december 2017 practical nursing · 2019-09-29 · a current resume of the nominee must be submitted...
TRANSCRIPT

PRACTICAL NURSINGCOMMITTED TO EXCELLENCE
December 2017
Janou Dufresne, LPN volunteered as a nurse in Vietnam through the International Volunteer HQ program. Read more about Janou’s experience on page 16.
2Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
3Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
TABLE OF CONTENTS
College of Licensed Practical Nurses of Manitoba463 St. Anne’s Road Winnipeg, MB R2M 3C9 Telephone: (204) 663-1212 Toll Free: 1-877-663-1212 Email: [email protected]
Publications Agreement #40013238
Fragrance-Free NoticeIn response to health concerns, CLPNM has a Fragrance-Free Policy and is a scent-free environment. Please do not use scented products while on the CLPNM premises for work, education, appointments, or other business.
PRESIDENT Cheryl Geisel LPN
BOARD OF DIRECTORS District I – Jodi La France LPN – Jacqueline Hornsby LPN District II – Elisa Wiebe LPN – Camille Martyniw LPN – Rodney Hintz LPN – Kristi Cantelo LPN Public Members – Tricia Conroy – Darlene Barbe – Diwa Marcelino – Gary McPherson – Robert Young
EXECUTIVE DIRECTOR Jennifer Breton, LPN RN BN
EXECUTIVE OFFICE Vicky Bering Executive Operations Coordinator
Buffie Babb, B Comm (Hons) CPA CGA Business Manager
Renata Neufeld, BA (Hons) MPA Consultant, Policy, Governance and Communications
REGISTRATION DEPARTMENT Carrie Funk, LPN Deputy Registrar
Kathy Halligan, BA (Hons) CTESL CACE Consultant, Credential Assessment
Dina Bering Registration Coordinator
CONDUCT DEPARTMENT Christy Froese, LPN Conduct Case Manager
RECEPTION AND ADMINISTRATIVE SUPPORT Kennedy Gagawchuk Administrative Assistant
Gail Bialek Administrative Assistant
PROFESSIONAL NURSING PRACTICE DEPARTMENT Tracy Olson, LPN Consultant, Practice
EDUCATION AND PROGRAM EVALUATION DEPARTMENT Brenda Wohlgemuth, LPN BA Consultant, Education Programs Evaluation
ADVERTISINGTo advertise in the Practical Nursing Journal, please contact: McCrone Publications Inc. Email: [email protected] Toll Free: 1-800-727-0782 Fax: 1-866-413-9328
2017/2018 Office Closure DatesOffice closed at 1200hrs December 21, 2017 and re-opens at 0930hrs January 2, 2018
January 16
Office closed
February 13
from 0930hrs to
1300hrs only
February 19
March 30
April 2
May 21
June 4
June 21
July 2
Office closed July 30 and re-opens at 0930hrs August 13
September 3
October 8
November 12
Office closed at 1200hrs December 21, 2018 and re-opens at 0930hrs January 2, 2019
President’s Message 4
Call for Nominations 2018 5
Nomination Rules 6
RHPA Status Update 7
Investigation Committee Activity Report to the Board of Directors 8
Understanding Your Professional Standards 12
Nursing Abroad Enriched my Nursing Practice in Manitoba 16
Cannabis: True or False? 19
Results of the 2017 Suitability Check Pilot Program 20
Ask a Practice Consultant: Nursing Leadership Practice 21
Practice Direction: Assignment and Delegation to Unregulated Care Providers
23
Practice Direction: Fitness to Practice 27
2017 CCP Audit Notice 29
Returning to LPN Practice 30
January 2018 Student Registration Renewal 32
2017/2018 Fee Schedule 33

Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba4
PRESIDENT’S MESSAGE
As this year draws to a close, our province has seen a number of
significant changes in the operation of our healthcare system. The
College of Licensed Practical Nurses of Manitoba (CLPNM) recognizes
that changes of this scale can lead to a great deal of uncertainty.
CLPNM has been meeting with many employers and programs across the province to share this information.
While the scope of LPN practice is not changing, these inquiries might suggest that employers are seeking ways to ensure they are utilizing all members of the health care team, including LPNs, to full scope.
Manitobans benefit when all health system resources – including human resources – are optimized. The CLPNM will continue its conversations with employers as one of its ongoing efforts to serve the public interest.
Although uncertainty can be difficult, it can also bring opportunity. For example, taking a closer look at how health services are delivered presents an opportunity to identify skills and resources that are already available within the system, and that could be better utilized to meet the health needs of Manitobans.
Employers have begun contacting the CLPNM to seek out information on the scope, education and competencies of a licensed practical nurse (LPN) in order to assist them with health service planning. In response, the
– Cheryl Geisel, LPN
I wish all of our registrants a very Merry Christmas and Happy Holidays. To those working over the holiday season, thank you for your unwavering commitment to making Manitobans’ safety and health your top priority.

5Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Call for Nominations – Board of Directors
In accordance with Article 5 of the CLPNM By-Laws, election of the Board of Directors shall be held by May 1 each year. The positions of the Directors stated below expire June 4, 2018, and are now open for nomination. All registrants on the active practicing register of the College of Licensed Practical Nurses of Manitoba, whose primary location of practice falls within the electoral District that is accepting nominations, are invited to submit names of nominees:
District 1 (within Winnipeg city limits): One vacancy
District 2 (outside Winnipeg city limits): Two vacancies
To view the area captured within the Winnipeg city limits, please see here.
ProcessA current resume of the nominee must be submitted with the original nomination form by February 23, 2018, at 1630hrs. Forms that are not accurately completed will not be accepted. Please refer to the Nominations Rules for more information.
Nominator InformationWe (1) Print: , Registration Number
Signature , Date
(2) Print: , Registration Number
Signature , Date
(3) Print: , Registration Number
Signature , Date
Registrants in good standing on the active practicing register of the College of Licensed Practical Nurses of Manitoba, in accordance with approved Nomination Rules do hereby nominate (print name) to represent District on the Board of Directors of the CLPNM.
Nomination AcceptanceNote for nominees: regular attendance at board meetings is required of all board members. The board is expected to meet six to seven times per year. Future board meeting dates are available on the CLPNM website here. Please ensure that you review these dates prior to accepting a nomination.
I (print name), , registration number , a registrant in good standing on the active practicing register of the CLPNM, whose primary location of practice falls within District do hereby accept the nomination for election to the position of Director on the Board of the CLPNM. I declare that I have reviewed the Nomination Rules and I confirm that I meet the criteria for nomination and for membership on the board, as described therein. I declare that if elected I do hereby consent to serve as a Board Director for the term 2018-2020.
Signed this day of ,20 .
Signature: (nominee).
CALL FOR NOMINATIONS 2018

6Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
NOMINATION RULES
1. Nomination forms shall be submitted to the CLPNM by the deadline.
2. Each nominee is eligible to run in one electoral district per election.
3. To be eligible for nomination and for membership on the Board of Directors, a practising registrant must:
a. be registered in good standing with the CLPNM
b. have a primary location of practice that falls within the electoral district in which he or she is seeking nomination
c. not have any union affiliation other than that required for employment
d. not hold an employment position as a manager of LPNs with responsibility for hiring, evaluations, discipline or terminations of LPNs
e. not currently be a member of another regulated health profession
f. not be the subject of an ongoing CLPNM investigation or disciplinary proceeding
g. not have been the subject of a finding under The Licensed Practical Nurses Act, and
h. not have been convicted of an indictable offence.
4. A valid nomination includes:
a. a complete CLPNM-approved nomination form,
b. the signature of at least three (3) CLPNM registrants who are in good standing on the active practising register and whose primary location of practice falls within the electoral district in which the candidate is nominated,
c. the written consent of the nominee,
d. current resume of the nominee, and
e. a signed declaration of eligibility and consent from the nominee.
5. Nomination forms that have been altered or changed must be initialed by the nominee and by all three (3) nominators in order to be valid.
6. To be eligible, the College must receive all required documents on or before the established deadline date by email or regular mail.
7. If the number of eligible nominees in any electoral district does not exceed the number of vacancies in that district, the nominee shall be elected by acclamation.
Source: CLPNM Policy BG-4 Nominations and Elections, and CLPNM By-Law Articles 4, 5 and 8
Published: December 12, 2017

7Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
RHPA STATUS UPDATE
Licensed Practical Nurses (LPN) may have heard that registered nurses (RNs) will be governed under
The Regulated Health Professions Act (RHPA), beginning May 31, 2018. This may leave some LPNs wondering
if the RHPA will govern their profession and practice at the same time. Here are some answers to a few
questions you may have.
When will LPNs transition to the RHPA?
The Government of Manitoba has not yet announced when the practical nursing profession will transition to the RHPA. In the meantime, LPNs will continue to be regulated under the LPN Act.
I’ve heard that the RHPA authorizes RNs to perform certain health care activities defined as “reserved acts.” Does that mean these activities will be “reserved” for the RN profession exclusively, and no other profession will be authorized to perform them?
No. If more than one health profession has the competence to perform an activity defined in the RHPA as a reserved act, the Government of Manitoba may authorize more than one health profession to perform it.
Will LPNs be regulated under the RHPA beginning May 31, 2018, at the same time as the province’s RNs?
No. The LPN profession will transition to the RHPA at a later date. That date has not yet been determined.
Will my practice be affected after May 31, 2018, when RNs are regulated under the RHPA but LPNs are not?
No. As an LPN, your practice and authority will not be affected by the RNs’ transition to the RHPA.
You will continue to be governed under the LPN Act and regulated in accordance with the existing standards of your profession.
Which reserved acts will be authorized for LPNs when the RHPA takes effect for the practical nursing profession?
This decision has not yet been made. As part of the RHPA transition process, the CLPNM will make recommendations to the Government of Manitoba. These recommendations will be informed by consultations with LPNs, educators, employers and other stakeholders. The CLPNM will identify, in its proposal, the activities LPNs are performing safely and competently within Manitoba’s health care system today. Ultimately, the Government of Manitoba will determine which reserved acts to authorize for each health profession.
Where can I learn more about the reserved acts?
You can review the CLPNM’s FAQs on the reserved acts here.
What if I have more questions?
Please contact the CLPNM by email at [email protected] or by phone at 204-663-1212 or 1-877-663-1212 toll free.

8Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
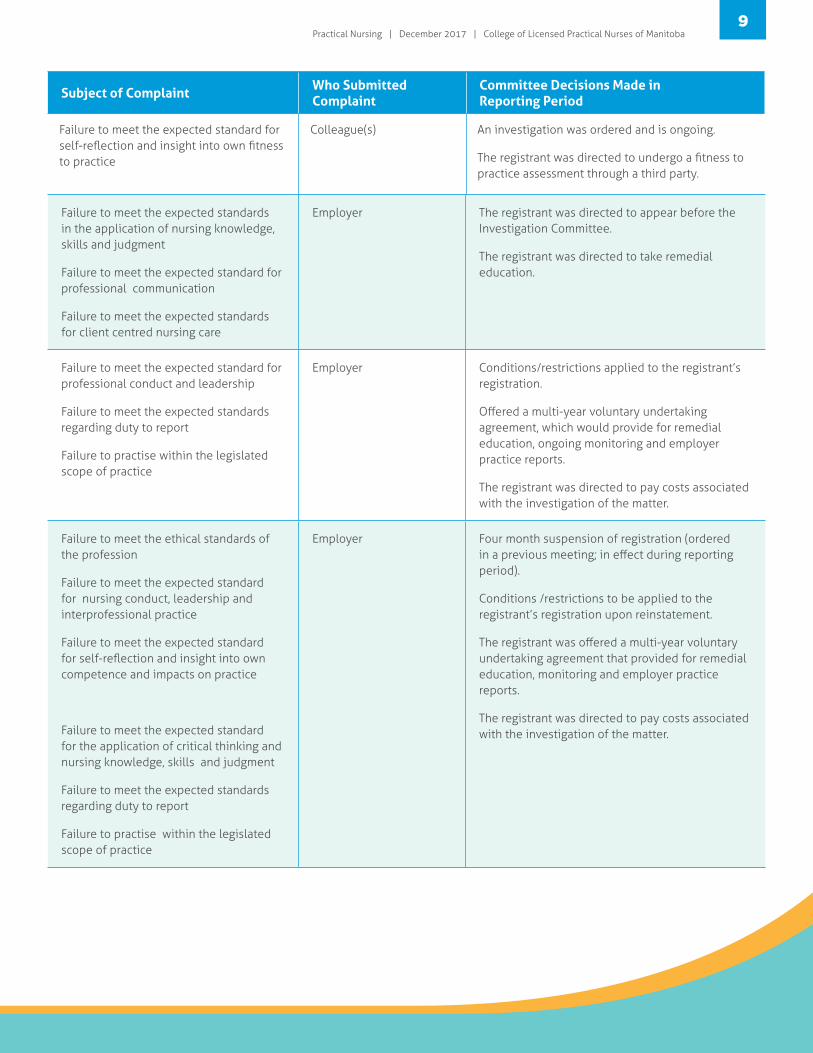
INVESTIGATION COMMITTEE ACTIVITY REPORT TO THE BOARD OF DIRECTORS
Reporting Period: August 18, 2017 – November 17, 2017
Subject of Complaint Who Submitted Complaint
Committee Decisions Made in Reporting Period
Failure to meet expected standard for professional conduct
Failure to meet the expected standards for the application of nursing knowledge, skills and judgment
Employer Conditions/restrictions applied to the registrant’s registration.
An investigation was ordered and is ongoing.
Failure to meet the expected standards related to the obligations of a regulated health professional
Failure to meet the expected standard for self-reflection and insight into own fitness to practice
CLPNM
Executive Director
Registrant does not hold current active practicing registration.
Conditions/restrictions to be applied to the registrant’s registration should they be eligible to reinstate.
Offered a multi-year voluntary undertaking agreement, which would provide for ongoing monitoring and employer practice reports.
Failure to meet the expected standard for self-reflection and insight into own fitness to practice
CLPNM Executive Director Conditions/restrictions applied to the registrant’s registration.
Offered a multi-year voluntary undertaking agreement, which provides for ongoing monitoring and employer practice reports.
Failure to meet the expected standards for the application of nursing knowledge, skills and judgment
CLPNM
Executive Director
A practice audit was ordered and is ongoing.
Failure to meet the expected standards for the application of nursing knowledge, skills and judgment
Employer Conditions/restrictions applied to the registrant’s registration.
A practice audit was ordered and is ongoing.
An investigation was ordered and is ongoing.
Failure to meet the expected standards in the application of nursing knowledge, skills and judgment
Failure to meet the expected standards for client centred nursing care
Employer Conditions/restrictions applied to the registrant’s registration.
An investigation was ordered and is ongoing.
9Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Subject of Complaint Who Submitted Complaint
Committee Decisions Made in Reporting Period
Failure to meet the expected standard for self-reflection and insight into own fitness to practice
Colleague(s) An investigation was ordered and is ongoing.
The registrant was directed to undergo a fitness to practice assessment through a third party.
Failure to meet the expected standards in the application of nursing knowledge, skills and judgment
Failure to meet the expected standard for professional communication
Failure to meet the expected standards for client centred nursing care
Employer The registrant was directed to appear before the Investigation Committee.
The registrant was directed to take remedial education.
Failure to meet the expected standard for professional conduct and leadership
Failure to meet the expected standards regarding duty to report
Failure to practise within the legislated scope of practice
Employer Conditions/restrictions applied to the registrant’s registration.
Offered a multi-year voluntary undertaking agreement, which would provide for remedial education, ongoing monitoring and employer practice reports.
The registrant was directed to pay costs associated with the investigation of the matter.
Failure to meet the ethical standards of the profession
Failure to meet the expected standard for nursing conduct, leadership and interprofessional practice
Failure to meet the expected standard for self-reflection and insight into own competence and impacts on practice
Failure to meet the expected standard for the application of critical thinking and nursing knowledge, skills and judgment
Failure to meet the expected standards regarding duty to report
Failure to practise within the legislated scope of practice
Employer Four month suspension of registration (ordered in a previous meeting; in effect during reporting period).
Conditions /restrictions to be applied to the registrant’s registration upon reinstatement.
The registrant was offered a multi-year voluntary undertaking agreement that provided for remedial education, monitoring and employer practice reports.
The registrant was directed to pay costs associated with the investigation of the matter.
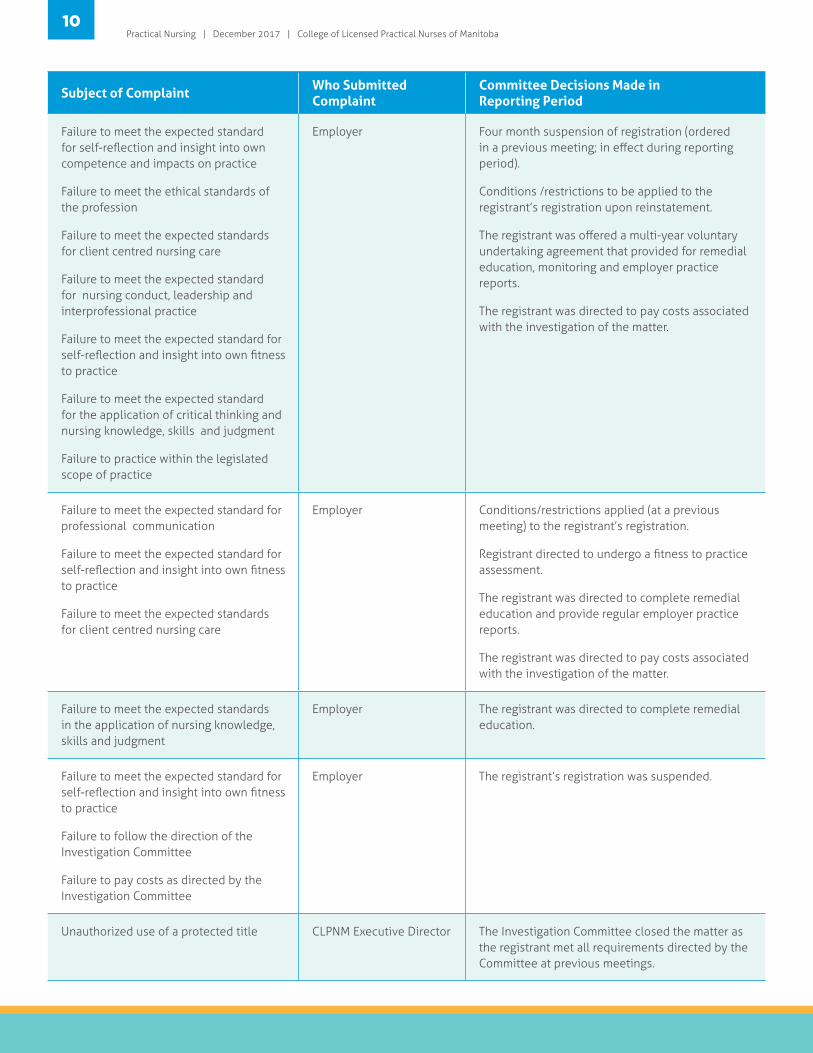
10Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Subject of Complaint Who Submitted Complaint
Committee Decisions Made in Reporting Period
Failure to meet the expected standard for self-reflection and insight into own competence and impacts on practice
Failure to meet the ethical standards of the profession
Failure to meet the expected standards for client centred nursing care
Failure to meet the expected standard for nursing conduct, leadership and interprofessional practice
Failure to meet the expected standard for self-reflection and insight into own fitness to practice
Failure to meet the expected standard for the application of critical thinking and nursing knowledge, skills and judgment
Failure to practice within the legislated scope of practice
Employer Four month suspension of registration (ordered in a previous meeting; in effect during reporting period).
Conditions /restrictions to be applied to the registrant’s registration upon reinstatement.
The registrant was offered a multi-year voluntary undertaking agreement that provided for remedial education, monitoring and employer practice reports.
The registrant was directed to pay costs associated with the investigation of the matter.
Failure to meet the expected standard for professional communication
Failure to meet the expected standard for self-reflection and insight into own fitness to practice
Failure to meet the expected standards for client centred nursing care
Employer Conditions/restrictions applied (at a previous meeting) to the registrant’s registration.
Registrant directed to undergo a fitness to practice assessment.
The registrant was directed to complete remedial education and provide regular employer practice reports.
The registrant was directed to pay costs associated with the investigation of the matter.
Failure to meet the expected standards in the application of nursing knowledge, skills and judgment
Employer The registrant was directed to complete remedial education.
Failure to meet the expected standard for self-reflection and insight into own fitness to practice
Failure to follow the direction of the Investigation Committee
Failure to pay costs as directed by the Investigation Committee
Employer The registrant’s registration was suspended.
Unauthorized use of a protected title CLPNM Executive Director The Investigation Committee closed the matter as the registrant met all requirements directed by the Committee at previous meetings.

11Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Subject of Complaint Who Submitted Complaint
Committee Decisions Made in Reporting Period
Failure to meet the expected standards in the application of nursing knowledge, skills and judgment
Employer Registrant does not hold active practicing registration.
Registrant directed to undergo an assessment prior to determining eligibility to reinstate registration.
Failure to meet the expected standards related to the obligations of a regulated health professional
Failure to comply with direction from the CLPNM
CLPNM Executive Director The registrant was directed to complete remedial education and to complete education related to the jurisprudence of the profession.
Failure to meet the expected standards in the application of nursing knowledge, skills and judgment
Failure to meet the expected standard for interprofessional practice
Employer The matter was closed as the registrant satisfactorily met all of the requirements and directions of a two year voluntary undertaking agreement.
Failure to meet the expected standard related to professional communication, confidentiality and privacy
Member of the Public The matter was closed as the registrant met all of the direction set forth by the Investigation Committee at previous meetings.
Failure to practise within the legislated scope of practice
Employer The matter was closed as the registrant met all of the direction set forth by the Investigation Committee at previous meetings.
Failure to meet the expected standards related to the obligations of a regulated health professional
Failure to meet the expected standard for ethical and professional interprofessional and intraprofessional practice
Employer The registrant’s registration was suspended for four months (decision made in a previous meeting).
Conditions/restrictions to be applied to registration when the registrant reinstates.
The registrant was offered a multi-year voluntary undertaking agreement that provided for ongoing monitoring of practice and conduct.
Failure to meet the expected standard for self-reflection and insight into own fitness to practice
CLPNM Executive Director Conditions/restrictions applied to the registrant’s registration.
The registrant was offered a multi-year voluntary undertaking agreement which provided for monitoring, remedial education and employer practice reports.
Failure to meet the expected standards in the application of nursing knowledge, skills and judgment
Employer The Investigation Committee closed the matter as the registrant met all requirements directed by the Committee at previous meetings.

12Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
UNDERSTANDING YOUR PROFESSIONAL STANDARDS
Regulatory Bulletins are now Practice Directions!
For greater consistency across regulated health professions, the CLPNM’s regulatory bulletins are now called practice directions. The name change does not change the intent or effect of these documents.
Standards of practice, practice directions, professional standards… what does all this mean?
Practical nurses may find themselves wondering how all the documents that guide the practical nursing
profession relate to one another. This overview is intended to clarify the purpose and effect of the documents
that guide practical nurses and their practice in Manitoba.
Professional Standards
Professional standards communicate how members of the profession are expected to practise and conduct themselves. They ensure that the public can expect a consistent level of professionalism and competence from all members of a regulated profession.
Professional standards, unlike the College of Licensed Practical Nurses of Manitoba’s (CLPNM) general guidance documents, establish professional responsibilities. A failure to meet the professional responsibilities described in these documents could result in an investigation, practice audit, and potentially in professional discipline.
The CLPNM has three types of documents that establish and describe professional standards:
The Code of Ethics, which describes the ethical standards of the profession.
The Standards of Practice, which describe the standards for professional nursing practice and conduct.
Practice Directions, which are used to enhance, explain or expand on the professional responsibilities described in the Standards of Practice. While the Standards of Practice are general and high-level, practice directions tend to provide detailed guidance on a specific topic.
All licensed practical nurses (LPN), graduate practical nurses (GPN), and student practical nurses (SPN) are expected to practise and conduct themselves in accordance with professional responsibilities described in these documents. All of these documents are available on the CLPNM website.
Guidance Documents
Guidance documents are used as communication tools to share information that may be helpful to CLPNM applicants and registrants, employers and other stakeholders.
The CLPNM’s guidance documents do not, on their own, create enforceable requirements, but many of them exist to help CLPNM registrants better understand requirements that have already been established in law, professional standards, or CLPNM policy. The CLPNM has several types of guidance documents, including competency documents, fact sheets, guides and interpretive documents.
Competency Documents
These documents are intended to help LPNs, employers and other stakeholders understand the competencies of a Manitoba LPN. These include the entry-level competencies, which are expected of all those who join the profession, and the broader nursing competencies for LPNs, which include competencies that fall within the scope of the profession, but which may vary between LPNs depending on their education and experience.
Fact Sheets and Guides provide information about CLPNM programs and processes, or “how to” instructions. The Continuing Competence Program (CCP) Instruction Guide is an example. It does not create the requirement to participate in the CLPNM’s Continuing Competence Program; that obligation is created in the LPN Act, and the details of the program are set out in the

13Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
CLPNM’s CCP practice direction. The CCP Instruction Guide does, however, explain to LPNs each of the steps they must follow in order to meet the requirements of the program.
Interpretive Documents are developed to clarify and promote the understanding of concepts or requirements described in legislation, regulations, and professional standards. At the present time, the
CLPNM has only published one interpretive document on the Duty to Report. As the profession nears coming under The Regulated Health Professions Act (RHPA), practical nurses can expect to see several more interpretive documents.
OVERVIEW OF DOCUMENTS THAT GUIDE THE PRACTICAL NURSING PROFESSION IN MANITOBA
LEGISLATIONAND BY-LAWS
PROFESSIONALSTANDARDS
GUIDANCEDOCUMENTS
Establishes practical nursing as a profession. Describes the CLPNM’s duty and authority, requirements for registration, and offences, among other things.
Describes detailed requirements for registration and renewal, and requirements for practical nursing education programs.
Describe rules for election and appointment to the CLPNM Board of Directors, member fees, and member rights and obligations, among other things.
Describe general responsibilities for professional practice and conduct that apply to all members in all settings.
Describes the ethical responsibilities of members of the profession.
Describe responsibilities for professional practice and conduct in more detail than the Standards of Practice, or in relation to a specific area of practice or topic.
Describe entry-level competencies expected of all new LPNs and additional competencies that fall within the full scope of the profession.
Clarify and explain concepts and requirements in law or professional standards.
Offer information about CLPNM processes or programs, and “how to” instructions.
THE LICENSED PRACTICAL NURSES ACT
THE LICENSED PRACTICAL NURSES REGULATION
THE CLPNMBY-LAWS
STANDARDS OFPRACTICE
CODE OF ETHICS
PRACTICE DIRECTIONS
COMPETENCY DOCUMENTS
INTERPRETIVEDOCUMENTS
FACT SHEETS AND GUIDES

14Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Laws and By-Laws
Legislation also guides the profession. Although there are several pieces of legislation that establish obligations for health care professionals in general,1 the legislation that governs the profession of practical nursing in Manitoba is:
The Licensed Practical Nurses Act
The LPN Act establishes practical nursing as a regulated profession, establishes the CLPNM and its authority, establishes criteria for registration, and sets out the scope of practice of the profession, among other things.
The LPN Act also describes the additional rules that can be made in regulations and in by-laws.
The Licensed Practical Nurses Regulation
Regulations are a form of subordinate legislation established by the executive branch of the Government.2 They set out detailed requirements to complement the enabling Act. The LPN Regulation expands on the requirements for education, registration and renewal set out in the LPN Act.
The By-Laws of the CLPNM
The LPN Act provides the profession with authority to make its own rules on specific topics, referred to as “by-laws.” Most of the CLPNM By-Laws describe how the organization and profession are to be governed; however, some by-laws establish rights and obligations of applicants and members of the profession. As an example, Article 3 of the By-Laws requires all CLPNM registrants to keep their contact information and employers up-to-date in their registration profiles.
The Regulated Health Professions Act
The RHPA is umbrella legislation that will eventually govern 22 regulated health professions in Manitoba. The RHPA does not yet apply to LPNs. When it does, it will replace the LPN Act and its Regulation. LPNs may have heard that their RN colleagues will be under the RHPA in 2018. This may create some confusion, and leave some LPNs wondering if the RHPA will apply to their practice at that time as well. It will not.
The Government of Manitoba has not yet stated publicly when the LPN profession will transition to the RHPA. Until it is known when the practical nursing profession will transition to the RHPA, LPNs will continue to be regulated under the LPN Act.
All of the documents referred to in this article are accessible on the CLPNM website. Any person with questions is encouraged to contact the CLPNM by email [email protected] or by phone at 204-663-1212 or 1-877-663-1212 toll free.
You have probably noticed that the CLPNM frequently quotes or refers to the LPN Act and the LPN Regulation in the documents we develop to guide the LPN profession.
We do that because our authority and our obligations as a regulator are derived from these two pieces of legislation.
1 For example, The Personal Health Information Act, or any laws that establish a duty to report. For more information, see the CLPNM’s Interpretive
Document on the Duty to Report.
2 See Duhaime’s Law Dictionary entry on Regulations at: http://www.duhaime.org/LegalDictionary/R/Regulation.aspx

15Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Acute Care Nurses in All Areas New Oncology Nurses; Palliative Care Nurses; Geriatric Nurses Primary Care, Home & Community Health Nurses; Tele-Health Nurses Nurse Practitioners, Transition, Outpost & Occupational Health Nurses
This workshop provides an update and overview on the pathophysiology of cancer, how it starts, how it spreads, the role of oncogenes, the role of the environment (viruses, hormones, chemicals, etc.) as well as many other facts and tidbits about the growth and differentiation of cells. Nomenclature, grading and staging of tumors will be explained. Specific cancers to be discussed include breast cancer, prostate cancer, lung cancer, skin cancer, hematologic malignancies, brain tumors and GI cancers.
arb Bancroft is a widely acclaimed nursing teacher who has taught courses on Advanced BPathophysiology, Pharmacology, and Physical Assessment to both graduate and undergraduate students. Also certified as a Pediatric Nurse Practitioner, she has held faculty positions at the University of Virginia, the University of Arkansas, Loyola University of Chicago, and St. Xavier University of Chicago. Barb is known for her extensive knowledge of pathophysiology and as one of the most dynamic nursing speakers in North America today. Delivering her material with equal parts of evidence based practise, practical application, and humour, she has taught numerous seminars on clinical and health maintenance topics to healthcare professionals, including the Association for Practitioners for Infection Control, The Emergency Nurses' Association, the American Academy of Nurse Practitioners, and more.
WHO SHOULD ATTEND?
Oncology UpdateWhat Every Nurse Needs to Know About Cancer
WINNIPEG, March 12, 2018 • Canad Inn Polo Park0830 to 1600 hrs.
BARB BANCROFT, RN, MSN, PNP
The Big C - From the Beginning The Definition of Cancer Embryology – Differentiation and Maturation of Cell Lines The Role of Oncogenes in the Loss of Control of Maturation and Differentiation The Role of Angiogenesis in the Development of a Malignant Tumour The Role of Growth Factors and Hormones in Oncogenesis The Role of Chronic Inflammation
Benign & Malignant Tumours - Nomenclature & Characteristics Understanding the Nomenclature Characteristics of Benign and Malignant Tumours Understanding the Grading and Staging of Tumours Understanding Tumour Markers: CA-125, HER2, BRCA, ALK, CD20, CEA, PD-L1 What is “Triple Negative” Breast Cancer?
Environmental Causes of the Loss of Control of Maturation and Differentiation Viruses, Bacteria Radiation Obesity; Hormonal Triggers Age; Genetics Smoking
Treatment & Prevention of Cancers The “Old” Standbys The Newer “Targeted” Therapies - Monoclonal Therapies, Checkpoint Inhibitors, PARP
Inhibitors, Tyrosine Kinase Inhibitors Old Drugs with New Indications - Thalidomide, Aspirin Hormonal Therapies
Notes on Specific Cancers - What's New, What's Old, What's inthe Future Breast Cancer, Colorectal Cancer, Lung Cancer, Prostate Cancer Malignant Melanoma
00 $159. + $7.95 GST = $166.95 Super Early Rate (on or before Jan. 8, 2018)
00 $169. + $8.45 GST = $177.45 Early Rate (on or before February 5, 2018)00 $179. + $8.95 GST = $187.95 Middle Rate (on or before March 5, 2018)00
$189. + $9.45 GST = $198.45 Regular Rate (after March 5, 2018)
Obstetrical Nurses; L&D, Midwives, Ante and Postpartum; Fetal Assessment Nurses, Lactation Consultants
Neonatal Nurses: Level 1, 2, & 3 Nursery Staff; Neonatal Nurse Practitioners Childbirth, Obstetrical and Neonatal Educators; Managers Women's Health Practitioners; Intimate Partner Violence Counsellors; Selected
Gyne & Public Health Nurses Social Workers, Drug Addiction Counsellors, Sexual Health Counsellors
It is estimated that up to twenty percent of all newborns are exposed prenatally to alcohol, illicit drugs, and prescription opiates. Identifying the mother and her newborn are the first steps required for individualized treatment for the specific drugs. Neonates are extremely sensitive to the environment which must be altered by creative nursing interventions. Nurses can potentially have greatest impact, since women are most likely to be receptive to treatment while pregnant or immediately postpartum. Participants will leave equipped to assess mothers and their newborns and intervene with individualized care.
aureen Shogan is a Neonatal Clinical Nurse Specialist in an NICU and Mother-Baby MUnit at Deaconess Hospital in Spokane, Washington, and Neonatal Nurse Consultant to 23 community hospitals. A graduate of Sacred Heart Nursing School, Gonzaga and Washington State Universities, she has experience as an NICU manager, transport nurse, clinical educator and parenting educator. Maureen has served on the editorial boards of Neonatal Network, Mother Baby Journal, and JOGNN, and has taught at national and regional workshops for NANN, AWHONN and others. Maureen has worked with chemically addicted pregnant and parenting moms for over 20 years and is a consultant to the Washington and Idaho Departments of Child Welfare and Social Services.
WHO SHOULD ATTEND?
Drug Use in PregnancyWINNIPEG, April 23, 2018 • Canad Inn Polo Park
0830 to 1600 hrs. MAUREEN SHOGAN, MN, RNC
Identification, Treatment, & Outcomes for Mom & Babe
The World of Drug Use: Crack, Crank, Oxys, Weed, Speed, & Ecstasy Manufacture & use of Methamphetamine, Cocaine, Opiates, Marijuana, & Ecstasy The Difference Between Crack and Crank Snorting, Smoking, Shooting, Injecting, Bumper Boosting, & Welders’ Oxygen Speed Balling, Ice, Crystal, Rollin’, & Special K Spice & Bath Salts: Dangerous Drugs Hide Within
Identifying Physiologic Symptoms of Maternal Use Major Clues that a Mom is using: What are the Signs? Physical Complications of Use: Abscesses, Tooth Loss, Meth Mite Zits Possible Maternal Physiologic Effects of Meth, Cocaine, Marijuana, Oxys & Hydros Complications: Changes in Fetal Heart Rate and Uterine Responses to Vasoconstrictors When Labour Drugs Given by the Nurse Interact with Other Drugs in the Mom's System Pain Control for the Mom Using Oxys & Hydros or Methadone Buprenorphine (The New Methadone)
Maternal Lifestyle and Behavioural Red Flags Dispelling the Myths of what a Drug User “Looks Like” Maternal Issues of Intimate Partner Violence, Isolation, Illegal Activities, and Infections What in the Maternal History may Lead you to Suspect Drug Use? Deciphering Mysteries of Maternal Behaviours while High on Uppers or Downers Co-occuring Mental Illnesses
Neonatal Symptoms and Care of the Prenatally Exposed Newborn Differentiate Neonatal Symptoms of Uppers versus Downers Exposure Neonatal Abstinence Scoring (NAS). When do we Start and how Often do we Assess? What is the Difference between Neonatal Drug Withdrawal and “Drug Affected”? Special Nursing & Environmental Care Interventions for the Neonate Considerations when the Mom wants to Breast Feed
Potential Outcomes of the Infant Exposed Prenatally to Drugs Who experiences “Dopamine Depletion Syndrome”? Potential Outcomes of Prenatal Marijuana & Meth Exposure at 4 to 9 Years of Age Where does Prematurity fit into the Drug Exposure Puzzle?
Quarrying in the Quagmire of Maternal Drug Use Assessment Which Questions will elicit Factual Maternal History of Drug Use? Why do some Patients tell some Nurses Everything & Other Nurses Nothing? Using the 4 Ps: Use in Pregnancy, Partner, Parents, & Prior to Pregnancy Staying Non-Judgemental in Difficult Situations
00 $159. + $7.95 GST = $166.95 Super Early Rate (on or before Jan. 29, 2018)00 $169. + $8.45 GST = $177.45 Early Rate (on or before March 12, 2018)00 $179. + $8.95 GST = $187.95 Middle Rate (on or before April 9, 2018)00 $189. + $9.45 GST = $198.45 Regular Rate (after April 9, 2018)
16Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
NURSING ABROAD ENRICHED MY NURSING PRACTICE IN MANITOBA
In 2017, Janou Dufresne, a Manitoba-based licensed practical nurse (LPN) was given the opportunity to
participate in the nursing journey of a lifetime. While volunteering as a nurse overseas, she was exposed to
different models and methods of patient care, established lasting relationships with care providers from around
the world, and gained experiences and perspectives that will inform her nursing practice for years to come.
Janou Dufresne has been an LPN since November 2015. Upon graduating from the Diploma in Practical Nursing program at Université de Saint-Boniface, she took a position on a medical unit in a rural hospital. However, Janou could not help but remember of a program called International Volunteer HQ (IVHQ), which she learned about in nursing school. She had always wanted to travel, and this program could provide her with the opportunity to continue to develop her nursing knowledge and skills and travel the world at the same time.
In August 2016, Janou applied for and was accepted into the IVHQ program. From over 35 destinations to choose from, she chose to volunteer in Vietnam. Even though IVHQ offered programs in many other countries like Uganda, Africa and Peru, Janou decided that Vietnam was the best match for her because she would be provided with an opportunity to work in a hospital setting, which she believed would enable her to learn more. In January of 2017, Janou left for her three-month trip of a lifetime to Vietnam. While a typical rotation with IVHQ lasted only two weeks with one facility, she planned to volunteer
Volunteers with the IVHQ program: Quynh Sumo RN BN (Vietnam), Janou Dufresne LPN (Canada), Janine Parel RN BN (Australia), and Khanh Hoang Volunteer Coordinator for Medical Group (Vietnam).
17Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
for three months. This would give her the opportunity to try many different areas of nursing in the facility.
When Janou arrived in Vietnam, she settled into the shared accommodations that IVHQ had arranged for her. She lived with other volunteers from the program who, like her, had traveled to Vietnam from other countries. Other volunteers came from Australia, New Zealand, France, Europe, South America and the USA, and they all came with a variety of skill sets. Volunteers consisted of nurses, nursing students, lab technicians, physiotherapists, speech therapists, and medical doctors. Janou states that she valued the opportunity to meet these other health care professionals, which gave her the chance to build new relationships, learn about different cultures and learn about health care all over the world.
At the hospital where Janou was assigned, all volunteer healthcare professionals worked rotations. The rotations were scheduled dependent upon their skill sets. For example, first-year nurses would often work with rehabilitation patients, assisting them with their activities of daily living, transfers or established rehabilitation programs. They would also work with pediatric patients and patients who had been admitted with genetic conditions. Nursing students provided assistance with activities of daily living and exercise, which were outlined in the patients’ rehabilitation program.
A typical day for Janou began at 0800 when she arrived at the hospital. She
would begin her shift by completing a medication pass, which typically took 1 ½ to 2 hours. Afterwards, the nurses would proceed to the nursing station to complete their charting. Volunteers were not allowed to see the charts, so they assisted with other tasks until lunch. During the one hour lunch break, Janou and her roommates would make the long trek back home, quickly eat, and then make the trip back to the hospital for the afternoon.
Janou had the opportunity to spend a great deal of time volunteering in the head trauma ward, where she assisted in preparing and administering IV and IM medications. She was thankful for the two days per week she spent in that role. As a result, she feels that she has become an expert at landmarking sites. Janou also assisted in the operating room (OR) during orthopedic surgeries. Volunteers like Janou, with education as a healthcare professional, could assist in the OR; however, this involved simple tasks such as assisting with holding a limb in place throughout a procedure. When not on the head trauma ward or in the OR, Janou also carried out wound care.
Throughout her time volunteering with the IVHQ program, Janou noted several differences in the health care environment and culture of the facility compared to the Manitoba-based facility where she had previously worked. For example, she recalls that the facility was primarily exposed to the elements. The nursing station and all hallways were outdoors. She also noted that,
as a result of scarce resources, supplies that are often taken for granted in Canadian facilities, such as gloves, were treated as valuable commodities. Janou also noticed differences in health care culture. For example, while nurses in Canada are expected and encouraged to ask questions, questions were not encouraged in the facility where she volunteered. Despite the many differences, Janou found that many of the processes and principles of nursing utilized in Vietnam were similar to those she had learned in Canada.
While caring for her patients, Janou saw that family played a large role in the patient’s care and recovery. Patients in the facility were never alone. They always had family members with them, and family members were active participants in their care. Observing the positive impacts of families’ involvement, Janou began to view her holistic care of patients differently upon returning to nursing practice in Manitoba. She states that she now has a conscious habit of involving her clients’ families in the care of their loved one as much as possible.
Not only did Janou have an amazing experience and make some lifelong friends, she also learned useful techniques and processes that she could apply in her everyday nursing practice back in Canada. She feels more confident than ever in her nursing practice, and she hopes to again one day receive the opportunity to travel abroad with IVHQ.

18Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Nurses in Acute Care, Critical Care, and Long Term Care Settings Nurses in Home Care and Rehabilitation Settings Wound Care and Infection Control Nurses Adult Nurse Practitioners and Diabetes Educators
Leg ulceration is a chronic health issue posing significant burden on individual patients and the health care system. This workshop will describe the clinical approach to diagnose and differentiate various types of ulcers in the lower extremity due to venous insufficiency, lymphedema, arterial compromise, malignancy, inflammatory diseases, infection, and other systemic conditions. Participants will develop an understanding of the mechanisms and rationale behind the appropriate use of compression therapy for the treatment of chronic edema and lower extremity ulcers. Discussion will also focus on holistic care including the needs to optimize medical treatment and lifestyle modifications. Participant will develop a pragmatic local wound care approach that is based on best practice evidence.
r. Kevin Woo is an Assistant Professor at Queen's University, School of Nursing in Kingston, DCanada. Kevin is an adjunct research professor at the Western University teaching for their Masters of Clinical Science in Wound Healing program. He is the Early Researcher Award recipient 2014-2019 from the Ministry of Research and Innovation. He is the co-editor of Chronic Wound Care 5, a clinical source book for health care professionals. He served on expert panels to develop Best Practice Guidelines (BPG) in collaboration with Registered Nurses Association in Ontario for the Assessment and Management of Stage 1 to 4 Pressure Ulcers and Screening for Dementia, Delirium and Depression in older persons. Kevin maintains his clinical expertise and functions as an Advanced Wound Consultant at the West Park Health Center, a specialized chronic care and rehabilitation hospital in Toronto. Additionally, he is the Web Editor for Advances in Skin and Wound Care journal web site and he is a member of several editorial boards.
WHO SHOULD ATTEND?
WINNIPEG, May 7, 2018 • Canad Inn Polo Park0830 to 1600 hrs. Dr. KEVIN WOO, Ph.D, RN, FAPWCA
Leg Ulcers Assessment &
Management
Overview of Wound Healing Physiology Phases of Wound Healing Review of Arterial System; Venous System; Lymphatic System What Makes Chronic Wounds Chronic?
Wound Healing Wound Bed Preparation; Debridement Infection Management; Importance of Moisture Balance
Vascular Evaluation Differential Diagnosis; Medical History & Risk Factors; Physical
Examination Invasive and Non-Invasive Arterial Studies: Think ABPI Studies of Venous Insufficiency
Management of Arterial & Venous Leg Ulcers Medical Therapies & Surgical Interventions Approach to Non-Healable Arterial Leg Wounds For Venous Leg Ulcers: Compression Therapies: Elastic or Inelastic? How to Apply Compression to Venous Leg Ulcers; Dos, Don’ts, and Secrets
Management of Mixed Venous Arterial Disease The Evidence and the Controversy
Management of Lymphedema Medical & Surgical Therapies What Can be Done to Promote Lymphatic Drainage?
Atypical leg ulcers Inflammatory Diseases; Proliferative Diseases Lipidema
00 $159. + $7.95 GST = $166.95 Super Early Rate (on or before Feb. 12, 2018)
00 $169. + $8.45 GST = $177.45 Early Rate (on or before March 26, 2018)
00 $179. + $8.95 GST = $187.95 Middle Rate (on or before April 23, 2018)
00 $189. + $9.45 GST = $198.45 Regular Rate (after April 23, 2018)
WHO SHOULD ATTEND? RNs, NPs, RPNs, & LPNs in All Areas Acute & Critical Care, Special Care Areas Geriatric, Home, Community, and Primary Care Outpost Nurses, Occupational Health Nurses; Transition Coordinators Nurse Practitioners, Tele-Health Nurses, Educators, Managers
9000 Drugs, Where to Start? Differentiate Quickly Among the Classes of Drugs with the “Suffix” of Each Class The “statins”, the “prils” the “triptans” and the “sartans” The “prazoles” and the “afils” The “olols”, the “alols”, the “ilols” and the “dipenes” The “coxibs” the “mabs”, and the “glitizones” The “conazoles”, the “cyclovirs” and more
Clinical Uses and Mechanism of Action: The Key Things You Need to Know Analgesics; Drugs for Diabetes; Targeted Therapies Cholesterol-Lowering Agents, Anti-Hypertensives Anti-Fungal and Anti-Viral Agents
Understanding the Common Treatment Regimens for Selected Clinical Conditions Hypertension; Chronic Heart Failure Diabetes Mellitus Type 2 Depression
You're Taking WHAT??? Clinical Interactions Between Drugs, Alternative Therapies and Food The Effect of Grapefruit Juice on the Metabolism of Certain Drugs Foods with Potassium; Foods with Vitamin K St John's Wort
Specific Mechanisms of Actions of Drugs in Popular Use The “Highway System” and the “prils” The Nocturnal Liver and the “statins” The Proton Pump and the “prazoles”
The Buzz on Medical Cannabis - What the Evidence Says Indications; Contraindications Methods & Issues with Use
There are a staggering number of drugs that nurses are expected to keep current with. Without some systematic way of categorizing the information, it's easy to become overwhelmed by such a vast amount of information. This course is aimed at simplifying the volume of drug information into easier recall and to crystallize the key things you need to know about the major categories of drugs. And as always, a day with Barb Bancroft will include humour along with important clinical applications that will help you remember and apply the material on a daily basis in your clinical setting.
arb Bancroft is a widely acclaimed nursing teacher who has taught courses on Advanced BPathophysiology, Pharmacology, and Physical Assessment to both graduate and undergraduate students. Also certified as a Pediatric Nurse Practitioner, she has held faculty positions at the University of Virginia, the University of Arkansas, Loyola University of Chicago, and St. Xavier University of Chicago. Barb is known for her extensive knowledge of pathophysiology and as one of the most dynamic nursing speakers in North America today. Delivering her material with equal parts of evidence based practise, practical application, and humour, she has taught numerous seminars on clinical and health maintenance topics to healthcare professionals, including the Association for Practitioners for Infection Control, The Emergency Nurses' Association, the American Academy of Nurse Practitioners, and more.
Pharmacology Update for Nurses
BARB BANCROFT, RN, MSN, PNP
Simplify, Don’t Mystify...
WINNIPEG, June 4, 2018 • Canad Inn Polo Park0830 to 1600 hrs.
00 $159. + $7.95 GST = $166.95 Super Early Rate (on or before Feb. 26, 2018)00 $169. + $8.45 GST = $177.45 Early Rate (on or before April 16, 2018)00
$179. + $8.95 GST = $187.95 Middle Rate (on or before May 22, 2018)00 $189. + $9.45 GST = $198.45 Regular Rate (after May 22, 2018)

19Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
CANNABIS: TRUE OR FALSE
With legal access to
cannabis for medical
purposes and the
Federal Government’s
announcement that it will
legalize the recreational use
of cannabis by July 2018,
some licensed practical
nurses may question how
this applies to them and
their nursing practice.
Once cannabis is legal, licensed practical nurses can assume it is safe and appropriate to use before or during a nursing shift. True or false?
False. The potential legalization of cannabis does not mean that it is safe and appropriate to consume in all environments and for all purposes. Most nurses will recognize the parallels of cannabis use with alcohol consumption. The fact that alcohol consumption is legal for those over the age of 18 does not mean that it is safe or appropriate for a nurse to be under the influence of alcohol during a nursing shift. The same is true, and will continue to be true, for impairment resulting from the use of any drug, including cannabis, while providing nursing care.
The College of Licensed Practical Nurses of Manitoba (CLPNM) cannot inquire about, nor have any influence over, a licensed practical nurse’s ability to use medically-authorized cannabis before or during a nursing shift. True or false?
False. The CLPNM will continue its current practices related to fitness to practice. The CLPNM will not interfere in a medically-authorized course of treatment; however, in keeping with its legislated duty to govern the profession in the best interest of the public, the CLPNM must assess whether a licensed practical nurse can continue to practise safely, competently and ethically while using cannabis. If the CLPNM determines that client safety cannot be assured, and if reasonable
accommodations cannot be put in place, the CLPNM may place conditions and/or restrictions on the nurse’s practice until the nurse’s course of treatment is complete.
Cannabis does not cause impairment. True or false?
False. Although its effects may vary from individual to individual, and from product to product, Health Canada’s guidance on cannabis for health care professionals identifies that cannabis can contribute to impaired cognition and psychomotor functioning, and in some users it can have psychiatric effects.
The CLPNM has concerns that changes to cannabis laws will result in more practice concerns and complaints. True or false?
False. The CLPNM has confidence that the upcoming legalization of cannabis for recreational purposes will not significantly contribute to conduct and practice issues, because it recognizes that licensed practical nurses are professionals who understand the importance of safe practice and appropriate behaviour.
Any practical nurse who may have additional questions about their responsibilities when using medically-authorized cannabis, or legalized recreational cannabis in the future, are encouraged to review the CLPNM’s Practice Direction on Fitness to Practice. This document can be accessed on the CLPNM’s website, or you can contact the CLPNM’s Practice Department at 204-663-1212 or 1-877-663-1212 for further information.
1 Health Canada (2013). Information for Health Care Professionals: Cannabis (marihuana, marijuana) and the cannabinoids. Retrieved online at: https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-use-marijuana/information-medical-practitioners/information-health-care-professionals-cannabis-marihuana-marijuana-cannabinoids.html#chp771

20Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
RESULTS OF THE 2017 SUITABILITY CHECK PILOT PROGRAM
Historically, applicants to
the College of Licensed
Practical Nurses of Manitoba
(CLPNM) were only required
to provide suitability checks1
during the application
process and at the time of
initial registration. After
this initial submission,
registrants were only
required to answer a series
of self-disclosure questions
annually when renewing
their annual registration.
In preparation for the transition under The Regulated Health Professions Act, which has more stringent legislative requirements, the CLPNM implemented a process of confirming that registrants of the practical nursing profession do not have a history of conduct that places the public at risk. Likewise, this confirmation process adds to public protection and confidence in the profession overall. It is also consistent with requirements implemented by other regulators in Manitoba and with existing legislative requirements. In order to prepare for this incoming legislation, the CLPNM implemented a pilot program in 2017, in which approximately 10% of its registrants were selected to participate.
The CLPNM randomly selected 300 registrants to participate, and registrants were notified in January 2017. This correspondence also informed these registrants that failing to supply the three suitability checks by August 15, 2017, would negatively impact their ability to renew their registration for 2018. Furthermore, registrants were informed that if any positive or adverse information was discovered on any of the suitability checks, the CLPNM would be required to conduct a registration risk assessment, in which the registrant would incur additional fees and possible delays in processing their renewal application. Lastly, registrants were informed that a possible outcome of a registration risk assessment could include a referral to the CLPNM’s Investigation Committee and/or Board of Directors for professional misconduct.
Of the 300 registrants selected for this process, 24 registrants missed the August 15, 2017 deadline and were therefore considered ineligible for renewal. Additionally, seven registrants resigned their registration effective November 30, 2017, so their names were removed from the pilot program. Out of the remaining 269 registrants, it was confirmed that three registrants had criminal offences that had not been previously disclosed to the CLPNM; therefore, the CLPNM conducted individual registration risk assessments to determine the extent of the risk to the public.
As this process supports the CLPNM’s mandate to regulate the profession in the best interest of the public, and holds registrants accountable for their conduct, the CLPNM will be implementing this requirement on a grander scale in the upcoming year. This means that all registrants will be required to provide up-to-date suitability checks approximately once every five years as an ongoing requirement for CLPNM active practicing registration. Registrants will be notified in advance if they are required to submit suitability checks as part of their registration renewal application.
Questions or concerns?
Please review the CLPNM’s Periodic Criminal Record and Abuse Registry Fact Sheet for more information on this topic; alternatively, you can contact us at [email protected], or by phone at 204-663-1212 or 1-877-663-1212 toll free.
1 The term suitability check refers to the following documents: a Canadian criminal record check with vulnerable sector search, a
Manitoba-issued adult abuse registry check, and a Manitoba-issued child abuse registry check.

21Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
ASK A PRACTICE CONSULTANT: NURSING LEADERSHIP PRACTICE
• demonstrating openness to new ideas, which may change, enhance or support nursing practice;
• presenting a positive image of nursing;
• acting as a role model, resource and mentor to clients, learners, nursing peers and colleagues;
• promoting and supporting practical nursing and other health team members to practise to their full scope of practice;
• advocating for changes to policies and protocols, which impede the profession from meeting client needs and the professions standards;
• contributing to the development of policies and procedures for the delivery of competent safe nursing care;
• promoting practice environments, which support the nurses’ mental, physical and emotional well-being;
• advocating for clients, professional practice environments and the nursing profession, and
“I’ve just had my annual performance appraisal at my place of employment. My manager states that I need to improve my nursing leadership practice. What does that mean exactly?”
Nurses sometimes believe that their skill and ability to perform clinical procedures are the primary things that make them appear professional and competent to those receiving care, to their colleagues, and to the public. Mistakenly, many believe that leadership in nursing is reserved for only those in formal leadership positions, but effective leadership must be incorporated into every nurse’s practice, no matter their position or area(s) of practice.
The health care system requires strong, consistent and knowledgeable nurse leaders from numerous nursing positions and from various nursing environments. Nurse leaders must be visible, inspire others, support professional nursing practice, and contribute to quality professional practice environments. In order to be able to provide quality nursing care, the integration of leadership is an essential component to a nurse’s practice.
The College of Licensed Practical Nurses of Manitoba’s (CLPNM) eighth practice standard, Professional Leadership, states:
The Licensed Practical Nurse (LPN) demonstrates professional leadership in the delivery of quality nursing and health care services to the public.
The LPN achieves this by:
• promoting and participating in the continuing development of the discipline of practical nursing;
• promoting efforts to achieve a healthier society.
Why is leadership important?
Leadership is necessary for a variety of reasons in the nursing profession. A nurse’s leadership skills are the first thing clients, families, and colleagues notice, which is why LPNs must incorporate leadership competence in their practice. These skills allow others to gain confidence in a nurse’s abilities, and for the nurse to gain the respect and trust from their clients and team members. LPNs who demonstrate an effective leadership style have an opportunity to assist in the growth of other health care team members, as leading by example is an effective way to positively influence others. This in turn assists in creating a health care team’s effective leadership competence, which contributes to the achievement of client care goals, efficiencies in health care system delivery and to optimal clinical practice.
22Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
What does a nurse leader look like?
Nurse leaders are often described as being visionary, and equipped with strategies and a desire to lead their teams to future goals. They are dynamic, passionate, and have a motivational influence on other people. Being solution-focused and having a genuine desire to inspire others are other characteristics of a nurse leader. Nurse leaders also demonstrate a consistent commitment to honour moral, ethical, spiritual, and artistic values and principles that inspire trust and confidence.
The LPN leader models professional behaviour and is described as a driving force admired by others. Effective nurse leaders are confident while using problem-solving processes independently to maintain group effectiveness.
Leadership in practice
The nurse leader envisions a quality working environment and what is needed in order to achieve one. Leadership within the practice environment requires nurses to feel empowered to take action. When nurses feel empowered, their desire to engage within the environment increases. Even though it is important for nurse leaders to share power with others, otherwise known as empowerment, it is equally crucial that these leaders emit a respectful attitude and an ability to collaborate effectively with all members of the health care team.
Interdisciplinary collaboration, along with interpersonal skills, increases efficiency in health care delivery and brings all members of the health care team together. Interpersonal skills are the life skills we use every day to interact and communicate with other people, both individually and in groups. People with good interpersonal skills are usually perceived as optimistic, calm, confident and charismatic, which are qualities often appealing to others.
People who have worked on developing strong interpersonal skills are known to demonstrate strong leadership competence in both their professional and personal lives.
Some examples of how LPNs can engage in leadership include:
• developing good planning, time management, and organizational skills;
• integrating effective communication strategies that include effective listening skills;
• incorporating professional conflict resolution skills during times of contention;
• joining work-place committees or working groups (i.e. policy reviews, occupational health and safety), and
• developing and applying a positive attitude and emotional intelligence into daily practice.
Emotional intelligence is the ability to identify and manage one’s own emotions and the emotions of others. It includes the ability to:
• accurately perceive emotions;
• access and generate emotions so as to assist thought;
• understand emotions and emotional knowledge, and
• reflectively regulate emotions so as to promote emotional and intellectual growth.
Having emotional intelligence means to have control of one’s own emotions and to have emotional maturity. Studies have shown that the best and most successful leaders have a highly developed level of emotional intelligence. In addition, those who have had emotional intelligence training have more professional longevity than those who have not.
The effects of poor leadership
Nurses with limited leadership skills can be detrimental to organizations as they may diminish staff morale, thwart creativity, and create unnecessary job stress. Combining poor or toxic leadership with the stressful nature of the job itself leads to lackluster work, poor morale, decreased productivity, increased absenteeism, and high turnover. This may lead to poor or compromised client outcomes.
Poor interpersonal skills also negatively impact a nurse’s leadership capacity. Communication that belittles, embarrasses, or blames will lead to the isolation of workers and escalate conflict in the workplace. One of the greatest challenges to address toxic leadership in an organization is simply that it becomes widely tolerated. Apathy often leads to an organizational culture that makes toxic leadership acceptable. This may eventually lead workers to accept the situation of poor leadership as the new norm, which is unacceptable in an environment that is dedicated to the optimal health and wellbeing of the public.
Conclusion
Leadership development must continue throughout a nurse’s career. Continually being open to new ideas and experimenting with new concepts and approaches while frequently exploring educational opportunities will enhance a nurse’s leadership competence. No matter a nurse’s level of expertise, nurses in all domains of practice must maximize their leadership potential. It is then with this collective energy of shared leadership that nurses can form strong networks and relationships that ultimately result in optimal client outcomes and excellence in their nursing practice.
Resources
CLPNM (2004). Standards of Practice.
CLPNM (2014). Code of Ethics.

23Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
PRACTICE DIRECTION: ASSIGNMENT AND DELEGATION TO
UNREGULATED CARE PROVIDERS
This practice direction describes the responsibilities of Manitoba’s practical nurses when assigning and delegating client care tasks to unregulated care providers. This practice direction was created in collaboration with the College of Registered Nurses of Manitoba and the College of Registered Psychiatric Nurses of Manitoba.
Practice directions assist practical nurses in understanding their responsibilities and legal obligations, enabling them to make safe and ethical decisions within their practice. Practical nurses are expected to comply with the information disseminated in practice directions. Failure to do so may result in investigation for misconduct and/or an audit of the nurse’s practice.
Background
Unregulated care providers are formal members of the health care team who are not regulated and who have a scope of employment defined by their employer based on their qualifications and education.
Unregulated care providers are accountable to their employer for their individual actions and decisions. While no legislation formally defines their role, legislation restricts certain activities and roles to regulated professionals. This limits the scope of employment of the unregulated care provider.
Unregulated care providers include, but are not limited to, resident aides, health care aides, service workers in the community, psychiatric assistants, home support workers, and in some settings, office assistants.
Assignment
Nurses1 may assign unregulated care providers client care tasks, within the unregulated care provider’s scope of employment.
When assigning tasks, the nurse is required to:
• Use the nursing process to determine a plan of care and/or collaborate with other regulated professionals to determine a plan of care before assigning the task.
• Understand the scope of employment of the unregulated care provider and assign only tasks that fall within their position description and employer policies.
• Provide guidance and collaborate with the unregulated care provider.
• Collaborate with the health care team to determine an appropriate plan for
re-assessment, monitoring and evaluation of the plan of care based on an assessment of risk associated with the client, task, environment and unregulated care provider (see Appendix A).
• Intervene when unsafe or unethical practice is identified. Interventions may include guidance, teaching and direction, clarification of the plan of care and, if necessary, reporting to the appropriate authority.
Delegation
There are circumstances where it is necessary to delegate tasks to unregulated care providers in order to provide access to care.
Delegation is the extension of authority by a nurse or other regulated professional to an unregulated care provider who does not have the authority to perform the task as an assignment through their scope of employment.
Delegation is always client-specific and the task cannot be further delegated or transferred to another client.
1 In this document, the use of the word nurse refers to Licensed Practical Nurses (LPNs), Registered Nurses (RNs) and
Registered Psychiatric Nurses (RPNs).
24Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Nurses may delegate tasks outside of the unregulated care provider’s scope of employment as long as the task meets the following conditions:
• The employer supports delegation of the task.
• The task would normally be performed by a client or their family member as part of self-care.
• The task has defined limits and does not require the nursing process.
• The need, response and possible outcomes have been identified and documented for the client.
Making the Decision to Delegate a Task
The nurse is required to:
1. Confirm that the employer supports delegation to an unregulated care provider and follow applicable policies and procedures.
2. Be competent and authorized to perform the task they are delegating.
3. Assess the client and determine that a need exists that cannot be met through assignment of the task to an authorized health-care provider.
4. Assess the competence of the unregulated care provider in relation to the delegated task on the specific client.
5. Identify the risk to the client through an assessment of the client, task, unregulated care provider and environment (see Appendix A).
6. Be satisfied that the decision to delegate is appropriate in the context of the client, task, unregulated care provider and environment.
7. Include information about the decision to delegate and process of delegation when obtaining informed consent from the client for the task.
8. Document the decision to delegate.
Engaging in the Process of Delegation
The nurse is required to:
1. Provide client-specific teaching to the unregulated care provider until the nurse is satisfied that the unregulated care provider is competent to perform the task in the context of the task, client and environment.
2. Ensure that support and consultation is available during the performance of the task.
3. Provide periodic monitoring and evaluation of the unregulated care provider’s competence.
4. Remain responsible for the decision to delegate and the ongoing assessment of the client’s health status and plan of care.
5. Utilize the nursing process to determine appropriate monitoring and evaluation of the plan of care based on assessment of the client, task, environment and unregulated care provider.
6. Terminate the delegation if a change in client status or the unregulated care provider’s competence indicates that the delegation is no longer appropriate or acceptable to the client.
Glossary
Assignment: Allocation of clients or specific client care tasks to health care providers. Occurs within the scope of practice of a regulated professional and within the scope of employment of an unregulated care provider.
Authorized health care provider: May be a regulated professional or an unregulated care provider. Regulated professionals are authorized through legislation and must meet requirements as set by their regulatory college. Unregulated care providers are authorized by their employer through their scope of employment. Scope of employment may only include activities that are not restricted through legislation.
Client-specific: Performed on a specific client. Limits of the task are specific to the individual client and cannot be transferred to another client.
Decision to delegate: Decision made by an individual nurse to extend authority to an unregulated care provider to perform a specific task on a specific client.
Delegation: Extending authority to perform a specific client care task to an unregulated care provider who does not otherwise have the authority to perform the task.
Regulated professional: Professional regulated through legislation who provides or administers health services.
Health care provider: Paid provider of health care services.
Nursing process: Assessment, diagnosis or determination, planning, intervention and evaluation of and managing of the outcomes of care.
Plan of care: Written guideline for client care that documents the client’s health care needs. It includes assessment data, list of problems and therapies as well as expected criteria used to evaluate care.
Process of delegation: Process of extending authority to an unregulated care provider.

25Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Routine activities of living: Activities that would normally be performed by the client or their family member as part of self-care. To assess a task as a routine activity of living, the need, response and outcome of the task must be predictable.
Risk: Potential of harm to the client.
Scope of employment: Range of responsibilities defined by an employer through position descriptions and policies.
Task: One part of client care. Has clearly defined limits.
Teaching: Providing instruction for a task where the goal is to determine that the person receiving instruction is competent to perform the task.
Unregulated care providers: Formal members of the health care team who are not regulated by a regulatory body and who have a scope of employment defined by their employer, based on their qualifications and educational preparation. Unregulated care providers are accountable and responsible to their employers for their individual actions and decisions.
For More Information
Visit our website at www.clpnm.ca for more information and resources.
Contact us with questions at: 463 St. Anne’s Road Winnipeg MB R2M 3C9 Phone: 204-663-1212 Toll Free: 1-877-633-1212 Email: [email protected]
About the CLPNM
The CLPNM is the governing body for the licensed practical nursing profession in Manitoba. Mandated to govern its members in a manner that serves and protects the public interest, the CLPNM establishes practice requirements for the provision of safe and effective nursing care.
References
The following documents were consulted during the development of this practice direction.
Canadian Nurses Association (2005). Unregulated Health Workers: A Canadian and Global Perspective
College and Association of Registered Nurses of Alberta (2014). Assignment of Client Care: Guidelines for Registered Nurses
College of Registered Nurses of British Columbia (2013). Assigning and Delegating to Unregulated Care Providers
College of Registered Nurses of Nova Scotia (2012). Assignment and Delegation Guidelines for Registered Nurses and Licensed Practical Nurses
Khaled,M., Nolan, M., Raijo, T., Shah, N., Prokop, L., Varkey, P., Murad, M. (2014). Creating a Patient-Centered Health Care Delivery System: A Systematic Review of Health Care Quality from the Patient Perspective
National Council of State Boards of Nursing (2016). National Guidelines for Nursing Delegation
Tourangeau, Anne et al. (2015). The Role of Nurses in Assigning, Delegating, Teaching and Supervising Patient Care Activities to Unregulated Care Providers in Home Care: A Jurisdictional Scan of Legislation, Regulation and Policy in Canada
World Health Organization (2008). Task Shifting: Rational Redistribution of Tasks Among Health Workforce Teams

26Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Appendix A
Factors to Consider when Assessing Risk to the Client
Lower Risk
Client
• Health status is well-defined and their condition is not expected to change negatively.
• Willing and able to direct care.
Task
• Has been established as routine and is performed as part of daily care.
• Is not expected to endanger the client’s health or well-being when performed properly.
• Involves few steps and minimal technical psychomotor skill.
• Has predictable outcomes.
• Not altered in different settings.
Unregulated Care Provider
• Has previous experience performing the task.
• Has relevant foundational education.
Environment
• Receives frequent ongoing assessment and care planning by a regulated professional.
• Allows for adequate time for training, evaluation and ongoing maintenance of competence.
• Contains clearly written procedures and policies.
• Enables supervision and supports that allow monitoring of the unregulated care provider as well as opportunity for the unregulated care provider to consult as necessary.
Higher Risk
Client
• Health status is not well-defined and/ or changes or atypical responses may be anticipated.
• Has multiple health care needs.
• Unwilling or unable to direct care.
Task
• Is not routine and may vary in need.
• May endanger the client’s health, mental health or overall well-being.
• Involves numerous steps and a high degree of technical/psychomotor skill.
• Has risk of unpredictable outcomes.
• Requires high degree of technical/psychomotor skill.
• May require altering in different settings.
Unregulated Care Provider
• Has never performed the delegated task.
• Has no related foundational education/ competencies.
Environment
• Has limited or unavailable ongoing assessment, care planning and evaluation by a regulated health care provider.
• Has a limited amount or type of training provided.
• Does not contain written policies and procedures or has inadequate written policies and procedures.
• Does not allow for adequate supervision and support.
Adapted from: College of Registered Nurses of British Columbia (2013). Assigning and Delegating to Unregulated Care Providers.

27Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
PRACTICE DIRECTION: FITNESS TO PRACTICE
Practice directions assist Manitoba’s practical nurses to understand their professional responsibilities
and legal obligations, enabling them to make safe and ethical decisions within their practice. All CLPNM
registrants are expected to practice in accordance with the information disseminated in practice
directions. Failure to do so may result in an investigation for misconduct and/or a practice audit.
Fitness to Practice
Manitoba’s practical nurses (referred to simply as “nurses” in this document) have a responsibility to adhere to their professional standards, articulated in the Standards of Practice and Code of Ethics of their profession. These standards include:
• demonstrating the knowledge, skill and judgment relevant to their practice
• identifying, responding to, and reporting situations of unsafe practice
• displaying the characteristics and attributes of a professional
• maintaining personal well-being, and
• accepting accountability and taking responsibility for their professional conduct and decisions.
In order to meet these standards and to provide safe, competent and ethical care, nurses are expected to take responsibility and to accept accountability for their fitness to practice.
Nursing roles differ, and a nurse’s fitness to practice will be dependent on the nurse’s specific duties, the environment in which the nurse is practicing, and
the population for whom the nurse is providing care. The CLPNM interprets fitness to practice as having the physical, mental and psychological capacity to consistently meet the demands of the nurse’s position and to care for clients safely, competently and ethically.
Fitness for nursing practice includes but is not limited to having the consistent ability to: meet the physical demands of the position, think critically, perform complex calculations, make appropriate judgments, sustain focus and concentration, communicate effectively, and learn and recall complex concepts and skills appropriate to the practice area. A nurse whose capacity to perform these functions is impaired may not be fit to practice.
The Nurse’s Role
As a nurse, you are expected to engage in reflective self-assessment and to take responsibility for ensuring that you are fit to practice before doing so.
This responsibility includes, but is not limited to:
• taking reasonable and timely action to address risks to your personal well-being if those risks might also contribute to a marked departure in your capacity for safe, competent and ethical practice
• reporting to your employer when your fitness to practice is limited by a short-term but acute condition (e.g. illness or injury), so that your employer can arrange for accommodations and/or alternative staffing
• reporting to both your employer and to the CLPNM if
• you have an ongoing condition, disorder or addiction, or
• you are on a treatment plan, such as a medication regimen,
that has the potential to result in a marked departure from the capacity for safe, competent and ethical practice
• not working while impaired by the use drugs or alcohol, and
• reporting situations of unsafe practice to appropriate authorities, which includes reporting when you believe that another health care provider is, or has been,
• impaired at work by the use of drugs or alcohol, or
• suffers from a condition, disorder, or addiction of a nature or to an extent that the member is not fit to practice.1
1 See also the CLPNM’s Interpretive Document on the Duty to Report at http://clpnm.ca/wp-content/uploads/Duty-to-Report.pdf

28Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Note that if you have an ongoing condition, disorder or addiction that impairs, or is likely to impair, your fitness to practice, the duty to self-disclose the matter to the CLPNM applies even if you are on an extended leave of absence from your employment. This provides the CLPNM the opportunity to carry out an assessment of your fitness to practice before you return to work.
It is also important for nurses to be aware that the consumption of drugs and alcohol will not be accepted as a valid reason for falling below the accepted standard of practice, even if the drug is legal and taken pursuant to a prescribed medication regimen. Nurses are knowledgeable about pharmacology, and therefore, are aware that many medications can contribute to impaired cognition and functioning. Examples include but are not limited to cannabis, opioids and benzodiazepines. If you are on a medication regimen that has the potential to cause a marked departure in your capacity for safe, competent and ethical practice, the CLPNM will not seek to interfere with your treatment; however, in keeping with its duty of public protection, the CLPNM must assess whether it is safe for you to continue to practice without accommodations or restrictions during the course of your treatment.
If you are unsure if your health condition, disorder, addiction, or medication regimen poses a risk to your clients, contact the CLPNM before returning to work.
The CLPNM’s Role
The CLPNM is mandated, in legislation, to regulate the profession of practical nursing in a manner that serves and protects the public interest. This duty includes protecting the public from unsafe and incompetent practice.
Practical nursing is a safety-sensitive profession. Therefore, if a concern regarding your fitness to practice arises, the CLPNM must conduct a fitness to practice assessment to determine whether any action is necessary to
protect the public from a risk of harm. In order to conduct the assessment, the CLPNM may direct you to provide documentation, including reports from health care providers, employers, and others.
Each circumstance is different. Having a health condition or disorder does not mean that you will be deemed unfit to practice. A health condition that is appropriately managed may pose no risk to the public at all. Even if your capacity for practice is diminished and the CLPNM identifies that there is some risk to the public, you may still be able to practice safely with appropriate accommodations and/or restrictions on your practice that mitigate the risk.
Making a self-disclosure about your fitness to practice allows the CLPNM to gather the information necessary to determine the presence and extent of the risk, and work with you and your employer to identify appropriate options. Proactively reporting your condition to the CLPNM also demonstrates insight, good judgment, professionalism, and a desire to protect your clients from harm.
In some circumstances, a fitness to practice concern may also be associated with, or may lead to, a concern about your professional conduct. Examples include:
• failing to identify and mitigate a risk to your clients resulting from a marked departure in your capacity for safe, competent and ethical practice, even if it is temporary
• failing to proactively self- disclose to the CLPNM an ongoing health condition, disorder, addiction, or treatment plan, that a reasonable and prudent nurse would expect to impair your capacity for safe, competent and ethical practice
• being untruthful when responding to any question about your fitness to practice posed by the CLPNM, for example, at the time of initial, renewal or reinstatement of registration
• working while impaired by the use of drugs or alcohol,
• any fitness to practice concern that contributes to professional misconduct (e.g. when a substance use disorder is associated with one or more acts of drug diversion).
If a fitness to practice concern is associated with a concern about your professional conduct, the matter may be referred to the CLPNM’s Investigation Committee.
However, when a nurse is forthright, takes appropriate action, and proactively discloses the matter to the CLPNM, the nurse and the CLPNM will work together to identify the solutions that best serve and protect the interests of Manitobans.
Conclusion
By promoting, maintaining and taking responsibility for your fitness to practice, you can help to ensure your clients receive safe and appropriate care, while also helping to maintain trust and confidence in your profession.
For More Information
Contact us with questions at 463 St. Anne’s Road Winnipeg MB R2M 3C9 Phone: 204-663-1212 Toll Free: 1-877-633-1212 Email: [email protected]
About the CLPNM
The CLPNM is the governing body for licensed practical nurses (LPNs), graduate practical nurses (GPNs) and student practical nurses (SPNs) in Manitoba. Its duty is to govern its registrants in a manner that serves and protects the public interest. The CLPNM establishes professional standards for the provision of safe and effective nursing care.

29Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
References
The following documents were consulted during the development of this practice direction.
Canadian Council of Practical Nurse Regulators (2013). Becoming a Licensed Practical Nurse in Canada: Requisite Skills and Abilities. Retrieved from: http://www.ccpnr.ca/wp-content/uploads/2013/09/IJLPN-RSA-Final.pdf
Canadian Human Rights Commission (2017). Impaired at Work: a guide to accommodating substance dependence - Frequently Asked Questions [webpage content]. Retrieved from: http://www.chrc-ccdp.gc.ca/eng/content/impaired-work-guide-accommodating-substance-dependence-frequently-asked-questions
CLPNM (2003). Standards of Practice.
CLPNM (2014). Code of Ethics.
CLPNM (2016). Regulatory Bulletin: Duty to Report.
College and Association of Registered Nurses of Alberta (n.d.). Fitness to Practise [webpage content]. Retrieved from: http://www.nurses.ab.ca/content/carna/home/maintain-my-registration/requirements/fitness-to-practice.html/
College of Licensed Practical Nurses of Alberta (2015). Fitness to Practice and Incapacity: Interpretive Document. Retrieved from: http://www.nurses.ab.ca/content/carna/home/maintain-my-registration/requirements/fitness-to-practice.html/
College of Licensed Practical Nurses of Nova Scotia (n.d.). Fitness to Practice and Incapacity: Guidelines for LPNs and Others. Retrieved from: http://clpnns.ca/wp-content/uploads/2015/09/Fitness-to-Practice-and-Incapacity-FINAL.pdf
College of Nurses of Ontario. (2009). Incapacity: A process guide. Retrieved from: http://www.cno.org/Global/docs/ih/42008_fsIncapacity.pdf
College of Nurses of Ontario (2012). Nursing and fatigue. Retrieved online at: http://www.cno.org/en/learn-about-standards-guidelines/educational-tools/ask-practice/nursing-and-fatigue/
College of Registered Nurses of British Columbia. (2008). Fitness to Practice: The challenge of maintaining physical, mental and emotional health. Retrieved from: https://www.crnbc.ca/Standards/ProfessionalStandards/Documents/329FitnessPractice.pdf
College of Registered Nurses of Manitoba (2010). Substance Abuse/Misuse: Fact Sheet. Retrieved from: https://www.crnm.mb.ca/uploads/ck/files/RN(NP)s%20MAID%20may17.pdf
Health Canada (2013). Information for Health Care Professionals: Cannabis (marihuana, marijuana) and the cannabinoids. Retrieved online at: https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-use-marijuana/information-medical-practitioners/information-health-care-professionals-cannabis-marihuana-marijuana-cannabinoids.html
Louisiana State Board of Nursing (2010). Advisory Statement Regarding Practicing While Taking Prescribed Narcotic Medication. Retrieved from: https://www.lsbn.state.la.us/Portals/1/Documents/DeclaratoryStatements/Declerat20.pdf
Malliarakis, K.D., Smiths, V., Darbo, N. (2012). Regulatory Management of Substance Use in High-Risk Nurse Populations. Journal of Nursing Regulation, 2(4), 32-39.
Manitoba (2001). The Licensed Practical Nurses Act. C.C.S.M. c. L125
National Council of State Boards of Nursing (2016). A Changing Environment: 2016 NCSBN Environmental Scan. Journal of Nursing Regulation, 6(4), 4-37. http://dx.doi.org/10.1016/S2155-8256(16)31007-9
Important information if you are participating in the 2017 CCP Audit!
The CLPNM will contact you by email to inform you of audit outcomes. It is essential that your email address, and all other contact information on file with the CLPNM remain accurate and up-to-date throughout the audit to ensure you do not miss time-sensitive communication that could affect your license.
Maintaining accurate contact information is a requirement of all CLPNM members as per the CLPNM By-Laws.
To review the CLPNM By-laws and the CLPNM Practice Direction: Continuing Competence Program, please visit the CLPNM website.
Information regarding CCP audit timelines can also be found on CLPNM’s website in the CCP Instruction Guide.
2017 CCP AUDIT NOTICE

30Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Former Manitoba licensed practical nurses (LPN) who wish to return to practical nursing in Manitoba, must first
apply to have their eligibility for reinstatement assessed. A reinstatement assessment is used by the College
of Licensed Practical Nurses of Manitoba (CLPNM) to determine whether the length of time the applicant has
been away from practice could impact the individual’s readiness to provide safe and competent nursing care.
Opening a Reinstatement File
In order to open a reinstatement file with the CLPNM, applicants must submit the following items:
• Part 1 – CLPNM Reinstatement Assessment Application Form
• A non-refundable deposit in the amount of $477.74 towards the CLPNM Board-approved reinstatement fee1
A reinstatement assessment file will not be opened until both the application form and fee have been received and processed by the CLPNM. Any documents received by the CLPNM prior to opening a reinstatement file will be held by the CLPNM for 30 days and then destroyed.
Required Documentation
Once a reinstatement file has been opened, the applicant will have up to six months to ensure all of the following documentation is submitted to the CLPNM:
• Part 2 - Unauthorized Practice Declaration Form
• Part 3 – Verification of Registration Form from any regulatory authority that has licensed the applicant to practise
Pre-assessment
The first step in the process is to submit the Reinstatement Pre-assessment Form, which is found on the CLPNM website. Based on information provided on the form, the Registration Department will then email the appropriate reinstatement application package to the email address provided by the applicant. The CLPNM does not provide paper copies of the reinstatement application package.
It is important to note that if a reinstatement applicant has unresolved issues with CLPNM’s Investigation Committee, Discipline Committee and/or the Board of Directors, s/he must first resolve the issues before opening a reinstatement file with the CLPNM. Also, it is important to note that any conditions or restrictions associated with the applicant’s registration prior to leaving the CLPNM register may be reapplied to a reinstated active practising registration.
a profession in the past seven years. This includes any authority with whom they are currently licensed, and authorities that regulate the practise of other professions in Manitoba or in any other jurisdiction.
• Part 4 - Verification of Hours Form from all employers with whom the applicant has been employed as an LPN within the last four years.
• A current (within 6 months from the date of issue) Canada-wide Criminal Record Check with a Vulnerable Sector Search
• A current (within 6 months from the date of issue) Manitoba-issued Child Abuse Registry Check
• A current (within 6 months from the date of issue) Manitoba-issued Adult Abuse Registry Check
Please note that a reinstatement application will only be assessed when all documents have been received; the onus is on the applicant to ensure that all requirements have been supplied. Please note that the CLPNM does not accept reinstatement documents by email or fax; furthermore, all photocopies must be notarized by a Notary Public.
RETURNING TO LPN PRACTICE
1 Fees subject to change. For CLPNM’s current fee schedule, please access the fee schedule on the CLPNM website.

31Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
Assessment Process
Once the CLPNM receives all of the required documentation, the Registration Department will assess the file to determine the applicant’s eligibility to return to the active practising register. The CLPNM may request additional information or documents to assist with this assessment process; likewise, should a registration risk assessment be required, the applicant is responsible for all related costs. Once the assessment is complete, correspondence will be sent to the applicant’s address on file with the CLPNM.
Assessment Outcomes
Possible outcomes of the reinstatement assessment may include one or more of the following:
• Notification of eligibility to apply for active practising registration
• A referral for a Clinical Competence Assessment (CCA)
• A referral to the Practical Nursing Refresher (PNR) program
• A referral to other remedial education
• A decision that the applicant is not a suitable candidate for reinstatement
Costs associated with any assessment and/or education are the responsibility of the applicant and are not included in the CLPNM reinstatement fees.
Registration Decision1
Applicants will be notified of all CLPNM registration decisions in writing, and should the reinstatement assessment provide evidence that the applicant is eligible for reinstatement, an enrolment application form will be provided at that time.
For further information regarding the reinstatement process, please visit the CLPNM website at www.clpnm.ca and review the Reinstatement Fact Sheet located under the “Resource” tab.
Alternatively, you can contact the CLPNM by email at [email protected] or by phone at 204-663-1212 or toll free at 1-877-663-1212.
1 Official registration decisions of the CLPNM will be communicated in writing. No verbal representations or warranties by any staff of the CLPNM will be binding on the CLPNM or relevant to the assessment process by the CLPNM or any subsequent appeal to the Board of the CLPNM.

32Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
In accordance with The Licensed Practical Nurses Act and the Licensed Practical Nurses Regulation, student
practical nurse (SPN) registration is mandatory for all individuals enrolled in a College of Licensed Practical
Nurses of Manitoba (CLPNM) Board-approved practical nurse education program.
How do I know if it is time for me to renew?
The easiest way to confirm your SPN expiry date is to search your name on the Public Register, which can be accessed by visiting the CLPNM website and clicking on “Find an LPN.” The Public Register will list your registration number, your name, your current register (student year 1 or student year 2) and your current expiry date.
It is important to note that SPN registration dates directly correspond to the cohort/intake date of your practical nurse education program, and registration is only valid for a maximum of 12 consecutive months. For example, if your classes begin January 4 but your SPN application is not approved until February 14, your SPN expiry date will be January 4 of the following year as that is when classes for that intake/cohort began. You must remember to renew your student registration yearly and be aware of all deadlines and expiry dates.
How do I renew?
By now you should have received an email from the CLPNM with information on how to renew your SPN registration online. If you have not received this email, please contact the CLPNM right away as it contains important information related to time sensitive deadlines and fees.
How do I access my online profile?
On the CLPNM website, in the top right hand side of the homepage, you must enter your CLPNM log-in credentials, which were provided to you when your student year 1 registration was approved. Once you have entered into your profile, you will be able to access the online renewal system.
I completed my online renewal; how do I know if it was successful?
Once you have submitted an online renewal for student registration, the quickest way to verify if it has been approved is to check the CLPNM’s Public Register. If your student registration has been approved by the CLPNM, the Public Register will reflect a new expiry date.
Please note that the CLPNM may need to contact you about your submitted renewal application prior to your renewal being approved by the CLPNM. As the CLPNM communicates primarily through email correspondence, it is your responsibility to check your email, including your junk folders, for CLPNM correspondence.
What happens if I am late or do not renew?
The deadline to supply your renewal application is four weeks from the date of re-entry into the program. If your completed application is received after the four week deadline, you will be responsible for a late filing fee and assessment fee prior to your registration being approved. It is in your best interested to renew early, so the CLPNM can contact you if there are any concerns with your application.
Please note that without CLPNM SPN registration, you are not entitled to use the protected title of student practical nurse, which may negatively impact your ability to be enrolled in practical nurse education. Furthermore, any unauthorized use of the protected title will be subject to all fees and penalties, which may include a referral to the CLPNM’s Investigation Committee.
Lastly, should you fail to renew your SPN registration, or if you are deemed no longer eligible for SPN registration, you will not be eligible to apply for graduate practical nurse registration, nor be eligible to apply to sit the Canadian Practical Nurse Registration Examination.
Do you want more information about student registration? If yes, please visit:
http://clpnm.ca/registration/students-and-graduates/.
JANUARY 2018 STUDENT REGISTRATION RENEWAL

33Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
2017/2018 FEE SCHEDULE
Pre-authorized Payment Plan (PPP): 10 payments of $38.85 on the 15th of each month from Nov/17 - Aug/18
Payment Options: Visa, Mastercard, Debit, Money Order
Please note that if there is any discrepancy between a fee amount noted in this schedule, and a fee amount noted in another CLPNM document, the fee amounts noted in this schedule will be considered correct.
All fees are subject to change.
Amount GST Total
Active Practicing Registration Renewal Fee (Sep 1 - Nov 1) $370.00 $18.50 $388.50
Nov 2 - Nov 30 (Add late filing administration fee 135.00) $505.00 $25.25 $530.25
Dec 1 - Dec 15 (Add default re-activation fee 170.00) $675.00 $33.75 $708.75
Reinstatement of Registration $825.00 $41.25 $866.25
Application for Enrolment, Active Practicing Registration $470.00 $23.50 $493.50
(Includes a practicing fee of 370.00 and enrolment fee of 100.00)
Graduate Registration Fee $100.00 $5.00 $105.00
Graduate Registration Renewal Fee $100.00 $5.00 $105.00
Student Registration Fee $50.00 $2.50 $52.50
Student Registration Renewal Fee (2nd year students) $50.00 $2.50 $52.50
Late Filing Administrative Fee - Graduates and Students $65.00 $3.25 $68.25
Exam Fee (CPNRE) $400.00 $20.00 $420.00
Late Filing Administrative Fee - Exam $65.00 $3.25 $68.25
DNW - Did Not Write $90.00 $4.50 $94.50
Re-scoring Exam Fee $90.00 $4.50 $94.50
IEN Credential Assessment $420.00 $21.00 $441.00
Endorsement (If currently registered in another Canadian jurisdiction) $300.00 $15.00 $315.00
Re-assessment Fee $150.00 $7.50 $157.50
Practice Hour Assessment Fee $150.00 $7.50 $157.50
Registration Assessment Fee - LPN $150.00 $7.50 $157.50
Registration Assessment Fee - SPN $100.00 $5.00 $105.00
Verification of Registration $90.00 $4.50 $94.50
Educational Session (if directed by order of the CLPNM) $300.00 $15.00 $315.00
Unauthorized Practice Penalty $1,200.00 $60.00 $1,260.00
Appeal of Registration Decision $200.00 $10.00 $210.00
Non-Negotiable Transaction Fee $50.00 $0.00 $50.00
Administrative Fee $90.00 $4.50 $94.50

34Practical Nursing | December 2017 | College of Licensed Practical Nurses of Manitoba
santeenfrancais.com
Les services sociaux et de santé. Offrez-les. Demandez-les… en français.