screening and assessment in autism spectrum disorders january 14, 2011 joette james, ph.d.,...
TRANSCRIPT

Screening and Assessment in Autism Spectrum Disorders
January 14, 2011
Joette James, Ph.D., Pediatric Neuropsychologist
Presentation Outline
•Early Detection and Screening
•Screening Instruments•Neuropsychological
Evaluation•Executive Functioning•Social Cognition
Why Early Detection/Screening?
• Autism is no longer rare- prevalence rates of 60-116 per 10,000 (Baird et al. 2006, Fombonne, 2006)
• There are identified diagnostic criteria, which target three domains: communication, social interaction, restricted, repetitive and stereotyped behaviors, interests and activities (APA, 2000)
• Confirmation of diagnosis in Autism Spectrum Disorders usually occurs ≥ 3 to 4 years of age (average=4 - 5.5 years in US [CDC, 2007]); but parents often report concerns earlier

Why Early Detection/Screening?
• Several models of early intervention exist, and have shown quantifiable gains in communication, social interaction, cognition, quality of life and independence
• Reduce delay between PCP referral to ASD specialist
• Stability of diagnosis when made at ≥ 24 months (Charman et al., 2005, Cox et al., 1999)
Social/Emotional Milestones (Greenspan, Prizant and Wetherby, 2004)
At 4 months:– Turn towards sounds?– Smile back when you smile?
At 9 months:– Smile often when playing with you?– Coo or babble when happy, cry when
unhappy?
At 12 months:– Use pointing or other showing gestures to
draw attention to something of interest– Exchange many back and forth smiles,
gestures, sounds in a row
Social/Emotional Milestones (Greenspan, Prizant and Wetherby, 2004)
At 18 months:– Use lots of gestures with words to get needs met,
like pointing or taking you by the hand and saying, “want juice”?
– Do simple pretend play, like feeding a doll or stuffed animal, and attracting your attention by looking up at you?
At 24 months:– Do pretend play with you with more than one action,
like feeding the doll and then putting the doll to sleep?
– Enjoy being next to children of the same age and show interest in playing with them, perhaps giving a toy to another child?
•Red Flags in ASD (Wetherby, Woods, Allen et al., 2004)
Impairment in Social Interaction:
- Lack of appropriate eye gaze
– Lack of warm, joyful expressions
– Lack of sharing interest or enjoyment – Lack of response to name
Red Flags in ASD
Impairment in Communication:• Lack of showing gestures
• Lack of coordination of nonverbal communication
• Unusual prosody (little variation in pitch, odd intonation, irregular rhythm, unusual voice quality)

Red Flags in ASD
Repetitive Behaviors & Restricted Interests:
• Repetitive movements with objects • Repetitive movements or posturing of
body, arms, hands, or fingers
Screening for ASDs
• Screening is defined as “a brief assessment procedure designed to identify children, who, because of the risk of a possible learning problem or handicapping condition should proceed to a more intensive level of diagnostic assessment” (Meisels & Atkins-Burnett, 1994)
• AAP recommends universal screening for ASDs at both 18 and 24 months (Johnson et al., 2007)
• Two levels- Level 1- at-risk children in general population; Level 2- identify risk for Autism among range of developmental problems
Types of Screening Instruments
• Infant versus Toddler versus preschool/school-age
• Autism versus Asperger’s Disorder
• Observational/Interactive versus Checklist
• Parent versus Professional
CAST (Williams et al., 2004)
• Childhood Asperger Syndrome Test • Level 1 parent screener• For use in ages 4 to 11• 37-item questionnaire (including 6
control items)• Scoring: Maximum score is 31, with 15
as cutoff for ASD or related social-communication difficulties
• Sensitivity: 0.88-1.0; Specificity: 0.97-0.98
ASSQ (Ehlers, Gillberg and Wing, 1999)
• Autism Spectrum Screening Questionnaire• Level 2 parent or teacher screener• For use in ages 6 to 17• 27-item checklist (No/Somewhat/Yes)• 11 items relate to social interaction, 6 to
communication, 5 to restricted/repetitive behaviors, remaining to associates symptoms
• Recommended cutoff is 19 for parents, 22 for teachers
• Sensitivity: 0.62-0.82 (parent); 0.65-0.70 (teacher)

SCQ (Rutter et al., 2003)
• Social Communication Questionnaire; formerly Autism Screening Questionnaire (ASQ)
• Developed from Autism Diagnostic Interview, Revised (ADI-R)
• For use with ≥4 yrs, mental age at least 2 years
• Parent checklist, 40 yes/no items• Current (past 3 months) and Lifetime forms• Social, communication, behavior items; cutoff
is 15• Sensitivity: 0.85-0.96; Specificity: 0.67-0.80
SRS (Constantino, 2005)
• Social Responsiveness Scale (4-18 years)• 65-item scale, Likert scoring• Parent and teacher versions,
male/female forms• 5 subscales: Social Awareness, Social
Cognition, Social Communication, Social Motivation, Autistic Mannerisms
• Total T-score ≥76 from 2 informants strongly suggests ASD
The Neuropsychological Evaluation- Role
• neural substrates of behavior• cognitive profile underlying “symptoms”
(internal logic of negative behaviors)• description of strengths and
weaknesses (versus diagnosis)• prediction of risk and identification of
environments and settings conducive to success

Neuropsychological Domains
• Attention• Executive Functions• Language• Nonverbal Cognition• Learning/Memory• Social Cognition• Sensory/Motor Abilities
Cognitive Profile in High Functioning Autism
WEAKNESSES• Social Cognition• Executive
Function• Language
Pragmatics• Motor
STRENGTHS• Verbal Data Bases• Rote Learning• Detail Analysis• Crystallized
Intelligence
Functional Domains of the Executive
– Initiate - begin task, activity, attention– Working Memory - hold information actively in
mind– Inhibit - stop an action or not react to impulse– Shift - move from one task or situation to another– Plan - anticipate future events and develop steps– Organize - establish, maintain order– Self-monitor - attend to behavior/output; revise– Emotional Control - regulate emotional response
Outcome of “Good” Executive Functioning
• Purposeful, goal-directed activity• Active problem solving • Self-control• Independence• Reliability and consistency• Positive self-efficacy • Internal locus of control

The “Dysfunctional” Executive
– Initiate - deficits beginning task, activity– Working Memory - difficulties holding information
actively in mind– Inhibit - problems stopping an action– Shift - difficulties moving from one task or situation
to another, perseveration, rigidity– Plan - deficits anticipating future events and
developing steps– Organize - problems establishing, maintaining order– Self-monitor - lack of attention to own behavior or
performance– Emotional Control - deficits regulating emotional
response

Executive Function ComponentsMost Affected in ASD
Measurement issues in EF: Comprehensive assessment indicates all domains are affected (Gioia et al, 2002), especially:
• Shift (Rumsey, 1985, Courchesne, 1994)• Plan/Organize (Ozonoff, 1991, Hughes, 1994)• Literature reviews: Pennington & Ozonoff,
1996; Sergeant, Geurts & Oosterlaan, 2002

BRIEF- Inhibit
• Gets in your face• Has trouble stopping when silly• Is squirmy• Does not stop laughing at joke when friends
stop• Has to be closely supervised• Des not think before doing• Acts wilder or sillier than others in groups• Makes odd noises, hums, mutters or sings• Interrupts others

BRIEF- Shift
• Does same thing over and over for no apparent reason
• Is stubborn• Cannot get a disappointment off their mind• Resists accepting a different way to solve a
problem• Becomes upset with new situations• Tries same approach to problems even when it
doesn't work• Acts upset by change in plans• Not creative in problem solving
BRIEF- Working Memory
• Is absent-minded• When given three things to do,
remembers only the first or last• Trouble with multistep chores• Forgets when he was doing• Trouble remembering things even for a
few minutes
BRIEF- Plan/Organize
• Tests poorly despite knowing answers• Good ideas but can't get the job done• Written work poorly organized• Starts project without the right materials• Trouble planning for future play activities• Does not connect tonight's homework with
grades• Unrealistic goals• Underestimates time needed to complete
tasks
BRIEF- Monitor
• Doesn't ask for help when needed• Doesn't check work for mistakes• Makes careless errors• Poor handwriting• Unaware of how behavior affects others• Leaves work incomplete

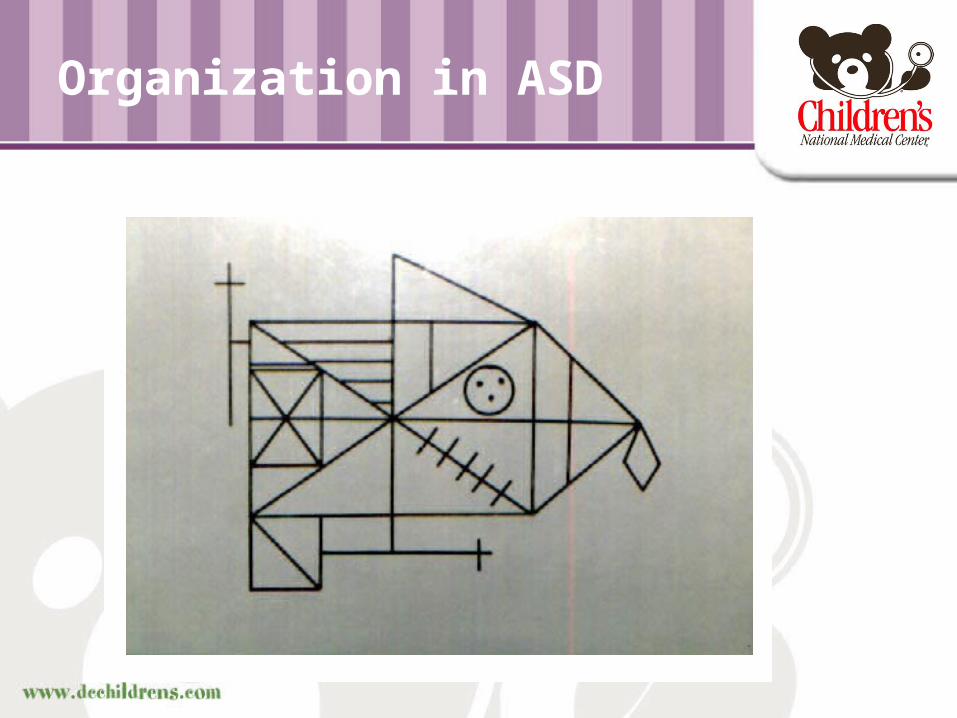
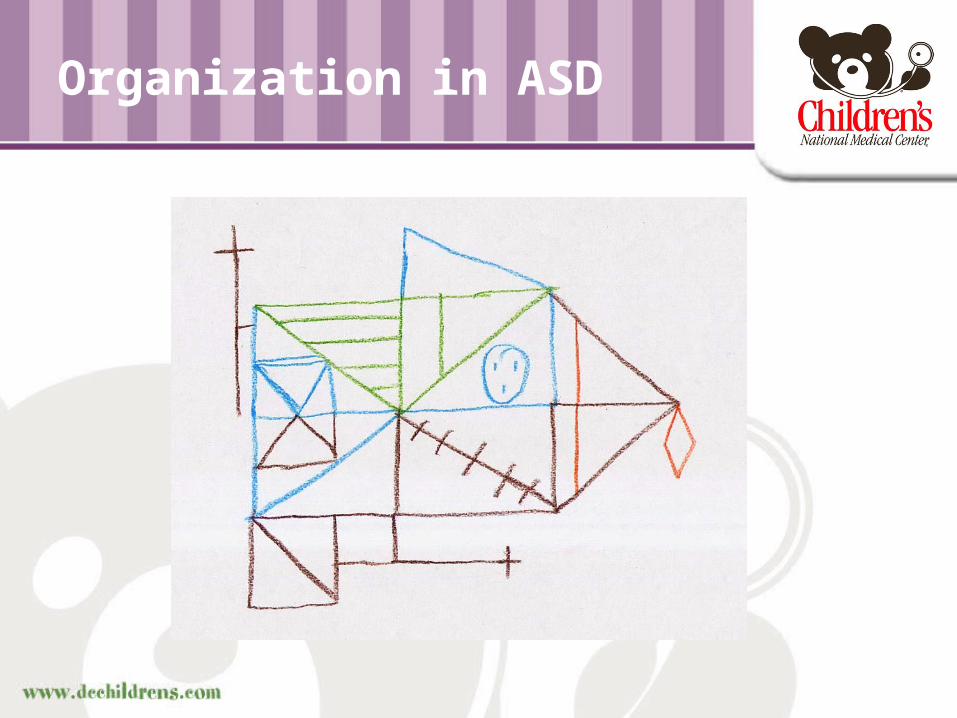
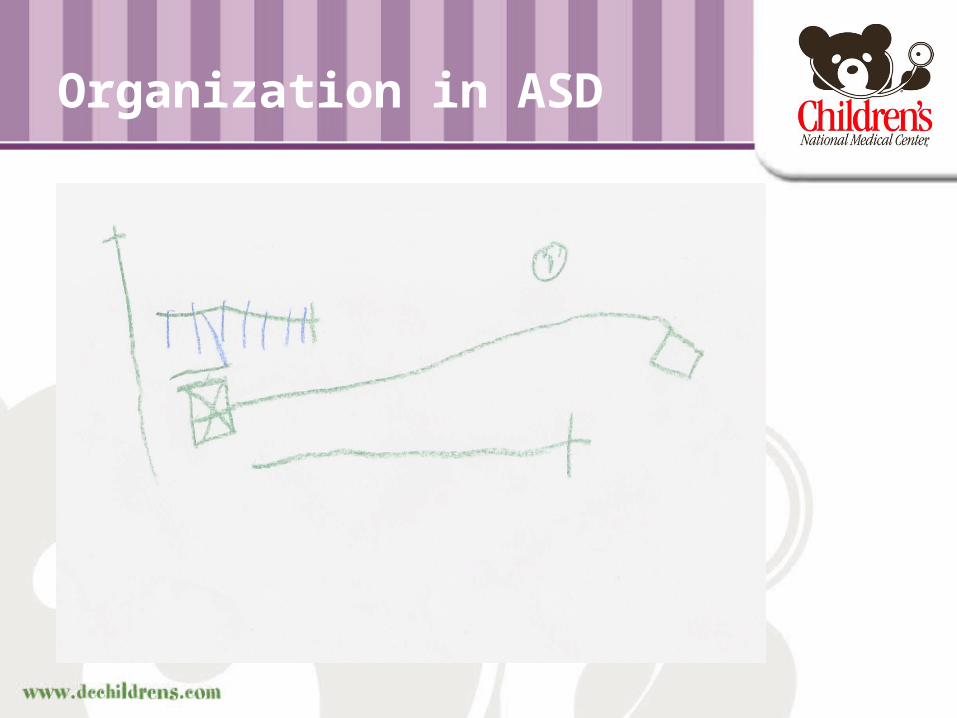
Organization in ASD
• Children with ASD show:– Intact (even superior) vocabulary, verbal
learning and verbal knowledge– But, difficulty organizing/accessing their
verbal databases and communicating effectively
– Intact appreciation of visual detail– But difficulty organizing complex visual data
Organization in ASD
Organization in ASD
Organization in ASD
Social Skills and Executive Functioning
• Respect for others• Social give and take• Ability to respond
to needs of others• Getting big picture
in a social setting• Real world social
skills
• Inhibition, Self-Monitor
• Poor shifting of attention
• Inflexibility, Emotional Control
• Organization Deficits
• Multiple EF demand
Social Cognition Defined
The ability to comprehend socially relevant information.
In social psychology- study of social knowledge, social structure, group behavior, social influence, processing bias
In evolutionary biology- learning and memory in social context, territoriality, dominance, subordination
In developmental psychology- relationship between cognitive abilities and social competence, learning in social context (Vygotsky)
In clinical context- one aspect of social cognition is the understanding of mental states, including false belief (Theory of Mind)

Components of Social Cognition
• Recognize faces- ubiquity of facial expressions
• Interpret and express emotion in: intonation, facial expression, body language, gesture, verbal nuance
• Label emotions in self and others• Describe others meaningfully• Discern social rules/ problem-solve • Engage in imaginative play• Understand social role• Understand the nature of relationships

Skills of Emotional Competence (Saarni, 1999)
• Awareness of one’s emotional state• Ability to discern other’s emotions• Ability to use the vocabulary of emotion• Capacity for empathy and sympathy• Ability to realize that inner emotional state
need not correspond to outer expression• Capacity for adaptive coping to distress/self-
regulation• Understanding how type of relationship (and
context) define how emotions are expressed

Social Interaction and the Early Environment
• Social orienting/referencing (auditory and visual)– Within a few days of birth, babies show a preference
for their mother’s face and voice over others– Newborns prefer to look at whole faces vs. scrambled
faces– Babies are drawn to look where another is looking,
prefer direct eye contact (Farroni et al., 2002)
• Joint attention– The ability to share a common focus with another
person (i.e. looking in the direction that the other person is looking, following a pointing gesture)- apparent from the first year of life
– Central to characterizing toddlers with autism (Lord, 1995)
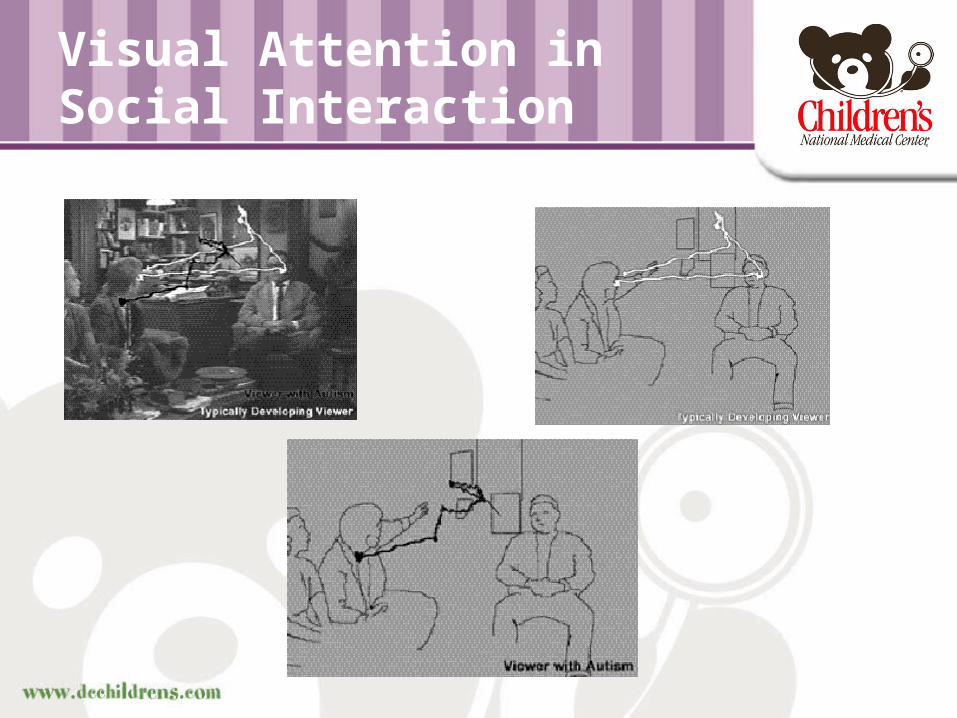
Visual Attention in Social Interaction
Theory of Mind
• Ability to ascribe beliefs and desires to others in order to predict behavior/ inferring the mental states of others
• Awareness of pretense, irony, deception, cause and effect, motivation
• Sally and Ann scenarios (Baron-Cohen, 1985)
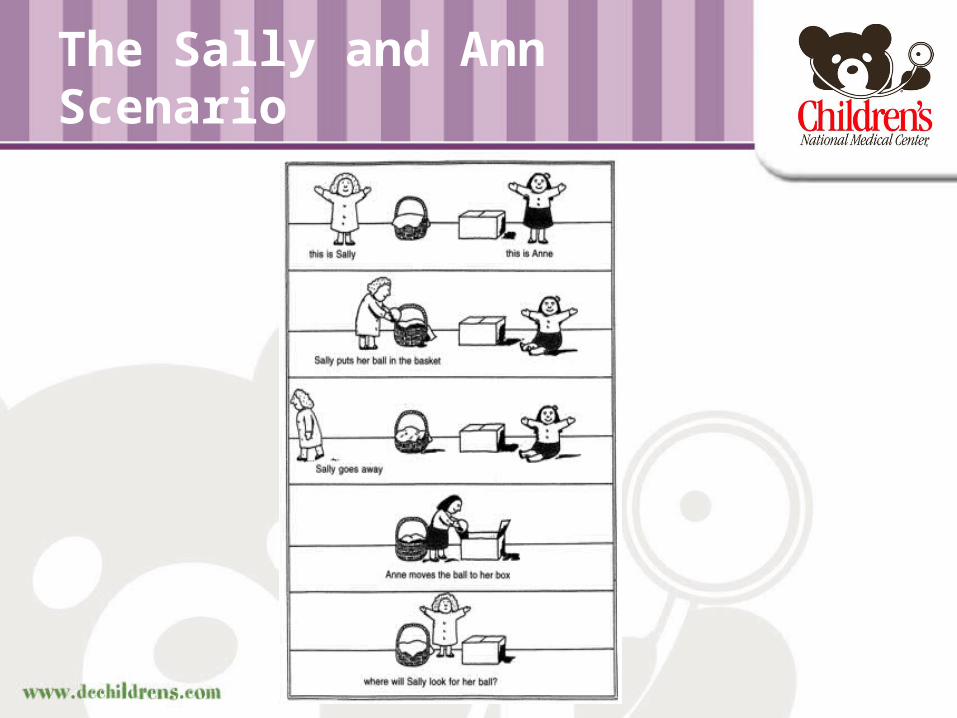
The Sally and Ann Scenario
Assessing Social Cognition- Test of Language Competence• Test of Language Competence (TLC)-
Oral Expression: Recreating Speech Acts- child is shown a picture with three “overheard” words- task is to formulate meaningful sentence within a social context
• In autism- description versus conversation, difficulties with formulation/organization (EF)
Assessing Social Cognition- Roberts Apperception Test• Roberts Apperception Test- 6 cards-
Homework, Nightmare, Anger, Parents’ Concern, Bullies, Tragedy
• Is child able to:– Read emotional cues (simple/complex)– Social problem solve (adaptive ?)– Organize/formulate language
Roberts Apperception Test
In response to “Anger Card”:“ He is happy and lifting the chair up.
And his mother said don’t do that, so he put the chair down and walked away happy.”
In response to “Bully Card”:“Once there was a little boy who was
always confused. And those two boys said “What’s the matter?” “I’m always confused,” said the boy. That’s the end.”

Assessing Social Cognition- NESPY-II
• Affect Recognition– Recognition of emotional expressions-
same/different, affect matching, memory – Affect Recognition Total score, error-based
percentiles for individual emotions– Potential confounds: visual attention, visual
discrimination, attention, working memory
Assessing Social Cognition- NEPSY-II
• Theory of Mind– “assesses the ability to understand mental
functions such as belief, intention, deception, emotion, imagination and pretending”
– Includes classic “seeing leads to knowing,” “false belief,” “bluff” and “double bluff” tasks
– Potential confounds: attention, working memory, language
– Heterogeneity of items?
Autism Diagnostic Observation Schedule (ADOS- Lord et al.) • Designed to provide standardized
information about an individual’s social behavior with an unfamiliar adult, use of language and play
• Primary emphasis is on creating occasions in which the participant can take social initiative
Assessing Social Cognition- ADOS
• The ADOS is grouped into four modules based on expressive language level:– Module 1- Pre-verbal to 3-word phrases– Module 2- 3-word phrases to verbally fluent– Module 3- Fluent speech- toys used– Module 4- Verbally fluent- adolescent/adult
ability to converse without prompts
ADOS
• Scoring:– “0” no evidence of abnormality- not
necessarily normal but not autistic– “1” Behavior is present- but not sufficiently
severe, frequent- occasional– “2” Behavior is present an meets specific
mandatory criteria– “3” Behavior so predominant it interferes
with the assessment- later coded as a “2” in algorithm
ADOS
Module 3 Activities:1. Construction Task2. Make-Believe Play/Joint Interaction
Play3. Demonstration Task4. Description of Picture5. Telling a Story from a Book6. Cartoons
ADOS
Module 3 Activities:• Questions- Emotions• Questions- Social Difficulties and
Annoyance• Questions- Friends and Marriage• Questions- Loneliness• Creating a Story

Questions and Answers