dental management of cadio & respi patients
TRANSCRIPT

Good Morning
3/28/2015
3:23 PM

DENTAL MANAGEMENT OF THE
MEDICALLY COMPROMISED PATIENT
PRESENTED BY:
Keshav Mehta
BDS 4th Year3/28/2015
3:23 PM

Systemic diseases include:
1. Cardiovascular diseases
2. Respiratory diseases
3. Liver diseases
4. Endocrine diseases
5. Renal diseases
6. Neurogenic diseases
7. Blood diseases
9. Pregnancy & breast feeding 3/28/2015
3:23 PM

CARDIOVASCULAR DISODERS
3/28/2015
3:23 PM

Patient Evaluation/Risk Assessment
• Review medical history and engage in direct discussion of relevant issues
with the patient.
• Identify all medications and drugs being taken, or supposed to be taken,
by the patient.
• Examine the patient for signs and symptoms of disease, as well as obtaining
vital signs.
• Review/obtain recent laboratory test results or images.
• Obtain a medical consultation if the patient has a poorly controlled or
undiagnosed problem, or if the patient’s health status is uncertain.3/28/2015
3:23 PM

Main signs & symptoms of C.V.S diseases
1. Chest pain
2. Dysnea
3. cyanosis
4. palpitation
5. Syncope
6. Edema of ankles
7. Cold pale extremities
8. Clubbing fingers
9. Easy fatigue3/28/2015
3:23 PM

ISCHEMIC HEART DISEASES
Mode of presentation of ischemic heart disease:
1. Angina pectoris
2. Myocardial infarction
3. Acute coronary insufficiency
4. Cardiac arrhythmia
5. Heart failure
6. Sudden death ( cardiac arrest, ventricular fibrillation )
7. Asymptomatic ( silent3/28/2015
3:23 PM

Risk assessment for the dental management of patients with ischemic heart disease
involves three determinants:
1. Severity of the disease
2. Type and magnitude of the dental procedure
3. Stability and cardiopulmonary reserve of the patient
3/28/2015
3:23 PM

Dental Management Considerations for Patients with Stable (Mild)
Angina or Past History of Myocardial Infarction (MI), Without
Ischemic Symptoms
Analgesics: Ensure adequate postoperative pain control.
Anesthesia: Avoid use of excessive amounts of epinephrine; limit to two carpules of
1:100,000 epinephrine at a time (within 30-45 minutes); greater quantities may be
tolerated well clinically but with increasing risk.
. Anxiety: Use stress reduction protocol . Consider the use of preoperative oral sedation
1 hour before procedure, as well as using N2O-O2 inhalational sedation intraoperatively.
3/28/2015
3:23 PM

Bleeding:If patient is taking aspirin or other antiplatelet medication,
anticipate some excessive bleeding, but modification of drug regimen is not
required.
Chair position: Ensure a comfortable chair position and avoid rapid
position changes.
Drugs: The use of excessive amounts of epinephrine with nonselective beta
blockers can potentially cause a spike in blood pressure, but this is unlikely
and appears to be dose-dependent; avoid the use of epinephrine
impregnated retraction cord. 3/28/2015
3:23 PM

Equipment: Consider taking preoperative vital signs and the use of a pulse oximeter if
oral sedation is used, or if the patient becomes symptomatic.
Emergencies: Precipitation of an angina attack, MI, arrhythmia, or cardiac arrest is
possible. Have nitroglycerin readily available as well as oxygen. Be prepared to
perform CPR .
Follow-up: Ensure that patient is maintaining regular follow-up visits with physician
3/28/2015
3:23 PM

3/28/2015
3:23 PM

Heart Failure
It is the pathophysiological process in which the heart as a pump is unable to meet
the metabolic requirements of the tissue for oxygen and substrates despite the
venous return to heart is either normal or increased.
It is Clinical syndrome … can result from any structural or functional cardiac
disorder that impairs ability of ventricle to fill with or eject blood.
3/28/2015
3:23 PM

Dental Management Considerations in Patients with Heart Failure (HF)
Antibiotics: Patients with HF may be more susceptible to infection (leukopenia), but
usually this is not a problem. There is no need for antibiotic prophylaxis unless the
patient has a prosthetic heart valve or another cardiac condition.
Anesthesia: It is very important to achieve and maintain excellent anesthesia in
order to reduce stress and prevent cardiac crisis. Use of epinephrine (1 :100,000) at a
dose of no more than 2 carpules in local anesthetics generally causes no problems,
but patients should be monitored closely.
3/28/2015
3:23 PM

Anxiety Patients: with untreated or poorly controlled HF may appear very anxious and
stressed and are at risk for cardiac crisis. Use of special anxiety/stress reduction
techniques.
Chair position: Positioning usually is not a problem if the patient is under good medical
management;
however, a patient who is becoming hypotensive and syncopal from cardiac stress and
pulmonary congestion may not tolerate the supine position.
Consultation: Once the patient is under good medical management, the dental treatment
plan can
be implemented without changes. Initially, however, consultation with the patient’s
physician to establish the level of control is recommended as part of the management
program.
3/28/2015
3:23 PM

3/28/2015
3:23 PM
Devices: Dental patients with a diagnosis of HF may have pacemakers, implanted
defibrillators, or prosthetic valves, in which case published guidelines should be
followed.
Drugs: Patients with HF typically are on many medications. The dentist should be
aware of potential side effects and interactions. The use of epinephrine or other
pressor amines must be avoided. Digitalis toxicity may present a problem, so
prevention should be exercised in treating those patients.

HYPERTENSIVE DISEASES
Hypertension is considered to be the elevation of the blood pressure
greater than 140/90 mm of mercury
Uncontrolled hypertension can have the following surgical and anesthetic
complications:
1. It reflects on the cardiac status of the patient, thereby increasing the
anesthetic risk to the patient.
2. It causes excessive bleeding from the operation site, thereby
complicating the surgical procedure, as well as significant blood loss for
the patient 3/28/2015
3:23 PM

Preoperative Investigations
Chest radiograph—posteroanterior view for detecting
cardiac enlargement
ECG
USG of the kidneys
Ophthalmic evaluation for papilledema and retinal
hemorrhage
Renal function tests (blood urea nitrogen, serum creatinine and serum
electrolyte).3/28/2015
3:23 PM

Preoperative Medication and Management
The patient’s blood pressure should be monitored and controlled
within the normal permissible limits, prior to the surgical
procedure.
If the patient is on antihypertensives, the morning dose of
medication prior to surgery must be given with sips of water.
3/28/2015
3:23 PM

Intra and Postoperative Management
1. The blood pressure should be monitored continuously intra and
postoperatively.
2. The patient’s cardiac status should also be monitored on the ECG
machine and on the pulse oximeter.
3. Antihypertensives must be continued intra- and postoperatively.
4. If the patient is on diuretics, the patient must be supplemented
postoperatively with intravenous potassium supplements.
5. If the procedure is performed under local anesthesia, then local anesthetic
without adrenaline or bupivacaine, which does not have any significant
effect on the cardiac status is to be used.3/28/2015
3:23 PM

Prevention of problem Detection of patients with hypertension and referral to a physician if poorly controlled
or uncontrolled. Defer elective dental treatment if blood pressure (BP) is ≥180/110 mm
Hg.
• For patients who are being treated for hypertension, consider the following:
• Take measures to reduce stress and anxiety.
• Avoid the use of erythromycin or clarithromycin in patients taking a calcium channel
blocker.
• Avoid the long-term use of nonsteroidal antiinflammatory drugs (NSAIDs).
• Provide oral sedative premedication and/or inhalation sedation.
• Provide local anesthesia of excellent quality.
• For patients who are taking a nonselective beta blocker, limit epinephrine to ≤2
cartridges of 1 : 100,000 epinephrine.
• Avoid epinephrine-containing gingival retraction cord.
• For patients with upper-level stage 2 hypertension, consider intraoperative monitoring
of BP, and terminate appointment if BP reaches 180/110.
• Make slow changes in chair position to avoid orthostatic hypotension. 3/28/2015
3:23 PM

PROPHYLACTIC ANTIBIOTIC
REGIMEN FOR CARDIAC PT.
1. Under L.A
a) Adults---- 2gm Amoxicillin or 2gm Ampicillin
(1 hour before treatment orally) OR
(1/2 hour ,,, ,,,,,,,,,,, injection)
B) Children----- 50 mg per Kg Amoxicillin or
Ampicillin
3/28/2015
3:23 PM

IF PATIENT IS ALLERGIC:
Adult --------- Clindamycin 600 mg OR
Azathromycin 500 mg OR
Cephazolin 1 gm
(1 hour before tt. Orally)
( ½ ,,, ,,,, ,,, injection)
Child --------- Clindamycin 20 mg per Kg.
Azathromycin 15 mg per Kg.
3/28/2015
3:23 PM

2. Under G.A
a) Adults----- 1gm Amoxicillin I.V at induction.
OR 3gm Amoxicillin orally 4 hours before induction followed by
3gm Amoxicillin immediately after recovery.
OR 300mg Clindamycin I.M ½ hour before induction.
OR 300mg Clindamycin I/V at induction
b) Children ------ (5–10 years)1/2 adult
. (< 5 years) 1/4 adult
3/28/2015
3:23 PM

3/28/2015
3:23 PM

RESPIRATORY
DISORDERS
3/28/2015
3:23 PM

RESPIRATORY DISORDERS
Respiratory diseases can be categorized into obstructive and infiltrative
pulmonary diseases. Obstructive pulmonary diseases include, chronic
obstructive pulmonary conditions like asthma, chronic bronchitis,
pneumothorax and emphysema. Infiltrative diseases are inclusive of
diseases that cause inflammatory changes in the alveolar walls. Any
respiratory disease is first characterized by dyspnea.3/28/2015
3:23 PM

Common symptoms:
1. cough.
2. wheezing.
3. cyanosis.
4. finger clubbing
AVOID
1. General anesthesia: leads to hypoxia .
2. Analgesics & narcotics: leads to respiratory depressants.
3/28/2015
3:23 PM
BRONCHIAL ASTHMA
It is due to bronchospasm or hyperirritability of the
tracheo_bronchial tree.
Patient is treated by:
1. Corticosteroids inhalators.
2. Bronchodilator.
3. Beta adrenergic stimulator.
3/28/2015
3:23 PM

Preoperative Investigations
1. Chest radiograph—posteroanterior view
2. Pulmonary function tests
3. Blood investigations like arterial blood gases
4. Sputum AFB/Culture
5. Bronchoscopy, if required.
The patient should be counseled to discontinue beedi/cigarette smoking
prior to the procedure. Any acute infection should be treated by antibiotics.
The patient should be on bronchodilators pre, intra, and postoperatively.
The patient must carry inhaler for use in case of an emergency.3/28/2015
3:23 PM
Dental Management
Considerations in Patients with Asthma
Patient Evaluation/Risk Assessment
• Evaluate and identify asthma as a medically confirmed or likely diagnosis along with
its severity and type if present.
• Obtain medical consultation if asthma is poorly controlled (as indicated by wheezing or
coughing, or a recent hospitalization) or is undiagnosed, or if the diagnosis is uncertain.
Ecourage current smokers to stop smoking.
3/28/2015
3:23 PM

Antibiotics: Avoid erythromycin, macrolide antibiotics, and ciprofloxacin in patients
taking theophylline.
Anesthesia: The clinicians may elect to avoid solutions containing epinephrine or
levonordefrin because of sulfite preservative.
Anxiety: Provide stress-free environment through establishment of rapport and openness
to reduce risk of anxiety-induced asthma attack. If sedation is required, use of nitrous
oxide– oxygen inhalation sedation and/or small doses of oral diazepam is recommended.
3/28/2015
3:23 PM

Allergy: Asthmatics with nasal polyps are increased risk for allergy to aspirin.
Avoid aspirin use.
Blood pressure: Monitor blood pressure during asthma attack to observe for the
development of status asthmaticus
Chair position: Semisupine or upright chair position for treatment may be better
tolerated.
Devices: Instruct patient to bring current medication inhaler to every appointment;
use prophylactically in moderate to severe disease. Obtain spirometry reading to
determine level of control. Use pulse oximetry to monitor oxygen saturation during
dental procedure.
3/28/2015
3:23 PM
Drugs: Avoid precipitating odorants and drugs (aspirin). Avoid use of barbiturates
and narcotics, which can depress respiration and release histamine, respectively.
Supplemental steroids are unlikely to be needed in routine dental care; provide usual
morning corticosteroid dose the morning
of surgical procedures.
Equipment: Use low-flow (2 to 3 L/minute) supplemental O2 when oxygen
saturation drops below 95%; it also may become necessary when oxygen saturation
drops below 91%.
3/28/2015
3:23 PM

Emergencies: Recognize signs and symptoms of a severe or worsening asthma
attack: inability to finish sentences with one breath, ineffectiveness of
bronchodilators to relieve dyspnea, recent drop in FEV1 as determined by
spirometry, tachypnea with respiratory rate of 25 breaths/minute or
more, tachycardia with heart rate of 110 beats/ minute or paradoxical pulse.
Follow-up: Ensure that patient is receiving adequate medical follow-up care
on a routine basis.
3/28/2015
3:23 PM
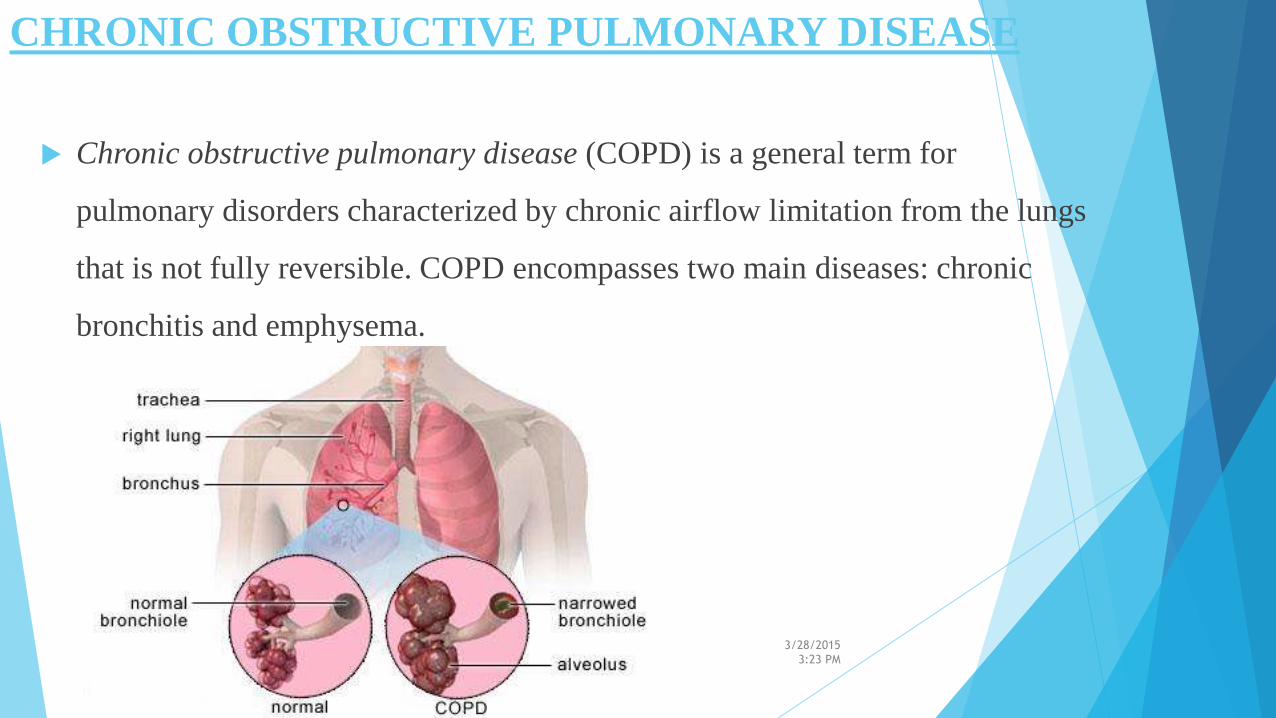
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Chronic obstructive pulmonary disease (COPD) is a general term for
pulmonary disorders characterized by chronic airflow limitation from the lungs
that is not fully reversible. COPD encompasses two main diseases: chronic
bronchitis and emphysema.
3/28/2015
3:23 PM
Patient Evaluation/Risk Assessment
• Evaluate and determine whether COPD is present.
• Obtain medical consultation if the condition is poorly controlled
(as manifested by dyspnea, coughing, or frequent upper respiratory infections)
or undiagnosed, or if the diagnosis is uncertain.
Review history and clinical findings for concurrent heart disease.
• Encourage current smokers to stop smoking.
Dental Management
Considerations in Patients with Chronic Obstructive Pulmonary Disease (COPD)
3/28/2015
3:23 PM
Antibiotics: Avoid erythromycin, macrolide antibiotics, and ciprofloxacin in patients
taking theophylline. In patient who has received courses of antibiotics for upper
respiratory infections, oral and lung flora may include antibioticresistant bacteria.
Anesthesia: Local anesthesia can be used without change in technique. Avoid
outpatient general anesthesia.
Anxiety: Avoid nitrous oxide–oxygen inhalation sedation in patients with severe
(stage 3 or worse) COPD. Consider low-dose oral diazepam or another
benzodiazepine, although these agents may cause oral dryness.
.3/28/2015
3:23 PM
Blood pressure: Patients with COPD can have cardiovascular comorbidity. Assess
blood pressure.
Chair position: Semisupine or upright chair position may be better for treatment in
these patients.
Devices : Avoid use of rubber dam in patients with severe disease. Use pulse
oximetry to monitor
oxygen saturation. Spirometry readings are helpful in determining level of control.
3/28/2015
3:23 PM

Drugs: Avoid use of barbiturates and narcotics, which can depress respiration.
Avoid use of antihistamines and anticholinergic drugs because they can further
dry mucosal secretions. Supplemental steroids are unlikely to be needed to
perform routine dental care; the usual morning corticosteroid dose should be
taken on the day of surgical procedures.
3/28/2015
3:23 PM
Equipment: Monitor oxygen saturation with pulse oximeter during sedation and
invasive procedures. Use low-flow (2 to 3 L/minute) supplemental O2 when oxygen
saturation drops below 95%; it may become necessary when oxygen saturation drops
below 91%.
Follow-up: At each follow-up appointment, encourage patient to quit smoking, and
examine oral
cavity for lesions that may be related to smoking. Avoid treatment if upper respiratory
infection is present.
3/28/2015
3:23 PM
References
3/28/2015
3:23 PM

3/28/2015
3:23 PM
HAVE A NICE DAY!!!