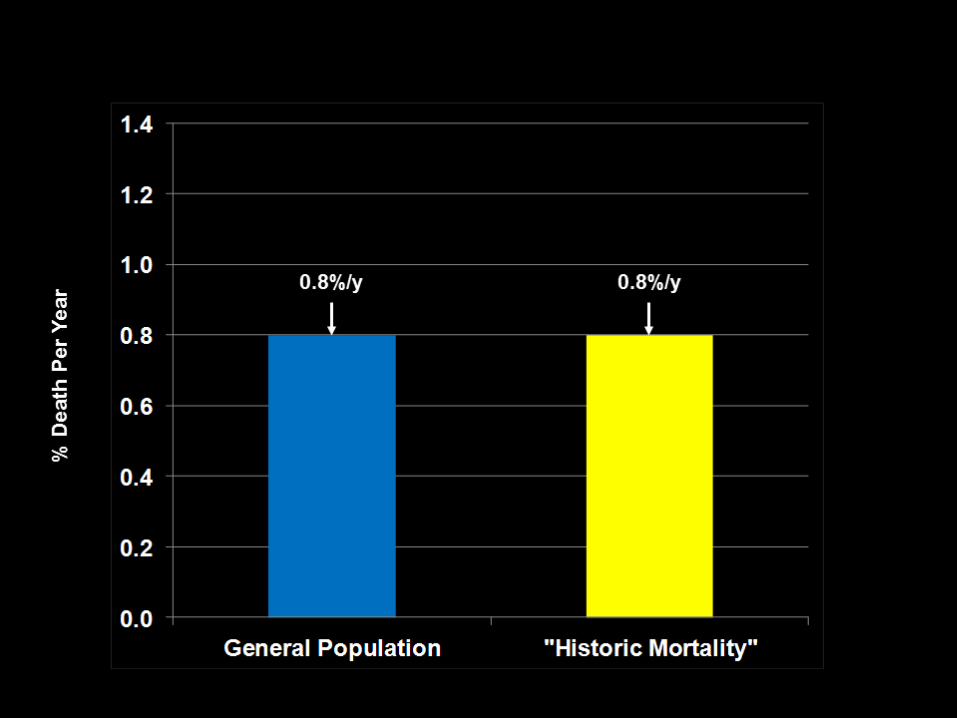
Evidence for Decreased HCM Mortality:
1000 Patients Presenting in Mid-Life (30-59y)
MHIF/ Tufts
0
0.5
1
1.5
2
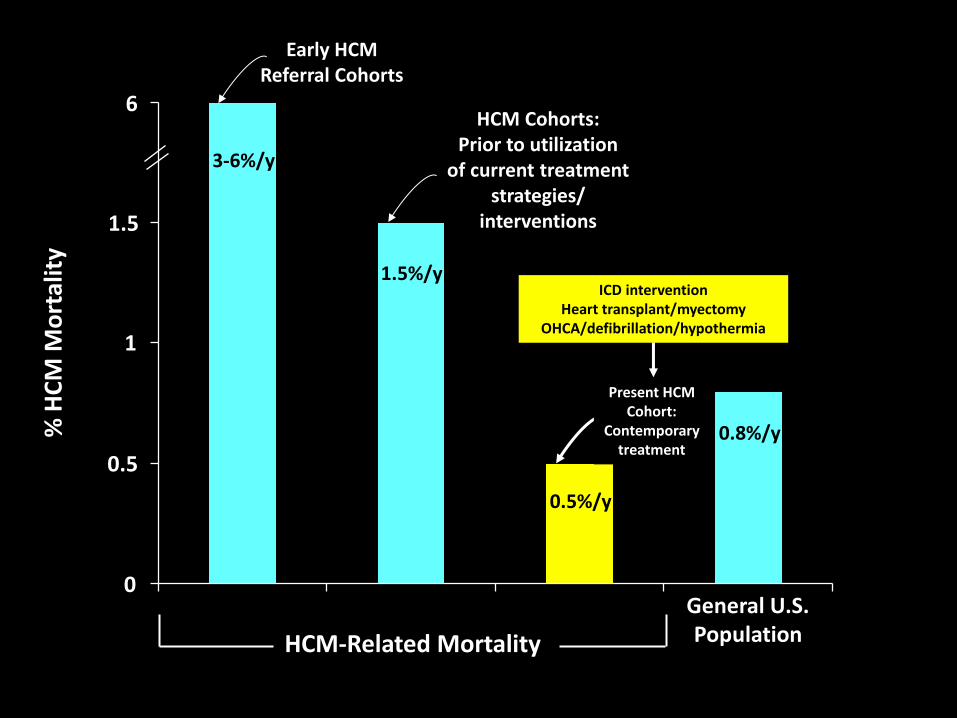
% H
CM
Mo
rtal
ity
HCM-Related Mortality
0
0.5
1.5
1
6
General U.S. Population
0.8%/y
0.5%/y
1.5%/y
3-6%/y
Early HCM Referral Cohorts
HCM Cohorts: Prior to utilization
of current treatment strategies/
interventions
ICD intervention Heart transplant/myectomy
OHCA/defibrillation/hypothermia
Present HCM Cohort:
Contemporary treatment

ESC Prognostic Score…
1. Misclassifies most HCM patients with SD or ICD interventions with low risk scores
2. Fails to protect most patients from SD without ICDs
3. Is inferior to conventional risk stratification according to ACC/AHA (HCM) Guidelines
Risk stratification in HCM often requires fully informed patient and measure of physician judgment in shared decision making—not
possible with rigid math/stats prediction formula

ARE WE CLINICIANS…
OR STATISTICIANS??

Rebuttal


THERE REALLY IS NO MIDDLE GROUND HERE
INTUITIVELY…
How can a complex mathematical model with 7 variables, including 2 which have little
to do with SD, reliably predict SD in a heterogeneous genetic disease in which SD
events are uncommon (5%)?
Answer:

IT DOESN’T
% P
atie
nts
Wit
h/W
ith
ou
t IC
D In
terv
en
tio
n/S
ud
den
De
ath
Appropriate ICD
Intervention
No Appropriate ICD
Intervention
ESC Risk Score
<4% <4% 4-6% 4-6% >6% >6% Risk/5y Risk/5y
<4% 4-6% >6% Risk/5y
Sudden Death
Assessment of ESC Sudden Death Risk Score (n = 1649)
60%
26%
63%
9%
70 patients left vulnerable to SD without protection from ICD… using ESC risk score

Who Does ESC Risk Score Miss?
• Virtually all nonobstructive patients with massive LVH
• Most with syncope as single risk marker
• Many with family history of SD as single risk marker
• Some with 2 risk factors: family history SD + NSVT
General
• 30 y/o + syncope + LV 34mm
• 40 y/o + NSVT + LV 30mm
• 20 y/o + family history SD + LV >25mm
Specific

“Truth is what your contemporaries let you get away with.”
Richard Rorty, 1931-2007

WHAT’S MISSING FROM ESC RISK MODEL?
• CMR and LGE • LV apical aneurysm • End stage (EF <50%)

1.0
0.8
0.6
0.4
0.0
0 5 15 10 20
HCM patients without LV apical aneurysms
HCM patients with LV apical aneurysm
Log-rank test p<0.001
Years from First Evaluation
Su
rviva
l fre
e fro
m H
CM
re
late
d
mo
rta
lity a
nd
a
dve
rse
eve
nts
0.2
HCM Related Death or Adverse Clinical Events
in 70 Patients with LV Apical Aneurysms
8.1%/year
1.7%/year

70 patients left vulnerable to SD without protection from ICD… using ESC risk score

70 patients left vulnerable to SD without protection from ICD… using ESC risk score

70 patients are left vulnerable to sudden death without protection from the ICD…when using ESC risk score

No Risk Factors: Unnecessary ICD
Over-Treatment : ESC Risk Score
• LVOTG 100 mm Hg + LA 50mm (40 y/o)
• LVOTG 0 + LA 55mm (18 y/o)
• LVOTG 50 mm Hg + LA 40mm (20 y/o)


0
10
20
30
40
50
60
70
80
90
100%
Pat
ien
ts W
ith
/Wit
ho
ut
ICD
Inte
rve
nti
on
/Su
dd
en D
eat
h
Appropriate ICD
Intervention
No Appropriate ICD
Intervention
<4% 4-6% >6%
Risk/5y
Sudden Death*
<4% 4-6% >6%
Risk/5y
<4% 4-6% >6%
Risk/5y
<4% 4-6% >6%
Risk/5y
Survivors Without
ICDs/Events
ESC Risk Score
70 patients are left vulnerable to sudden death without protection from the ICD…when using ESC risk score

no risk
factors age
maximum
wall
thickness 16 18 20 25 30 35 40 45 50 55 60 65 70
10 1.80 1.74 1.68 1.53 1.40 1.28 1.17 1.07 0.98 0.90 0.82 0.75 0.68
12 2.17 2.09 2.02 1.85 1.69 1.55 1.41 1.29 1.18 1.08 0.99 0.90 0.83
14 2.56 2.47 2.38 2.18 1.99 1.82 1.67 1.53 1.39 1.28 1.17 1.07 0.98
16 2.94 2.84 2.74 2.51 2.29 2.10 1.92 1.76 1.61 1.47 1.34 1.23 1.12
18 3.31 3.19 3.08 2.82 2.58 2.36 2.16 1.98 1.81 1.65 1.51 1.38 1.26
20 3.63 3.50 3.38 3.10 2.83 2.59 2.37 2.17 1.99 1.82 1.66 1.52 1.39
22 3.90 3.76 3.63 3.32 3.04 2.78 2.55 2.33 2.13 1.95 1.78 1.63 1.49
24 4.08 3.94 3.80 3.48 3.19 2.92 2.67 2.44 2.24 2.04 1.87 1.71 1.56
26 4.18 4.04 3.90 3.57 3.27 2.99 2.74 2.50 2.29 2.10 1.92 1.75 1.60
28 4.19 4.04 3.90 3.57 3.27 2.99 2.74 2.51 2.29 2.10 1.92 1.75 1.60
30 4.09 3.95 3.82 3.49 3.20 2.93 2.68 2.45 2.24 2.05 1.88 1.72 1.57
32 3.91 3.78 3.65 3.34 3.06 2.80 2.56 2.34 2.14 1.96 1.79 1.64 1.50
34 3.66 3.53 3.41 3.12 2.85 2.61 2.39 2.19 2.00 1.83 1.67 1.53 1.40
36 3.34 3.22 3.11 2.84 2.60 2.38 2.18 1.99 1.82 1.67 1.53 1.39 1.28
38 2.97 2.87 2.77 2.53 2.32 2.12 1.94 1.78 1.62 1.49 1.36 1.24 1.14
40 2.59 2.50 2.41 2.21 2.02 1.85 1.69 1.54 1.41 1.29 1.18 1.08 0.99
Calculated 5-year Risk in Patients Without Conventional Risk Factors (using left atrial size =44mm and LVOT gradient =12mmHG)

0
1
2
3
4
Sudden Death Appropriate ICDIntervention
No AppropriateIntervention
Survivors WithoutICDs/Events
Series 1
3.8
ESC
Ris
k Sc
ore
ICDs
3.2 3.3
2.1
ns
p < 0.001








Using the ESC Risk Score…
65 of our patients would have been vulnerable to sudden death without protection from ICDs.

CONTEMPORARY HCM MORTALITY BY AGE
<29 y 30-59 y >60 y Total
No. Patients
474 1000 428 1902
HCM Mortality
0.5%/y 0.5%/y 0.6%/y 0.5%/y

Evidence for Reduced HCM Mortality:
n=1000 Presenting 30-59y
What is possible………

Contemporary C-V treatment options offer HC patients a reasonable aspiration for
reduced mortality and extended longevity. The ICD has altered clinical course
affording the possibility of normal or near normal life expectancy.