development and validation of a digital head posture measuring
TRANSCRIPT

●
n●
g●
cpata1prr●
coactghld●
av(E
Atuif
A
CCb
TDd1
1
Development and Validation of a Digital Head PostureMeasuring System
ERIC S. HALD, RICHARD W. HERTLE, AND DONGSHENG YANG
heitTosshrwcTpmcw
dlart
pha
●
mrmdcaplto
hm
PURPOSE: To report the accuracy and repeatability of aew digital head posture measuring system.DESIGN: Prospective study, clinical laboratory investi-
ation.METHODS: The digital head posture measuring system
onsists of a head-mounted motion tracker, a standardersonal computer, and customized software to samplend display 3-dimensional (3D) head posture in real-ime. Using a mechanical head posture measuring devices a reference, 3D head positions of an artificial head and2 human subjects were recorded with the digital headosture device. Accuracy of the digital device outputs,elationship between digital outputs and actual headotations, and repeatability of the tests were analyzed.
RESULTS: The digital head posture device showedonsistent outcomes when compared to the mechanicalne. The digital outputs of 3D rotations are very close toctual artificial head and human head rotations. Theorrelation coefficients of the linear relationship betweenhe digital outputs and actual head movements werereater than 0.99. Repeatability tests for the artificialead and human subjects for all 3D rotations had 95%
imits of agreement angles less than �6 degrees and �8egrees, respectively.CONCLUSIONS: The digital head posture device is an
cceptable device with high accuracy, repeatability, andalidity in measuring head posture in 3 dimensions.Am J Ophthalmol 2009;147:1092–1100. © 2009 bylsevier Inc. All rights reserved.)
NOMALOUS HEAD POSTURE IS A COMMON CLINI-
cal symptom caused by ocular, orthopedic, andneurologic disorders.1–3 While a variety of condi-
ions may be responsible, anomalous head posture attrib-table to visual system abnormalities, or ocular torticollis,s quite common in children. For example, it has beenound that about 62% of child patients with nystagmus
Supplemental Material available at AJO.com.ccepted for publication Dec 15, 2008.From the Ocular Motor Neurophysiology Laboratory, The UPMC Eye
enter, Department of Ophthalmology, Pediatric Ophthalmology, Thehildren’s Hospital of Pittsburgh and University of Pittsburgh, Pitts-urgh, Pennsylvania.Inquiries to Dongsheng Yang, 3705 5th Ave, Room 2952, Main Tower,
he Ocular Motor Neurophysiology Laboratory, The UPMC Eye Center,epartment of Ophthalmology, Pediatric Ophthalmology, The Chil-
cren’s Hospital of Pittsburgh and University of Pittsburgh, Pittsburgh, PA5213; e-mail: [email protected]
© 2009 BY ELSEVIER INC. A092
ave anomalous head posture.4 There is evidence thatarly corrective surgery for children with ocular torticollismproves visual function5 and may prevent musculoskele-al problems resulting from uncorrected ocular torticollis.2,3
hus, an effective technique for accurate measurement ofcular torticollis in children is needed to assist withurgical planning. However, current techniques for mea-uring anomalous head posture, including a mechanicalead posture device6 or a cervical range of motion device7
equires extensive patient cooperation not always availableith children. This makes accurately measuring a younghild’s torticollis virtually impossible using such devices.he ideal device for measuring head posture requires littleatient cooperation and provides instantaneous reliableeasurements. When such a device is proven useful for
hildren, it will be easily applicable for adult patients asell.Head rotation about 3 axes is usually measured in
egrees. We will use head-turn for rotation around theongitudinal axis (y-axis), chin-up/down for rotationround the interaural axis (x-axis), and head tilt forotation around the naso-occipital axis (z-axis) of the headhroughout the study.
In the present study, we have developed a digital headosture measuring system and tested it with an artificialead and normal human subjects. We will report theccuracy and repeatability of measurements.
METHODS
DEVICES: Mechanical Head Posture Measuring Device. Aechanical head posture measuring device was used as the
eference to validate our digital head posture device. It wasounted on the same helmet with the digital head posture
evice. The mechanical head posture measuring deviceonsists of 2 intersecting plastic protractors, a grid pattern,nd a laser. The grid pattern with marked angles wasrojected on to a screen and used in combination with theaser to measure head-turn and chin-up/down. The pro-ractors were used to measure head tilt. A complete settingf the mechanical head posture device is shown in Figure 1.
The Digital Head Posture Measuring System. The digitalead posture measuring system consists of a motion trackerounted on an adjustable headset, a controller personal
omputer, and custom software for data recording and
LL RIGHTS RESERVED. 0002-9394/09/$36.00doi:10.1016/j.ajo.2008.12.026

vdim2pTtaaffdsbfehca(Cnsrmroptmrdh
dwsmshtvta
●
dt
hSp
Fddppa
FamTtho
DIGITAL HEAD POSTUREVOL. 147, NO. 6
isualization. A photo including mechanical head postureevice and digital head posture measuring system is shownn Figure 2. The figure has 3 main parts: 1) a computeronitor showing numerical outputs and a simulated head;
) a helmet with laser pointer and protractors; and 3) aair of spectacle frames with the mounted motion tracker.he motion tracker can be mounted on either helmet or
he frame. The motion tracker is commercially availablend uses hybrid techniques including magneticometer,ccelerometer, and gyroscope made by InterSense (Bed-ord, Massachusetts, USA). It uses a local-level geographicrame with it x-axis pointing north, y-axis east and z-axisown. The reported rotation angles can be described as aequence of rotation applied to the device starting with itsody axis initially aligned with its axis of the referencerame in space and resulting in the current orientation. Forxample, the sequence starts with a rotation of rightead-turn about the z-axis, followed by a rotation ofhin-up about the new y-axis (the axis of the device body),nd followed by a rotation of head-tilt about the new x-axisthe axis of the device body). The software was written in�� by one of our collaborators. Using the same coordi-ate frame as the tracker, the digital head posture measuringystem continuously measures a patient’s head posture at aate of 20 Hz and presents a real-time animation of a headovement on a liquid crystal display along with numerical
eadings. It records and saves the data into a computer file forffline analysis. The saved data include the initial headosition, ending head position, and the difference betweenhe 2 positions (head posture in degrees). It is claimed by theanufacturer that the tracker works with full 360 degrees
ange with angular accuracies of 0.25 degrees for chin-up/own and head tilt measurements and 0.50 degrees foread-turn measurements.
Artificial Head. To produce accurate head rotation, weeveloped an artificial head. The artificial head was builtith a multi-directional rotation joint (Manfrotto, Bas-
ano Del Grappa, Italy) that allows 3-dimensional (3D)ovement and a foam head similar to the human head in
ize. A regular laser pointer was mounted on the artificialead close to the joint. When the laser was aligned withhe center of the display grid pattern, horizontal andertical rotations were projected on the display grid pat-ern. The intersecting protractors were set on top of thertificial head to measure head tilt.
PROCEDURES: The mechanical head posture measuringevice including protractors/laser pointer was used for bothhe measurement of artificial head and human subjects.
Measuring Rotations of the Artificial Head. The artificialead was placed 1.1 meters from the display grid pattern.pecial care was taken to mount the laser close to pivot
IGURE 2. A photo showing the mechanical head posture andigital head posture devices. The digital head posture deviceisplays numerical outputs and a simulated head on the com-uter monitor. A helmet that carries the mechanical headosture device and the sensor of the digital head posture device,nd a spectacle frame for the sensor are included.
IGURE 1. Schematic draw for the mechanical head posturend digital head posture devices. The crossed protractors areounted on top of the helmet and are used to measure head tilt.he laser pointer set at the level of the display grid center, close
o nose-level, along with display grid, is used to measureead-turn and chin-up/down. The digital head posture device isn top of the helmet and below the protractors.
oint of the head (at nose level) and level it with the
MEASURING SYSTEM 1093

cws
fidt
cocsqicistq
n8
pwpb
hhapttdptltlthdpqs
FrcT
1
enter of the display pattern. The laser and display patternere used to measure head-turn and chin-up/down. The
ize of the display pattern covers 80H � 80W degrees.
One-dimension Rotations of the Artificial Head. The arti-cial head was rotated in horizontal, vertical or torsionalimensions in 10-degree increments up to 40 degrees. Sixests for each head position were performed.
Three-dimension Rotations of the Artificial Head. To in-orporate all abnormal head positions that can possiblyccur in clinical patients, the artificial head was rotated inombination of horizontal, vertical, and torsional dimen-ions in 10-degree increments up to 30 degrees in eachuadrant. The artificial head was directly rotated from annitial zero position to a final 3D position of head-turn �hin-up/down � head tilt. The difference between thenitial position and the final position was recorded. Nopecific order of rotations was used. Each head position wasested 3 times for a total of 72 head positions in 4uadrants.
Measuring Rotations of Human Subject’s Head. Twelveormal adult subjects (20 to 48 years old, 4 females and
IGURE 3. Measured outputs for 1-dimensional rotations of thotations. The average outputs are identical to actual rotationhin-up/down vs horizontal rotations. The outputs varied withinhe outputs varied within a degree as well.
males) with normal head posture and normal vision d
AMERICAN JOURNAL OF094
articipated in the investigation. All head positions testedere 3D positions. Only adult subjects were selected toarticipate in the tests because the tests require subjects toe cooperative.The distance from the screen to the center of subjects’
ead was 1.1 meters. Subjects were seated and held theiread at a primary position (0 degrees in all 3 dimensions)t the beginning of each trial. An adjustable head rest waslaced against their backs to restrain their body’s transla-ional movements. After the subject’s primary head posi-ion was set, the laser pointed to the center of theisplay pattern, and the protractor pointed to a zeroosition. The digital head posture measuring system washen zeroed by pressing the space bar on the computer. Aocation in the grid was given to the subjects; subjectsurned their head to point a dot at the location with theaser, such as a 10-degree 3D head position of left head-urn, chin-up, and left head tilt. Subjects turned theireads in increasing angles in 10-degree increments to 30egrees, as indicated by the dots in Figure 1. Each subjectarticipated in 3 sets of tests for all 3D head positions in 4uadrants, resulting in a total of 72 head positions for eachubject. The subjects did not have any feedback from the
ificial head. (Top left) Measured head-turn vs actual horizontaltheir correlation coefficient is 0.99. (Top right) Outputs of
gree. (Bottom left) Outputs of head tilt vs horizontal rotations.
e arts and1 de
igital outputs.
OPHTHALMOLOGY JUNE 2009

●
hawrdb
1c2t
●
Rh
tTphcrt1piaavtaaTAaa
FOfDpdq
V
DATA ANALYSIS: Head position data from the artificialead and from normal subjects were analyzed graphicallynd statistically. Correlation coefficients for each rotationere calculated over the range of angles measured. The
epeatability of the artificial head data and normal subjectata was determined using 95% limits of agreement (LoA)etween 2 of the 3 tests using Equation 1.8
95% LoA � Mean � 1.96� Standard Deviation of Differences [1]
To determine repeatability, the difference between Testand Test 2, Test 2 and Test 3, and Test 3 and Test 1 were
alculated along with the mean of Test 1 and Test 2, Testand Test 3, and Test 3 and Test 1. These values were
hen used in Equation 1 to assess repeatability.
RESULTS
RESULTS FROM THE ARTIFICIAL HEAD: One-dimensionotations of the Artificial Head. Average outputs of digital
IGURE 4. Measured average outputs of the digital device futputs of head-turn vs horizontal rotations. Data for right hea
or left head-turn are in the left side of the figure (quadrants IIata for chin-up rotations are in the upper part of the figure (art of the figure (quadrants III and IV); (Bottom left) Outputsevice are close to the actual rotations. All correlation coefficieuadrants.
ead posture measuring system for horizontal head-turn of t
DIGITAL HEAD POSTUREOL. 147, NO. 6
he artificial head are displayed in Figure 3. In Figure 3,op left, the head-turn outputs from the digital headosture measuring system are almost identical to the actualorizontal rotation of the artificial head. The correlationoefficient between the horizontal outputs and horizontalotations is 0.99. Figure 3, Top right and Bottom left showshat the chin-up/down and head tilt outputs varied withindegree as the artificial head moved to different horizontalositions. Average outputs of digital head posture measur-ng system for chin-up/down of the artificial head are alsolmost identical to the actual vertical rotation of thertificial head. The correlation coefficient between theertical outputs and vertical rotations is 0.99. Similar tohe horizontal rotation of the artificial head, the horizontalnd torsional outputs varied within 1 degree as thertificial head moved to different vertical positions (see theable for the detailed values of each head position).verage outputs of digital head posture measuring system
re almost identical to the actual torsional rotations of thertificial head as well. The correlation coefficient between
dimensional (3D) rotations of the artificial head. (Top left)rn are in the right side of the figure (quadrants I and IV); dataII). (Top right) Outputs of chin-up/down vs vertical rotations.rants I and II); data for chin-down rotations are in the upperad tilt vs torsional rotations. All measured outputs of the digitalre greater than 0.99. I, II, III, and IV represent first to fourth
or 3-d-tu
and Iquadof hents a
he torsional outputs and torsional rotations was 0.99. The
MEASURING SYSTEM 1095
ht(
r1c
tretbhwaaIhrumtph
p
Eit
ttdBc(rc(otTbdfm�m��3
●
FmTt
1
orizontal and vertical outputs varied within 1 degree ashe artificial head moved to different torsional positionssee the Table for details).
The results from pure horizontal or vertical or torsionalotations of the artificial head clearly demonstrated the-dimensional (1D) movements produced little to noross-talk to other dimensions.
Three-dimension Rotations of the Artificial Head. For ro-ations of the artificial head in all 3 dimensions concur-ently, outputs of digital head posture measuring system forach head position are plotted in 4 quadrants according tohe direction of head rotation (Figure 4). Data for com-ined 3D rotations with right head-turn are in the rightalf panel (quadrants I and IV); combined 3D rotationsith left head-turn are in the left half panel (quadrants IInd III); chin-up is in the upper panel (quadrants I and II);nd chin-down is in the bottom panel (quadrants III andV). Data for right and left head tilt in combination withead-turn and chin-up/down are presented in each quad-ant. Outputs of digital head posture for head-turn, chin-p/down, and head tilt are very close to their actualechanical head posture angles (Figure 4). The correla-
ion coefficients between the outputs of digital headosture measuring system and movements of the artificialead are higher than 0.99.To determine the repeatability, 95% LoA were com-
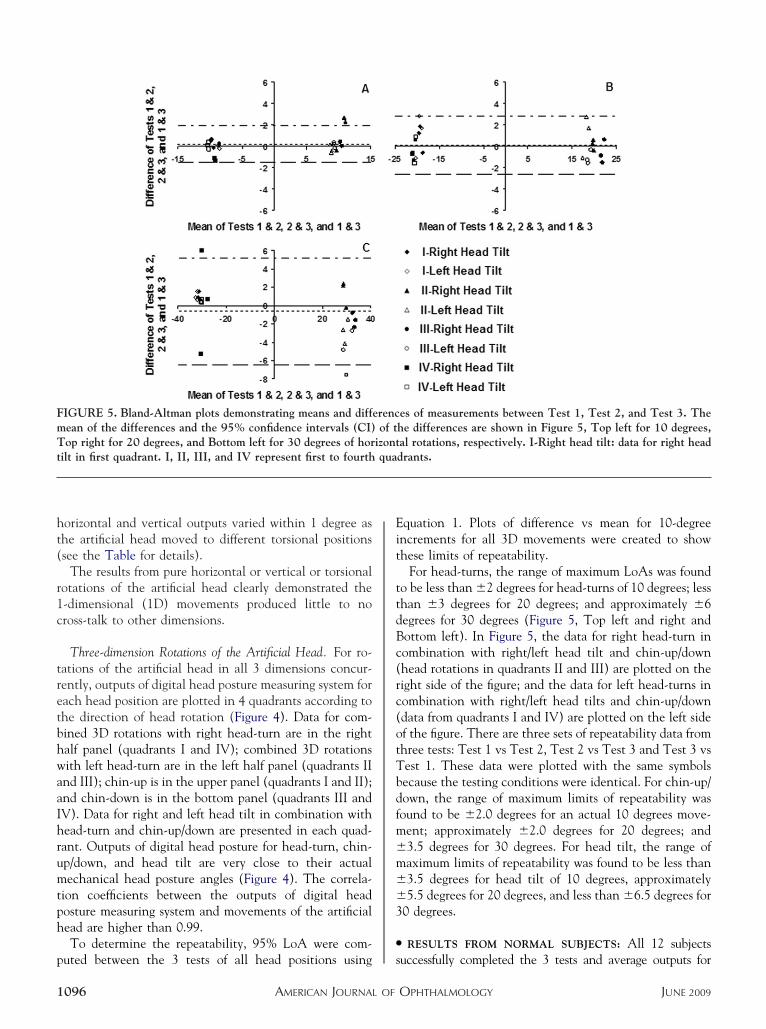
IGURE 5. Bland-Altman plots demonstrating means and diffean of the differences and the 95% confidence intervals (CI)op right for 20 degrees, and Bottom left for 30 degrees of hor
ilt in first quadrant. I, II, III, and IV represent first to fourth
uted between the 3 tests of all head positions using s
AMERICAN JOURNAL OF096
quation 1. Plots of difference vs mean for 10-degreencrements for all 3D movements were created to showhese limits of repeatability.
For head-turns, the range of maximum LoAs was foundo be less than �2 degrees for head-turns of 10 degrees; lesshan �3 degrees for 20 degrees; and approximately �6egrees for 30 degrees (Figure 5, Top left and right andottom left). In Figure 5, the data for right head-turn inombination with right/left head tilt and chin-up/downhead rotations in quadrants II and III) are plotted on theight side of the figure; and the data for left head-turns inombination with right/left head tilts and chin-up/downdata from quadrants I and IV) are plotted on the left sidef the figure. There are three sets of repeatability data fromhree tests: Test 1 vs Test 2, Test 2 vs Test 3 and Test 3 vsest 1. These data were plotted with the same symbolsecause the testing conditions were identical. For chin-up/own, the range of maximum limits of repeatability wasound to be �2.0 degrees for an actual 10 degrees move-ent; approximately �2.0 degrees for 20 degrees; and3.5 degrees for 30 degrees. For head tilt, the range ofaximum limits of repeatability was found to be less than3.5 degrees for head tilt of 10 degrees, approximately5.5 degrees for 20 degrees, and less than �6.5 degrees for
0 degrees.
RESULTS FROM NORMAL SUBJECTS: All 12 subjects
es of measurements between Test 1, Test 2, and Test 3. Thehe differences are shown in Figure 5, Top left for 10 degrees,al rotations, respectively. I-Right head tilt: data for right headdrants.
erencof t
izontqua
uccessfully completed the 3 tests and average outputs for
OPHTHALMOLOGY JUNE 2009

F(t
Fma
V
IGURE 6. Average outputs of the digital device for 3D rotations of human subjects. The conventions are identical to Figure 4.Top left) Head-turn outputs vs horizontal rotations. (Top right) Chin-up/down outputs vs vertical rotations. (Bottom left) Headilt vs torsional rotations. All correlation coefficients are greater than 0.99.
IGURE 7. Bland-Altman plots demonstrating means and differences of measurements between Test 1, Test 2, and Test 3. Theean of the differences and the 95% CI of the differences are shown in Figure 7, Top left for 10 degrees, Top right for 20 degrees,
nd Bottom left for 30 degrees of horizontal rotations, respectively. The conventions are identical to Figure 5.
DIGITAL HEAD POSTURE MEASURING SYSTEMOL. 147, NO. 6 1097

hdFaFbslarrlttccrIaccan(d
ti
hr
pEitam�ddhafiovwildd3m�f
colu
1
ead-turn, chin-up/down, and head tilt were computed andisplayed in Figures 6, Top left and right and Bottom left. Inigure 6, the head position data are plotted in 4 quadrants inccordance with the direction of head rotation, the same as inigure 4. For head-turn (Figure 6, Top left), data for com-ined 3D rotations with right turn are displayed in the rightide of the figure (quadrants I and IV), with left turn in theeft side (quadrants II and III). When left turns were associ-ted with left tilts and when right turns were associated withight tilts, outputs of head-turns were lower than the actualotations. When right turns were combined with left tilts andeft turns were combined with right tilts, average outputs ofhe digital head posture measuring system were nearly iden-ical to rotations of the mechanical head posture device. Forhin-up/down (Figure 6, Top right), data for 3D rotation withhin-up are presented in the upper part of the figure (quad-ants I and II), with chin-down in the lower part (quadrantsII and IV). When chin-ups were associated with right tilts,nd chin-downs were associated with left tilts, outputs ofhin-ups/downs were lower than the actual rotations. Whenhin-ups were associated with left tilts, and chin-downs weressociated with right tilts, outputs of chin-ups/downs wereearly identical to the actual rotations. For head tilt rotationFigure 6, Bottom left), the outputs of associated chin-up/own were close to the actual rotations.
Analysis of the normal subject data for 3D head rota-ions showed high correlation between angles of mechan-
TABLE. Data Sheet for One-Di
Head-turn
Chin-up/down Mean SD
40.000 0.583 0.319
30.000 0.450 0.259
20.000 0.983 0.293
10.000 0.233 0.468
0.000 0.000 0.000
�10.000 0.300 0.551
�20.000 0.833 0.753
�30.000 0.833 0.602
�40.000 0.633 0.423
Head tilt Mean SD
40.000 0.033 0.103 �
30.000 0.083 0.160 �
20.000 �0.017 0.041 �
10.000 0.033 0.052 �
0.000 0.000 0.000
�10.000 0.000 0.000 �
�20.000 0.033 0.052
�30.000 0.033 0.082
�40.000 0.033 0.151 �
SD � standard deviation.
Data in the left column are actual rotation angles and that in bold
cal head posture measuring system and angles of digital t
AMERICAN JOURNAL OF098
ead posture measuring system for all 3 dimensions. Cor-elation coefficients were higher than 0.99.
Ninety-five percent limits of repeatability were com-uted between the 3 tests of all 12 normal subjects usingquation 1. Plots of difference vs mean for 10-degree
ncrements of all 3D movements were created to showhese limits of repeatability (Figures 7, Top left and rightnd Bottom left). As shown in Figure 7, the range ofaximum limits of repeatability was found to be less than2.5 degrees for head-turns of 10 degrees; less than �3.0
egrees for 20-degree head-turns; and approximately �4egrees for 30-degree head-turns. In Figure 6, the data foread positions of right turn in combination with head tiltnd chin-up/down are plotted on the right side of thegure, with left head-turn on the left side. There are 3 setsf repeatability data from 3 tests: Test 1 vs Test 2, Test 3s Test 3 and Test 3 vs Test 1. These data were plottedith the same symbols because the testing conditions were
dentical. For chin-ups/downs, the range of maximumimits of repeatability was found to be less than �2.5egrees for 10-degree chin-ups/downs; approximately �3egrees for 20-degree chin-ups/downs; and �4 degrees for0-degree chin-ups/downs. For head tilts, the range ofaximum limits of repeatability was found to be less than4.5 degrees for 10-degree tilts; approximately �6 degrees
or 20-degree tilts; and less than �8 degrees for 30-degree
ional Artificial Head Rotations
Chin-up/down Head tilt
n SD Mean SD
50 0.389 �0.500 0.167
67 0.288 �0.367 0.234
83 0.387 �0.117 0.098
17 0.560 0.083 0.360
00 0.000 0.000 0.000
67 0.393 �0.033 0.082
67 0.476 �0.333 0.497
00 0.533 �0.433 0.121
00 0.379 �0.417 0.306
SD Mean SD
3 0.194 40.400 0.2280 0.176 30.167 0.6927 0.117 19.783 0.5340 0.155 10.083 0.3430 0.000 0.000 0.0003 0.137 �9.617 0.6497 0.082 �19.400 0.3740 0.063 �29.567 0.3780 0.243 �39.667 0.446
mns are for digital head posture device outputs.
mens
Mea
39.629.519.710.10.0
�9.9�20.1�29.9�40.2
Mean
0.18
0.15
0.01
0.10
0.00
0.03
0.06
0.00
0.05
ilts.
OPHTHALMOLOGY JUNE 2009

M
mtwG3ddLmcYotpmhr2iwmbuBpcvapm
sh2rhsrtvtrsat
stwator
hcwptcw
mdhsmthtmtpa
hottdtcp
pscaoc
hw
FuF
V
DISCUSSION
OST CLINICIANS USE SIMPLE OBSERVATION TO DETER-
ine anomalous head posture for clinical use. Accordingo a report from Kim and associates,9 the range of the erroras from 2 degrees to 18 degrees in visual estimation.ranet and associates10 had a similar observation. For a
0-degree head-turn, examiners estimate varied from 10egrees to 50 degrees. There have been several methodseveloped to measure abnormal head posture. Young andundström used photographic methods to measure abnor-al head posture,11,12 but their data analysis was time
onsuming, and the results were not promptly available.ang and associates reported using a L3D system consistingf a head mounted laser pointer and a display grid patterno measure head postures.6 However, this method requiresatients to be very cooperative because translationalovements of the head might be displayed on the grid asead rotations. Using an inclinometer and Rustrak Rangerecorder, a portable device was developed to measure 1- or-dimensional head position.13–16 Because of the portabil-ty of the device, it could measure head posture duringalking. However, there have been only 2-dimensionaleasurements reported using such a device. It has also
een reported that a cervical range of motion device is aseful device for abnormal head posture measurement.7
ut in clinical practice, reading the small marks of a headosition on 3 meters is not as easy when testing younghildren whose heads move quickly and frequently. Con-ersely, a digital head posture measuring system canccurately measure the anomalous head posture for childatients, report results promptly, and digitize the measure-ents for later reference without any hand-writing errors.Using a commercially available motion tracker and a
tandard personal computer, we have developed a digitalead posture measuring system (Hald ES, et al. IOVS008; 49: ARVO E-Abstract 756). The results of 1Dotation from the artificial head showed that the digitalead posture measuring system is highly accurate in mea-uring 1D head rotation (Figure 3; Table 1). For 3Dotations of the artificial head measured in all quadrants,he outputs of head-turn, chin-up/down, and head tilt wereery close to the actual head rotations (Figure 4), andhere is no significant difference between the actualotations and measured digital head posture measuringystem outputs. Linear relationships between the outputsnd actual head rotations are shown to have high correla-ion coefficients for all rotations in each quadrant (0.99).
The average outputs of digital head posture measuringystem of 3D head movements from normal subjects are closeo actual head rotations (Figure 6). When left head-turnsere associated with left tilts and when right head-turns weressociated with right tilts, outputs of head-turns were lowerhan the actual rotations. The relationship between outputsf the digital head posture measuring system and actual head
otations is linear, and the correlation coefficients are as iDIGITAL HEAD POSTUREOL. 147, NO. 6
igh as 0.99 for these conditions. For head tilts, whenhin-ups were associated with right tilt, and chin-downsere associated with left tilt, output of the digital headosture measuring system for chin-up/down were lowerhan the actual rotations. We believe these errors might beaused by inaccurate rotations of the human heads guidedith the mechanical head posture measuring device.Additionally, we fitted a linear mixed effects model toeasured chin-up/downs as a function of true chin-up/
owns. The results indicate that measured chin-up/downas a nonconstant bias. The bias changes linearly with theize of the rotations. Using this linear relationship, weade a correction for the chin-up/down outputs of greater
han 1 standard division. After the correction, the digitalead posture measuring system outputs are very close tohe true rotations (Figure 8). This implies to us that theeasurement errors can be reduced with software correc-
ion in further clinical application of the digital headosture measuring system (see Supplemental Appendixvailable at AJO.com).
The repeatability of the method has been shown to beigh. The results of head-turn and chin-up/down outputsf the digital head posture measuring system showed thathe range of 95% LoA were less than �5 degrees, althoughhe head tilt showed a larger range of repeatability, �8egrees for the movement of 30 degrees. The reason whyhe head tilt movements had larger range of repeatabilityould be partially attributable to reading errors from therotractors.Measurement of head posture using the digital head
osture measuring system is quick and easy, each mea-urement takes only a few seconds. Multiple tests can beompleted within a few minutes. The motion tracker issmall (1.5 � 2 � 9 cm) device that can be mounted
n a frame of spectacles (see Figure 2) and used forhildren.
Taking all results into account, we think the digitalead posture measuring system is an acceptable deviceith high accuracy, repeatability, and validity in measur-
IGURE 8. Corrected outputs of the digital device for chin-p/down in human subjects. The conventions are identical toigure 6.
ng head posture in 3D.
MEASURING SYSTEM 1099

TR(ao
aa
1
HIS STUDY WAS PARTLY SUPPORTED BY NATIONAL EYE INSTITUTE (NEI) GRANT NO. EY015797, BETHESDA, MARYLAND ANDesearch to Prevent Blindness, New York, New York. The authors indicate no financial conflict of interest. Involved in design and conduct of study
E.S.H., R.W.H., D.Y.); data collection (E.S.H., D.Y.); management, analysis, and interpretation of data (E.S.H., R.W.H., D.Y.); critical review of therticle (R.W.H.); and literature search and writing of the article (D.Y.).This study was Institutional Review Board (IRB) approved by the Universityf Pittsburgh IRB.
We thank Dr Bing Wu, Carnegie Mellon University, Pittsburgh, Pennsylvania, for help with the software of the digital head posture measuring systemnd Dr Richard Bilonick, Department of Ophthalmology, University of Pittsburgh, Pittsburgh, Pennsylvania, for his assistance with data analysis. Welso thank Fight For Sight for their generous Summer Student Fellowship grant.
1
1
1
1
1
1
1
REFERENCES1. Nucci P, Kushner BJ, Serafino M, Orzalesi N. A multi-
disciplinary study of the ocular, orthopedic, and neurologiccauses of abnormal head postures in children. Am J Oph-thalmol 2005;140:65–68.
2. Rubin SE, Wagner RS. Ocular torticollis. Surv Ophthalmol1986;30:366–376.
3. Ballock RT, Song KM. The prevalence of nonmuscula causesof torticollis in children. J Pediatr Orthop 1996;16:500–504.
4. Hertle RW, Zhu X. Oculographic and clinical characteriza-tion of 37 children with anomalous head postures, nystag-mus, and strabismus: the basis of a clinical algorithm. JAAPOS 2000;4:25–32.
5. Hertle RW, Dell’Osso LF, FitzGibbon EJ, et al. Horizontalrectus muscle tenotomy in children with infantile nystagmussyndrome: a pilot study. J AAPOS 2004;8:539–548.
6. Yang D, Hertle RW. Gaze-dependent and time restrictedvisual acuity measures in patients with infantile nystagmussyndrome (INS). Am J Ophthalmol 2005;139:716–718.
7. Kushner BJ. The usefulness of the cervical range of motiondevice in the ocular motility examination. Arch Ophthalmol2000;118:946–950.
8. Bland JM, Altman DG. Statistical methods for assessingagreement between two methods of clinical measurement.
Lancet 1986;1:307–310.AMERICAN JOURNAL OF100
9. Kim DS, Coats DK, McCreery KM, et al. Accuracy ofclinical estimation of abnormal head postures. Binocul VisStrabismus Q 2004;19:21–24.
0. Granet DB, Ventura RH, Miller-Scholte A, et al. Markedvariability amongst pediatric ophthalmologists in designatingthe diagnostic gaze position angles in ocular motility evalu-ations. Binocul Vis Strabismus Q 2001;16:291–296.
1. Young JD. Head posture measurement. J Pediatr OphthalmolStrabismus 1988;25:86–89.
2. Lundström F. Registration of natural head posture in chil-dren. Swed Dent J Suppl 1982;15:147–152.
3. Usümez S, Orhan M. Inclinometer method for recording andtransferring natural head position in cephalometrics. Am JOrthod Dentofacial Orthop 2001;120:664–670.
4. Usumez S, Uysal T, Orhan M, Soganci E. Relationshipbetween static natural head position and head positionmeasured during walking. Am J Orthod Dentofacial Orthop2006;129:42–47.
5. Usumez A, Usumez S, Orhan M. Effect of complete dentureson dynamic measurement of changing head position: A pilotstudy. J Prosthet Dent 2003;90:394–400.
6. Murphy KE, Preston CB, Evans WG. The development ofinstrumentation for the dynamic measurement of changinghead posture. Am J Orthod Dentofacial Orthop 1991;99:
520–526.OPHTHALMOLOGY JUNE 2009

A
mioOwme
w“
rm
Ttwhci
T
V
SUPPLEMENTAL APPENDIX
LINEAR MIXED EFFECTS MODEL WAS USED TO MODEL
easured pitch as a function of true pitch. This modelncluded a random intercept to account for subject heter-geneity. A weighting function was included in the model.bservations with larger magnitudes were given lesseight. This was necessary because higher magnitudeeasurements were more imprecise. The weights were
stimated as:
1
|pitch|�
here � was estimated approximately as 0.771 and
pitch” denotes the true or actual pitch. The function bDIGITAL HEAD POSTUREOL. 147, NO. 6
elating the observed measurement to the true measure-ents was:
measured pitch � 0.003 � 0.850 true pitch
he 95% confidence interval for the slope was from 0.843o 0.857 and the 95% confidence interval for the interceptas from -0.146 to 0.151. There was very little subjecteterogeneity–the standard deviation of the random inter-ept was 0.170. The measurement error standard deviations a function of true pitch:
�0.2052|pitch|2�0.771
he results indicate that measured pitch has a nonconstant
ias, and the bias changes linearly with size of the rotation.MEASURING SYSTEM 1100.e1

DDtI
1
Biosketch
ongsheng Yang, PhD, is an Assistant Professor of Ophthalmology and Bioengineering at the University of Pittsburgh andirector of the Laboratory of Ocular Motor Research in the Department of Ophthalmology. Dr Yang has published more
han 30 research papers and 2 book chapters in the field of vision research. His research has been supported by Nationalnstitute of Health. Dr Yang research interest is focused on ocular motility.
AMERICAN JOURNAL OF OPHTHALMOLOGY100.e2 JUNE 2009
EpDcSm
V
Biosketch
ric S. Hald is a Senior Bioengineering student at the University of Pittsburgh. He has been a Research Assistant for theast two years in the Laboratory of Ocular Motor Research in Children’s Hospital of Pittsburgh, under the direction ofrs Dongsheng Yang and Richard Hertle. Mr Hald has presented posters at the AAPOS 2007 and ARVO 2008
onferences, detailing his various stages of work with a digital head posture measuring device. He received Fight-For-ight’s Summer Research Fellowship Grant for Summer 2008 to continue his research in developing a head postureeasuring device. His career interests include pediatric and ophthalmologic medicine.
DIGITAL HEAD POSTURE MEASURING SYSTEMOL. 147, NO. 6 1100.e3