diabetes mellitus what's new and what hasn't changed martin c. young md pediatric...
TRANSCRIPT


Diabetes MellitusDiabetes MellitusWhat's new and what hasn't changedWhat's new and what hasn't changed
Martin C. Young MDMartin C. Young MDPediatric EndocrinologistPediatric Endocrinologist
Pediatric Specialized CarePediatric Specialized CareRapides Medical Center, Alexandria LARapides Medical Center, Alexandria LA

Defining Diabetes Mellitus (DM)Defining Diabetes Mellitus (DM)
Chronic hyperglycemiaChronic hyperglycemia Acute complicationsAcute complications Chronic complicationsChronic complications
– macrovascularmacrovascular– microvascularmicrovascular– otherother


Types of DMTypes of DM
Type 1Type 1 Type 2Type 2 OtherOther

Type 1 & Type 2 DMType 1 & Type 2 DM
Type 1 (IDDM)Type 1 (IDDM)– childhood infection of pancreas resulting childhood infection of pancreas resulting
in autoimmune destruction and loss of in autoimmune destruction and loss of insulininsulin
– insulin insulin dependentdependent Type 2 (NIDDM)Type 2 (NIDDM)
– insulin resistance leading to pancreatic insulin resistance leading to pancreatic exhaustionexhaustion
– insulin insulin requiringrequiring (often) (often)

DM is Common 1DM is Common 1
PrevalencePrevalence– world: 150 millionworld: 150 million– USA: 20 million (6% population)USA: 20 million (6% population)
1/3 all cases undiagnosed1/3 all cases undiagnosed High risk groupsHigh risk groups
– AfroAmerican x2AfroAmerican x2– Hispanic x2Hispanic x2– American Native x5American Native x5

DM is Common 2DM is Common 2
10% of people aged >20 yrs10% of people aged >20 yrs 20% of people aged >60 yrs20% of people aged >60 yrs USA 1997-2004 increase across ages USA 1997-2004 increase across ages
18-80 approx 40%18-80 approx 40%


DM is ExpensiveDM is Expensive
US costs per annum >$ 100 billionUS costs per annum >$ 100 billion


Diagnosing DMDiagnosing DM
Your patient has DM until otherwise Your patient has DM until otherwise proven!proven!
http://www.diabetes.orghttp://www.diabetes.org


OGTT 1OGTT 1

Prediabetes Prediabetes
Impaired fasting glucose (IFG)Impaired fasting glucose (IFG)– FBG 100-125 mg/dlFBG 100-125 mg/dl
Impaired glucose tolerance (IGT)Impaired glucose tolerance (IGT)– BG 140-199 mg/dl at 2 hours on OGTTBG 140-199 mg/dl at 2 hours on OGTT
IFG & IGT are not benignIFG & IGT are not benign

OGTT 2OGTT 2

Risk for Death by Fasting and 2-hour Risk for Death by Fasting and 2-hour Blood Glucose LevelBlood Glucose Level
<6.1 6.1–6.9 7.0
11.1
7.8–11.0
<7.8
Fasting plasma glucose (mmol/l) 2-ho
ur p
lasm
a gl
ucos
e
(mm
ol/l)
2.5
2.0
1.5
1.0
0.5
0.0
Haz
ard
rat
io
Adjusted for age, center, sexDECODE Study Group. Lancet 1999;354:617–621

THE FUNAGATA DIABETES STUDY
Impaired Glucose Tolerance is a CV Risk Factor
Tominaga M, et al. Impaired glucose tolerance is a risk factor for cardiovascular disease, but not impaired fasting glucose. Diabetes Care1999;22:920-4.
NormalIGT (2 hr PG 140-200)DM (2 hr PG >200)
1.00
Cumulative Cardiovascular Survival
0.99
0.98
0.97
0.96
0.95
0.94
0
1.00
0.98
0.96
0.94
0.92
0
NormalIFG (FPG 110-126)DM (FPG >126)
0 1 2 3 4 5 6 7 0 1 2 3 4 5 6 7
Year Year

Values to RememberValues to Remember
Fasting blood glucose >100 mg/dlFasting blood glucose >100 mg/dl– think "pre-diabetes" (IFG)think "pre-diabetes" (IFG)
Random blood glucose > 140 mg/dlRandom blood glucose > 140 mg/dl– think "prediabetes" (IGT)think "prediabetes" (IGT)
Blood glucose > 200 mg/dl at any Blood glucose > 200 mg/dl at any timetime– think "diabetes"think "diabetes"

How DM Presents 1How DM Presents 1
Classic symptomsClassic symptoms– polydipsia & polyuriapolydipsia & polyuria– weight lossweight loss
AccidentallyAccidentally– urinalysisurinalysis– random blood glucoserandom blood glucose
SuspiciouslySuspiciously– recurrent candidiasisrecurrent candidiasis

How DM Presents 2How DM Presents 2
ScreeningScreening– asymptomaticasymptomatic– high risk groupshigh risk groups

Screening for DM 1Screening for DM 1
Aged >45 yrsAged >45 yrs Aged <45 yrs, fat plus other risk Aged <45 yrs, fat plus other risk
factorfactor– 11stst degree relative with diabetes degree relative with diabetes– physically inactivephysically inactive– high risk ethnic grouphigh risk ethnic group– hypertensionhypertension– dyslipidemiadyslipidemia

Screening for DM 2Screening for DM 2
– PCOSPCOS– IFG or IGT on OGTT previouslyIFG or IGT on OGTT previously– Acanthosis nigricansAcanthosis nigricans– Vascular diseaseVascular disease

Screening for DM 3Screening for DM 3
Fasting blood glucoseFasting blood glucose OGTT (2 hr)OGTT (2 hr)
Suspicious of DM?Suspicious of DM?
Random blood glucoseRandom blood glucose Fasting blood glucoseFasting blood glucose OGTTOGTT HbA1c (glycated hemoglobin)HbA1c (glycated hemoglobin) Fructosamine (glycated albumin)Fructosamine (glycated albumin) GlycoMark (1,5-Anhydroglucitol)GlycoMark (1,5-Anhydroglucitol)
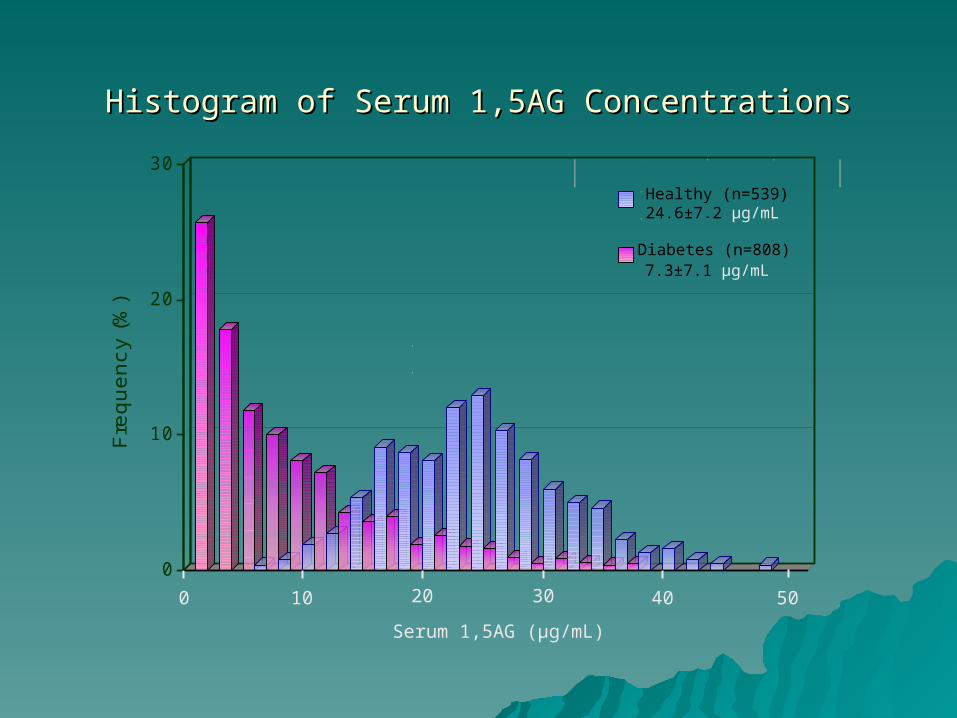
Histogram of Serum 1,5AG ConcentrationsHistogram of Serum 1,5AG Concentrations
0
10
20
30
Fre
qu
en
cy
(%)
Healthy (n=539)24.6±7.2 µg/mL
Diabetes (n=808) 7.3±7.1 µg/mL
0 10 20 30 40 50
Serum 1,5AG (µg/mL)

Diabetes & FriendsDiabetes & Friends
Associated Associated syndromessyndromes
ComorbiditiesComorbidities
"You're never "You're never alone with alone with diabetes"diabetes"

Syndromes Associated with Type 2 Syndromes Associated with Type 2 DMDM
Metabolic syndrome (MS)Metabolic syndrome (MS) Polycystic ovarian syndrome (PCOS)Polycystic ovarian syndrome (PCOS) Obstructive sleep apnea syndrome Obstructive sleep apnea syndrome
(OSAS)(OSAS)

Metabolic Syndrome (MS)Metabolic Syndrome (MS)
ObesityObesity HypertensionHypertension DyslipidemiaDyslipidemia Acanthosis nigricansAcanthosis nigricans Abnormal glucose homeostasisAbnormal glucose homeostasis
A prothrombotic, proinflammatory, atherogenic, endothelial A prothrombotic, proinflammatory, atherogenic, endothelial dysfunctional condition.dysfunctional condition.

Acanthosis Nigricans 1Acanthosis Nigricans 1

Acanthosis Nigricans 2Acanthosis Nigricans 2

Overlap of Type 2 DM and MS

Polycystic Ovarian SyndromePolycystic Ovarian Syndrome
(Polycystic ovaries)(Polycystic ovaries) Hyperandrogenemia or hirsuitismHyperandrogenemia or hirsuitism Menstrual disturbanceMenstrual disturbance

MS, DM, PCOS OverlapMS, DM, PCOS Overlap
The "full catastrophe"

OSASOSAS
Obstructive apnea during sleep due Obstructive apnea during sleep due to airway occlusion from obesityto airway occlusion from obesity
Recurrent hypoxemiaRecurrent hypoxemia– pulmonary hypertensionpulmonary hypertension– RV strain failureRV strain failure
Recurrent arousal from sleepRecurrent arousal from sleep– daytime fatigue, etcdaytime fatigue, etc
HypertensionHypertension Atrial fibrillationAtrial fibrillation

Why PCOS, MS & OSAS are Why PCOS, MS & OSAS are Related to Type 2 DMRelated to Type 2 DM
Insulin resistanceInsulin resistance– causes PCOS and Type 2 DMcauses PCOS and Type 2 DM– can result from OSAScan result from OSAS
HyperinsulinismHyperinsulinism– hypertensionhypertension– dyslipidemiadyslipidemia– acanthosis nigricansacanthosis nigricans– ovarian production of androgensovarian production of androgens

Non-alcoholic Fatty Liver Disease 1Non-alcoholic Fatty Liver Disease 1
NAFLD (non-alcoholic steatohepatitis, NAFLD (non-alcoholic steatohepatitis, NASH)NASH)
Fatty infiltration of liver assocaited Fatty infiltration of liver assocaited with obesity, MS and Type 2 DMwith obesity, MS and Type 2 DM
May progress to cirrhosisMay progress to cirrhosis

Non-alcoholic Fatty Liver Disease 2Non-alcoholic Fatty Liver Disease 2

Type 2 DMType 2 DM
• 90 % of all diabetes mellitus90 % of all diabetes mellitus• 99% all adult diabetes99% all adult diabetes• Approaching 30-50% of all childhood Approaching 30-50% of all childhood
diabetesdiabetes• Formally very rare in childrenFormally very rare in children• Profoundly underdiagnosed – "silent"Profoundly underdiagnosed – "silent"• A disease of genes interacting with the A disease of genes interacting with the
"Western Way" of overeating and "Western Way" of overeating and underexercisingunderexercising
Type 2 DM Type 2 DM PathophysiologyPathophysiology
• Key concept I: Key concept I: insulin resistanceinsulin resistance– geneticgenetic– obesityobesity– inactivityinactivity– OSASOSAS
• Key concept II: Key concept II: glycemic loadglycemic load– high glycemic index (GI) foodshigh glycemic index (GI) foods

Insulin ResistanceInsulin Resistance

Bad Genes & Bad Bad Genes & Bad ChoicesChoices

Progression of Type 2 Progression of Type 2 DMDM
PhasePhase InsulinInsulin GlucoseGlucose
11 NN22 IGTIGT
33 IFGIFG
44 NN DM -oral DM -oral medsmeds
55 DM -insulinDM -insulin

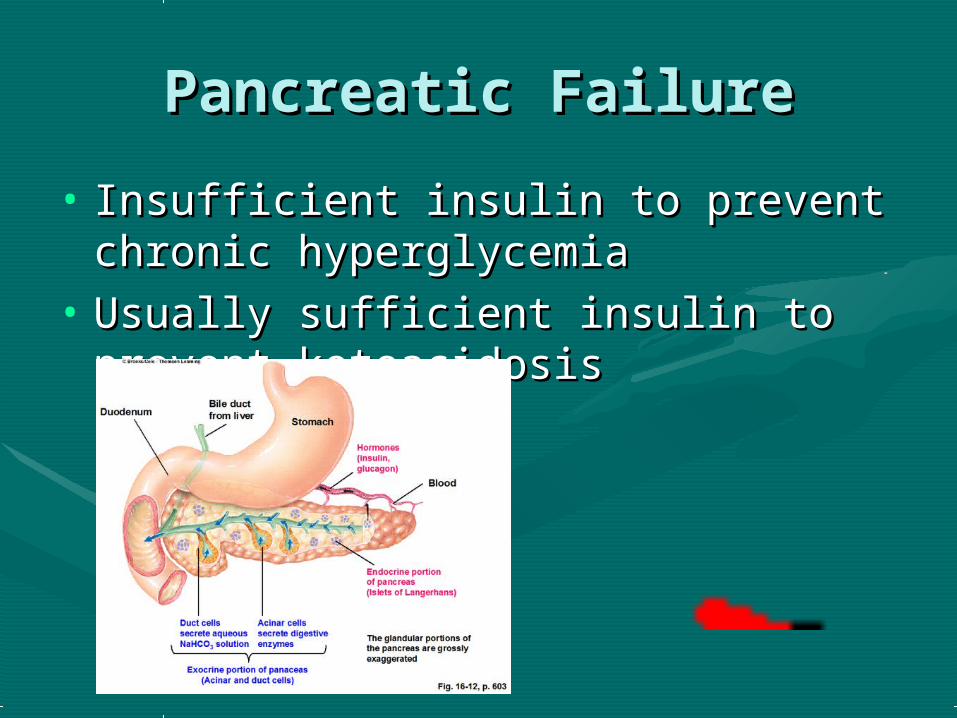
Pancreatic FailurePancreatic Failure
• Insufficient insulin to prevent Insufficient insulin to prevent chronic hyperglycemiachronic hyperglycemia
• Usually sufficient insulin to prevent Usually sufficient insulin to prevent ketoacidosisketoacidosis


Look for Comorbidities!Look for Comorbidities! Complications of DMComplications of DM
– eye diseaseeye disease– vascular diseasevascular disease– neuropathyneuropathy– nephropathynephropathy– dermatopathydermatopathy
Associated syndromesAssociated syndromes– MSMS– PCOSPCOS– OSASOSAS– NAFLD/NASHNAFLD/NASH

Eye DiseaseEye Disease
RetinopathyRetinopathy CataractsCataracts

Vascular DiseaseVascular Disease
Peripheral arterial diseasePeripheral arterial disease Ischemic heart diseaseIschemic heart disease Cerebral vascular diseaseCerebral vascular disease

NeuropathyNeuropathy
Peripheral sensory neuropathyPeripheral sensory neuropathy

NephropathyNephropathy
Urine microalbuminUrine microalbumin

DermatopathyDermatopathy
Diabetic ulceration & ischemiaDiabetic ulceration & ischemia NecrobiosisNecrobiosis Granuloma annulareGranuloma annulare
Associated Syndromes 1Associated Syndromes 1
MSMS– acanthosis nigricansacanthosis nigricans– obesityobesity– hypertensionhypertension
PCOSPCOS– hirsuitismhirsuitism– menstrual irregularitymenstrual irregularity– acneacne

Associated Syndromes 2Associated Syndromes 2
OSASOSAS– snoringsnoring– restless sleeprestless sleep– night sweatsnight sweats– daytime fatigue/headachedaytime fatigue/headache
NAFLD/NASHNAFLD/NASH– hepatomegalyhepatomegaly

Tests for the Newly Diagnosed Tests for the Newly Diagnosed DM patient 1DM patient 1
Eye examEye exam ABI (doppler)ABI (doppler) Filament test (nerve conduction)Filament test (nerve conduction) UrineUrine
– glucoseglucose– ketonesketones– microalbuminmicroalbumin

Tests for the Newly Diagnosed Tests for the Newly Diagnosed DM patient 2DM patient 2
BloodBlood– lipid panellipid panel– LFTsLFTs– TSHTSH– HbA1c, fructosamine, GlycoMarkHbA1c, fructosamine, GlycoMark
Uncertain Type 2 vs. Type 1 DM?Uncertain Type 2 vs. Type 1 DM?– fasting insulin fasting insulin – diabetes autoimmune screening panel.diabetes autoimmune screening panel.

Treatment of Type 2 DMTreatment of Type 2 DM
Treatment of complications and Treatment of complications and comorbiditiescomorbidities
Medical nutrition therapy (MNT)Medical nutrition therapy (MNT) Therapeutic exercise (TE)Therapeutic exercise (TE) Oral hypoglycemicsOral hypoglycemics InjectiblesInjectibles
– insulininsulin– otherother

Treatment - ObesityTreatment - Obesity
Appetite suppressantsAppetite suppressants Orlistat (Xenical)Orlistat (Xenical) MNT to produce loss of fatMNT to produce loss of fat Bariatric sugeryBariatric sugery

Treatment - HypertensionTreatment - Hypertension
AntihypertensivesAntihypertensives– ACE inhibitorsACE inhibitors– othersothers

Treatment - dyslipidemiaTreatment - dyslipidemia
Antihyperlipidemic Antihyperlipidemic drugsdrugs– statinsstatins– otherother

Treatment – MSTreatment – MS
AspirinAspirin StatinsStatins MNTMNT

Treatment - PCOSTreatment - PCOS
OCPOCP SpironolactoneSpironolactone MNTMNT OtherOther

OSASOSAS
Tonsillectomy & Tonsillectomy & adenoidectomyadenoidectomy
Nasal CPAPNasal CPAP MNT for fat loss.MNT for fat loss.
Treatment - NephropathyTreatment - Nephropathy
ACE inhibitorsACE inhibitors MNT – protein MNT – protein
restrictionrestriction

Treatment – Eye DiseaseTreatment – Eye Disease
Cataract removalCataract removal Laser surgery for Laser surgery for
retinopathyretinopathy

Treatment - NASHTreatment - NASH
Alchohol restrictionAlchohol restriction AntihyperlipidemicAntihyperlipidemic
ss Vitamin EVitamin E MNT MNT

Medical Nutrition Medical Nutrition TherapyTherapy
• TraditionalTraditional• Non-traditionalNon-traditional

MNT – Traditional 1MNT – Traditional 1
• "Low fat/ high carb "Low fat/ high carb diet"diet"– CHO 45-65% of CHO 45-65% of
caloriescalories– PROT 10-35%PROT 10-35%– FAT 20-35%FAT 20-35%– high fiberhigh fiber– low sodiumlow sodium– low cholesterol (<200 low cholesterol (<200
mg/d)mg/d)– low saturated fat low saturated fat
(<7% calories)(<7% calories)

MNT – Traditional 2MNT – Traditional 2
• For obese patientsFor obese patients– calorie restrictioncalorie restriction
• women 1000-1200kcal/dwomen 1000-1200kcal/d• men 1200-1600 kcal/dmen 1200-1600 kcal/d
– aim for 20-30 lb weight loss total @ 1-2 aim for 20-30 lb weight loss total @ 1-2 lbs/weeklbs/week
• EffectivenessEffectiveness– improves glycemic controlimproves glycemic control– reduces BPreduces BP– improves dyslipidemiaimproves dyslipidemia– little weight loss – typically 4 lbs after 1 yearlittle weight loss – typically 4 lbs after 1 year

MNT – Nontraditional 1MNT – Nontraditional 1
• Low CHO <130g/d (often <80g/d)Low CHO <130g/d (often <80g/d)• Low glycemic index (LGI)Low glycemic index (LGI)• VegetarianVegetarian• Stone ageStone age

Therapeutic ExerciseTherapeutic Exercise
• Aerobic exerciseAerobic exercise– at least 30 mins x3/weekat least 30 mins x3/week

Drug TherapyDrug Therapy
Oral HypoglycemicsOral Hypoglycemics Parenteral medicationsParenteral medications Inhaled insulinInhaled insulin

Oral Hypoglycemics 1Oral Hypoglycemics 1

Oral Hypoglycemics 2Oral Hypoglycemics 2
SecretagoguSecretagoguesesmost useful early most useful early
onon
SulfonylureasSulfonylureas– glyburide (Diabeta)glyburide (Diabeta)– glipizide (Glucotrol)glipizide (Glucotrol)– glimepiride glimepiride
(Amaryl)(Amaryl)
MeglitanidesMeglitanides– repagliniderepaglinide

Oral Hypoglycemics 3Oral Hypoglycemics 3
Insulin Insulin sensitizerssensitizers
BiguanidesBiguanides– metforminmetformin
ThiazolidinedionesThiazolidinediones– pioglitazone (Actos)pioglitazone (Actos)– rosiglitazone rosiglitazone
(Avandia)(Avandia)– troglitazone troglitazone
(Rezulin)(Rezulin)

Oral Hypoglycemics 4Oral Hypoglycemics 4
Absorbtion Absorbtion blockersblockers
glucosidase glucosidase inhibitorsinhibitors– miglitol (Glyset)miglitol (Glyset)– acarbose (Precose)acarbose (Precose)

Oral Hypoglycemics 5Oral Hypoglycemics 5
Combination Combination drugsdrugs
GlucovanceGlucovance– metfrominmetfromin– glyburideglyburide
MetaglipMetaglip– metformin metformin – glipizideglipizide
Oral Hypoglycemics 6Oral Hypoglycemics 6
Each drug lowers Each drug lowers HbA1c by HbA1c by
approximately 1-approximately 1-2%2%

Oral Hypoglycemics 7Oral Hypoglycemics 7
Polypharmacy is the rulePolypharmacy is the rule Most patients are going to be on at Most patients are going to be on at
least two drugsleast two drugs Use drugs from different groupsUse drugs from different groups
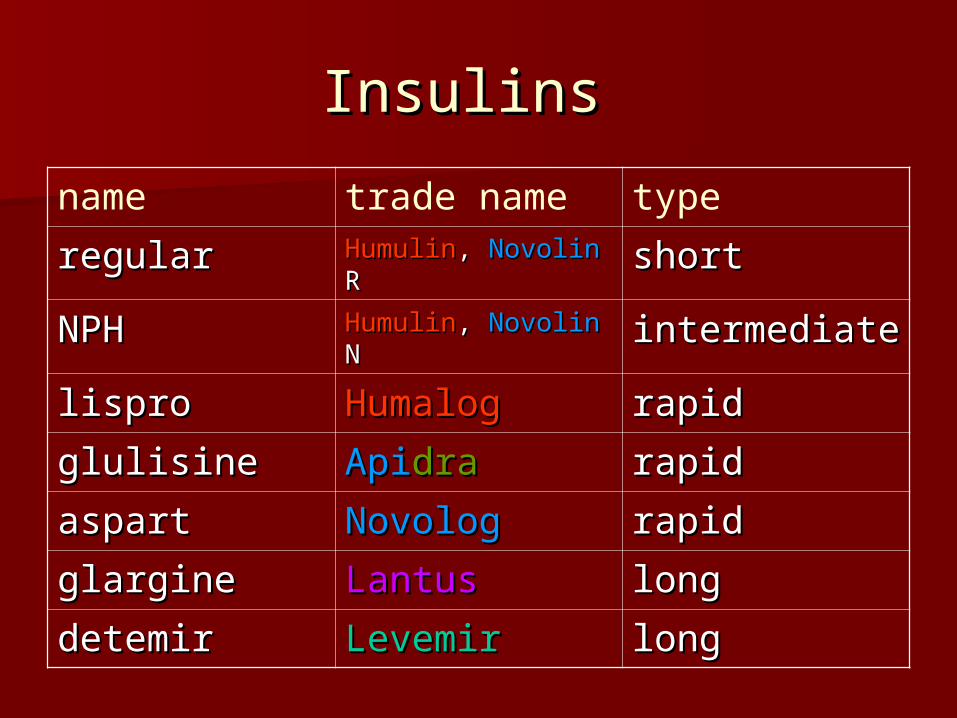
Insulins Insulins
name trade name type
regularregular HumulinHumulin, , NovolinNovolin R R shortshort
NPHNPH HumulinHumulin, , NovolinNovolin N N intermediateintermediate
lisprolispro HumalogHumalog rapidrapid
glulisineglulisine ApiApidradra rapidrapid
aspartaspart NovologNovolog rapidrapid
glargineglargine LantusLantus longlong
detemirdetemir LevemirLevemir longlong

Insulin ProfilesInsulin Profiles

Regular & NPH InsulinsRegular & NPH Insulinspeak actions: R ~ 3 hrs, N ~ 6 hrs

Rapid Acting InsulinsRapid Acting Insulins
peak action: ~ 1 hr


LantusLantus
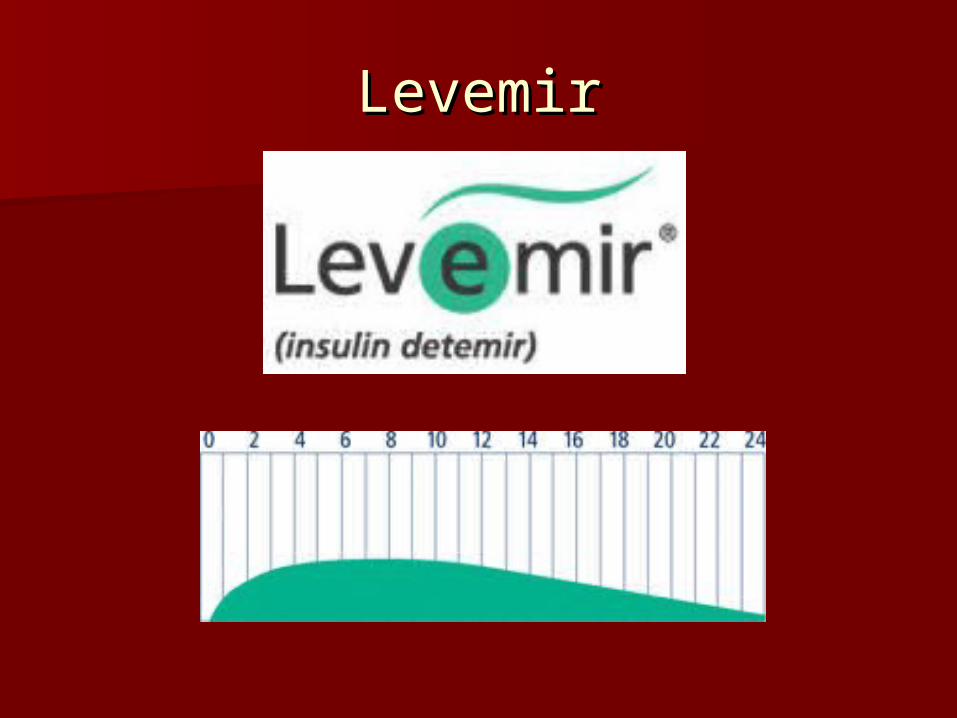
LevemirLevemir

Mixed InsulinsMixed Insulins
HumulinHumulin
HumalogHumalog
NovologNovolog
70/3070/30 50/5050/50
75/2575/25 50/5050/50
70/3070/30

Insulin Delivery Devices 1Insulin Delivery Devices 1
PensPens– disposabledisposable– rechargablerechargable

Insulin Delivery Devices 2Insulin Delivery Devices 2

Insulin Delivery Devices 3Insulin Delivery Devices 3

Inhaled InsulinInhaled Insulin
ExuberaExubera

Other Injectable Drugs 1Other Injectable Drugs 1
Exenatide (Byetta)Exenatide (Byetta)– insulin insulin
secretagoguesecretagogue– peptidepeptide– gila monster salivagila monster saliva– use with other use with other
drugsdrugs– no hypoglycemiano hypoglycemia– bidbid

Other Injectable Drugs 1Other Injectable Drugs 1
Pramlintide (Symlin)Pramlintide (Symlin)– analogue of analogue of
hormone amylinhormone amylin– polypetidepolypetide– slows gastric slows gastric
emptyingemptying– induces satietyinduces satiety– opposes glucagonopposes glucagon
reduces posprandial reduces posprandial BGBG
– give with mealsgive with meals used with insulin

Traditional Rx of Type 2 DMTraditional Rx of Type 2 DM
Step 1Step 1: MNT &TE: MNT &TE Step 2Step 2: 1: 1stst drug drug Step 3Step 3: 2: 2ndnd drug drug Step 4Step 4: 3: 3rdrd drug drug Step 5Step 5: insulin: insulin
Each step added as Each step added as satisfactory HbA1c satisfactory HbA1c is not achieved by is not achieved by the preceding the preceding
Very slow process Very slow process over months to over months to yearsyears

Modern "Aggressive" Rx of Modern "Aggressive" Rx of Type 2 DM from Time of Type 2 DM from Time of
DiagnosisDiagnosis HbA1c > 10 % HbA1c > 10 %
– oror FPG >260 mg/dlFPG >260 mg/dl
– oror SymptomaticSymptomatic
– oror KetoticKetotic
IMMEDIATE IMMEDIATE INSULININSULIN

Modern "Aggressive" Rx 2Modern "Aggressive" Rx 2
HbA1c 8-10 %HbA1c 8-10 %
– e.g Glucovancee.g Glucovance 2.5/500 bid2.5/500 bid max 20/2000 per max 20/2000 per
dayday
Immediate Immediate combination oral combination oral hypoglycemic drughypoglycemic drug
Titrate dose up Titrate dose up rapidly every rapidly every month using short month using short term markers of term markers of controlcontrol

Modern "Aggressive" Rx 3Modern "Aggressive" Rx 3
HbA1c < 8%HbA1c < 8% Monotherapy with Monotherapy with drug of choicedrug of choice
Titrate dose up Titrate dose up rapidly every rapidly every month using short month using short term markers of term markers of controlcontrol
Add further drugs Add further drugs (different actions) if (different actions) if necessarynecessary

Modern "Aggressive" Rx 4Modern "Aggressive" Rx 4
HbA1c not < 7% by HbA1c not < 7% by 6 months6 months Start Start
InsuliInsulinn

Insulin Regimens for Type 2 Insulin Regimens for Type 2 DMDM
Step one: once Step one: once daily long actingdaily long acting– LevemirLevemir– LantusLantus
Step two: mixed Step two: mixed insulin at breakfastinsulin at breakfast
Step three: mixed Step three: mixed insulin at supperinsulin at supper
etc. etc.
Titrate to fasting Titrate to fasting blood glucoseblood glucose

Assessing Rx SuccessAssessing Rx Success
Measures of glycemic controlMeasures of glycemic control– HbA1cHbA1c– fructosaminefructosamine– GlycoMarkGlycoMark– self monitoring of blood glucose (SMBG)self monitoring of blood glucose (SMBG)

Measures of Glycemic ControlMeasures of Glycemic Control
1,5AGFructosamine
10 89 7 56 4 3 12 0
HbA1C
Bloodglucose
Weeks before measurement

Glycated Hemoglobin (HbA1c) 1Glycated Hemoglobin (HbA1c) 1

Glycated Hemoglobin (HbA1c) 2Glycated Hemoglobin (HbA1c) 2

Glycated Hemoglobin (HbA1c) 3Glycated Hemoglobin (HbA1c) 3
FructosamineFructosamine

GlycoMark GlycoMark
Oral Supply1,5AG
(5-10mg/day)
Blood stream
TissuesInternal Organs
(500-1000 mg)
Kidney
Urinary excretion
(5-10mg/day)
Oral Supply1,5AG
(5-10mg/day)
Blood Stream(1,5-AG
LevelLower)
TissuesInternal Organs
(500-1000 mg)
Kidney
Urinary excretion (INCREASED)
Normoglycemia Hyperglycemia
GlucoseBlocks
Reabsorption

SMBGSMBG
Value in Type 2 DM Value in Type 2 DM not established not established
Useful for titrating Useful for titrating insulininsulin

SummarySummary
Increasing prevalence of Type 2 DMIncreasing prevalence of Type 2 DM Diagnostic criteria for DM, IGT, IFGDiagnostic criteria for DM, IGT, IFG Screening for DMScreening for DM Comorbidities & associated Comorbidities & associated
syndromessyndromes Aggressive Rx of Type 2 DMAggressive Rx of Type 2 DM New insulinsNew insulins New measures of glycemic controlNew measures of glycemic control