department of public protection ems division citizen’s academy presentation 2015
TRANSCRIPT
Department of Department of
Public Public ProtectionProtection
EMS DIVISIONEMS DIVISIONCitizen’s Academy Citizen’s Academy Presentation 2015Presentation 2015

Introductions and WelcomeIntroductions and Welcome
Today’s Presentation:
Ambulance on Display (lunchtime) Who and What is “Volusia County EMS” EMS is MUCH More than a Fast Response
and Ride to the Hospital Emphasis on Quality and Clinical
Excellence Important changes/improvements to the
pre-hospital community health care system Why we do what we do.
3
Service BackgroundService Background
FDOH Licensed Primary Provider of Advanced Life Support FDOH Licensed Primary Provider of Advanced Life Support (ALS) level Emergency Ambulance Services for Volusia (ALS) level Emergency Ambulance Services for Volusia CountyCounty
Independent Emergency Medical Foundation (EVAC) Independent Emergency Medical Foundation (EVAC) incorporated October 1981, taking over county EMS incorporated October 1981, taking over county EMS responsibilities for Beacon Ambulance.responsibilities for Beacon Ambulance.
Fall 2011, EMF dissolved and EVAC transitioned into a Fall 2011, EMF dissolved and EVAC transitioned into a county division under Public Protectioncounty division under Public Protection
4
Service BackgroundService Background Serves a diverse population of 500,000 residents + transient Serves a diverse population of 500,000 residents + transient
population (contiguous populations, seasonal and tourists)population (contiguous populations, seasonal and tourists) 1100 1100 diversediverse square miles square miles
Urban to Ultra-RuralUrban to Ultra-Rural Significant Events (Speed & Bike Weeks, et al)Significant Events (Speed & Bike Weeks, et al) Staff of over 180 skilled EMS staffStaff of over 180 skilled EMS staff
Field care providersField care providers Support (ASTs)Support (ASTs) MaintenanceMaintenance Administrative/AccountingAdministrative/Accounting
Provides 24/7 ambulance coverage, high of 23 “peak time” Provides 24/7 ambulance coverage, high of 23 “peak time” units down to 11 at nightunits down to 11 at night
Emergency “911” and Hospital Interfacility TransportEmergency “911” and Hospital Interfacility Transport
5
Service BackgroundService Background
Vehicles drive approximately 1.5 million miles/year (road Vehicles drive approximately 1.5 million miles/year (road miles & engine hours)miles & engine hours)
Continuing medical education – over 4000 course hoursContinuing medical education – over 4000 course hours Division specific operational/clinical educationDivision specific operational/clinical education Collaborative training opportunities with local emergency Collaborative training opportunities with local emergency
response partners (fire, law enforcement, emergency response partners (fire, law enforcement, emergency management) management)
Anatomy & Physiology LabAnatomy & Physiology Lab HIGH PERFORMANCE EMS MODELHIGH PERFORMANCE EMS MODEL
6
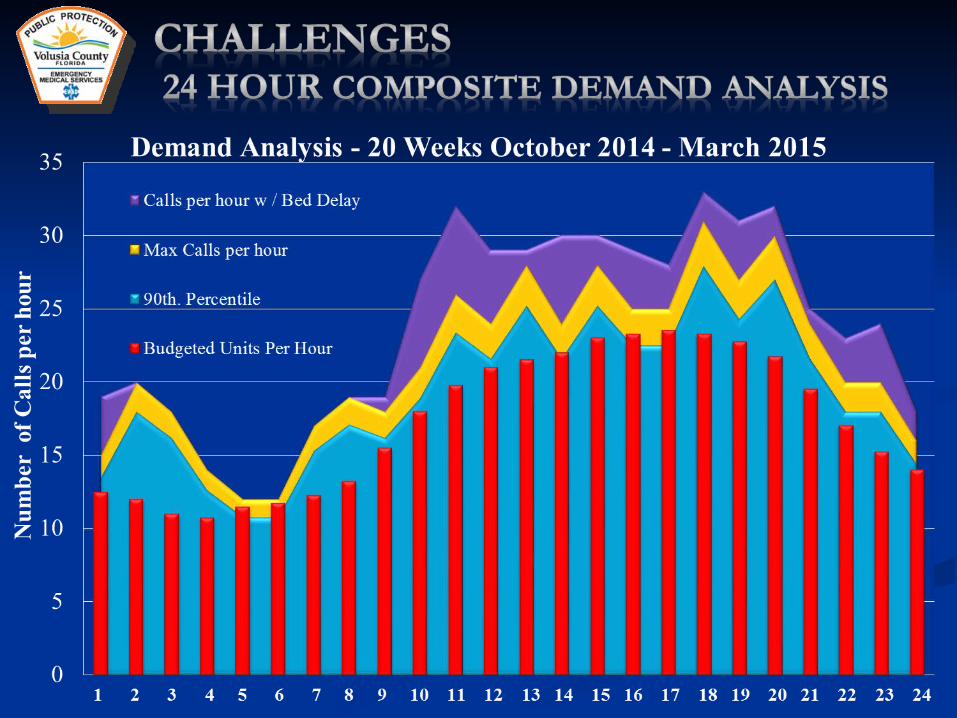
Ever Increasing Ever Increasing DemandDemand
•Over 85,000 Over 85,000 emergency callsemergency calls•50,000+ Patient 50,000+ Patient TransportsTransports•Linear increase in Linear increase in demand demand
• (3-5%/year)(3-5%/year)• Aging (sicker) Aging (sicker)
PopulationPopulation
7
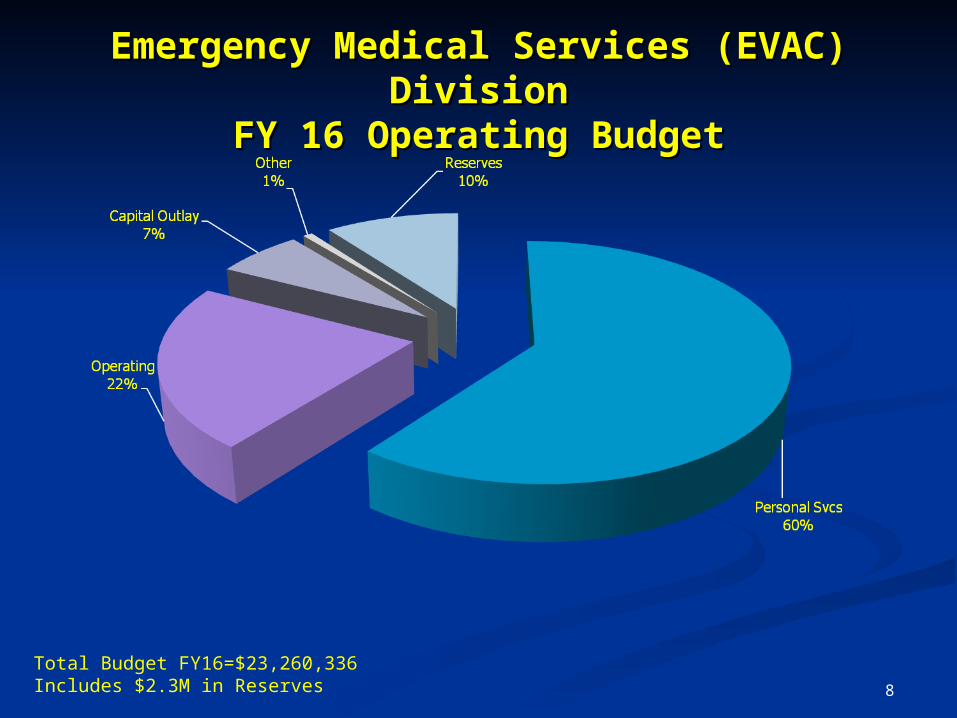
Emergency Medical Services (EVAC) DivisionEmergency Medical Services (EVAC) DivisionFY 16 Operating BudgetFY 16 Operating Budget
8
Total Budget FY16=$23,260,336Includes $2.3M in Reserves

Emergency Medical Services Division (EVAC)Emergency Medical Services Division (EVAC)FY 16 Operating RevenueFY 16 Operating Revenue
9
Total Revenue = $24,509,566Includes Fund Balance of $3,339,389
Medical Reimbursement Medical Reimbursement BasicsBasics
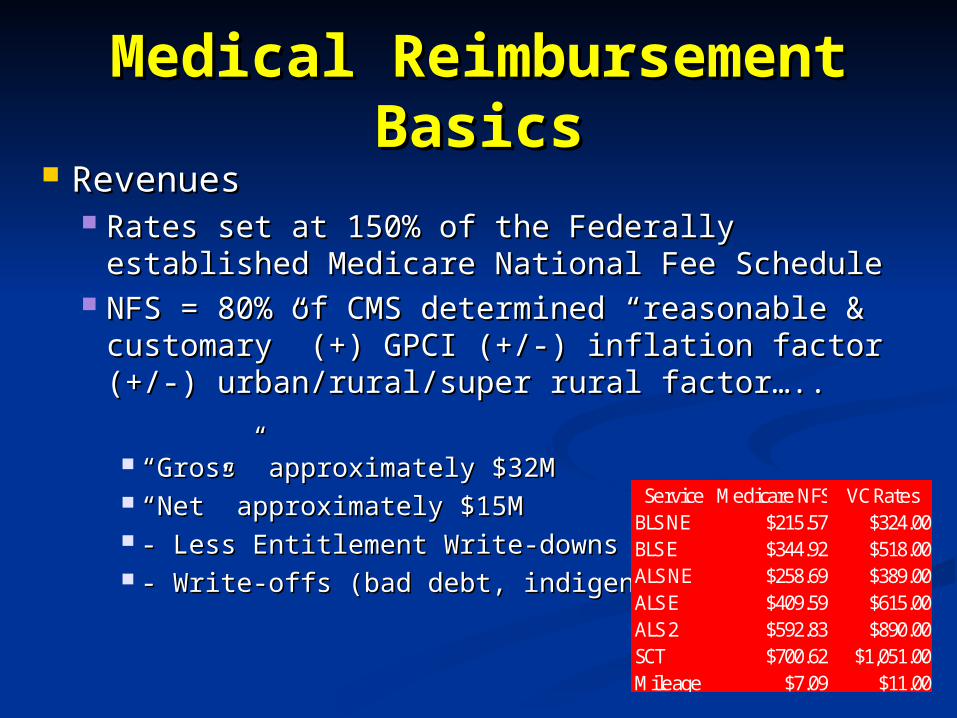
RevenuesRevenues Rates set at 150% of the Federally established Rates set at 150% of the Federally established
Medicare National Fee ScheduleMedicare National Fee Schedule NFS = 80% of CMS determined “reasonable & NFS = 80% of CMS determined “reasonable &
customary” (+) GPCI (+/-) inflation factor (+/-) customary” (+) GPCI (+/-) inflation factor (+/-) urban/rural/super rural factor…..urban/rural/super rural factor…..
““Gross” approximately $32MGross” approximately $32M ““Net” approximately $15MNet” approximately $15M - Less Entitlement Write-downs- Less Entitlement Write-downs - Write-offs (bad debt, indigence, etc)- Write-offs (bad debt, indigence, etc)
Service Medicare NFS VC RatesBLS NE $215.57 $324.00BLS E $344.92 $518.00ALS NE $258.69 $389.00ALS E $409.59 $615.00ALS 2 $592.83 $890.00SCT $700.62 $1,051.00Mileage $7.09 $11.00
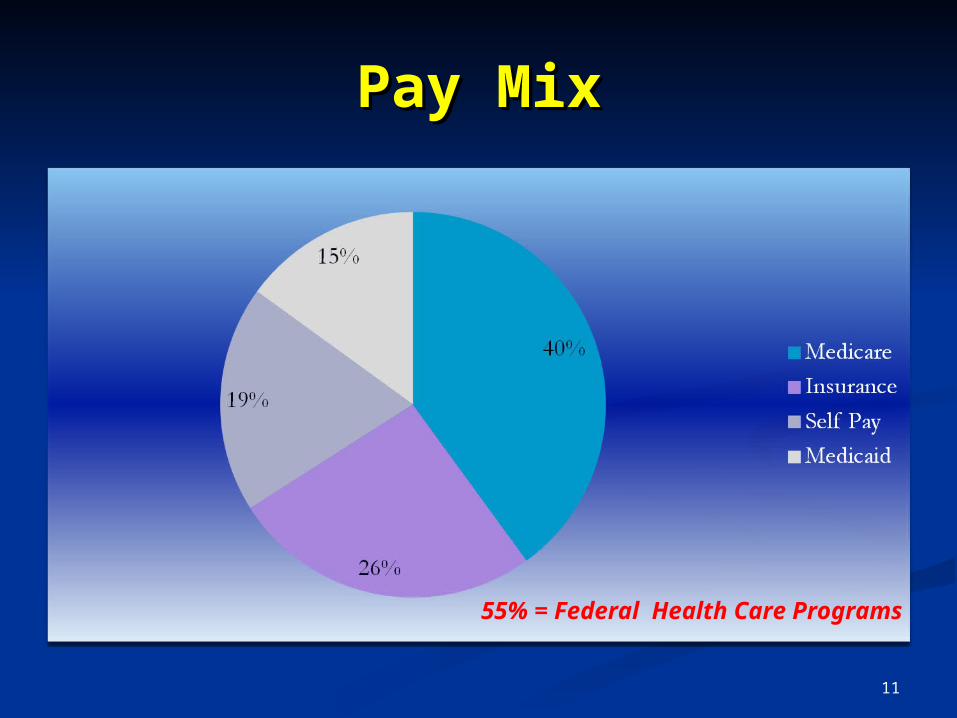
Pay MixPay Mix
55% = Federal Health Care Programs
11
High Performance EMS High Performance EMS ??
• Traditional DeploymentTraditional Deployment• Station BasedStation Based• Geographic coverage (“covering Geographic coverage (“covering
dirt”)dirt”)•High PerformanceHigh Performance
• Uses Historical Statistical Uses Historical Statistical ModelingModeling
• Predicts/Identifies emergency call Predicts/Identifies emergency call location probabilitieslocation probabilities
• Stages vehicles to meet predicted Stages vehicles to meet predicted demand (intersection staging)demand (intersection staging)
• Maximizes deployment and Maximizes deployment and efficiencyefficiency
12
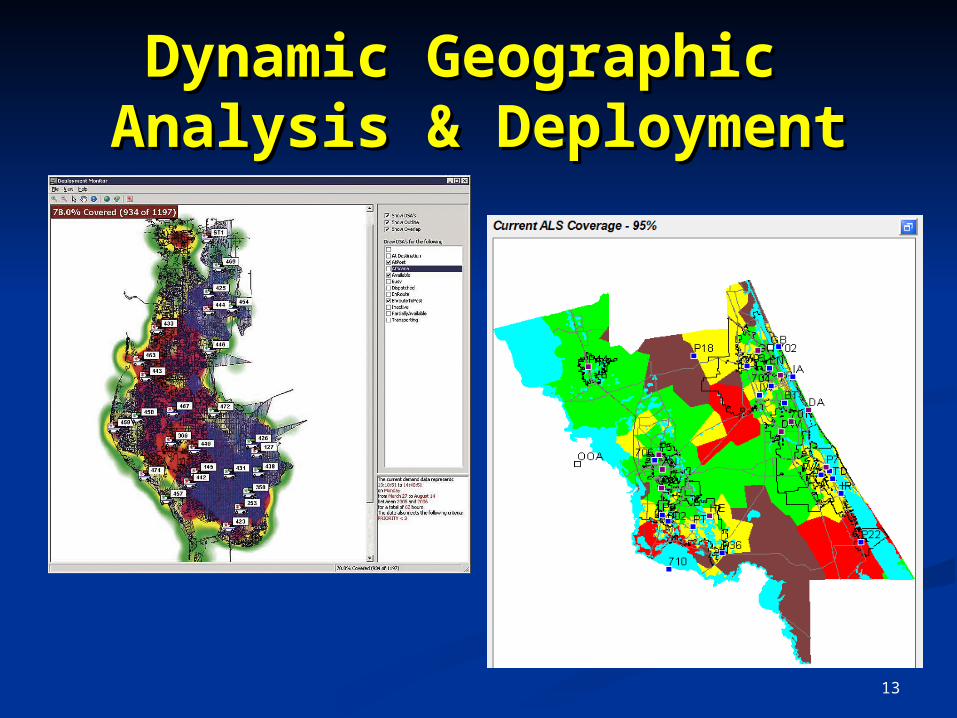
Dynamic Geographic Dynamic Geographic Analysis & DeploymentAnalysis & Deployment
13
EMS is….EMS is…. NOTNOT just a fast ride/easy access to the hospital. just a fast ride/easy access to the hospital.
The clinical skills and treatment provided by the The clinical skills and treatment provided by the Paramedics and EMTs, NOT the vehicle!Paramedics and EMTs, NOT the vehicle!
Clinically/Operationally focused on quality HEALTH Clinically/Operationally focused on quality HEALTH CARECARE
Fast Becoming Recognized as an Fast Becoming Recognized as an integral partnerintegral partner of of the total health care delivery system …the total health care delivery system …BEGINNING BEGINNING WITH THE INITIAL ACCESS POINT.WITH THE INITIAL ACCESS POINT.
Often stressed due to inappropriate utilization, Often stressed due to inappropriate utilization, sometimes not immediately available for true sometimes not immediately available for true emergenciesemergencies
15
EMS Includes….EMS Includes…. The PublicThe Public 911 Call Takers & Dispatchers911 Call Takers & Dispatchers Fire first responseFire first response Augmented Public Safety AgenciesAugmented Public Safety Agencies
Law enforcementLaw enforcement Beach patrolBeach patrol
Aeromedical TransportationAeromedical Transportation EMSEMS Local Health SystemsLocal Health Systems
16
Basic v Advanced Life Basic v Advanced Life Support Support
•In simple terms In simple terms - Determined - Determined by the level of education and by the level of education and capabilities of the respondercapabilities of the responder•Emergency Medical Emergency Medical TechnicianTechnician
• ““Associate” degree level Associate” degree level educationeducation
• Basic ‘noninvasive’ skills -Basic ‘noninvasive’ skills -• CPRCPR• Wound careWound care• SplintingSplinting
17
Basic v Advanced Life Basic v Advanced Life Support Support
•ParamedicsParamedics• ““Bachelors Degree”Bachelors Degree”• Higher skill level, “Invasive”Higher skill level, “Invasive”
• Medications/Fluid Medications/Fluid administrationadministration
• Advanced airway skillsAdvanced airway skills• 12 lead ECG Interpretation12 lead ECG Interpretation
18
NOT THIS!NOT THIS!
19
Clinical & Operational Clinical & Operational ExcellenceExcellence
Medical Direction and ControlMedical Direction and Control EMS does not function without physician oversightEMS does not function without physician oversight Sets treatment policies and proceduresSets treatment policies and procedures Ensures clinician capabilityEnsures clinician capability Monitors compliance and careMonitors compliance and care
20
Future VisionFuture Vision Not all 911 Calls are Emergencies!Not all 911 Calls are Emergencies!
Emergencies are largely Self determined/defined by the caller.Emergencies are largely Self determined/defined by the caller.
Continued Concentration on Clinical & Continued Concentration on Clinical & Operational Quality Practices & ExcellenceOperational Quality Practices & Excellence
Clinical Integration from 911 to Hospital DischargeClinical Integration from 911 to Hospital Discharge ““Right Care, Right Time, Right Place” Right Care, Right Time, Right Place” Develop Advanced Practice/Community Health Develop Advanced Practice/Community Health
Paramedic CliniciansParamedic Clinicians Determine correct clinical pathwayDetermine correct clinical pathway Concentrate on True EmergenciesConcentrate on True Emergencies
21
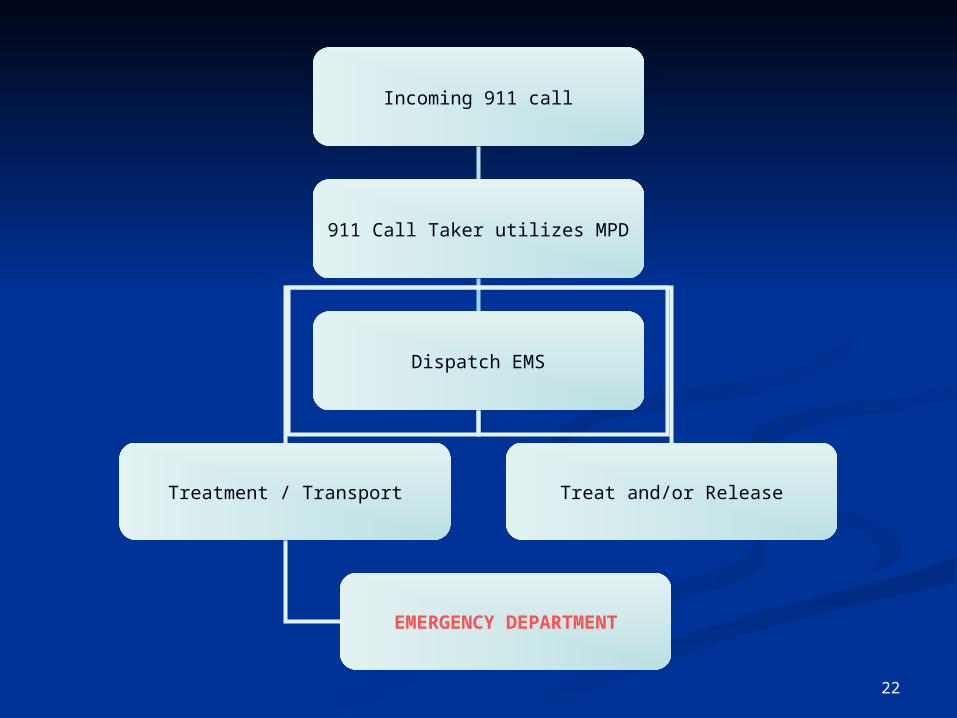
Incoming 911 call
911 Call Taker utilizes MPD
Dispatch EMS
Treatment / Transport
EMERGENCY DEPARTMENT
Treat and/or Release
22
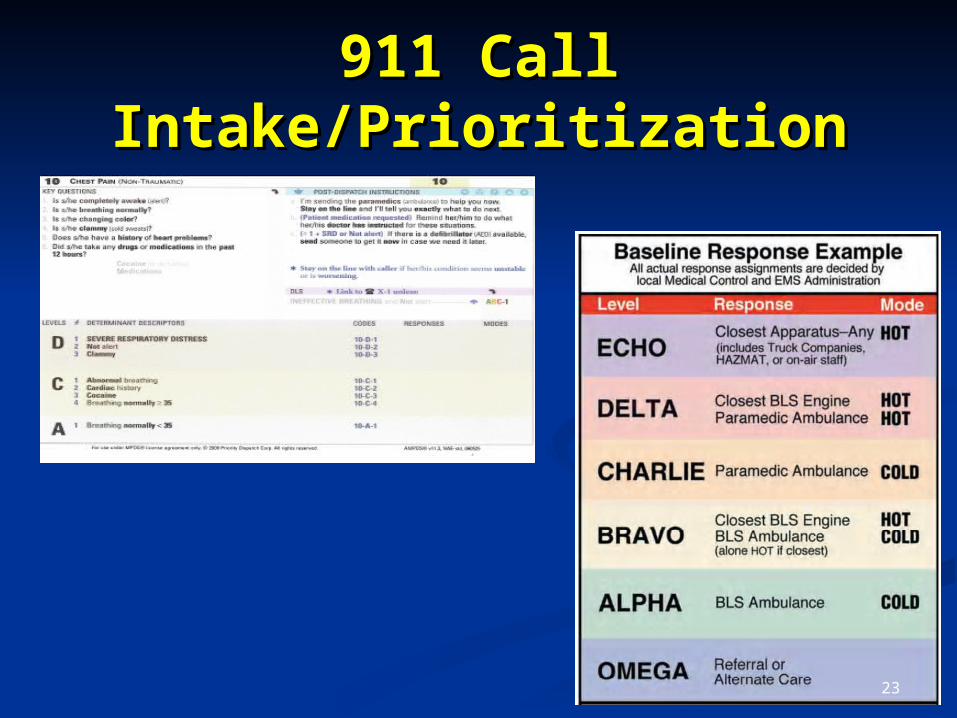
911 Call 911 Call Intake/PrioritizationIntake/Prioritization
23
VCEMS COMMUNITY HEALTH INITIATIVEVCEMS COMMUNITY HEALTH INITIATIVE
“NURSE TRIAGE”“NURSE TRIAGE”
Defining actual need:Defining actual need: Secondary supplemental RN-based telephone triage Secondary supplemental RN-based telephone triage
process for low acuity calls for assistanceprocess for low acuity calls for assistance Not all calls to 911 are emergencies!Not all calls to 911 are emergencies! Provides the Provides the right care, right place, right timeright care, right place, right time…… Collaboration with local Hospital Systems & Collaboration with local Hospital Systems &
coalitionscoalitions Provides a solution which May NOT necessarily Provides a solution which May NOT necessarily
result in a response by EMSresult in a response by EMS
24
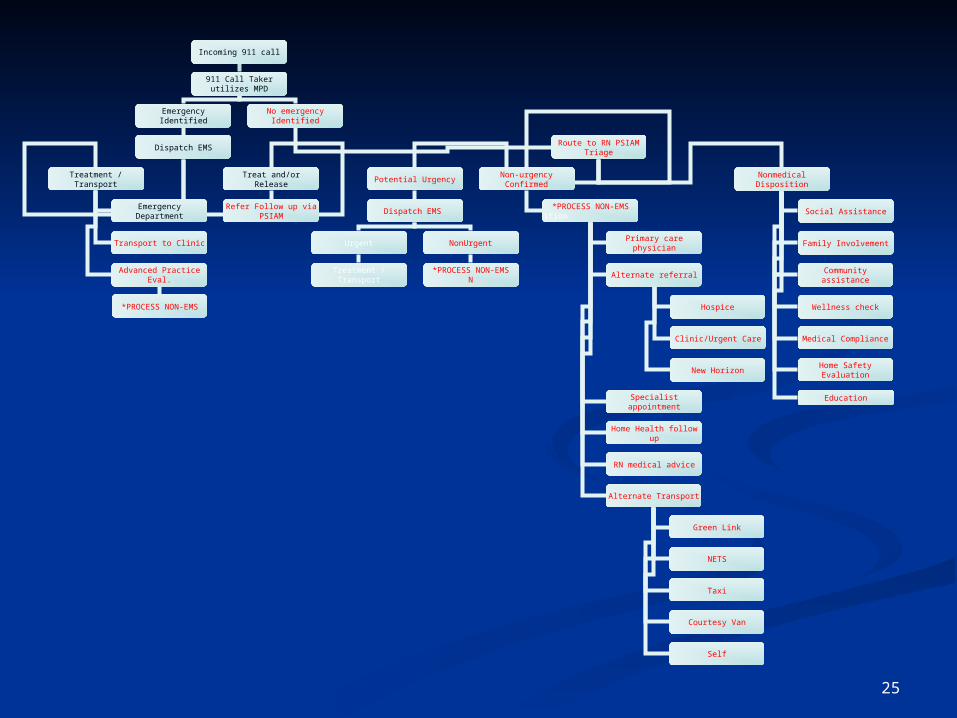
Incoming 911 call
911 Call Taker utilizes MPD
Emergency Identified No emergency Identified
Route to RN PSIAM TriageDispatch EMS
Non-urgency ConfirmedPotential Urgency
Dispatch EMS
Urgent NonUrgent
Treatment / Transport*PROCESS NON-EMS
N
*PROCESS NON-EMSition
Primary care physician
Alternate referral
Specialist appointment
Home Health follow up
RN medical advice
Treatment / Transport
Emergency Department
Treat and/or Release
Transport to Clinic
Advanced Practice Eval.
Refer Follow up via PSIAM
*PROCESS NON-EMS
Alternate Transport
Hospice
Clinic/Urgent Care
Nonmedical Disposition
Social Assistance
Family Involvement
Community assistance
Wellness check
New Horizon
Medical Compliance
Home Safety Evaluation
Green Link
NETS
Taxi
Courtesy Van
Self
Education
25
The Emerging EMSThe Emerging EMSand National Health Care and National Health Care
ParadigmParadigm Elements of Affordable Care Act (“Obamacare”) here Elements of Affordable Care Act (“Obamacare”) here
to stay regardless of political outcometo stay regardless of political outcome Encourages “Best Practice” (Quality Practice)Encourages “Best Practice” (Quality Practice) EMS’ Verified/Recognized Impact on Clinical EMS’ Verified/Recognized Impact on Clinical
Outcomes Outcomes Mutual development of alternate clinical pathways Mutual development of alternate clinical pathways
and destinationsand destinations Enhanced Practice/Community Health ParamedicsEnhanced Practice/Community Health Paramedics Regardless of Acuity, Provide the Correct Level of Regardless of Acuity, Provide the Correct Level of
Care.Care.
26

Technology
27

28
If you are reading this –THANK YOU!
Citizen’s Academy Citizen’s Academy Presentation 2015Presentation 2015