decision making and end of life care associate professor of clinical medicine, geriatrics and...
TRANSCRIPT

Decision Making andEnd of Life Care
Associate Professor of Clinical Medicine, Geriatrics and CardiologyChief, Bioethics Consultation Service
Montefiore Medical Center, Albert Einstein College of MedicineGNYGCC December 2012

Outline• Informed consent• Decision making capacity• Advance directives• DNR• Palliative Care • Hospice

Mrs. Millie Clark• 73 year old woman• Hypertension, tobacco use• In ER with chest pain, dyspnea• ECG shows acute anterior MI• Recently retired paralegal• Lives with husband• Treated appropriately by ER• Plan for cardiac catheterization• Mrs. Clark refuses

Informed Consent• Process of shared decision making based on
mutual respect and participation• NOT
– Legal protection for the health care provider– A form
• Elements– Disclosure/information exchange– Capacity– Voluntariness– Authorization
Decision Making CapacityFour Elements• Understand• Reason about risks/benefits• Appreciate consequence to self• Make a choice
NOT• A+0 x 3• Any specific diagnosis or prognosis• Memory• MMSE

Decision Making Capacity
• Decision specific• Sliding scale
– Therapeutic Index = Gain/Risk– Lower capacity level needed for choice with
high therapeutic index– Higher capacity level needed for choice with
low therapeutic index– Accept vs. refuse recommended treatment

Challenges• What to disclose
– Diagnosis, prognosis, treatment options, risks/benefits, recommendation
• Standards– Reasonable person, professional, subjective
• Threats to voluntariness– Coercion vs. manipulation vs. framing/persuasion
• Exceptions– Emergency
• Legal requirement vs. ethical obligation

Treatment Refusal• Mrs. Clark refusing cardiac catheterization in
setting of acute anterior MI• Refusal is the beginning of a conversation• Risks/Benefits• Reasons for refusal• Husband arrives in ER, reassures Mrs. Clark• With family support, decides to proceed with
cath

Mrs. Millie Clark• 10 years later - 83 years old, 5 hospitalizations
– HF, COPD
• Lived independently until hip fracture 9 mos. ago• Discharged to sub-acute rehab
– Rehab limited by HF, COPD
• Cognitive and functional decline– Now in long term care
• Pneumonia, worse despite oral antibiotics• Transferred to the ER• Respiratory distress, hypotensive• ER doc deliberates how she should be treated

How to treat Mrs. Clark?• Why is this a question?
• Preference sensitive decision– More than 1 reasonable option– Lifelong implications– Uncertainty
• Values modify equation• Medical facts options

Other questions• Do we have to put her on a ventilator?
– Are we killing her?• Who decides?• Does she have advance directives?• Why is there no info on the NH paperwork?• What is her quality of life?
– Is it a life worth prolonging?• Who can find her family and talk to them?• How can we treat her suffering? • Should Mrs. C be admitted to the ICU?

How to decide?• Decisions should be
• INDIVIDUALIZED
• And made through a
• SHARED DECISION MAKING process analyzing the
• BENEFITS and BURDENS of each care option in the context of each patient’s
• PROGNOSIS, VALUES and GOALS OF CARE.

Shared Decision Making• Patient and clinician work together to
develop plan of care
• Mrs. Clark is only able to mumble yes/no to simple questions

Mrs. Millie Clark• Lacks capacity for decision about intubation
Two questions1.Who is appropriate surrogate decision
maker?– Health Care Proxy– Family surrogate
2.How do I get to know who Mrs. Clark is?– Values
• Advance Directives• Loved ones• Medical providers
Advance Directives• 1. Proxy directive: Formally assigning
decision-making power to a trusted person (health care proxy or durable power of attorney for health care).
• 2. Treatment directive: Expressing wishes about the kind of care preferred in case of inability to decide independently (living will or oral statements).

Role of the Health Care Agent
• Health care agent is the representative of the patient
• Entrusted to speak for the patient• Involved in the discussions• Must be willing, capable of taking on the
proxy role

Mrs. Mille Clark
• No designated a health care agent• Widow, Mr. Clark died 5 years ago• 2 children Ron and Barbara• 2 brothers and 1 sister• 5 grandchildren

Decision making for the incapacitated patient• If no HCP, turn to next of kin as informal
surrogate decision makers• Hierarchy• States vary regarding rights and
responsibilities of non-HCP surrogates• NYS Family Health Care Decisions Act
– June 2010– Empowers informal surrogates to decide– Limits authority of surrogate for decisions about
life sustaining treatment
How should surrogates decide?• Patient’s known preferences
– prior oral or written statements
• Patient’s wishes to the best of their knowledge– what the patient would do (substituted judgment)
• What is best for the patient – Balance benefits and burdens (best interest)
• Autonomy– Designated decision maker– Decide as patient would

Advance Directives• 1. Proxy directive: Formally assigning
decision-making power to a trusted person (health care proxy or durable power of attorney for health care).
• 2. Treatment directive: Expressing wishes about the kind of care preferred in case of inability to decide independently (living will or oral statements).
Living Will• Standard for articulating decisions in advance• If…. Then….• Requires interpretation in real time• Boilerplate language diminishes
– Specificity (gives unintended directions)– Sensitivity (leaves out important directions)
• Current situation may not have been anticipated• Can’t do shared decision making with a living will• Patients who have a living will are assumed to
have a set of values (shorthand)• Preferences change over time

Mrs. Millie Clark• No living will• She and her children are close• Arrive to the ER within a few minutes• Would your mother want to be on a
ventilator?

Communication• Good communication is important• Breaking bad news• Patient and loved ones are under stress• Not easy to talk about prognosis, values• Emotional• Frank information delivered
compassionately• Communication preferences vary

Communication• Language is critical
• Unhelpful, but common– “do everything”– “what should we do if your mother’s heart stops?”– ‘there’s nothing more we can do”
• Get to know the patient, demonstrate respect• Appropriate amount of detail, no jargon• Lay out options in nonjudgmental way• Prompt for questions
• “Tell me about your mother”• “What do you understand so far?”

• Voice of the patient, report patient’s preferences• Minimize influence of own values and preferences• Challenges
– May not know patient’s preferences accurately– Surrogate has important concerns, values, preferences,
interests– Patients may want surrogates to consider their own
values and concerns – Patients may want surrogates to interpret wishes in
context of medical facts
• Cultural variation• Definition of autonomy
Traditional Surrogate Role

Being a Surrogate Decision Maker• Emotional distress/grief• Other significant stressors• Insecure over role, unsure of decisions• Marginalized from decision making process• Often only involved at end of life• Different perspective from clinicians• Want more guidance• Variability in preferred approach

Shared Surrogate Decision Making
• Assess decision making preferences• Share the burden of decision• Learn about the patient as a person• Patient values guide medical
recommendations

Mrs. Millie Clark• Children and ER doc decide to go ahead with
intubation and ventilator support• Other family• Uncertainty in prognosis• Hopeful that she’ll eventually do rehab• No ventilator long term• To her, that is not a life worth living• Want to know that they could take her off of
ventilator in future• Time limited trial
Potential Goals of Care
• Cure of disease• Avoidance of
premature death • Maintenance or
improvement in function
• Prolongation of life
• Relief of suffering• Quality of life• Staying in control• A good death • Support for families
and loved ones

Goals of Care• Applying the patient’s values to the available
medical options• Clinicians define the options, benefits and
burdens – achievable goals• Patients/families weigh the B/B and place value
on outcomes• Why difficult?
– Time constraints– Requires expert communication skills– Breaking bad news– Uncertainty– Broad view of possible goals– Weeds

Mrs. Millie Clark• Given the plan for time limited trial of ventilator
to determine whether this intervention supports Mrs. Clark to recover to a functional status which she would consider a life worth living, but not to use it to maintain her in a prolonged dependent state, the MD suggests a DNR order

Do Not Resuscitate• Order not to do ACLS in the setting of
cardiac or respiratory arrest– Not a statement about treatment in general
• If no DNR order, patient assumed to want attempt at resuscitation
• Do not attempt resuscitation• Common values based discussion• Popular culture vs reality

Do Not Resuscitate• Often thought of as short hand for goals of
care or patient’s values• NOT a goal of care• Best approached as one of many
decisions made subordinate to the big picture
• Risks/benefits of CPR differ in different care settings
• Ron and Barbara authorize a DNR order

Palliative Care• Is Millie Clark appropriate for palliative care?

Palliative Care• Interdisciplinary, patient and family-centered
care that aims to relieve suffering and improve quality of life for patients with serious or life threatening illness and their families
• Suffering– Physical, practical, existential, psychosocial, spiritual
• It is offered simultaneously with all other appropriate medical treatment.
• Across the continuum of care
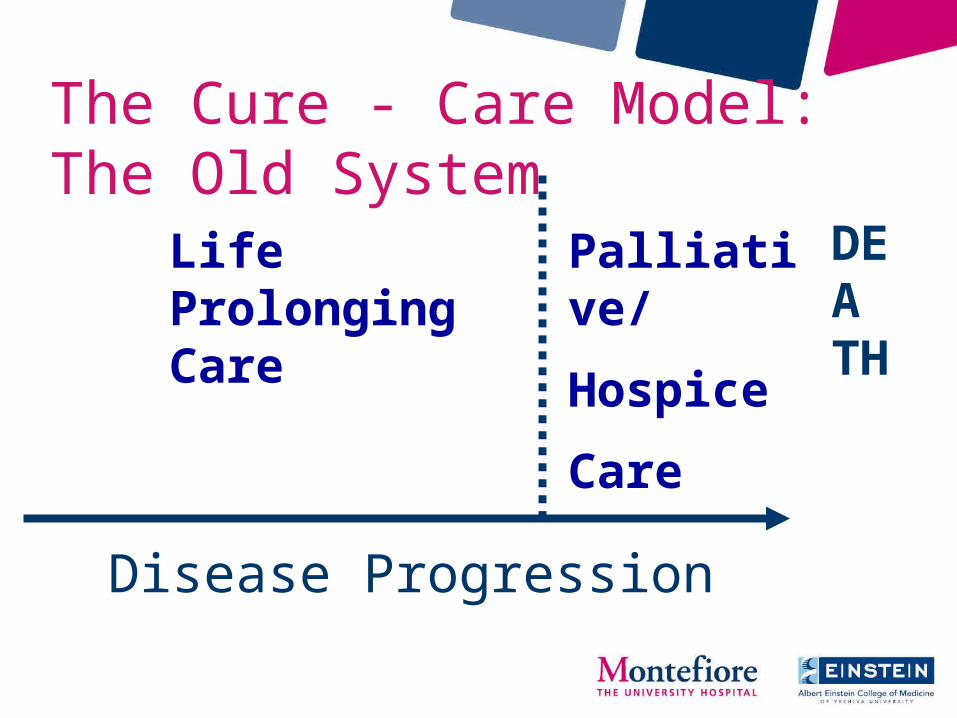
The Cure - Care Model: The Old System
Life Prolonging Care
Palliative/
Hospice
Care
DEATH
Disease Progression

Death &Bereavement
Diagnosis
Disease modifying therapy
Palliative Care
Palliative Care
NHWG; Adapted from work of the Canadian Palliative Care Association & Frank Ferris, MD
HospiceCare

Palliative Care• Communication• Assessment and treatment of
symptoms• Psychosocial, spiritual and
bereavement support• Care coordination

Hospice• End of life care• Focused on comfort• Eligibility criteria
– Prognosis of ≤ 6 months if disease follows its usual course
– Willingness to give up regular Medicare coverage for curative or life prolonging treatment of the terminal illness
• Pays for extra services/ equipment

• Thank you• Questions