department of urology school of medicine chairman: prof ... · university of messina prostatitis...
TRANSCRIPT
UNIVERSITY OF MESSINA
Prostatitis and BPH:myth or real evolution ?
Department of Urology
Chairman: Prof. Giuseppe Morgia
School of Medicine

Introduction
•What is the BPH ?
•What is the prostatitis ?

Introduction
Recent studies assessed a strong relationship between Prostatitis and Benign Prostatic Hyperplasia (BPH)
Flogosis could play a relevant role in the prostatic diseases progression
A causative role for inflammation in the pathogenesis of BPH was firstproposed by Moore RA in 1937 but for the major part of the 20th
century the “embryonal reawakening theory” dominated the field ofBPH
Today investigations ofexperimentally induced
prostatitis in mice and ratssuggest that BPH is an
immune-mediated inflammatorydisease

BPH/PROSTATITISTraditionally, prostatitis has been considered a condition which affects
younger men but little attention has been given to the associationBPH/Prostatitis despite the high prevalence of both condition in ageing men
Collins MM et al J Urol 2002 7465 pts with BPH of which 38,7% + prostatitis
5053 pts with prostatitis of which 57,2% + BPH
Nickel reported that approximately 8% of men over 50 years suffer withsome mild prostatitis like symptoms vs 11% of younger men.
31681 pts

Almost all surgery-derived BPH specimens show inflammatoryinfiltrates at histologic examination
BPH/PROSTATITIS
Even if there is a lack of association of histological prostatitis andclinical prostatitis,the importance of inflammation, for years was
undervalued
Inflammatoryinfiltrates were
always consideredof no clinical
relevance
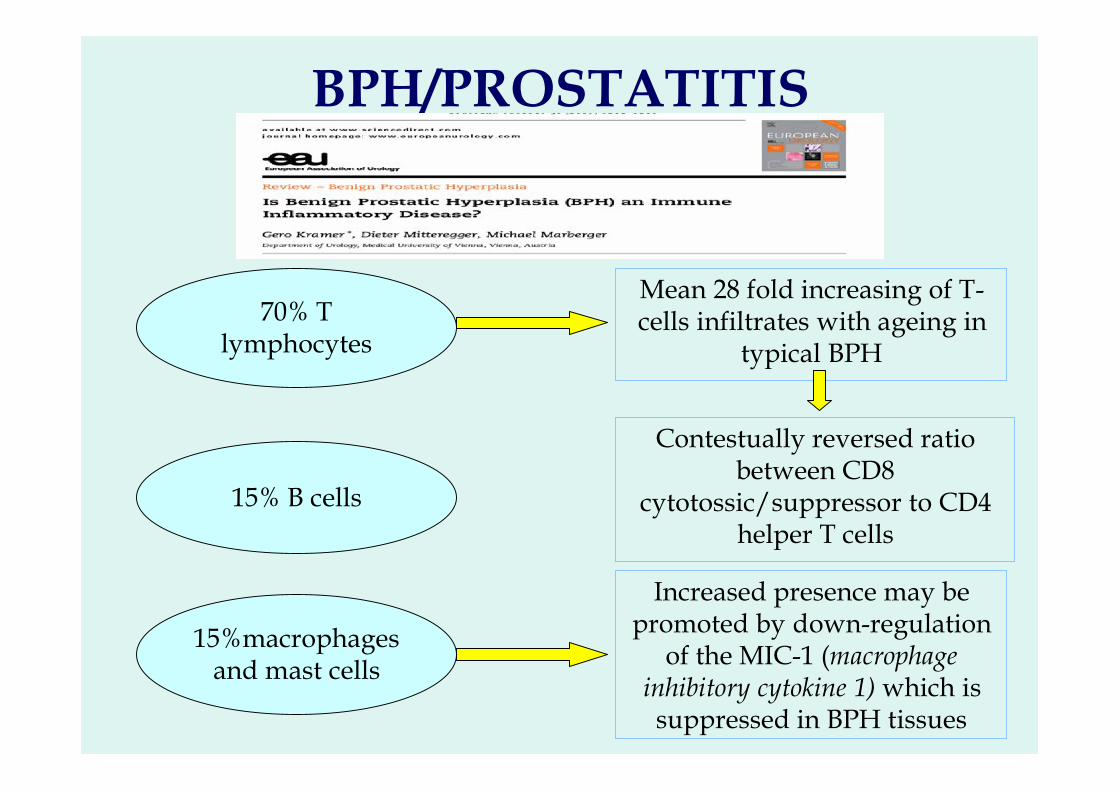
BPH/PROSTATITIS
70% Tlymphocytes
15% B cells
15%macrophagesand mast cells
Mean 28 fold increasing of T-cells infiltrates with ageing in
typical BPH
Contestually reversed ratiobetween CD8
cytotossic/suppressor to CD4helper T cells
Increased presence may bepromoted by down-regulation
of the MIC-1 (macrophageinhibitory cytokine 1) which issuppressed in BPH tissues

Agenda• Association of inflammation and
clinical BPH• Role of inflammation in the
pathogenesis of BPH• Flogosis and BPH progression• Flogosis and BPH treatment• Biomarkers of inflammation for BPH

57%
43%
Association of inflammation andclinical BPH
This relationship has been observed by Di Silverio et al. in a studyconducted over 3942 histologic specimens of pts affected by BPH
30%chronic flogosis
Di Silverio Eur Urol 2003
Flogosis No Flogosis

REDUCEREduction by DUtasteride of prostate Cancer Events
Evaluation of thebaseline relationshipbetween histologic
prostate inflammationand LUTS
Histologic flogosiswas detected in 78%
of men
Weak but statisticallysignificant correlation with
IPSS
It was performed an additionalinvestigation from the actually
available data

REDUCE: 5,597 pz
Conferma istopatologica di flogosi nel 94.5%• Cronica: 78%• Acuta: 16.5% (grado medio)
Nessuna correlazione tra:Stato infiammatorio acuto e CPSI score
Correlazione statisticamente significativa:Stato infiammatorio cronico e CPSI score
Nickel – J Urol 2007
REDUCEREduction by DUtasteride of prostate Cancer Events

Classificazione isto-patologica della flogosi prostatica
Aggregati di cell. Infiammatorie con distruzione tissutale oformazione di noduli/follicoli linfatici (>500)
3 o Severo
Aggregati di cell. Infiammatorie senza distruzione tissutale oformazione di noduli/follicoli linfatici (100-500)
2 o ModeratoCellule infiammatorie isolate (<100)1 o Modesto
Descrizione morfologica (densità delle cell.Infiammatorie/mm2)
Grado>50%Diffusa10-50%Multifocale<10%FocalePercentuale di tessuto coinvolta dagli infiltrati infiammatoriEstensioneInfiltrato inf. nello stroma e comunque ad una distanza>50 µmStromaleInfiltrato inf. nello stroma attorno ai dotti o acini (distanza<50µm)Perighiandolare
Infiltrato infiammatorio all’interno dei dotti/epitelio ghiandolare e/odel lume
Ghiandolare
Pattern istologicoLocalizzazioneanatomica
Irani et al – J Urol 1997Consensus Conference – Nickel 2001

Histologic evaluation was performed using a classification proposed by acentral laboratory (Bostwick Laboratories Richmond, VA, USA)
Graded average acute and chronic inflammation based on a 4-point scale
Scale based on average cell density andextent of tissue involvement
I II III IV
REDUCEREduction by DUtasteride of prostate Cancer Events

Delongchamps et al, J Urol 2008
Valutazione istopatologica prostatica su 167 autopsie:
BPH: 56%PC: 29%Flogosi: 67.6% (A 4%, C 53%, A+C 11%)
BPH + FC: 75% No BPH + FC: 50% (p<0.01)PC + FC: 55% No PC + FC: 58% (p>0.1)Nessuna correlazione tra FA e BPH/PC

BPH
+
C
FB
PH
K +
C
FK
113 (67,6%)
cronic
55%
75%
Delongchamps et al, J Urol 2008
A
C+A

• DRE• TRUS con ecocolor doppler
– Scintigrafia con leuco In111 (non praticabileroutinariamente)
Esistono segni clinici e parametri dilaboratorio che possono aiutare
l’individuazione dell’infiammazione ?
Esami clinici

• Esame urine e liquido seminale– Dosaggio di citochine e chemichine (IL-1,IL-6,
IL-8, TNF α (non praticabili routinariamente)– Dosaggio PGE-2, CRFR2 (nel tessuto) (non
praticabili routinariamente)
Esistono segni clinici e parametri dilaboratorio che possono aiutare
l’individuazione dell’infiammazione ?
Esami di laboratorio

Role of inflammation in thepathogenesis of BPH
BPH nodules are frequently composed by chronic inflammatoryinfiltrates mainly represented by activated T-cells and macrophages
Why the leucocyte population increases in BPH ?
Several hypotheses have been generated based onrecent basic research

Role of inflammation in thepathogenesis of BPH
Kramer G. Eur Urol 2007
After a probably primary injury it occurs an age dependent weakening of apostulated population of suppressor cells that actively supresses the recognitionof prostatic agents which leads to gradual infiltration of the prostate bylymphocytes and subsequent cascade of events that leads to BPH

Flogosis
Increeased leucocyte population
IL-2; IL-6; IL-8; IL-17; IFN-γ
Perpetuate chronic immune response
autoimmuneloop
Paracrineloop
Cox-2
Fibromuscolar Growth
Role of inflammation in thepathogenesis of BPH

Increased production ofIL-6; IL-8; IL-17
Immigration of T-cells into the area
Surrounding cells become targets and are Killed
Vacant spaces replaced by fibromuscolar nodes
Role of inflammation in thepathogenesis of BPH

• Le cellule T CD4+ attivate secernono IL-17, una citochinacapace di stimolare le cellule epiteliali, endoteliali efibroblastiche di produrre diverse molecole pro-infiammatoriecome IL-1β, TNF-a, IL-8 e COX-2 (Steiner et al, Prostate2003).
• Questi autori hanno dimostrato che il tessuto prostatico sanonon esprime IL-17, che però risulta elevato nelle cellulemuscolari liscie e nella parte apicale dei dotti epiteliali nellaIPB.
• Inoltre hanno dimostrato che il IL-17 aumenta la secrezione dialtre citochine pro-infiammatorie come IL-8, IL-6 e TGF- β.
• IL-8 e IL-6 sono 2 potenti fattori di crescita per le celluleprostatiche epiteliali e stromali.
• Questi dati suggeriscono che l’IL-17 gioca un ruolofondamentale nel processo infiammatorio presente in pz conIPB, essendo la principale citochina proinfiammatoria epromuovendo una cascata di altre molecole proinfiammatorie.
Role of inflammation in thepathogenesis of BPH

• Castro et al hanno dimostrato che le cellulesenescenti dell’epitelio prostatico secernonoFGF mediato dall’IL-8 e IL-1a.
• Le citochine proinfiammatorie inoltre induconol’espressione di COX-2. Wang et al hannodimostrato che le cellule che esprimono il COX-2hanno un ritmo di proliferazione più alto edeterminano la up-regulation del geneantiapoptotico Bcl2, offrendo così ulterioricorrelazioni fra infiammazione, apoptosi esquilibrio nella crescita prostatica.
Role of inflammation in thepathogenesis of BPH

ProstaticCancer
Oxidative Stress
PIA (Proliferative Inflammatory Atrophy)
HG PIN (High Grade Prostatic Intraepithelial Neoplasia)
Montorsi Arch It Urol Androl 2008
Inflammation and prostatic disease
ProstatitisBPH
Flogosis

Does intraprostatic inflammation have a role in the pathogenesisand progression of benign prostatic hyperplasia?
Flogosis/BPH Progression
Mishra VC BJU Int 2007
374 pts(TURP)
70% ACIfor AR
40% ACIfor LUTS
Objective: to compare the incidence of acute and/or chronicintraprostatic inflammation (ACI) in men undergoing TURP
for urinary retention and LUTS
Conclusions: the risk of urinary retention due to BPH wassignificantly greater in men with ACI than in those without,
and the association of TURP for retention with ACI wasstronger than that with prostate weight

Flogosis/BPH ProgressionData from the MTOPS study
( Medical Therapies of Prostatic Symptoms)
Chronicinflammatory
infiltrate was foundin 43% of the men
It was hypothesized that the presence ofhistological inflammation may be a predictor of
BPH clinical progression
In terms of:• Symptoms• Acute Uinary Retention (AUR)• BPH related surgery

Flogosis/BPH ProgressionData from the MTOPS study
( Medical Therapies of Prostatic Symptoms)
Patients in all groups (placebo, finasteride, doxazosin and doxazosin+ finasteride) with inflammation were more likely to progress
clinically
Overall clinical progression: 13,2%
No AUR
3,9% BPH related surgery
Chronic Inflammation
No Inflammation
Overall clinical progression: 21%
7,3% BPH related surgery
5,6% AURAccounted forevery AUR
event
Flogosis/BPH ProgressionIs the diagnosis of clinical prostatitis at a young age a
risk factor for development of later BPH?
St Sauver JL try to determine whether physician-diagnosedprostatitis was associated with later development of
symptomatic BPH in a longitudinal, population-basedsample of 2447 men residing in Olmsted County, Minnesota
Physician diagnosed prostatitis was associatedwith a 2.4 fold increased odds of later onset of
several BPH-associated events
Prostatitis may therefore be an earlymarker or a risk factor for
development of later prostatic orurologic problems
St Sauver JL Urology 2008

Flogosis/BPH TreatmentAnti-inflammatory agents should be investigated as new
targets for the treatment of BPH?
Minnery CH J Urol 2005
Benign prostatic hyperplasia cell line viability and modulation of jm-27 bydoxazosin and Ibuprofen
Doxazosin + Ibuprofen
• Significantly decreased of cellviability and induced apoptosisin BPH prostate lines
• Decreased expression of JM-27
Protein highly up-regulated insymptomatic BPH

Flogosis/BPH Treatment
Di Silverio F Eur Urol 2005
Combination therapy with rofecoxib and finasteride in the treatment of menwith lower urinary tract symptoms (LUTS) and benign prostatic hyperplasia(BPH).
Randomized
46 pts(LUTS + BPH)
Group A
Finasteride 5 mg/day
Group B
Finasteride 5 mg/day +Rofecoxib 25 mg/day
Assumption of the study: Cyclooxygenase-2 (COX-2) is expressedin human BPH tissue and displays either a pro-inflammatory effect
or a proliferative effect on prostate cells

Flogosis/BPH Treatment
Di Silverio F Eur Urol 2005
Combination therapy with rofecoxib and finasteride in the treatment of menwith lower urinary tract symptoms (LUTS) and benign prostatic hyperplasia(BPH).
8,7%Qmax > 3 ml/sec0%
34,7%IPSS reduction > 4 points0%
Group BGroup A
1 Month outcomes
6 Months Outcomes: Differences between two groups were no significant
It was hypothesized that theassociation of the drugs induced amore rapid improvement until the
effect of finasteride becomespredominant

Biomarkers for inflammation in BPHIf inflammation is associated with the pathogenesis,
symptoms and progression of BPH
Identification of specific Biomarkerswould be desirable
There are several candidates and many othersare currently being assessed by international
research group
These markers are generally non-specific for prostate or BPH
They could be useful to stratify pts according to the risk of developingBPH, to monitor symptoms and response to medical therapy

Biomarkers for inflammation in BPHMalondialdehyde in benign prostate hypertrophy: a useful marker?
Merendino RA Mediators Inflamm 2003
44 pts
22 pts BPH 22 pts control
Measurement of serum malondialdehyde (MDA),an index of inflammation and oxidative stress
Increased levels in the BPH pts andpositive correlation with PSA

Biomarkers for inflammation in BPHSerum C-reactive protein concentration and lower urinary tract
symptoms in older men in the Third National Health and NutritionExamination Survey (NHANES III)
Rohrmann S Prostate 2005
2337 menLUTS and BPH
Assessment of Symptoms and serum C- reactiveprotein concentration measurement
0,32 mg/dl
0,35 mg/dl
0,36 mg/dl
Men without symptoms, no surgery
Men with three or four symptoms
Men with one or two symptoms
Men withC-Reactive protein
> 3 mg/dl were1.47 times more
likely to have 3 ormore symptoms

Biomarkers for inflammation in BPHSeminal plasma cytokines and chemokines in prostate inflammation:interleukin 8 as a predictive biomarker in chronic prostatitis/chronic
pelvic pain syndrome and benign prostatic hyperplasiaPenna G Eur Urol 2007
83 patients9 men
(CP/CPPS IIIA)31 men
(CP/CPPS IIIB)
23 men (BPH)
Significantly increased levels of cytokines (IL-1alpha, IL-1beta, IL-6, IL-10, IL12p70) andchemokines (CCL1, CCL3, CCL4, CCL17,CCL22, CXCL8/IL-8) were observed in
seminal plasmas from patients with CP/CPPSor BPH. However, only IL-8 was significantly
elevated compared to controls in patientswith CP/CPPS IIIA - IIIB and BPH
Were evaluated seminal plasma levels of 8cytokines and 9 chemokins
20 men (controls)
IL-8 appears to be themost reliable and
predictive surrogatemarker to diagnose
prostate inflammatoryconditions, such asCP/CPPS and BPH

Conclusions
•In BPH enough evidence indicates that chronic immuneinflammation has a crucial role in the development of the disease
•Inflammation in the prostate gland appears to be more closelyrelated to BPH than the clinical syndrome chronic prostatitis
•Undestarding the mechanisms of the dysregulated immunepathways may help to design novel anti-immune inflamatorydrugs
•Futher investigations about the role of inflammation in BPH willexpand our understanding of BPH pathogenesis, its histologicaland clinical progression, allow risk stratification and suggestnovel treatent strategies

EFFETTI FARMACOLOGICI DI SERENOAREPENS PIU’ LICOPENE E SELENIO
(PROFLUSS®) NELLA FLOGOSI CRONICAASSOCIATA A BPH: STUDIO
MULTICENTRICO ITALIANO (PROFLUSSGROUP)

SCHEDULA DEL PROTOCOLLO

VALUTAZIONE DELLA RISPOSTAAL TRATTAMENTO
La valutazione immunoistochimica saràcondotta per la ricerca di linfociti T e dimacrofagi utilizzando rispettivamente glianticorpi monoclonali CD20, CD3 e CD68.Per ciascun preparato con colorazionepositiva si procederà alla conta dellecellule positive in tre campi con obiettivo20x; il valore medio sarà consideratoespressione della densità di linfociti T, B emacrofagi presenti nel preparato.