dementia: a terminal illness hospice for patients with dementia dr. joette greenstein medical...
TRANSCRIPT

Dementia: A Terminal illness
Hospice for Patients with Dementia
Dr. Joette GreensteinMedical Director, Columbus
Objectives
Define dementia and the prevalence, pathology and trajectories
Identify patients with dementia who are appropriate for hospice care
Review the hospice care benefits for patients with dementia
Explain the Cost of Dementia on the healthcare system
Explain How Hospice can help patients, families, physicians, and caregivers
04/18/23 2
Dementia Definition
Dementia isn’t a specific disease
It describes a group of symptoms affecting intellectual and social abilities severe enough to interfere with daily functioning
Variety of diseases that result in the death of neurons
91% of the time, it is an irreversible disorder that is progressive and Terminal
04/18/23 3
Dementia
The most common form of dementia is Alzheimer’s 60-80% of cases
Most elderly with dementia have Mixed form of Alzheimer’s and another form
Many of these signs apply to other dementias Common Symptom cluster at end of life
Different dementias have different trajectories, symptoms, and treatments Prognosis is related to function and other chronic conditions
04/18/23 4
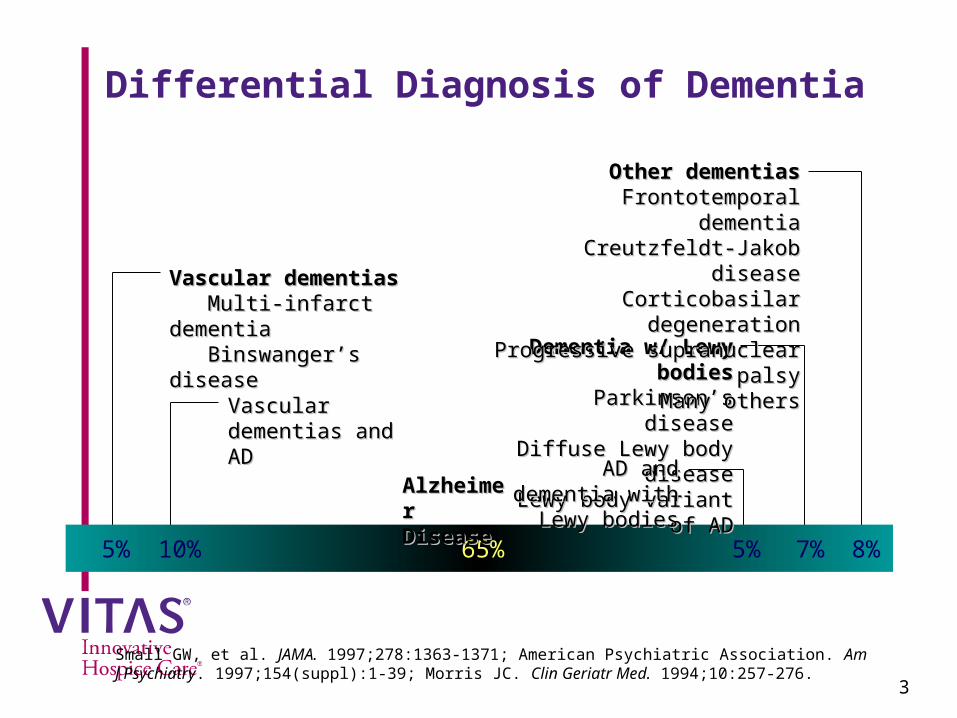
Differential Diagnosis of Dementia
5% 10% 65% 5% 7% 8%
Dementia w/ Lewy bodiesDementia w/ Lewy bodies Parkinson’s disease Parkinson’s disease
Diffuse Lewy body disease Diffuse Lewy body disease Lewy body variant of AD Lewy body variant of AD
Vascular dementias Vascular dementias and ADand AD
Other dementiasOther dementias Frontotemporal dementia Frontotemporal dementia
Creutzfeldt-Jakob disease Creutzfeldt-Jakob disease Corticobasilar degeneration Corticobasilar degeneration
Progressive supranuclear palsyProgressive supranuclear palsy Many others Many others
AD and dementia AD and dementia with Lewy bodieswith Lewy bodies
Vascular dementiasVascular dementias Multi-infarct dementia Multi-infarct dementia Binswanger’s disease Binswanger’s disease
Alzheimer Alzheimer DiseaseDisease
Small GW, et al. JAMA. 1997;278:1363-1371; American Psychiatric Association. Am J Psychiatry. 1997;154(suppl):1-39; Morris JC. Clin Geriatr Med. 1994;10:257-276.
3

Alzheimer's
There is a new case of Alzheimer’s dementia every 68 seconds! By Mid Century every 33 seconds!
Most common form of dementia
6th leading cause of death in the country 5th if over 65
Average duration 4-6 years after diagnosis People live 3-20 years after diagnosis
Lots of Variation
04/18/23 6
Alzheimer’sAD predicted to double every 20 years
“Silver Tsunami”
1/8 Americans >65 Have AD, 1/3 >85 Have AD
2013 5.2 million estimated to have Alzheimer’s 50% are not diagnosed By 2050 estimated to be 11.3 - 16 million
Gallup poll 1:10 Americans had a family member with AD, 1:3 knew someone with AD
67% of people dying from Dementias are in SNF 20% of LTC is cancer diagnosis and 28% other conditions
04/18/23 7
Hospice Related AD Stats
2013 Alzheimer’s Association report revealed in 2009 6% of hospice patients had Alzheimer’s as a primary diagnosis Another 11% had diagnosis of Non-Alzheimer’s dementia
NHPCO reports 12.8% of hospice admissions carried this diagnosis
The Cost of Dementia’s Will Soar
2013 Cost of care for patients who hold a dementia diagnosis is $203 Billion
• They are generally older• They have multiple medical problems DM, CAD,
CHF, and COPD• Have higher healthcare utilization and are at risk
for ED visits and readmission By 2050 the estimate is $1.2 Trillion Dollars Medicare and Medicaid cover 70% of the cost!
04/18/23 9
Cost of Care
2012 15.4 million Americans (60% family members) provide unpaid care to a person with ADRD. Provided 17.5 billion hours of unpaid care
Totaling an estimated $216.4 billion
04/18/23 10
Cost of Care Collateral Damage
Caring for Dementia is stressful for Caregivers and PCP’s Goals of care often put off
• Patient’s are complex and time consuming
Caregivers have higher healthcare utilization
Caregivers have higher number of chronic conditions
• Often Neglect treatment
Caregivers have higher rates of Depression
This Strains the entire health system even more!
04/18/23 11
Alzheimer’s Disease (AD)
One way to definitively diagnose AD - an autopsy identifying plaques and tangles that eventually strangle and destroy cells leading to the failure of other systems in the body
Symptoms - decline in ability to perform routine tasks, disorientation, difficulty in learning, loss of language skills, impairment of judgment, and personality changes
As AD progresses, the person becomes unable to care for themselves
Loss of brain cells eventually leads to the failure of other systems in the body

Normal Aging vs. Alzheimer’s
Temporarily forgetting a colleague’s name
Not being able to remember the name later
Forgetting the carrots on the stove until the meal is over
Forgetting that the meal was ever prepared
Unable to find the right word, but using a fit substitute
Uttering incomprehensible sentences
Forgetting for a moment where you are going
Getting lost on one’s own street
Talking on the phone, and temporarily forgetting to watch a child
Forgetting there is a child
Normal Possible Alzheimer’s
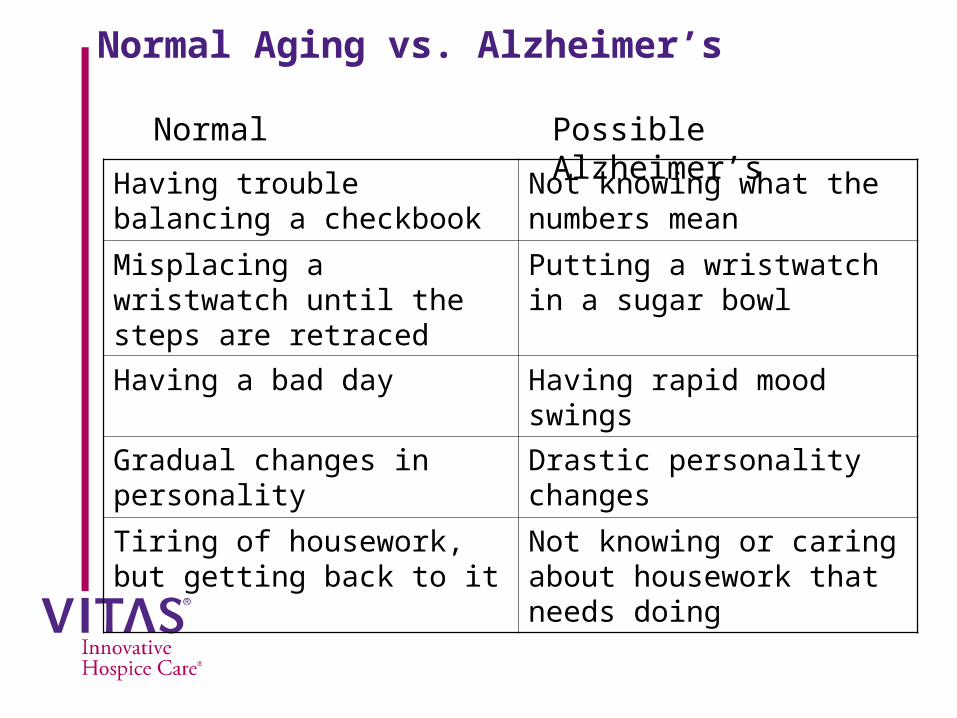
Normal Aging vs. Alzheimer’s
Having trouble balancing a checkbook
Not knowing what the numbers mean
Misplacing a wristwatch until the steps are retraced
Putting a wristwatch in a sugar bowl
Having a bad day Having rapid mood swings
Gradual changes in personality
Drastic personality changes
Tiring of housework, but getting back to it
Not knowing or caring about housework that needs doing
Normal Possible Alzheimer’s
AD Risk Factors
Age The older you get, the greater the risk
1 in 8 over 65 are diagnosed with AD 1 in 3 over 85
Family History (Heredity) Having a parent, brother or sister with AD increases risk of
disease. Risk increases if more than one family member has the illness.
Genetics Early on-set (age 30, 40, 50) caused by mutated gene
Most people have “late-onset” AD, develops after age 60

Top 10 Warning Signs
Memory loss that disrupts daily life Challenges in planning or solving problems Difficulty completing familiar tasks Confusion with time and place Trouble understanding visual images and spatial
relationships
04/18/23 16

Top 10 Warning Signs
New problems with words in speaking and writing
Misplace things and have trouble retracing steps
Decreased or poor judgment
Withdrawal from work or social activities
Changes in mood and personality
Seven Stages of Cognitive Decline
1. No Impairments
2. Very Mild
3. Mild
4. Moderate
5. Moderately severe
6. Severe
7. Very severe
Reisberg, et al (1990). Stage Specific Incidence of Potential Remediable Behavioral Symptoms in Aging and Alzheimer’s Disease. Bulletin of Clinical Neurosciences, 5.

Stages of Dementia
We start preparing hospice in late Stage 6 Severe Dementia Stage 6E
Unable to Live on their own
Dependent in most Activities of Daily Living
Incontinent of Bladder and Bowel
Stage 7 marks end stage dementia pathway Progressive Debility
Loss of ability to speak, ambulate, and interact with environment
04/18/23 19
Stage 6 Cognitive and Behavioral Changes
Severe Cognitive DeclineDeficits evident and widely vary; may include:
Unaware of current life events:
spouse name, dates, season Difficulties bathing, dressing, toilet, transfer, continence, feeding
Daily routine and sleeping patterns disturbed
Wandering away from home or caregiver

Stage 7 Cognitive and Behavioral Changes
Very Severe Cognitive DeclineStage when patient may be appropriate for hospice
Deficits are severe and generally include: Loss of verbal abilities – may grunt, groan
Incontinent – loses control of bladder/bowels
Loss of psychomotor skills like walking, sitting up and smiling
Sleeps longer and more often
Generalized and cortical neurological signs and symptoms are present: Problems with swallowing Visual hallucinations
What Does this Mean?
Alzheimer’s Disease Is A Terminal Diagnosis!
04/18/23 22

Death and Dementia
Generally, death is due to a complication, commonly infection.
Aspiration Pneumonia
Infected decubitus ulcer (associated osteomyelitis, sepsis, etc.)
UTI• These are the proximate causes of death. • Alzheimer's dementia is the primary cause of death
04/18/23 23

Treatment of Proximal Causes of Death
Enhance patient and family comfort Antibiotics (When appropriate)
Feeding tubes in rare cases
IV hydration (When appropriate)
Wound management:
prevention (frequent turning) debridement Wound Vac
04/18/23 24
Dementia Hospice Eligibility is Based on Decline
Cognitive decline: FAST score of 7, confusion, agitation
Functional decline: Increased Dependence in ADL’s,
Nutritional decline: Weight loss despite adequate intake or feeding
tube Clinical decline:
Worsening palliative performance scale, infections
04/18/23 25
Functional Decline
Functional Assessment Staging Tool-7 Stages 1. No difficulties
2. Subjective forgetfulness
3. Decreased job functioning and organizational capacity
4. Difficulty with complex tasks, instrumental ADLs
5. Requires supervision with ADLs
6. Impaired ADLs, with incontinence
7. A. Ability to speak limited to six words
B. Ability to speak limited to single word
C. Loss of ambulation
D. Inability to sit
E. Inability to smile
F. Inability to hold head up
04/18/23 26
Nutritional Decline
Difficulty swallowing or refusal to eat Caloric intake cannot be maintained
Patient/family refuses artificial nutritional support
If patient is already receiving artificial nutritional support Weight loss > 10% of normal body weight
Decreasing Body Mass Index (BMI) <22 kg/m2
Decreasing mid-arm muscle area (MMA)
04/18/23 27
Clinical DeclinePatient has had one or more of the following in the last 6-12
months: Aspiration pneumonia
Urinary tract infections
Blood infections (sepsis)
Pressure ulcers: Stage III or IV
Recurrent fevers, after antibiotics
Weight loss
Comorbid conditions: CHF, CVD, COPD, RLD, DM, CKD, Malignancy
04/18/23 28
Benefits of Hospice
Physical , spiritual and emotional symptoms are much better managed.
Allows patient to remain at home / LTC
Hospice staff (physician, nurse/CM, SW, Chaplain, HHA, Volunteer)
Comfort and dignity
DNR/DNI/DNH (note that none are required for hospice care)
Bereavement for surviving family/friends
Patients on hospice often live longer than they otherwise would.
04/18/23 29
Living Longer Through Hospice
Average length of hospice stay Primary Diagnosis of Alzheimer's increased from 67 days
(1998) to 106 days (2009)
Primary Diagnosis of Non Alzheimer’s Dementia increased 57 days (1998) to 98 days (2009)
04/18/23 30
Benefits of Hospice
Keeps patients in their home
Home health aide Allows patient to remain at facility/home Provides hands on experience for
staff/caregivers in caring for the terminally ill Benefits the physician
Focus Symptom control Goals of care Care of the terminally ill
04/18/23 31

Patient Case
80 y/o female, lives alone, known with AD for 8 years, recently hospitalized for aspiration pneumonia
ADLs: dependent, with urinary incontinence
Unable to ambulate and speech limited to 1-2 words (FAST 7C)
Weight loss of >10% last 6 months
Family’s goal is comfort, patient was moved to a nursing home and referred to hospice
04/18/23 32