dehydration nice lecture
TRANSCRIPT

Dehydration and Dehydration and rehydrationrehydration
Dr. saeid Dr. saeid
Family physician Family physician
20142014

Physiology Physiology
Composition of body fluids:Composition of body fluids: Water is the most plentiful constituent of human Water is the most plentiful constituent of human
body.body. Total body water (TBW) as a percentage of body Total body water (TBW) as a percentage of body
weight varies with age.weight varies with age. In term infants TBW is 75%In term infants TBW is 75% Premature have higher TBWPremature have higher TBW During the first year TBW decreases to 60%, During the first year TBW decreases to 60%,
and remains at this level until puberty.and remains at this level until puberty.
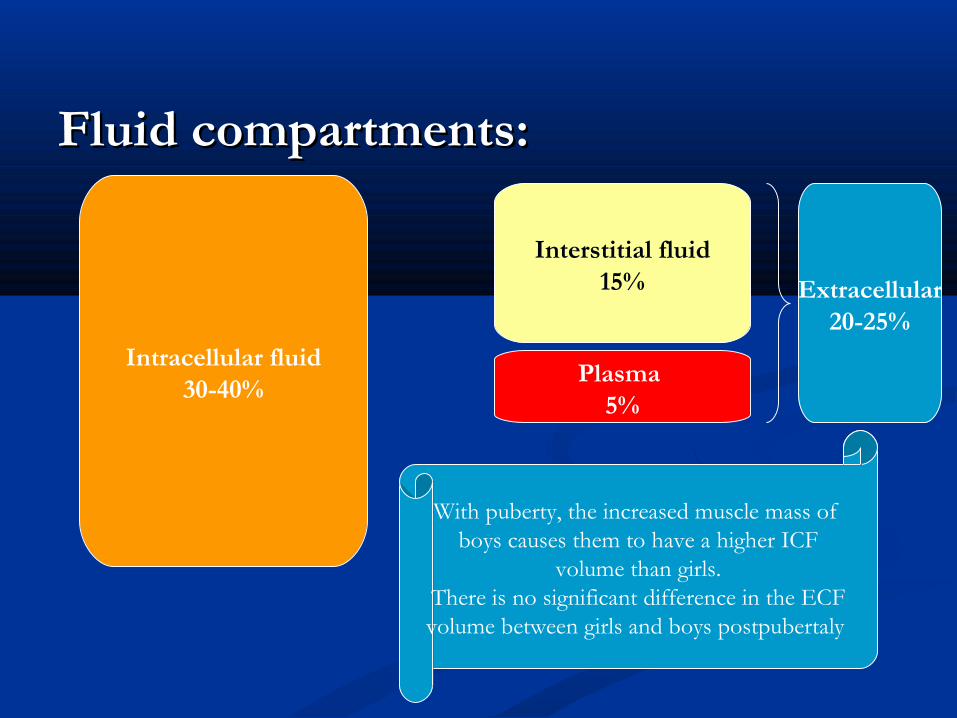
Fluid compartments:Fluid compartments:
Intracellular fluid30-40%
Interstitial fluid15%
Plasma 5%
Extracellular20-25%
With puberty, the increased muscle mass of boys causes them to have a higher ICF
volume than girls.There is no significant difference in the ECFvolume between girls and boys postpubertaly

Electrolyte composition:Electrolyte composition:

Osmolality:Osmolality:
The plasma osmolality is normally 285-295 The plasma osmolality is normally 285-295 mOsm/kg.mOsm/kg.
Osmolality = 2* Na + glucose/18Osmolality = 2* Na + glucose/18 If the osmolality in one compartment changes, If the osmolality in one compartment changes,
then water movement leads to a rapid then water movement leads to a rapid equalization of osmolality.equalization of osmolality.
Hypothalamus senses changes in the osmolality Hypothalamus senses changes in the osmolality through two receptors; one for ADH, the other through two receptors; one for ADH, the other for thirst.for thirst.
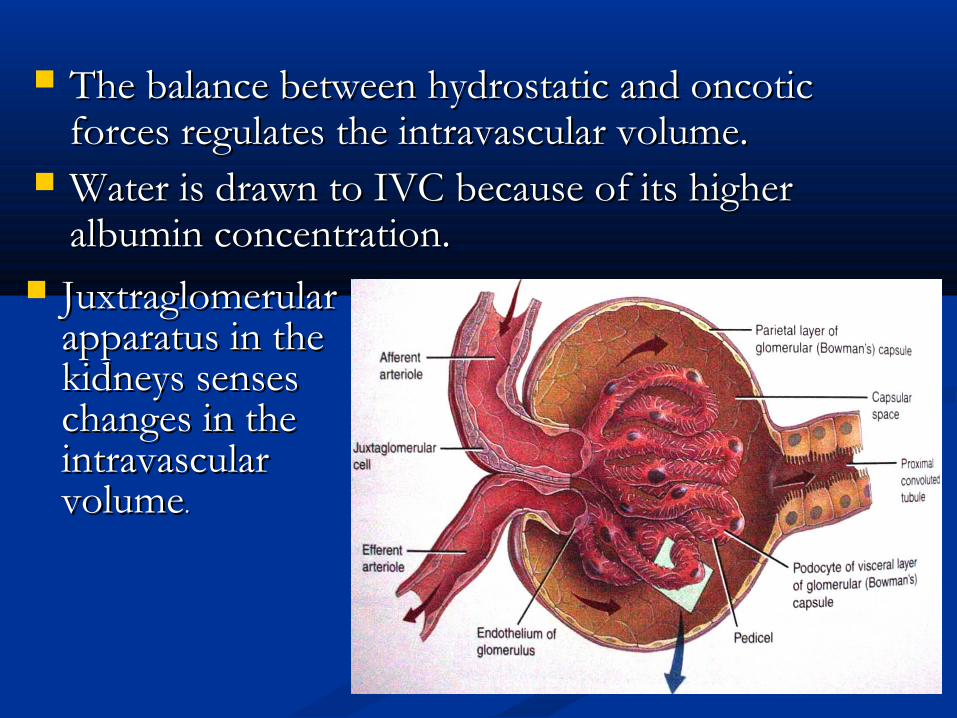
The balance between hydrostatic and oncotic The balance between hydrostatic and oncotic forces regulates the intravascular volume.forces regulates the intravascular volume.
Water is drawn to IVC because of its higher Water is drawn to IVC because of its higher albumin concentration.albumin concentration.
Juxtraglomerular Juxtraglomerular apparatus in the apparatus in the kidneys senses kidneys senses changes in the changes in the intravascular intravascular volumevolume..

Why is dehydration common in Why is dehydration common in infants?infants?
1.1. Infants have a different body composition to Infants have a different body composition to adults 70-80% body water content versus 60% adults 70-80% body water content versus 60% in adults.in adults.
2.2. High fluid intake: 150 ml/kg/day compared to High fluid intake: 150 ml/kg/day compared to 30-40 ml/kg/day in adults.30-40 ml/kg/day in adults.
3.3. Daily water turnover of 10-15% of body Daily water turnover of 10-15% of body weight copared to 3-5% in adults.weight copared to 3-5% in adults.
4.4. Relative reduction in renal ability to Relative reduction in renal ability to concentrate urine.concentrate urine.
5. Greater surface area/mass ratio resulting in 5. Greater surface area/mass ratio resulting in high insensible fluid losses through skin and high insensible fluid losses through skin and respiratory tract.respiratory tract.
6. Higher basal metabolic rate plus greater febrile 6. Higher basal metabolic rate plus greater febrile response to infection.response to infection.
7. Infants have little or no control over fluid 7. Infants have little or no control over fluid intake.intake.
A normal state of hydration is manifested by A normal state of hydration is manifested by bright eyes, moist tongue and good skin bright eyes, moist tongue and good skin turgor.turgor.
The fluid spaces:The fluid spaces:
First space = the intravascular spaceFirst space = the intravascular space Second space = the interstitial spaceSecond space = the interstitial space Third space = fluid in pleural cavity, peritoneal Third space = fluid in pleural cavity, peritoneal
cavity, GIT …etc.cavity, GIT …etc.Fluid losses in the third space are concealed and Fluid losses in the third space are concealed and
may be unconsidered.may be unconsidered.* Mild-moderate dehydration = ↓ interstitial * Mild-moderate dehydration = ↓ interstitial
volumevolume* Sever dehydration = ↓ intravascular volume* Sever dehydration = ↓ intravascular volume
Internationally: Internationally: diarrheal illnesses with diarrheal illnesses with subsequent dehydration account for nearly 4 subsequent dehydration account for nearly 4 million deaths per year in infants and children. million deaths per year in infants and children.
Mortality/Morbidity: Mortality/Morbidity: Mortality and morbidity Mortality and morbidity are generally dependent upon the severity of are generally dependent upon the severity of dehydration and the promptness of oral or dehydration and the promptness of oral or intravenous rehydration. If treatment is rapidly intravenous rehydration. If treatment is rapidly and appropriately obtained, morbidity and and appropriately obtained, morbidity and mortality are low. mortality are low.
Age: Age: Children younger than 5 years are at the Children younger than 5 years are at the highest risk. highest risk.
Dehydration:Dehydration:
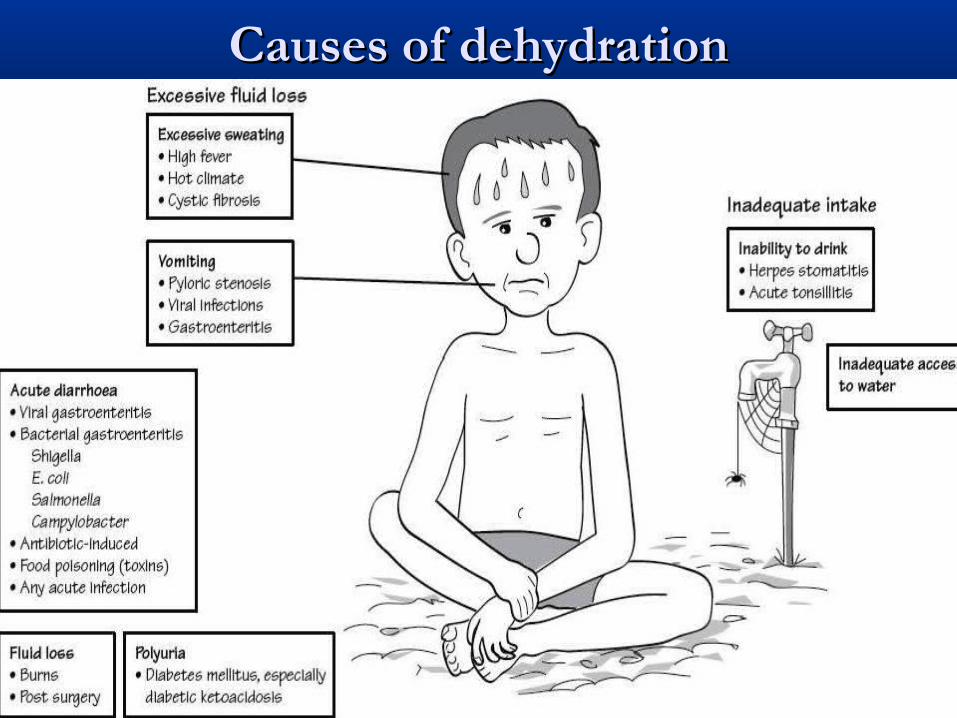
Causes of dehydrationCauses of dehydration

Assessment of the degree of Assessment of the degree of dehydration:dehydration:
History: History: Intake of fluids, including the volume, type Intake of fluids, including the volume, type
(hypertonic or hypotonic), and frequency(hypertonic or hypotonic), and frequency Urine output, including the frequency of Urine output, including the frequency of
voiding, presence of concentrated or dilute voiding, presence of concentrated or dilute urine, hematuriaurine, hematuria
Stool output, frequency of stools, stool Stool output, frequency of stools, stool consistency, presence of blood or mucus in consistency, presence of blood or mucus in stoolsstools
Emesis, including frequency and volume and Emesis, including frequency and volume and whether bilious or nonbilious, hematemesiswhether bilious or nonbilious, hematemesis

Contact with ill people, especially others with Contact with ill people, especially others with gastroenteritisgastroenteritis
Underlying illnesses, diabetes mellitus, Underlying illnesses, diabetes mellitus, hyperthyroidism, renal diseasehyperthyroidism, renal disease
FeverFever Appetite patternsAppetite patterns Weight lossWeight loss Recent antibiotic useRecent antibiotic use Possible ingestionsPossible ingestions
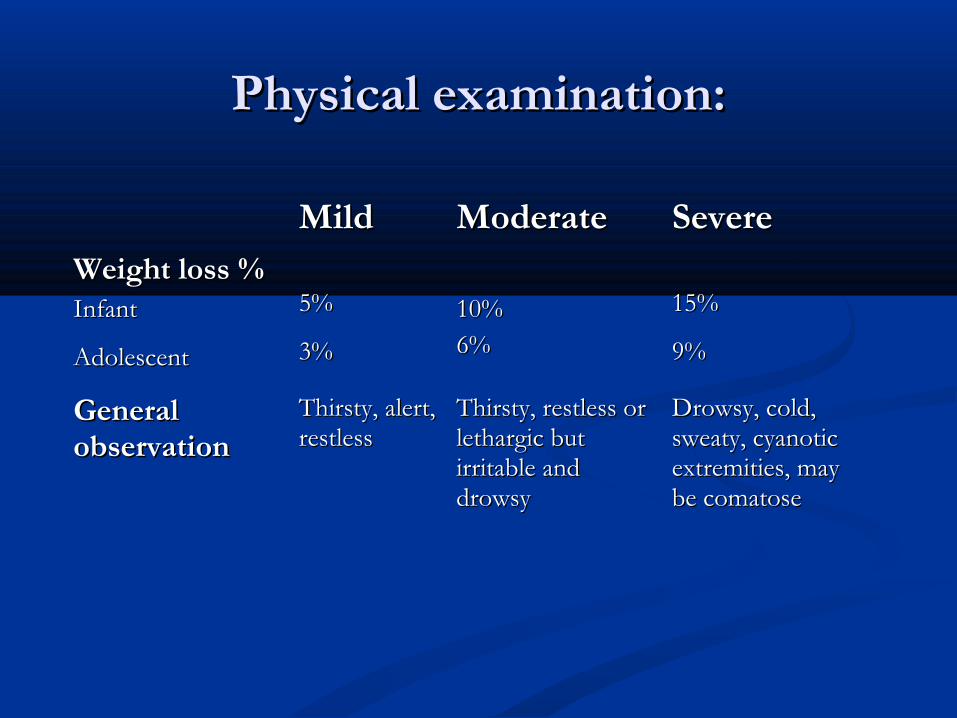
Physical examination:Physical examination:
MildMild ModerateModerate SevereSevere Weight loss %Weight loss %Infant Infant
AdolescentAdolescent
5%5%
3%3% 10%10%6%6%
15%15%
9%9%
General General observationobservation
Thirsty, alert, Thirsty, alert, restless restless
Thirsty, restless or Thirsty, restless or lethargic but lethargic but irritable and irritable and drowsydrowsy
Drowsy, cold, Drowsy, cold, sweaty, cyanotic sweaty, cyanotic extremities, may extremities, may be comatose be comatose

Physical examination...continuedPhysical examination...continued
Signs and Signs and symptomssymptoms
MildMild ModerateModerate SevereSevere
Tachycardia Tachycardia
Palpable pulsesPalpable pulses
Blood pressureBlood pressure
RespirationRespiration
FontanelleFontanelle
TearsTears
Mucous membraneMucous membrane
Skin turgorSkin turgor
Urine outputUrine output
AbsentAbsent
PresentPresent
NormalNormal
NormalNormal
NormalNormal
PresentPresent
MoistMoist
NormalNormal
NormalNormal
PresentPresent
Present (weak)Present (weak)
Postural hypotensionPostural hypotension
Deep, may be rapidDeep, may be rapid
Slightly depressedSlightly depressed
Present or absentPresent or absent
DryDry
Slight reductionSlight reduction
OliguriaOliguria
PresentPresent
DecreasedDecreased
HypotensionHypotension
Deep and rapidDeep and rapid
SunkenSunken
AbsentAbsent
Very dryVery dry
ReducedReduced
Anuria and sever oliguriaAnuria and sever oliguria


Types of dehydration:Types of dehydration:
According to the serum level of sodium, According to the serum level of sodium, dehydration is divided into:dehydration is divided into:
1.1. Isonatremic: serum [NaIsonatremic: serum [Na++] = 130-150 mEq/L] = 130-150 mEq/L
2.2. Hyponatremic: serum [NaHyponatremic: serum [Na++] is < 130 mEq/L] is < 130 mEq/L
3.3. Hypernatremic: serum [NaHypernatremic: serum [Na++] is > 150 mEq/L] is > 150 mEq/L

Pathophysiology:Pathophysiology:
Isonatremic dehydration:Isonatremic dehydration: It is the commonest, account for 70-80% of It is the commonest, account for 70-80% of
cases of dehydration.cases of dehydration. There is a proportionate loss of water and There is a proportionate loss of water and
sodium.sodium. The serum osmolality is the same.The serum osmolality is the same.

Account for 10-20%Account for 10-20% Disproportionately large net losses of water Disproportionately large net losses of water
compared with losses of electrolytes.compared with losses of electrolytes. Causes:Causes:
1.1. Inadequate intake of water, either due to Inadequate intake of water, either due to emesis, lack of access to water, or anorexia.emesis, lack of access to water, or anorexia.
2.2. Administration of badly home-prepared ORSAdministration of badly home-prepared ORS
3.3. Feeding a boiled skim milkFeeding a boiled skim milk
4.4. Increased evaporative water loss from fever, Increased evaporative water loss from fever, hot climate, and hyperventilation.hot climate, and hyperventilation.
HypernatremicHypernatremic dehydration:dehydration:

Children with hypernatremia often appear less ill Children with hypernatremia often appear less ill than children with a similar degree of isotonic than children with a similar degree of isotonic dehydration. This is because there is movement dehydration. This is because there is movement of water from intracellular to extracellular space of water from intracellular to extracellular space protecting the intravascular volume.protecting the intravascular volume.
It is the most dangerous one due to It is the most dangerous one due to complications of hypernatremia and its therapy.complications of hypernatremia and its therapy.
Children are often lethargic but irritable when Children are often lethargic but irritable when touched. Hypernatremia may cause fever, touched. Hypernatremia may cause fever, hypertonea, and hypertonea, and hyper-reflexiahyper-reflexia..
Hypernatremia can cause serious neurologic Hypernatremia can cause serious neurologic damage including hemorrhage and thrombosis. damage including hemorrhage and thrombosis. This appear to be secondary to movement of This appear to be secondary to movement of water from brain cells into the extracellular fluid, water from brain cells into the extracellular fluid, causing brain cell shrinkage and tearing blood causing brain cell shrinkage and tearing blood vessels within the brain.vessels within the brain.

The pinched abdominal skin has a doughy feel.The pinched abdominal skin has a doughy feel. Hypernatremia is associated with hyperglycemia Hypernatremia is associated with hyperglycemia
and mild hypocalcemia and mild hypocalcemia the mechanism is unknown.the mechanism is unknown. Seizures and coma are possible sequelae of the Seizures and coma are possible sequelae of the
hemorrhage, even though they are more hemorrhage, even though they are more common during treatment.common during treatment.
Thrombosis occur secondary to dehydration and Thrombosis occur secondary to dehydration and possibly hypercoagulability associated possibly hypercoagulability associated hypernatremia.hypernatremia.

Hyponatremic dehydration:Hyponatremic dehydration: Account for 10-15% of all patients with Account for 10-15% of all patients with
diarrheadiarrhea It is usually due to combination of sodium and It is usually due to combination of sodium and
water loss and water retention to compensate water loss and water retention to compensate for the volume depletion.for the volume depletion.
Causes:Causes:1.1. Diarrhea has, on average, a sodium Diarrhea has, on average, a sodium
concentration of 50 mEq/L. the patient drinks concentration of 50 mEq/L. the patient drinks water or formula which has low sodium, there water or formula which has low sodium, there will be a reduction in the serum sodium will be a reduction in the serum sodium concentration.concentration.

2. Volume depletion stimulates synthesis of ADH 2. Volume depletion stimulates synthesis of ADH thus reducing renal water excretion.thus reducing renal water excretion.
3. Loss of fluid with a high sodium concentration, 3. Loss of fluid with a high sodium concentration, as may occur with renal salt wasting, third space as may occur with renal salt wasting, third space losses, or diarrhea with a high sodium content losses, or diarrhea with a high sodium content (e.g. cholera).(e.g. cholera).
During hyponatremia there is movement of During hyponatremia there is movement of water into the cells causing increase in water into the cells causing increase in intracellular water and cell swelling; this is not intracellular water and cell swelling; this is not problematic in most tissues of the body, but it is problematic in most tissues of the body, but it is potentially catastrophic in the brain, increasing potentially catastrophic in the brain, increasing the intracranial pressure.the intracranial pressure.

There is a more substantial intravascular volume There is a more substantial intravascular volume depletion than a patient with hypertonic or depletion than a patient with hypertonic or isotonic dehydrationisotonic dehydration
Neurological symptoms include; nausea, Neurological symptoms include; nausea, vomiting, confusion, malaise, lethargy, headache, vomiting, confusion, malaise, lethargy, headache, seizure, and seizure, and decreased reflexesdecreased reflexes..
Acute severe hyponatremia can cause brain stem Acute severe hyponatremia can cause brain stem herniation, apnea, cheyne stoke breathing, and herniation, apnea, cheyne stoke breathing, and hypothermia.hypothermia.

Lab findings:Lab findings:
Laboratory data are generally not required if the Laboratory data are generally not required if the etiology is apparent and mild-to-moderate etiology is apparent and mild-to-moderate dehydration is present.dehydration is present.
Serum sodium concentration determines the Serum sodium concentration determines the type of dehydration.type of dehydration.
Blood PH, CO2, and HCO3 level to determine Blood PH, CO2, and HCO3 level to determine whether there is acidosis or alkalosis:whether there is acidosis or alkalosis:
Low pH, high CO2, and low HCO3 indicate Low pH, high CO2, and low HCO3 indicate metabolic acidosis; while high pH indicate metabolic acidosis; while high pH indicate metabolic alkalosis.metabolic alkalosis.

Anion gap to differentiate between the various Anion gap to differentiate between the various causes of metabolic acidosis which may occur causes of metabolic acidosis which may occur due to:due to:
1.1. Stool bicarbonate losses in children with Stool bicarbonate losses in children with diarrheadiarrhea
2.2. Secondary renal insufficiencySecondary renal insufficiency3.3. Lactic acidosis from decreased tissue perfusionLactic acidosis from decreased tissue perfusion Metabolic alkalosis may occur due to emesis Metabolic alkalosis may occur due to emesis
and nasogastric losses.and nasogastric losses.

Serum potassium concentration:Serum potassium concentration:Causes of hyperkalemia:Causes of hyperkalemia:1.1. Metabolic acidosis causing shinfting of Metabolic acidosis causing shinfting of
potassium into the extracellular fluid.potassium into the extracellular fluid.2.2. Renal failureRenal failure3.3. Congenital adrenal hyperplasia Congenital adrenal hyperplasia
Causes of hypokalemia:Causes of hypokalemia:1.1. Emesis (e.g. pyloric stenosis)Emesis (e.g. pyloric stenosis)2.2. Metabolic alkalosisMetabolic alkalosis3.3. Urinary potassium lossesUrinary potassium losses

Renal function tests: BUN and Renal function tests: BUN and serum creatinineserum creatinine
Blood urea is increased without renal Blood urea is increased without renal insufficiency secondary to increased passive insufficiency secondary to increased passive reabsorption of urea in the PCT due to reabsorption of urea in the PCT due to appropriate renal conservation of sodium and appropriate renal conservation of sodium and water. water.

The baseline normal creatinine concentration The baseline normal creatinine concentration increases with age e.g. in infants = 0.2 mg/dl, at increases with age e.g. in infants = 0.2 mg/dl, at 5 year 0.4 mg/dl, at 10 year 0.6 mg/dl, at 15 year 5 year 0.4 mg/dl, at 10 year 0.6 mg/dl, at 15 year 1 mg/dl.1 mg/dl.

Urinalysis:Urinalysis:
Urinalysis is most helpful in the measurement of Urinalysis is most helpful in the measurement of urine specific gravity, a specific gravity of less urine specific gravity, a specific gravity of less than 1.020 indicate mild or no dehydration or than 1.020 indicate mild or no dehydration or indicates a urinary concentrating defect, as in indicates a urinary concentrating defect, as in chronic renal disease or primary or secondary chronic renal disease or primary or secondary diabetes insipidus.diabetes insipidus.
Hyaline or granular casts, a few WBC and RBCs, Hyaline or granular casts, a few WBC and RBCs, and 30-100 mg/dl of proteinuria. These findings and 30-100 mg/dl of proteinuria. These findings remit with therapy and are not usually associated remit with therapy and are not usually associated with significant renal pathology.with significant renal pathology.

Hemoconcentration:Hemoconcentration: Hemoconcentration causes an increase in the Hemoconcentration causes an increase in the
hematocrit, hemoglobin, and serum proteins in hematocrit, hemoglobin, and serum proteins in dehydration. These values normalize with dehydration. These values normalize with rehydration. rehydration.
A normal hemoglobin concentration during A normal hemoglobin concentration during acute dehydration may mask an underlying acute dehydration may mask an underlying anemia. anemia.
A decreased albumin in a dehydrated patient A decreased albumin in a dehydrated patient suggests a chronic disease, such as malnutrition, suggests a chronic disease, such as malnutrition, nephrotic syndrome, or liver disease, or an acute nephrotic syndrome, or liver disease, or an acute process, such as capillary leak. process, such as capillary leak.
RehydrationRehydration

Oral rehydration:Oral rehydration:
ORS is used in many countries and has ORS is used in many countries and has significantly reduced the morbidity and mortality significantly reduced the morbidity and mortality from acute diarrhea.from acute diarrhea.
Mild and moderate dehydration from diarrhea of Mild and moderate dehydration from diarrhea of any cause can be treated effectively using a any cause can be treated effectively using a simple ORS containing glucose and electrolytes.simple ORS containing glucose and electrolytes.
The glucose or sucrose is present in ORS to The glucose or sucrose is present in ORS to enhance sodium and water absorption, not as a enhance sodium and water absorption, not as a calorie source.calorie source.

Composition of ORS (mmol/L):Composition of ORS (mmol/L):
Solution Solution GlucoseGlucose NaNa++ KK++ ClCl-- BaseBase Osmolality Osmolality
WHOWHO 111111 9090 2020 8080 3030 311311
RehydralRehydralyteyte
140140 7575 2020 6565 3030 310310
Pedialyte Pedialyte 140140 4545 2020 3535 3030 250250

Making ORS at home:Making ORS at home:

Some points about ORS for the mother:Some points about ORS for the mother: Wash your hands withWash your hands with soap and water before soap and water before
preparing solution, and before feeding the child. preparing solution, and before feeding the child.
Prepare a solution, in a clean pot, by mixing Prepare a solution, in a clean pot, by mixing - one teaspoon salt and 8 teaspoons sugar. If - one teaspoon salt and 8 teaspoons sugar. If possible, add 1/2 cup orange juice or some possible, add 1/2 cup orange juice or some mashed banana to improve the taste and provide mashed banana to improve the taste and provide some potassium. some potassium. or or - 1 packet of Oral Rehydration Salts (ORS) - 1 packet of Oral Rehydration Salts (ORS) - with one litre of clean drinking or boiled water - with one litre of clean drinking or boiled water (after cooled)(after cooled)Stir the mixture till all the contents dissolve.Stir the mixture till all the contents dissolve.

Give the sick child as much of the solution Give the sick child as much of the solution as it needs, in small amounts frequently.as it needs, in small amounts frequently.
Give child alternately other fluids - such as Give child alternately other fluids - such as breast milk and juices.breast milk and juices.
Continue to give solids if child is four Continue to give solids if child is four months or older. months or older.
If the child still needs ORS after 24 hours, If the child still needs ORS after 24 hours, make a fresh solution.make a fresh solution.
ORS does not stop diarrhoea. It prevents the ORS does not stop diarrhoea. It prevents the body from drying up. The diarrhoea will stop by body from drying up. The diarrhoea will stop by itself.itself.
Generally 5 ml every minute is well tolerated. If Generally 5 ml every minute is well tolerated. If the child vomits, wait ten minutes and give it the child vomits, wait ten minutes and give it again. Usually vomiting will stop as the child again. Usually vomiting will stop as the child becomes hydrated.becomes hydrated.

Intravenous solutions:Intravenous solutions:
A normal plasma osmolality is 285-295 A normal plasma osmolality is 285-295 mOsm/kg. infusing an intravenous solution mOsm/kg. infusing an intravenous solution peripherally with a much lower osmolality can peripherally with a much lower osmolality can cause hemolysis. Thus intravenous fluids are cause hemolysis. Thus intravenous fluids are generally designed to have an osmolality that is generally designed to have an osmolality that is either close to 285 or moderately higher.either close to 285 or moderately higher.
Indications for IV therapy:Indications for IV therapy:
1.1. Moderate dehydration when there is no Moderate dehydration when there is no improvement after the firs 4 hours of improvement after the firs 4 hours of treatment with ORS.treatment with ORS.
2.2. Severe dehydrationSevere dehydration
3.3. Uncontrolled vomitingUncontrolled vomiting
4.4. Patients unable to drink from extreme fatigue, Patients unable to drink from extreme fatigue, stupor, or comastupor, or coma
5.5. Patients with gastric or intestinal distentionPatients with gastric or intestinal distention

Composition of IV solutions:Composition of IV solutions:
Fluid Fluid NaNa++ ClCl-- KK++ CaCa+2+2 Lactate Lactate
NS (0.9% NaCl)NS (0.9% NaCl) 154154 154154
½ NS (0.45 NaCl)½ NS (0.45 NaCl) 7777 7777
¼ NS (0.225% NaCl)¼ NS (0.225% NaCl) 38.538.5 38.538.5
Ringer lactate Ringer lactate 130130 109109 44 33 2828

NS and ringer lactate are isotonic solutions used NS and ringer lactate are isotonic solutions used for the acute correction of intravenous volume. for the acute correction of intravenous volume.
½ NS and ¼ NS are the usual choices for ½ NS and ¼ NS are the usual choices for maintenance fluid therapy in children. These maintenance fluid therapy in children. These solutions are available with 20 mEq/L of KCl, solutions are available with 20 mEq/L of KCl, 10 mEq/L KCl, or no potassium.10 mEq/L KCl, or no potassium.

Monitoring of IV therapy:Monitoring of IV therapy:
1.1. Vital signs: pulse and blood pressureVital signs: pulse and blood pressure
2.2. Intake and output: fluid balance, urine output Intake and output: fluid balance, urine output and specific gravity.and specific gravity.
3.3. Physical examination: weight, clinical signs of Physical examination: weight, clinical signs of depletion or overload.depletion or overload.
4.4. Electrolytes: should be measured daily.Electrolytes: should be measured daily.
The treatment should be modified based on the The treatment should be modified based on the clinical situation of the patient.clinical situation of the patient.
Maintenance fluids:Maintenance fluids:
These fluids represent the normal daily water These fluids represent the normal daily water losses from the body which could be measurable losses from the body which could be measurable (urine and stool) and not measurable ((urine and stool) and not measurable (insensibleinsensible losses from the skin and lungs). The daily water losses from the skin and lungs). The daily water losses are as follow: urine 60%, insensible losses losses are as follow: urine 60%, insensible losses 35% (1/335% (1/3rdrd maintenance), and stool 5%. maintenance), and stool 5%.
Maintenance fluids are composed of a solution Maintenance fluids are composed of a solution of water, glucose, sodium, potassium, and of water, glucose, sodium, potassium, and chloride. chloride.

The glucose in maintenance fluids provides The glucose in maintenance fluids provides approximately 20% of the normal caloric needs approximately 20% of the normal caloric needs of the patient, this percentage is enough to of the patient, this percentage is enough to prevent the development of starvation prevent the development of starvation ketoacidosis and diminishes the protein ketoacidosis and diminishes the protein degradation that would occur if the patient degradation that would occur if the patient received no calories. received no calories.
Glucose also provides added osmoles, avoiding Glucose also provides added osmoles, avoiding the administration of hypotonic fluids, which the administration of hypotonic fluids, which may cause hemolysis.may cause hemolysis.
Maintenance fluids usually contain 5% dextrose. Maintenance fluids usually contain 5% dextrose. Children weighing less than 20 kg do best with Children weighing less than 20 kg do best with D5 in ¼ NS + 20 mEq/L of potassium D5 in ¼ NS + 20 mEq/L of potassium chloride. chloride.
In contrast, larger children and adults may In contrast, larger children and adults may receive the solution with D5 in ½ NS + 20 receive the solution with D5 in ½ NS + 20 mEq/L of potassium chloride.mEq/L of potassium chloride.

Calculation of maintenance water Calculation of maintenance water and electrolytes:and electrolytes:
Body weightBody weight WaterWater(ml/kg/24 hr)(ml/kg/24 hr)
SodiumSodium(mmol/kg/24hr(mmol/kg/24hr))
PotassiumPotassium(mmol/kg/24 hr)(mmol/kg/24 hr)
First 10 kgFirst 10 kg 100100 2-42-4 1.5-2.51.5-2.5
Second 10 kgSecond 10 kg 5050 1-21-2 0.5-1.50.5-1.5
Subsequent kgSubsequent kg 2020 0.5-10.5-1 0.2-0.70.2-0.7

Calculation of deficit:Calculation of deficit:
Water deficit = % dehydration * weightWater deficit = % dehydration * weight Sodium deficit = water deficit * 80 mEq/L, Sodium deficit = water deficit * 80 mEq/L,
while in hyponatremic dehydration it is while in hyponatremic dehydration it is calculated as follow sodium deficit = 0.6 * calculated as follow sodium deficit = 0.6 * weight * ([Naweight * ([Na++]]dd - [Na - [Na++]] ii))
Potassium deficit = water deficit * 30 mEq/LPotassium deficit = water deficit * 30 mEq/L % of dehydration % of dehydration ==
previous wt - current wtprevious wt - current wt 100100
previous wtprevious wt

Ongoing losses:Ongoing losses:
1.1. Fever leads to a predictable increase in insensible Fever leads to a predictable increase in insensible losses, causing a 10-15% increase in maintenance losses, causing a 10-15% increase in maintenance water needs for each 1water needs for each 1ooC increase in temperature C increase in temperature greater than 38 greater than 38 ooC.C.
2.2. Adjusting fluid therapy for gastrointestinal losses:Adjusting fluid therapy for gastrointestinal losses: The replacement of ongoing losses from diarrhea is a The replacement of ongoing losses from diarrhea is a
solution of 5% dextrose in ¼ NS + 15 mEq/L solution of 5% dextrose in ¼ NS + 15 mEq/L bicarbonate + 25 mEq/L potassium chloride. Replace bicarbonate + 25 mEq/L potassium chloride. Replace the stool ml/ml every 1-6 hr.the stool ml/ml every 1-6 hr.

The replacement of ongoing losses from emesis The replacement of ongoing losses from emesis is a solution of 5% dextrose in ½ NS + 10 is a solution of 5% dextrose in ½ NS + 10 mEq/L potassium chloride. mEq/L potassium chloride.
Replace output ml/lm every 1-6 hr.Replace output ml/lm every 1-6 hr.

3.3. Adjusting fluid therapy for altered renal output: Adjusting fluid therapy for altered renal output: Oliguria/Anuria: 1/3 maintenance, and replace Oliguria/Anuria: 1/3 maintenance, and replace
urine output ml/ml with ½ NS.urine output ml/ml with ½ NS. Polyruia: 1/3 maintenance, measure urine Polyruia: 1/3 maintenance, measure urine
electrolytes, and replace urine output ml/ml electrolytes, and replace urine output ml/ml with a solution that is based on the measured with a solution that is based on the measured urine electrolytes.urine electrolytes.
4.4. Output form surgical drains and chest tubes, Output form surgical drains and chest tubes, when significant, should be measured and when significant, should be measured and replaced.replaced.

Management of mild and moderate Management of mild and moderate dehydration:dehydration:
This can be successfully done by ORT. This can be successfully done by ORT.
1.1. Deficit: Deficit:
- Mild dehydration: 50 ml/kg/ 4 hr- Mild dehydration: 50 ml/kg/ 4 hr
- Moderate dehydration: 100 ml/kg/ 4 hr- Moderate dehydration: 100 ml/kg/ 4 hr
2.2. Maintenance: when rehydration is complete, Maintenance: when rehydration is complete, maintenance therapy should be started, using maintenance therapy should be started, using 100 ml of ORS/kg/ 24 hr until diarrhea stops.100 ml of ORS/kg/ 24 hr until diarrhea stops.

3.3. Ongoing loss: Ongoing loss: Supplementary ORS is given to replace ongoing Supplementary ORS is given to replace ongoing
losses form diarrhea or emesis, and additional 10 losses form diarrhea or emesis, and additional 10 ml/kg of ORS is given for each stoolml/kg of ORS is given for each stool
Fluid intake should be decreased if the patient Fluid intake should be decreased if the patient appears fully hydrated earlier than expected or appears fully hydrated earlier than expected or develops periorbital edema. develops periorbital edema.
Breastfeeding should be allowed after Breastfeeding should be allowed after rehydration in infants who are breastfed; in rehydration in infants who are breastfed; in other patients, their usual formula, milk, or other patients, their usual formula, milk, or feeding should be offered after rehydration.feeding should be offered after rehydration.

Treatment of sever dehydrationTreatment of sever dehydration
A- A-
Total intravenous fluid requirements in severe dehydration
Treat shock% of dehydration *
Weight (kg)Maintenance
Continuing losses:•Fever•Hyperventilation•Vomiting and diarrhea•Pooling of fluid in the gut

B- B-
Phase 1:Phase 1:
Treat shockTreat shock
(0-0.5 hr) Repeat * 2(0-0.5 hr) Repeat * 2
if necessary if necessary
Phase 2:Phase 2:
RehydrationRehydration
Initial intravenous fluid management in sever dehydration
20 ml/kg of NS or ringer lactate
No changeImproves
Low plasmasodium
Normalplasmasodium
High plasmasodium

Low plasmasodium
Normalplasmasodium
High plasmasodium
0.45% saline/dextrose+ KCl replacement
over 24 hours
0.45% saline/dextrose+ KCl replacement
over 48 hours
Close monitoring: fluid balance, clinical condition, weight,plasma creatinine and electrolytes

D-D-
C- C-
Maintenance intravenous fluid requirements
Calculating and replacing the ongoing loses
E-E-
An age appropriate diet should be started when the child is rehydrated

Management of isonatremic Management of isonatremic dehydration:dehydration:
1.1. Restore intravascular volume (treat shock): 20 Restore intravascular volume (treat shock): 20 ml/kg of NS or ringer lactate over 20 min ml/kg of NS or ringer lactate over 20 min (repeate if necessary until intravascular volume (repeate if necessary until intravascular volume restores which can be decided through restores which can be decided through continuous monitoring of the patient; lower continuous monitoring of the patient; lower heart rate, normalization of the blood pressure, heart rate, normalization of the blood pressure, improved perfusion, and more alert).improved perfusion, and more alert).
2.2. Calculate 24 hour maintenance water and Calculate 24 hour maintenance water and electrolyteselectrolytes
3.3. Calculate 24 hour deficit water and electrolytesCalculate 24 hour deficit water and electrolytes

4. The total amount of water and electrolytes are 4. The total amount of water and electrolytes are added together, then an appropriate fluid is added together, then an appropriate fluid is selected. Potassium is usually not included in selected. Potassium is usually not included in the IV fluids until the patient voids, unless the IV fluids until the patient voids, unless significant hypokalemia is present.significant hypokalemia is present.
5. Total correction is done within the first 24 5. Total correction is done within the first 24 hours. Administer half the calculated fluid hours. Administer half the calculated fluid during the first 8 hours, first subtracting any during the first 8 hours, first subtracting any boluses from this amount, then administer the boluses from this amount, then administer the reminder over the next 16 hours.reminder over the next 16 hours.
6. Replace ongoing losses as they occur 6. Replace ongoing losses as they occur
Management of hyponatremic Management of hyponatremic dehydration:dehydration:
Most patients do well with the same basic strategy of Most patients do well with the same basic strategy of isonatremic dehydration. The difference is in the isonatremic dehydration. The difference is in the calculation of sodium deficit.calculation of sodium deficit.
D5 ½ NS with 20 mEq/L KCl is usually effective.D5 ½ NS with 20 mEq/L KCl is usually effective. In general it is not necessary to increase the sodium In general it is not necessary to increase the sodium
beyond 135 mEq/L, because over correction is beyond 135 mEq/L, because over correction is associated with an increased risk of central pontine associated with an increased risk of central pontine myelinolysis (CPM). The risk of CPM also increases myelinolysis (CPM). The risk of CPM also increases with overly rapid correction of the serum sodium with overly rapid correction of the serum sodium concentration, so it is important to avoid increasing the concentration, so it is important to avoid increasing the sodium by more than 12 mEq/L each 24 hour.sodium by more than 12 mEq/L each 24 hour.

Patients with neurologic symptoms (e.g. Patients with neurologic symptoms (e.g. seizures) from hyponatremia need to receive an seizures) from hyponatremia need to receive an acute infusion of hypertonic (3%) saline to acute infusion of hypertonic (3%) saline to rapidly increase the serum sodium rapidly increase the serum sodium concentration. concentration.
Each milliliter of 3% NaCl increases the serum Each milliliter of 3% NaCl increases the serum sodium by approximately 1 mEq/L. A child sodium by approximately 1 mEq/L. A child with active symptoms often improves after with active symptoms often improves after receiving 4-6 ml/kg of 3% NaCl.receiving 4-6 ml/kg of 3% NaCl.
The patient’s sodium concentration is monitored The patient’s sodium concentration is monitored to ensure appropriate correction and the sodium to ensure appropriate correction and the sodium concentration of the fluid is adjusted concentration of the fluid is adjusted appropriately.appropriately.

Management of hypernatremic Management of hypernatremic dehydration:dehydration:
Restore intravascular volume: 20 ml/kg NS over Restore intravascular volume: 20 ml/kg NS over 20 min (repeat until intravascular volume 20 min (repeat until intravascular volume restored). Ringer lactate is not preferred because restored). Ringer lactate is not preferred because it is more hypotonic than NS.it is more hypotonic than NS.
Determine the time for correction based on the Determine the time for correction based on the initial sodium concentration:initial sodium concentration:
[Na]: 145-157 mEq/L: 24 hr [Na]: 145-157 mEq/L: 24 hr [Na]: 158-170 mEq/L: 48 hr[Na]: 158-170 mEq/L: 48 hr [Na]: 171-183 mEq/L: 72 hr[Na]: 171-183 mEq/L: 72 hr [Na]: 184-196 mEq/L: 84 hr[Na]: 184-196 mEq/L: 84 hr
Administer fluid at a constant rate over the time Administer fluid at a constant rate over the time for correction.for correction.
Return serum sodium levels toward the Return serum sodium levels toward the reference range by not more than 10 mEq/L/24 reference range by not more than 10 mEq/L/24 hr. (0.5 mEq/L/hr). Rapid correction can have hr. (0.5 mEq/L/hr). Rapid correction can have disastrous neurologic consequences, including disastrous neurologic consequences, including cerebral edema and death.cerebral edema and death.

Following adequate intravascular volume Following adequate intravascular volume expansion, rehydration fluids should be initiated expansion, rehydration fluids should be initiated with 5% dextrose in 0.9% NaCl. with 5% dextrose in 0.9% NaCl.
Serum sodium levels should be assessed every 4 Serum sodium levels should be assessed every 4 hours. hours.
If the sodium has decreased by less than 0.5 If the sodium has decreased by less than 0.5 mEq/L/h, then the sodium content of the mEq/L/h, then the sodium content of the rehydration fluid is decreased D5 in ½ NS). This rehydration fluid is decreased D5 in ½ NS). This allows for a slow controlled correction of the allows for a slow controlled correction of the hypernatremic state. hypernatremic state.
Replace ongoing losses as they occurReplace ongoing losses as they occur

Complications:Complications:
1.1. Loss of consciousnessLoss of consciousness
2.2. Hypovolemic shockHypovolemic shock
3.3. Acute renal failureAcute renal failure
4.4. Renal vein thrombosisRenal vein thrombosis
5.5. Electrolyte imbalanceElectrolyte imbalance
6.6. Relative erethrocytosisRelative erethrocytosis
7.7. DeathDeath

Total fluid = XTotal fluid = X X is given over 24 hours as followX is given over 24 hours as follow
½ X – boluses ¼ X ¼ X
8 hrs 8 hrs 8 hrs

Cases 1Cases 1
A 17 months old child presented with diarrhea A 17 months old child presented with diarrhea and vomiting 2 days before admission, and vomiting 2 days before admission, associated with fever of 40 oC, chills, toxic, associated with fever of 40 oC, chills, toxic, reduced frequency of urine, and his body reduced frequency of urine, and his body weight is 11.7 kg.weight is 11.7 kg.
1.1. DiagnosisDiagnosis
2.2. ManagementManagement
Case 2Case 2
An 18 months old child presented with watery-An 18 months old child presented with watery-rice diarrhea for 1 day before admission, no rice diarrhea for 1 day before admission, no passage of urine, no palpable pulses, and passage of urine, no palpable pulses, and seizures. Previous weight was 14 kg, and the seizures. Previous weight was 14 kg, and the current weight is 12.20 kg.current weight is 12.20 kg.
1.1. DiagnosisDiagnosis
2.2. Cause of seizureCause of seizure
3.3. Management Management

Thank youThank you