details of the accufix bipolar atrial ‘j’ leads 25, 2005 accufix research institute page 1 of 14...
TRANSCRIPT

April 25, 2005 Accufix Research Institute Page 1 of 14
Details of the ACCUFIX Bipolar Atrial ‘J’ Leads
INTRODUCTION
The ACCUFIX J leads (models 033-812, 329-701, and 330-801) were recalled on November 3, 1994 after 2 deaths and 2 reports of cardiac tamponade due to protrusion of the J wire. A prospective Multi-Center Study (MCS) began immediately, as recommended by an independent Physician Advisory Committee. The initial objective of this study was to estimate the prevalence of J wire fracture/protrusion and the reliability of chest x-ray and fluoroscopy to determine the status of the J wire (Phase I). In January 1995 (Phase II), the MCS study objectives were amended to identify predictors of fracture and assess the risk of extraction compared to the J wire injury risk. Phase III of the study (Injury Surveillance Program) was initiated April 1999 and focuses on monitoring the risk of J wire injury over time and comparing the cumulative J wire injury risk to the one time Fatal/Life-threatening risk of extraction. The Injury Surveillance Program (ISP) includes an active component, the multi-center study active surveillance program (MCSASP) with eleven centers from the original multi-center study sites and a voluntary component, which monitors worldwide injury reports.
Based on distribution records combined with patient registration records, it is estimated that 41,000 ACCUFIX J leads were implanted worldwide between 1988 and 1994 with 6400 estimated patients currently alive with an ACCUFIX J lead. All implanted leads now have an implant duration of at least 10 years. The objective of recent analyses is to estimate the risk of a patient actually experiencing a J wire injury during their remaining lifetime using the age group specific injury rates, combined with the age and gender adjusted Gompertz survival curves and the last known J wire status to estimate a probability of injury over time which can be compared to the one time Fatal/Life-threatening extraction complication risk.
The following is a summary of the information considered at the November 7, 2004 Physician Advisory Committee (PAC) meeting. The PAC used this information in arriving at their decision to modify the patient management recommendations based on the long implant duration of the currently implanted leads, the low probability of J wire injury projected over the next 20 years and the increasing probability of a fatal or life-threatening extraction complication over time which is highest in female patients.
PREDICTORS OF ACCUFIX ‘J’ WIRE FRACTURE AND PROTRUSION (MCS)
The analyses completed in November 2004 demonstrated that J-shape and prior cardiac surgery are predictive of both time to J wire fracture and time to J wire protrusion by univariate analysis with patients with true J shape and prior cardiac surgery at lower risk. Throughout multiple MCS data analyses as well as independent reports, open J shape has been a consistent predictor of J wire failure (combined Accufix J wire classification groups II, III, IV)1. In addition, lead swing is predictive of J wire fracture, but not of protrusion with patients with no lead swing at lower risk by univariate analysis. By multivariate analysis, J-shape, lead swing and prior cardiac surgery were independent predictors of fracture, with patients having a true J-shape lead, no lead swing and prior cardiac surgery at lower risk of J wire fracture. In part due to the low event rate, there were no significant multivariate predictors of protrusion.
1 Saliba, B., Ardesia, R., John, R., Venditti, F., Schoenfeld, M.: Predictors of Fracture in the Accufix Atrial “J” Lead. The American Journal of Cardiology, July 15, 1997, vol. 80, pp. 229-231. Kawanishi, D., Brinker, J., Kay, G., Love, C., Goldschlager, N., Mutter, M., Petitot, J.C., Pioger, G., Rozkovec, A.: Mechanical and Clinical Predictors of J-Wire Fracture and Injury in a Permanent Atrial Pacemaker Lead: Implications for Management. Journal American College of Cardiology, February 1996, pp. 74A. Telectronics Pacing System, Dear Doctor Letter mailed to implanting and following physicians of Accufix patients, August 25, 1995 pg 2.

April 25, 2005 Accufix Research Institute Page 2 of 14
Table 1 – Predictors of ACCUFIX ‘J’ Wire Fracture and Protrusion Fracture Protrusion
Variable
Univariate
Multivariate
Univariate
Multivariate
Gender NS NS NS NS Implant approach (Cephalic or Subclavian)
NS NS NS NS
J Shape (Closed J or Open J)
0.01 <0.01 0.01 NS
J wire Material (Elgiloy or MP35N)
NS NS NS NS
Lead Swing (No Swing or Any Swing)
0.01 0.03 0.05 NS
Prior Cardiac Surgery (Yes or No)
0.01 <0.01 0.01 NS
Age at Implant (0-50,51-70, >70)
NS NS NS NS
Values greater than 0.05 are considered not significant (NS). However, actual p-values are presented if between 0.05 and 0.1. Lower risk variable listed first where significant differences exist.
RISK OF ACCUFIX ‘J’ WIRE FRACTURE AND PROTRUSION
In November 2004, the PAC once again reviewed the MCSASP fluoroscopic screening data. J wire classification combining data from cinefluoroscopic imaging, post explant observations and returned device analysis was available on 1781 leads. In leads with at least one cinefluoroscopic screening, the number of screenings ranges from 1-20 (median 4). Serial fluoroscopic data includes 8,500 screenings of 1346 leads in 1332 patients.
Earlier engineering studies conducted by an independent failure analysis laboratory demonstrated that in-situ cyclic stresses on the J wire were, in some patients, sufficient over time to cause metal fatigue failure of the J wire.2 Due to the time related mechanism of metal fatigue, the most appropriate method of examining risk is one that incorporates implant duration of the lead. The cumulative hazard function measures the risk over time for an event such as J wire fracture, protrusion or injury. The cumulative hazard function can also be used to assess the constancy of risk, in which case the cumulative hazard function is a straight line, and it’s slope equals the risk per implant year. Because the exact time of fracture or protrusion of the J wire is not known (for example, a lead implanted in 1990 may show a protruded J wire at the time of the first fluoroscopic screening in 1994, or a lead with no J wire protrusion evident on a fluoroscopy in 1994 might show a protruded J wire on a later screening), the time to fracture or protrusion was estimated using a Weibull distribution.
Figure 1 demonstrates a decreasing risk of fracture over time as seen in the Weibull shape parameter (1.49), which is statistically different from one, e.g. a straight line (p=0.001). At 10 years post implant, the estimated fracture risk is 4.3%, while the estimated risk at 15 years post implant is 3.7%.
As shown in Figure 2, the cumulative risk of protrusion appears constant over time as seen in the Weibull shape parameter (1.11), which is not statistically different from one (p=0.47). Assuming a constant risk, the annual protrusion risk is estimated at 1.3% per year. At 10 years implant duration; there is a cumulative 13% probability of protrusion. There is a corresponding 87% probability of remaining free of protrusion at 10 years implant duration.
2 Hoffman, KR Williams BB Esthappan J, Chen SY, Carrol JD, Harauch H, Doerr V, Kay GN, Eberhardt A, Overland M, Determination of 3D positions of pacemaker leads from biplane angiographic sequences. Med Phys. 1997;24:1854-1862. Manning, C, Wenzel, T, Overland, M: Failure Analysis of Explanted Accufix Leads. PACE, 1999;22:717

Figure 1 – Cumulative risk of fracture for MCSASP ACCUFIX ‘J’ leads. The risk of fracture is decreasing over time based on the Weibull shape parameter (1.49), which is statistically different from one, e.g. a straight line (p=0.001). At 10 years post implant, the estimated fracture risk is 4.3% per year, while the estimated risk at 15 years post implant is 3.7% per year. Based on 434 Group II, III, IV leads out of 1781 leads with a J wire classification and implant date.
Figure 2 – Cumulative risk of protrusion for MCSASP ACCUFIX ‘J’ leads.
The risk of protrusion appears constant over time based on the Weibull shape parameter (1.11), which is not statistically different from one (p=0.47). Assuming a constant risk, the annual protrusion risk is estimated at 1.3% per year. Based on 125 Group III, and IV leads out of 1768 leads with a J wire classification and implant date.
April 25, 2005 Accufix Research Institute Page 3 of 14

April 25, 2005 Accufix Research Institute Page 4 of 14
INJURIES ASSOCIATED WITH THE ‘J’ WIRE (WORLDWIDE)
Reported clinical events were categorized as “Injury directly related to J wire”, “Injury possibly related to J wire” or “Clinical event not related to J wire”. The PAC established the following rules for “Injury directly related J wire”: (1) Direct clinical evidence of J wire injury or medical clinical judgment that the injury was caused by the J wire at the time of injury occurrence, (2) Documented cardiac tamponade or bloody pericardial effusion in medical records and an initial fluoroscopic evaluation after the event shows protrusion of the J wire, (3) Documented cardiac tamponade or pericardial effusion, fluoroscopic evaluation is not possible and the primary physician indicates there is no viable explanation other than J wire injury for the cardiac tamponade. The PAC reviewed and classified individual clinical cases where the above rules were not met or incomplete information existed.
The occurrence of J wire injury in the MCS/MCSASP patients before the initiation of the study was determined by review of medical records. Although the MCS/MCSASP provides substantial information about fracture and protrusion, there are only 2 directly related injuries reported in this closely followed population of patients. Because of the rarity of the J wire injuries in the MCS/MCSASP, worldwide injury reports are evaluated in order to obtain reasonable estimates of injury risk and time to event data.
Our last Dear Doctor letter, November 2000 reported 45 directly related injuries. As of November 2004, 48 injuries directly related to the J wire have been reported worldwide, representing 0.1% of the estimated 41,000 implants. The median time to injury is 35 months (range 4 to 125 months). Of the 11,745 deaths from all causes that have been reported to ARI, six of these were directly attributable to J wire injury (0.05%). The PAC classified two cases, with vague symptoms in conjunction with a migrated J wire, as possibly related J wire injuries.
Accufix Research Institute has mailed 9 previous Dear Doctor Letters to monitoring physicians communicating patient management guidelines and requesting all reports of injury related to the J wire be communicated to us. Figure 3 presents the number of reported injuries directly related to the J wire by calendar year in which they occurred. . It should be noted that the large number of worldwide extractions might have reduced the number of J wire injuries that may have occurred if the leads had not been extracted
The annual risk of injury is calculated by dividing the number of injuries (48 injuries) by the cumulative lead years of follow-up (101,784 lead years). The worldwide risk of injury is approximately 0.05% (95% CI: 0.04%-0.06%) per year, with a cumulative risk of injury of 0.5% ten years following implant. Table 2 displays the injury risk by age group. The injury risk is highest in patients with an implant age less than 51 years (0.13% per year) compared to patients with an implant age 51-70 (0.07% per year) and patients with an implant age greater than 70 (0.02% per year) overall p< 0.01.
Table 2 – Injury Risk by Age Group
Age at Implant 0-50 (n=11) 51-70 (n=26) 71+ (n=11) All Leads 0.13% / yr 0.07% / yr 0.02% / yr Fractured Leads 0.6% / yr 0.4% / yr 0.2% / yr Protruded Leads 1.7% / yr 1.1% / yr 0.6% / yr

Figure 3 - Number of ACCUFIX ‘J’ wire injuries by calendar year in which they occurred. Includes 48 directly related J wire injuries.
Most injuries (28 out of 48) occurred prior to initiation of fluoroscopic screening. Of the 20 injuries after fluoroscopic screening, 50% occurred within 6 months of screening. The median time from fluoroscopic screening to injury was 6 months (range 1-22 months). The limited number of injuries and the distribution of post fluoroscopic screening injury times makes it very difficult to identify an optimal screening interval. The low injury risk could support a longer screening interval, while the number of injuries which occurred within 6 months of last fluoroscopic screening class, could suggest maintaining a 6-monthly screening interval. For these reasons, the general recommendation for screening interval remains every 6 months with consideration of longer intervals based on individual factors including: (1) Patient informed decision regarding the risks (2) Risk of Fracture - Patients with closed J Shape, No J Swing and Prior Cardiac Surgery are at lower risk of fracture (3) Risk of Injury- Older patients are at lower risk of injury than younger patients (p<0.01). (4) Suitability of patient as an extraction candidate -The option of no further fluoroscopic screenings should be considered in patients who are not potential candidates for extraction.
WORLDWIDE LEAD EXTRACTIONS
Extracting pacemaker leads is not without risk. The Physician Advisory Committee recommended that extraction risk data be collected and evaluated for ACCUFIX leads.
Extraction complications were categorized as Fatal, Life-threatening or Other major. Life-threatening complications were those that require intensive care, result in cardiac arrest, or require emergency surgical intervention. Clinical events were categorized as other major if there was additional surgical intervention, subsequent infection or a high degree of medical intervention. Minor complications included those that extended the procedure time, caused some discomfort to the patient or negatively impacted quality of life.
Based on data presented at the November 2004 PAC meeting, a total of 5,984 extractions were reported to Accufix Research Institute (5784 intravascular; 195 primary thoracotomy). Post recall intravascular extractions with known outcome (4821 procedures; 54 Fatal/LT complications) were evaluated to determine the cumulative risk of Fatal/Life-threatening extraction complication based on gender and implant duration. Figure 4. Multivariate logistic regression analyses of intravascular extraction complications reported from all sources were performed using the following variables: implant duration, gender, protrusion classification prior to extraction, and patient age at extraction.
April 25, 2005 Accufix Research Institute Page 5 of 14

The risk of extraction increases over time with females at greater risk. At 10 years post implant, the female risk is 2.9% or approximately 3 times greater than the risk in males p<0.01. Protrusion classification is also associated with Fatal/Life-threatening extraction complication with an extraction complication 3.0 times more likely if the J wire is protruded than if it is not (95% CI: 1.6-5.6, p<0.1) Figure 4 - The Fatal/Life-threatening risk of extraction is displayed by gender and time from implant.
At 10 years post implant, the Fatal/Life-threatening extraction risk is 2.9% females; 1.1% males.
New Extraction Techniques
Although, the explant data collected by the ACCUFIX worldwide registry was not specifically designed to prospectively evaluate the efficacy or complications rates associated with laser or snare extraction techniques, the data housed in the database provides an opportunity to examine procedural success and complication rate outcomes compared to traditional extraction techniques.
Laser method
The “Technique/Tools” section of the Explant Form did not include a specific choice for laser; but did include a choice of “Other” and an associated comment field. This comment field was screened for indication of the use of laser, and subjects were classified as “Laser Mentioned” or “Laser Not Mentioned”. It should be noted that because laser extraction information was not specifically collected, it is likely that the category of “Laser Mentioned” is an under-representation of the actual cases where laser was utilized.
Multivariate logistic regression analyses of intravascular extraction complications, reported from all sources, were performed several times as explant information increased. Explant method (laser mentioned, laser not mentioned), implant duration, gender, protrusion classification prior to extraction, and patient age at extraction were included as possible explanatory factors. After adjusting for these possible explanatory factors, female gender, presence of protrusion and laser method mentioned were associated with an increased risk of Fatal/Life-threatening extraction complication. The initial results of these analyses were presented at NASPE3 and repeated over time with increasing data reaching similar conclusion.
3 Love, C., Gross, J., Kawanishi, D., Kay, G., Reeves, R., Davis, M., Pioger, G., Fee, J., Bartelson, B., Brinker, J.: Laser Technique versus Traditional Intravascular Extraction Techniques in the Accufix J Lead. PACE, April 2000, vol. 23, pt. 2, pp. 700 and Europace, July 2000, vol. 1, suppl. D, pp. D202.
April 25, 2005 Accufix Research Institute Page 6 of 14

April 25, 2005 Accufix Research Institute Page 7 of 14
The increased risk of extraction complication observed with laser method mentioned may be due to the limitation of data collection and/or the initial learning curve associated with the recent introduction of this technique. For the ACCUFIX lead population, laser technique has not been shown to provide a lower risk of extraction, and laser availability should not overwhelmingly influence the management of ACCUFIX patients.
Snare Removal of Protruding ACCUFIX J Wires
For patients with protruding J wires, percutaneous removal of the proximal “free” portion of the protruding J wire by catheter technique is an alternative to traditional lead extraction techniques.4 This technique leaves a functioning atrial lead in-situ. The explant form did provide an ability to note “Snare Technique”. Snare J wire removal was also identified by examining the data in “Lead remains” field, “J wire classification prior to explant” field and “J wire remains” field. Snare removal of J wire was identified in extraction attempts of protruding J wires where all of the lead remained, and only part of the J wire remained at the completion of the explant attempt. Based on the above criteria, extraction attempts were classified as “Snare Mentioned” or “Snare Not Mentioned”. Since Technique/Tools and Lead remains were not always populated in the explant form, it is likely that the category of “Snare Mentioned” is an under-representation of the actual cases where the snare technique was utilized.
Data submitted to ACCUFIX worldwide registry indicates 36 cases where snare removal of a J wire was mentioned among 4821 post recall intravascular extraction attempts with known outcome. In the small population in which snare removal was mentioned, there were no Fatal, no Life-threatening (LT) and no Other major complications, compared to 1.1% combined Fatal/LT (25 deaths) extraction complication percentage and a 4.5% major complication (Fatal, LT and Other Major) percentage in the intravascular extraction population with known outcome and no mention of snare removal.
The complication rates do not differ significantly, but due to the low complication rates and the very small number of leads where snare removal was mentioned, statistical power is very low. The PAC recommends that Snare removal of the J wire be considered in patients as an alternative to standard intravascular lead removal when the J wire has substantially protruded from the lead. Partial removal of the protruding portion of the J wire does not exclude the possibility that a remaining portion may protrude, although none have been reported. Therefore, continued fluoroscopic monitoring is recommended if snare removal of the J wire is chosen and a significant portion of the J wire remains.
FUTURE PROBABILITY OF ACCUFIX ‘J’ WIRE INJURY- ALL LEAD STATUS
The cumulative risk of J wire injury as presented earlier in this report represents only a potential risk of J- wire injury. The competing risk of mortality in very elderly patients from other causes is high and most patients will not live long enough to experience an injury from their ACCUFIX lead. As displayed in Figure 55, the observed probability of patient survival is 35% at 10 years post implant and a projected 14% survival at 15 years post implant based on the overall MCSASP survival data.
4 Lloyd, MA, Hayes DL, Stanson AW, Holmes Jr DR. Snare removal of a Telectronics Accufix atrial J retention wire. Mayo Clin Proc. 1995;70:376-379. 5 Gompertz B. On the nature of the function expressive of the low of human mortality, and on the new mode of determining the value of life contingencies. PhilosTrans R Soc Lond A Biol Sci 1825;115:513-580.

Figure 5 –Survival in MCSASP patients
A plot overlying the Kaplan-Meier and Gompertz estimates of survival shows good agreement between the non-parametric Kaplan-Meier estimates and the parametric Gompertz estimates.
We can estimate the risk of actually experiencing a J wire injury during a patient’s remaining lifetime by using the age group specific J wire injury rates combined with the age and gender adjusted Gompertz survival curve (Figure 6) to derive a family of age-dependent cumulative incidence curves. The cumulative incidence curves describe a patient’s probability of injury over time from implant (Figure 7). This curve will level out when there is almost zero chance that the patient is still alive (although the intrinsic risk of injury is still continuing at an assumed constant rate). The value of the cumulative incidence curve at that plateau point is the probability the patient will ever experience injury before dying.
April 25, 2005 Accufix Research Institute Page 8 of 14

Figure 6 –Survival Estimates by Age and Gender Kaplan-Meier and Gompertz curves from the MCSASP
Figure 7 – Cumulative Incidence of ACCUFIX ‘J’ Wire Injury by Age and Gender
The cumulative risk of injury taking into account the probability of patient survival is displayed by years post implant. Age and gender adjusted Gompertz survival curves combined with age group specific J wire injury rates are used to calculate the cumulative incidence of J wire injury since age and gender are significant predictors of patient survival and age is a significant predictor of J wire injury.
April 25, 2005 Accufix Research Institute Page 9 of 14
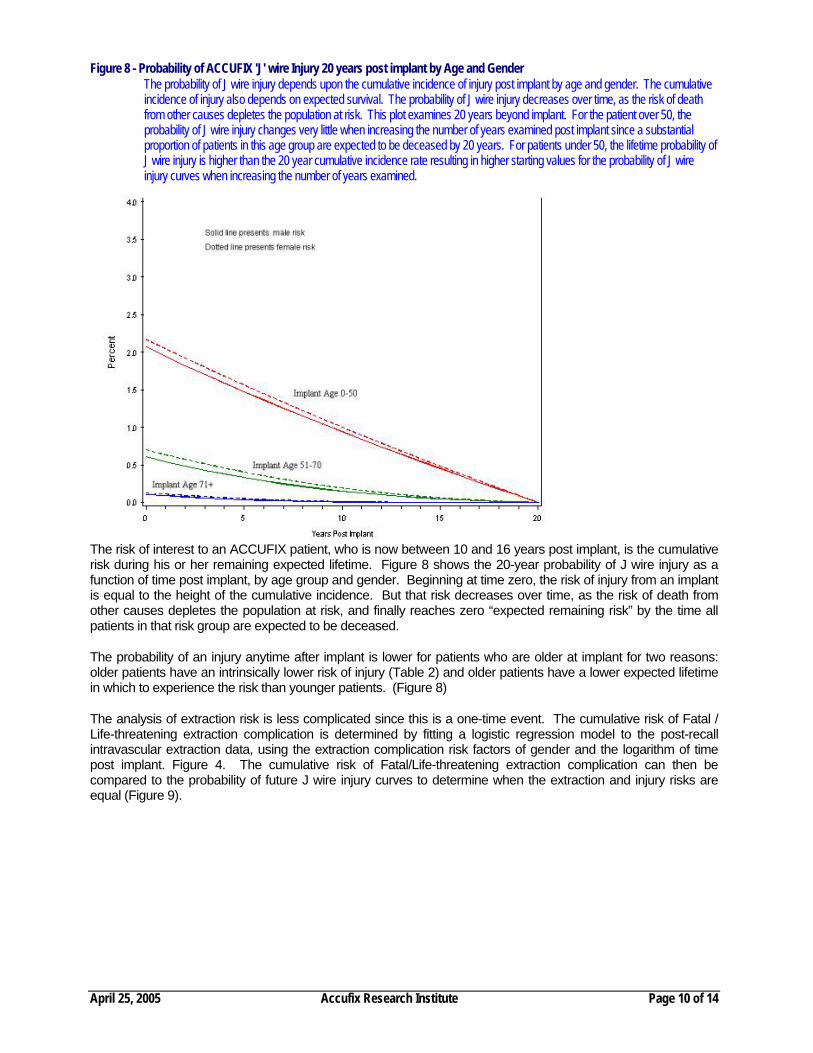
Figure 8 - Probability of ACCUFIX 'J' wire Injury 20 years post implant by Age and Gender The probability of J wire injury depends upon the cumulative incidence of injury post implant by age and gender. The cumulative incidence of injury also depends on expected survival. The probability of J wire injury decreases over time, as the risk of death from other causes depletes the population at risk. This plot examines 20 years beyond implant. For the patient over 50, the probability of J wire injury changes very little when increasing the number of years examined post implant since a substantial proportion of patients in this age group are expected to be deceased by 20 years. For patients under 50, the lifetime probability of J wire injury is higher than the 20 year cumulative incidence rate resulting in higher starting values for the probability of J wire injury curves when increasing the number of years examined.
The risk of interest to an ACCUFIX patient, who is now between 10 and 16 years post implant, is the cumulative risk during his or her remaining expected lifetime. Figure 8 shows the 20-year probability of J wire injury as a function of time post implant, by age group and gender. Beginning at time zero, the risk of injury from an implant is equal to the height of the cumulative incidence. But that risk decreases over time, as the risk of death from other causes depletes the population at risk, and finally reaches zero “expected remaining risk” by the time all patients in that risk group are expected to be deceased.
The probability of an injury anytime after implant is lower for patients who are older at implant for two reasons: older patients have an intrinsically lower risk of injury (Table 2) and older patients have a lower expected lifetime in which to experience the risk than younger patients. (Figure 8)
The analysis of extraction risk is less complicated since this is a one-time event. The cumulative risk of Fatal / Life-threatening extraction complication is determined by fitting a logistic regression model to the post-recall intravascular extraction data, using the extraction complication risk factors of gender and the logarithm of time post implant. Figure 4. The cumulative risk of Fatal/Life-threatening extraction complication can then be compared to the probability of future J wire injury curves to determine when the extraction and injury risks are equal (Figure 9).
April 25, 2005 Accufix Research Institute Page 10 of 14

Figure 9 - Probability of ACCUFXI ‘J’ Wire Injury for 20 years post implant is compared to Fatal/Life-threatening Extraction Complication Risk The probability of Accufix J wire injury is displayed by gender, implant age and time from implant. The Fatal/ Life-threatening risk of extraction is displayed by gender and time from implant. The extraction complication risk can be compared to the probability of J wire injury to determine the balance of risks between J wire injury and extraction. For the older patient, only a small number of patients will be surviving 20 years beyond implant. However, for the patient under 50, the 20-year probability of J wire injury may be an underestimate of the lifetime probability of J wire injury. The extraction and J wire injury probability may balance later in time than indicated on the graph below for very young patients (implant age 0-50) with long expected remaining lifetimes.
The crossing point of the future J wire injury and extraction risk curves indicates the point in time post implant when the two risks are equal. Prior to the crossing points, the 20-year probability of future J wire injury exceeds the one-time risk of fatal or life-threatening extraction complication. After the crossing points, the one-time risk of fatal or life-threatening extraction complication is greater than the 20-year probability of future J wire injury.
INCORPORATING LEAD STATUS INTO THE ACCUFIX LEAD BALANCE OF RISK CALCULATIONS
The analyses listed in the section above were useful in answering the clinical question of whether or not the risk of lead extraction exceeds the future risk of J wire injury based on a patient’s age, gender and time since implant. However, the previous analyses did not account for lead status when predicting the probability of future J wire injury. As the mechanism of J wire injury is such that a lead must be both fractured and protruded in order to cause a J wire injury, there was interest in incorporating lead status into the probability of future J wire injury and balance of risk analyses. Figure 9
Several possible methods for incorporating lead status into the balance of risk calculations were explored. The following is a summary of the findings based upon a method, which incorporates last known lead status into the balance of risk analyses.
Analysis Approach
April 25, 2005 Accufix Research Institute Page 11 of 14
In the Accufix database, each lead is assigned a “summary” lead status (Class I = intact, Class II = fractured, Class III = protruded, Class IV = migrated, or missing) based upon the combined information from x-ray, fluoroscopy, lead examination after explant or autopsy, and occurrence of J wire injury. Lead status is

April 25, 2005 Accufix Research Institute Page 12 of 14
“progressive” in that all leads begin in an intact state and must fracture in order to protrude and must protrude in order to migrate. Injury can only occur after the J wire protrudes (Class III or higher) through its polyurethane sheath. However, not all fractured leads will protrude and not all protruded leads will cause injury; hence, fracture and protrusion are necessary, but not sufficient, conditions for J wire injury. Since a protrusion must occur prior to J wire injury, a “protrusion” classification can be assigned to a lead associated with a J wire injury, even in the absence of lead status information determined in another manner.
The first step in earlier analyses has been to calculate the J wire injury rate, defined as the total number of injuries divided by total lead-time at risk for injury. Previously, J wire injury rates have been shown to differ by age at implant. Conventionally, age at implant has been categorized into 3 levels (0-50, 51-70, and 71+ years), and J wire injury rate calculations were performed by age at implant group to facilitate interpretation of results. Due to the limited number of injuries, stratification of the data by both age group and lead status (3 × 4 = 12 groups) results in unreliable estimates of J wire injury rates in any given stratum. Consequently, to incorporate lead status information into the balance of risk calculations, lead status is dichotomized as intact (Class I) vs. non-intact (Class II-IV).
Because J wire injury can only occur among protruded (Class III) or migrated (Class IV) leads, when lead status is dichotomized as intact (Class I) vs. non-intact (Class II-IV), the J wire injury rate, and consequently the probability of future J wire injury, is zero for the intact (Class I) group. Therefore, this group may be disregarded in the balance of risk analyses. Hence, the analyses incorporating lead status into the balance of risk are accomplished using the same methodology previously employed (see section above for overall lead status) but focusing on the subset of non-intact (Class II-IV) leads.
Results
An estimated 41,000 Accufix leads were distributed and implanted worldwide, with elapsed implant times ranging from 10 to 16 years as of the November 2004. Of these, 16,939 (41%) have an assigned lead status (Table 3 ), including 48 in patients with a directly related J wire injury (40 Class III and 8 Class IV).
Table 3 - Summary Lead Status
Class I 13,480 (79.6%) Class II 2,388 (14.1%) Class III 970 (5.7%) Class IV 101 (0.6%) 16,939
As in previous analyses, the overall (all lead) injury rate analyses were calculated for the population of leads having non-missing age at implant and follow-up information The non-intact (Class II-IV) injury rate analyses are based on a subset of leads with known lead status (Class II-IV), age group and follow-up information.
The balance of risks presented in earlier Dear Doctor Letters and repeated in the section above (Figure 9) describes the overall probability of future J wire injury based upon gender, age at implant and implant duration, but did not incorporate lead status information. Overlaid on these curves are plots of the probability of life-fatal or Life-threatening intravascular extraction complications by gender and time since implant. Figure 10 shows the results of repeating the balance of risk analyses on the subset of non-intact (Class II-IV) leads.
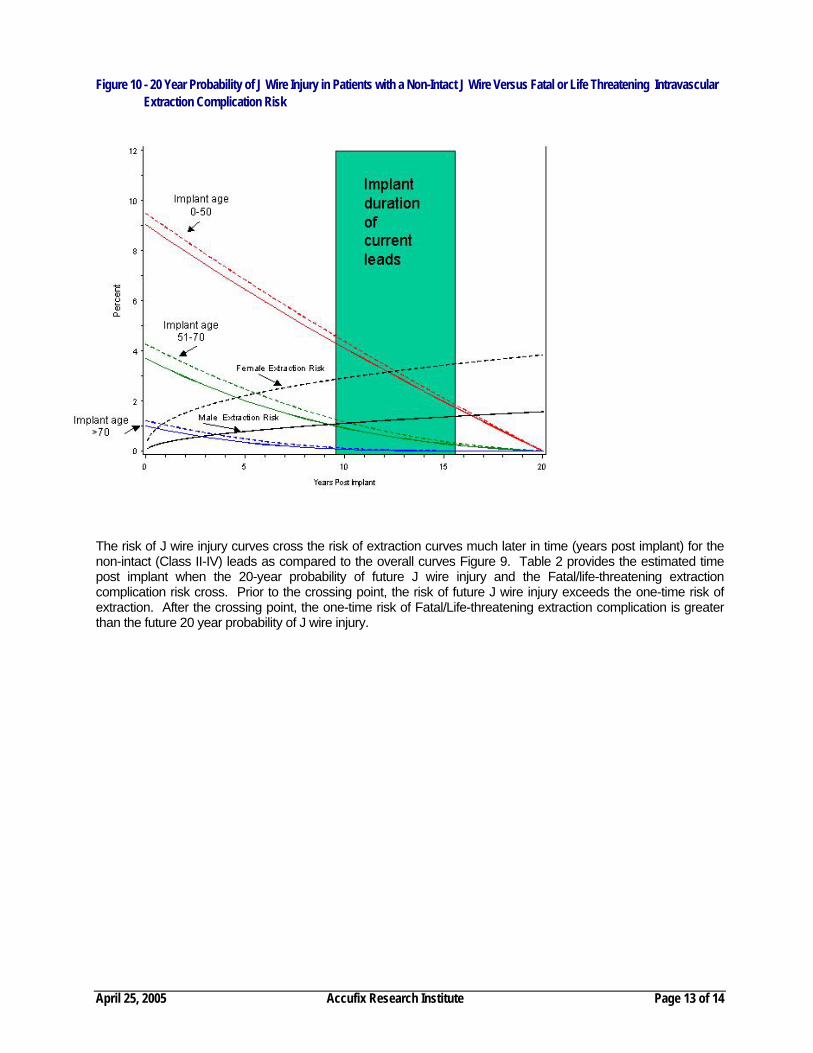
Figure 10 - 20 Year Probability of J Wire Injury in Patients with a Non-Intact J Wire Versus Fatal or Life Threatening Intravascular
Extraction Complication Risk
The risk of J wire injury curves cross the risk of extraction curves much later in time (years post implant) for the non-intact (Class II-IV) leads as compared to the overall curves Figure 9. Table 2 provides the estimated time post implant when the 20-year probability of future J wire injury and the Fatal/life-threatening extraction complication risk cross. Prior to the crossing point, the risk of future J wire injury exceeds the one-time risk of extraction. After the crossing point, the one-time risk of Fatal/Life-threatening extraction complication is greater than the future 20 year probability of J wire injury.
April 25, 2005 Accufix Research Institute Page 13 of 14
April 25, 2005 Accufix Research Institute Page 14 of 14
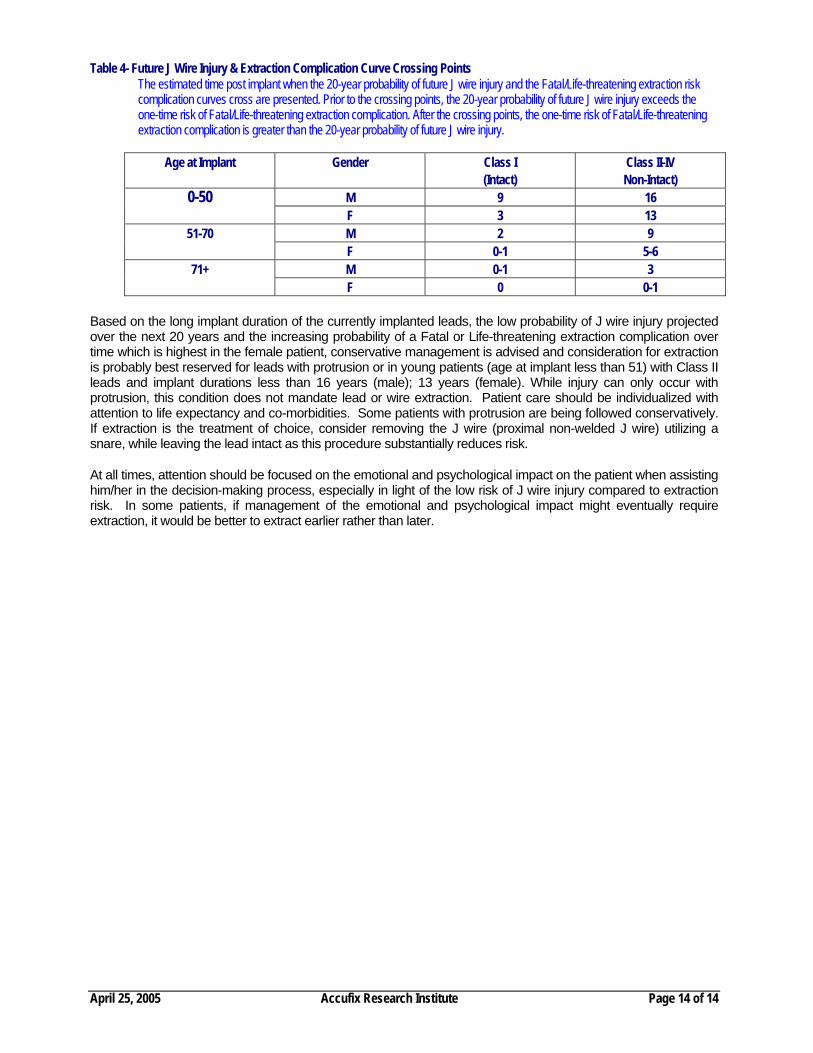
Table 4- Future J Wire Injury & Extraction Complication Curve Crossing Points The estimated time post implant when the 20-year probability of future J wire injury and the Fatal/Life-threatening extraction risk complication curves cross are presented. Prior to the crossing points, the 20-year probability of future J wire injury exceeds the one-time risk of Fatal/Life-threatening extraction complication. After the crossing points, the one-time risk of Fatal/Life-threatening extraction complication is greater than the 20-year probability of future J wire injury.
Age at Implant Gender Class I (Intact)
Class II-IV Non-Intact)
M 9 16 0-50 F 3 13 M 2 9 51-70 F 0-1 5-6 M 0-1 3 71+ F 0 0-1
Based on the long implant duration of the currently implanted leads, the low probability of J wire injury projected over the next 20 years and the increasing probability of a Fatal or Life-threatening extraction complication over time which is highest in the female patient, conservative management is advised and consideration for extraction is probably best reserved for leads with protrusion or in young patients (age at implant less than 51) with Class II leads and implant durations less than 16 years (male); 13 years (female). While injury can only occur with protrusion, this condition does not mandate lead or wire extraction. Patient care should be individualized with attention to life expectancy and co-morbidities. Some patients with protrusion are being followed conservatively. If extraction is the treatment of choice, consider removing the J wire (proximal non-welded J wire) utilizing a snare, while leaving the lead intact as this procedure substantially reduces risk.
At all times, attention should be focused on the emotional and psychological impact on the patient when assisting him/her in the decision-making process, especially in light of the low risk of J wire injury compared to extraction risk. In some patients, if management of the emotional and psychological impact might eventually require extraction, it would be better to extract earlier rather than later.