directorate of integrated child development services … 2012- 13 _final (mp).pdf2018-02-09asha awtc...
TRANSCRIPT

i
Directorate of Integrated Child Development Services
Madhya Pradesh
ii
CONTENTS
S.No. Subject Page
no.
List of annexure III
List of Tables IV
Abbreviations V
Section 1: Situation and Gap Analysis
a) Socio-economic and demographic profile of Madhya Pradesh
1-5
i. Administrative divisions
ii. Demography
iii. Vital Statistics in M.P.
iv. Socio-economic profile
v. Human development in MP
vi. Literacy rates
vii. Health profile
viii. Access to safe drinking water and sanitation
ix. Nutritional status of women and children
x. Road connectivity
b) Nutrition Policy of Madhya Pradesh 5
c) Inter-sectoral convergence for program implementation 6
d) Nutrition and health status of women and children 7
e) History of ICDS in Madhya Pradesh - Total number of ICDS
projects in the state
10
f) State’s financial contribution to ICDS implementation 11
g) Infrastructure status of operational AWC buildings 11
h) Status of operationalization of projects, AWCs and Mini-AWCs 13
i) Trends in coverage of beneficiaries for supplementary nutrition
and pre-school education
15
j) Training infrastructure –AWTCs, MLTCs 17
k) Major gaps/ constraints in program implementation 17
l) Initiatives taken by government of Madhya Pradesh for ICDS
programme
19
Section 2: VISION STATEMENT 26
Section 3: ORGANISATIONAL STRUCTURE OF ICDS PROGRAM
MANAGEMENT- STATE & DISTRICT LEVEL
27
Section 4: ANNUAL ACTION PLAN- PROGRAM COMPONENTS
4A Human Resources 32
4B Procurement of Materials and Equipment 36
4C Delivery of Services at AWCs 39
C1 Supplementary Nutrition (SN) 39
C2 Preschool Education (PSE) 46
C3 Nutrition and Health Education 50
C4 Immunization 52
C5 Health check-ups 52
C6 Referral Services 55
iii
4D Observation of Nutrition and Health Days 56
4E Information Education and Communication 57
4F Monitoring and Evaluation 61
4G Training and capacity building 63
4H Convergence with Line departments 64
4I Community Participation and Involvement of PRIs
65
a) Existing mechanism for community participation
b) Percent of AWCs participated in Gram Sabha meeting
c) AWC received any support from Panchayat
d) Gram Panchayat meetings attended by AWW
e) Percent of Panchayat Samiti meetings attended by AWWs
f) No. of districts where the Zila Parishads reviewed ICDS
program
4J Financial Management and Fund Flow Mechanism 67
4K New Initiatives to Strengthen ICDS Program during 2011-12 68
Summary of Action Plan (2012-13) 73
Budget Annual PIP (2012-13)
Time line of Activities (2012-13) 70
Section 5 : ADDITIONAL INFORMATION 74-82
Annexures 83-98
List of Annexure
1. Nutritional status of children in 50 districts (NIN 2010)
2. District-wise Rural, Tribal and Urban projects and AWCs
3. New government population norms for establishing AWCs
4. AWTCs and MLTCs in the state
5. District-wise number of NRCs
6. Training Calendar (2012-13)
7. Proposal for Annual Training Activity (2012-13)
8. Statement of Expenditure
iv
Abbreviations Used
AACP
ABM
ACCTO
ACDPO
ANC
ANM
AO
ASO
APIP
ASHA
AWTC
AWCs
AWWs
AWH
AYUSH
BALA
BCC
BPL
BPNI
BRGF
CARE
CBO
CDPO
CHC
CM
CMHO
DAP
DFID
DPHFW
Dept P&T
DLHS
DPC
DPM
DPO
DWCD
EBF
ECE
FY
GOI
GoMP
Adolescent Anemia Control Programme
Atal Bal Mission
Assistant Accounts Officers
Assistant Child Development Project Officer
Antenatal Care
Auxiliary Nurse Midwife
Accounts Officer
Assistant Statistical Officer
Annual Programme Implementation Plan
Accredited Social Health Activist
Anganwadi Training Centres
Anganwadi Centres
Anganwadi Worker
Anganwadi helper
Ayurved Unani Siddha Homeopathy
Building As Learning Aid
Behavior Change Communication
Below Poverty Line
Breast Feeding Network of sIndia
Backward Region Grant Fund
Cooperation for American Relief Everywhere
Community Based Organizations
Child Development Project Officer
Community Health Centre
Chief Minister
Chief Medical & Health Officer
District Action Plan
Department For International Development Department of Public Health and Family Welfare
Department of Post & Telegraph
District Level Health Survey
Departmental Promotion Committee
District Program Manager
District Program Officer
Department of Women and Child Development
Exclusive Breast Feeding
Early Childhood Education
Financial Year
Government of India
Government of Madhya Pradesh

v
Abbreviations Used
HFW
HR
IAP
IAS
ICDS
IDD
ICMR
IEC
IFA
IGMSY
IPC
IYCF
IYCN
KSY
LBW
LDC
LHV
LIC
MCPC
MHFW
MIS
MLTC
MMR
MO
MOU
MP
MP HSRP
MPLAD
MPR
MWCD
NGO
NFHS
NHE
NHED
NIN
NIPCCD
NIPI
NRC
NRHM
OBC
ORS
Health & Family Welfare
Human Resources
Indian Association of Pediatrics
Indian Administrative Service
Integrated Child Development Services
Iodine Deficiency Disorder
Indian Council of Medical Research
Information Education Communication
Iron Folic Acid
Indira Gandhi Matritva Sahogi Yojna
Inter Personal Communication
Infant and Young Child Feeding
Infant & Young Child Nutrition
Kishori Shakti Yojna
Low Birth Weight
Lower Divisional Clerk
Lady Health Visitor
Life Insurance Corporation
Mother & Child Protection Card
Ministry of Health & Family Welfare
Monitoring Information System
Middle Level Training Centre
Maternal Mortality Rate
Medical Officer
Memorandum of Understanding
Madhya Pradesh
Madhya Pradesh Health Sector Reform Programme
Member of Parliament Local Area Development
Monthly Progress Report
Ministry of Women and Child Development
Non Government Organization
National Family Health Survey
Nutrition & Health Education
Nutrition & Health Education
National Institute of Nutrition
National Institute of Public Cooperation and Child
Development
Norway India Partnership Initiative
Nutrition Rehabilitation Centre National Rural Health Mission
Other Backward Caste
vi
Abbreviations Used
PHC
PHFW
PIP
PRI
PSE
QPR
RCH
RUTF
SABLA
SAM
SC
SHG
SMS
SN
SNP
SPIP
SRC
SRS
SSA
ST
STRAP
TFR
THR
TLM
TNA
TSC
TV
U 5
UDC
U 5 MR
UNICEF
UT
USI
UN MDG
VAS
VHND
VHSC
WCD
WHO
Oral Dehydration Salt
Primary Health Centre
Public Health & Family Welfare
Project Implementation Plan
Panchayati Raj Institutions
Pre-school Education
Quarterly Progress Report
Reproductive Child Health
Ready to Use Therapeutic Food
Rajiv Gandhi Scheme for Empowerment of Adolescent Girls
Severe Acute Malnutrition
Scheduled castes
Self Help Groups
Sahyogini Matru Samiti
Supplementary Nutrition
Supplementary Nutrition Programme
State Programme Implementation Plan
State Resource Centre
Sample Registration Survey
Sarva Shiksha Abhiyan
Scheduled Tribes
State Training Action Plan
Total Fertility Rate
Take Home Ration
Teaching Learning Material
Training Need Assessment
Total Sanitation Caimpaign
Television
Under five
Upper Divisional Clerk
Under Five Mortality Rate
United Nations Children Fund
Union Territories
Universal Salt Iodization
United Nations Millennium Development Goals
Vitamin A Supplementation
Village Health & Nutrition Day
Village Health & Sanitation Committee
Women and Child Development
World Health Organization

1
SECTION- 1 SITUATION AND GAP ANALYSIS
a) Socio-economic and demographic profile of Madhya Pradesh
Madhya Pradesh, as the name indicates, is geographical heart of the Republic of India. It is
surrounded on the south by Maharastra, on the west by Gujarat, on the northwest by
Rajasthan, on the north by Uttar Pradesh, and on the east by Chattisgarh.
Madhya Pradesh, with total area of 308,245 sq. km, is the second largest state of India. It
has five distinct cultural regions – Bundelkhand, Baghelkhand, Rewanchal, Malwa and
Mahakoshal. The state, therefore, presents a fascinating mosaic of culture and regional
languages.
i. Administrative units in the state
The state comprises ten revenue divisions, 50 districts and 313 community development
blocks, including 89 tribal development blocks. The state’s 55,391, villages are covered by
22,029 Gram Panchayats. On an average a Gram Panchayat covers 2.5 revenue villages,
each village having an average population of 1090. A revenue village may consist of a
number of separate habitations known as tola, falia or majra, especially in tribal areas.
ii. Demography
The 2011 Census of India has recorded the State’s population as 72.6 million, out of this,
the rural population stands at 52.5million and the urban population 20.1 million. In absolute
numbers, the rural population has increased by 8.2million and the urban population by 4.1
million in the last decade. With about 6 percent of the total population of India, it is the
seventh most populous state in the country. The decadal growth of population during the
period 2001-2011 was 20.3%, which was significantly higher than the national average of
17.6%. The growth rate of population in rural and urban areas was 18.45 and 25.6%
respectively. The sex ratio in the state which was 919 in 2001 has risen by 11 points to 930
in 2011. The increase in rural areas has been 9 points from 927 to 936. The same in urban
areas has been 18 points from 898 to 916. The sex ratio in the state is comparatively lower
than that of India, 930 females per 1000 males in the state Vs. 940 at all India level
Out of the child population of 10.5 million in the age group of 0-6 in the state the rural child
population stands at 8.1 million and urban at 2.4 million in 2011. The child population has
declined by 0.2 million in the state – decline of 0.3 million in rural areas and increase of 0.1
million in urban areas.
In Madhya Pradesh, fall in child sex ratio in the age group of 0-6 years has reached 912.
The fall has been 20 points (932-912) for the state during 2001-2011.In rural areas the fall is
significant - 22 points (939-917) and in urban areas it is 12 points (907-895) over the last
decade.
The literacy rate of Madhya Pradesh as per 2011 Census is 70.6. In rural areas the literacy
rate is 65.3 and in urban areas it is 84.1. The male literacy rate which is 80.5 (Rual-76.6;
Urban-90.2) is higher than the female literacy rate of 60.0 (Rural-53.2; Urban-77.4).The gap
in literacy rate among males and females is 20.5 points in the state.

2
Table A. Demographic Profile of Madhya Pradesh
Madhya Pradesh
(Census 2011)
India
(Census, 2011)
Population Census (2011) 72,597,565* 1, 210,193,422
Male 37,612,920 (51.8%) 623,724,248
Female 34,984,645 (48.2%) 586,469,174
Sex Ratio( female / 1000 male) 930 940
Sex ratio (0-6 year) 912 914
Decadal growth rate of population
(%)
20.3 17.6
Density of population (per sq. km) 196 313
Scheduled caste population (%) 15.4 16.2
Scheduled tribe population (%) 20.3 8.2
Child Population 0-6years 10,548,295 (14.5%) 158,789,287(13.1%)
Child Population 0-6years ICDS# 9039076 (2010
population)
-
Child Population (Rural) ICDS 1160608 (2010
population)
-
Child Population (Urban) ICDS 5842939 (2010
population)
-
Child Population (Tribal) ICDS 2035529 (2010
population)
-
Literacy Rate
Total
Rural
Urban
70.6
65.3
84.2
74.0
68.9
84.9
Demographic data are from the Office of Census Commissioner and Registrar General
of India, New Delhi.
# projected population by Directorate, WCD
.
iii. Vital Statistics of Madhya Pradesh
Vital statistics of Madhya Pradesh are typical of a developing state with high burden of
mortality indicating poor state of health of the population. The state has the highest Infant
Mortality Rate, second highest Crude Death Rate and the third highest Maternal Mortality
Ratio in the country.
Table B. Vital Statistics Rates in Madhya Pradesh
Vital statistics rates (2007) Madhya Pradesh India
Crude Birth rate per 1000
population #
25.0 23.8
Crude Death rate per 1000
population #
8.0 7.5
IMR per1000 live births $ 67 50
IMR (Rural)$ 72 55
IMR (Urban)$ 45 34
IMR (Male)$ 66 49
IMR (Female)$ 68 52
Under 5 mortality rate (per 1000 live 89 98
3
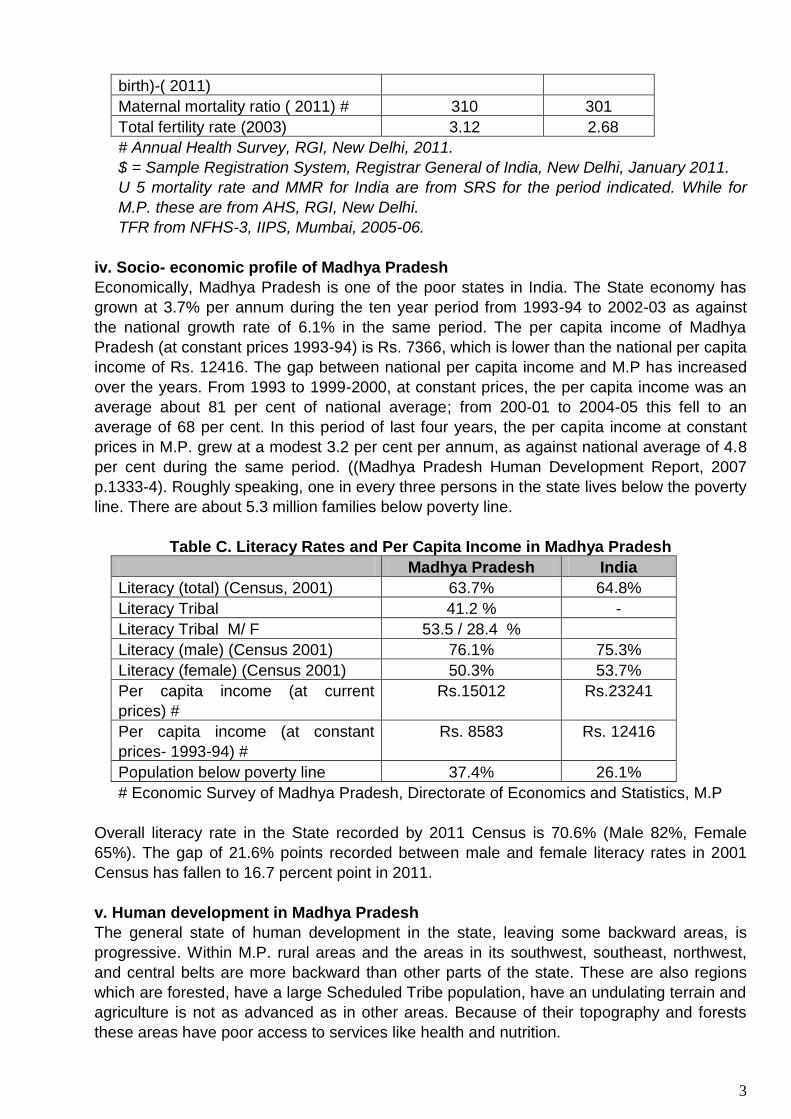
birth)-( 2011)
Maternal mortality ratio ( 2011) # 310 301
Total fertility rate (2003) 3.12 2.68
# Annual Health Survey, RGI, New Delhi, 2011.
$ = Sample Registration System, Registrar General of India, New Delhi, January 2011.
U 5 mortality rate and MMR for India are from SRS for the period indicated. While for
M.P. these are from AHS, RGI, New Delhi.
TFR from NFHS-3, IIPS, Mumbai, 2005-06.
iv. Socio- economic profile of Madhya Pradesh
Economically, Madhya Pradesh is one of the poor states in India. The State economy has
grown at 3.7% per annum during the ten year period from 1993-94 to 2002-03 as against
the national growth rate of 6.1% in the same period. The per capita income of Madhya
Pradesh (at constant prices 1993-94) is Rs. 7366, which is lower than the national per capita
income of Rs. 12416. The gap between national per capita income and M.P has increased
over the years. From 1993 to 1999-2000, at constant prices, the per capita income was an
average about 81 per cent of national average; from 200-01 to 2004-05 this fell to an
average of 68 per cent. In this period of last four years, the per capita income at constant
prices in M.P. grew at a modest 3.2 per cent per annum, as against national average of 4.8
per cent during the same period. ((Madhya Pradesh Human Development Report, 2007
p.1333-4). Roughly speaking, one in every three persons in the state lives below the poverty
line. There are about 5.3 million families below poverty line.
Table C. Literacy Rates and Per Capita Income in Madhya Pradesh
Madhya Pradesh India
Literacy (total) (Census, 2001) 63.7% 64.8%
Literacy Tribal 41.2 % -
Literacy Tribal M/ F 53.5 / 28.4 %
Literacy (male) (Census 2001) 76.1% 75.3%
Literacy (female) (Census 2001) 50.3% 53.7%
Per capita income (at current
prices) #
Rs.15012 Rs.23241
Per capita income (at constant
prices- 1993-94) #
Rs. 8583 Rs. 12416
Population below poverty line 37.4% 26.1%
# Economic Survey of Madhya Pradesh, Directorate of Economics and Statistics, M.P
Overall literacy rate in the State recorded by 2011 Census is 70.6% (Male 82%, Female
65%). The gap of 21.6% points recorded between male and female literacy rates in 2001
Census has fallen to 16.7 percent point in 2011.
v. Human development in Madhya Pradesh
The general state of human development in the state, leaving some backward areas, is
progressive. Within M.P. rural areas and the areas in its southwest, southeast, northwest,
and central belts are more backward than other parts of the state. These are also regions
which are forested, have a large Scheduled Tribe population, have an undulating terrain and
agriculture is not as advanced as in other areas. Because of their topography and forests
these areas have poor access to services like health and nutrition.
4
vi. Literacy The nineties was the defining decade in Madhya Pradesh in reduction of illiteracy. The
literacy rate in the state in 2011 was 70.63% (male 80.53 %, female 60.023%). The decadal growth in literacy rate in the state was 6.93% (Census 2001),
vii. Health Profile
Prevalence of communicable diseses like malaria, T.B. and diarrhoea is high. Diarrhoea is
an important cause of high infant mortality in the state, accounting for about 28% of all infant
deaths (Rajiv Gandhi Mission for Control of Diarrheal Diseases, Dept. of Health and Family
Welfare, GoMP, 2000). High prevalence of communicable diseases like malaria and
diarrhea among children and low level of immunization against vaccine preventable
diseases (reported later) are important etiological factors, among others, of malnutrition
among children.
IMR in the State has shown a continuous decline in recent years. But IMR of 67 per 1000
live births (SRS, Oct. 2009) is still ten percent point higher than the national rate of 57. The
NFHS III recorded the U5 mortality rate in MP as 94. Maternal Mortality Ratio, a sensitive
index of health of women in the reproductive age group, is 335 as against MMR of 254 at
national level.
Access of health services by women and children is poor. NFHS-3 reported low primary
immunization coverage among children. As per CES 2009 data, 43% of children below 23
months were fully immunized. Antenatal coverage, however, has increased from 61% to
81% between NFHS-2 and NFHS-3. The institutional delivery rate has also increased from
22 to 30 per cent during the same period.
The state government has taken a number of initiatives to increase institutional delivery,
which is expected to reduce maternal mortality ratio in the state in coming years. Institutional
delivery and immunization coverage (children fully immunized) rates in the state are 81.1 %
and 42.97 % respectively. (CES, 2009).
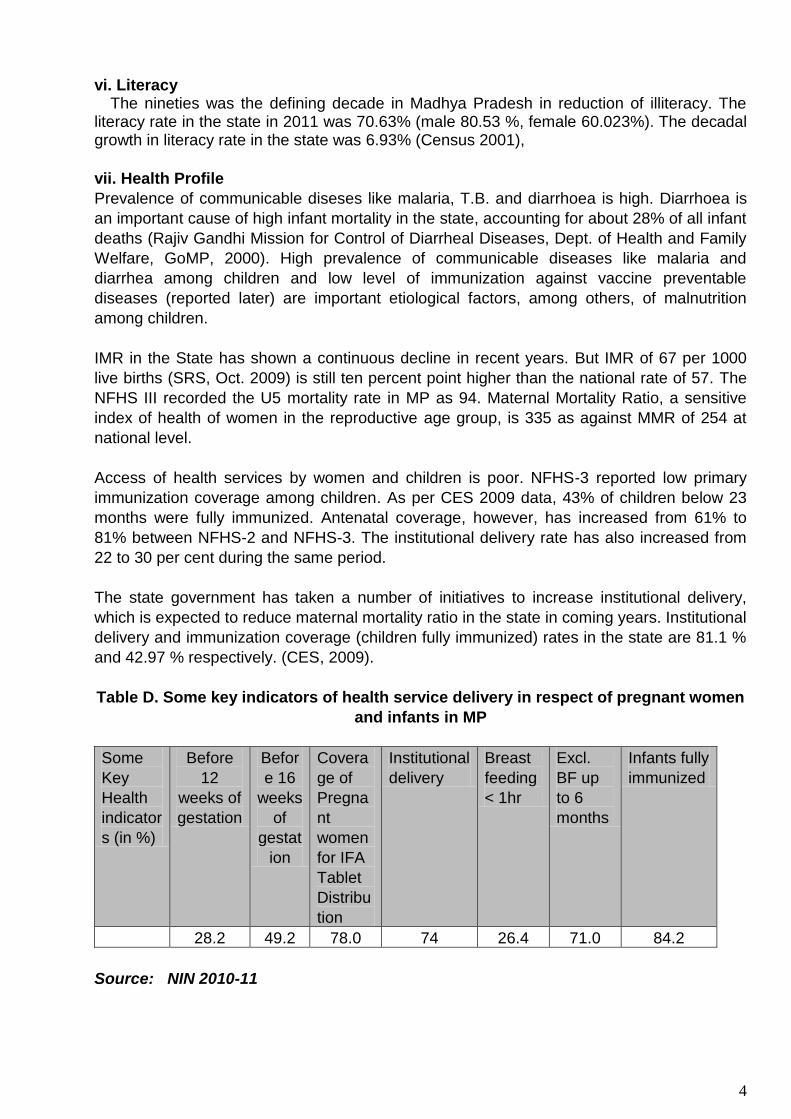
Table D. Some key indicators of health service delivery in respect of pregnant women
and infants in MP
Some
Key
Health
indicator
s (in %)
Before
12
weeks of
gestation
Befor
e 16
weeks
of
gestat
ion
Covera
ge of
Pregna
nt
women
for IFA
Tablet
Distribu
tion
Institutional
delivery
Breast
feeding
< 1hr
Excl.
BF up
to 6
months
Infants fully
immunized
28.2 49.2 78.0 74 26.4 71.0 84.2
Source: NIN 2010-11
5
viii. Access to safe water supply and sanitation
One in four persons in the state has access to safe drinking water supply (NFHS-3, 2006).
This ratio is less than 10 per cent (8.1%) in rural areas. Similarly, one in every 10 persons
(9.6%) has access to toilet facilities in rural areas.
The state has identified 126.2 thousand habitations for safe drinking water (40 liters per day
per person). Out of these, 96.30 thousand habitations have been provided safe drinking
water while another 22.10 thousand habitations have been partially covered under the
government program. To increase public participation in drinking water scheme (10% public
contribution) the government has initiated Swajal Dhara scheme. Under the total Sanitation
Program 5.38 lakhs personal toilets have been provided to the BPL families till August 2006.
(Economic Survey of Madhya Pradesh –2006-07)
x. Road connectivity in Madhya Pradesh
Roads:
The length of roads of all categories put together is about 72 thousand km in Madhya Pradesh. Work of improvement and upgradation of over 12050 km roads has been taken up in last one and half years. These include 1400 km National Highways, 2300 km State Highways, 3650 km important district roads and 4700 km rural roads. Over three-fourth of the work has already been completed. The performance of Madhya Pradesh in rural road construction has been lauded by the central government. So far, 10600 villages having upto one thousand population have already been connected to all weather roads and now only 3400 villages remain to be covered. The length of national highway in the state is 3700 kms while State highway extends to 7300 kms.(www.mpinfo.org- Dept of Public Relatio s, GoMP)
Railways:
The main rail route linking Northern India with Southern India passes through Madhya Pradesh. Main junctions in the state are Bhopal, Bina, Gwalior, Indore, Itarsi, Jabalpur, Katni, Ratlam and Ujjain. The divisional railways headquarters are at Bhopal, Ratlam and Jabalpur. (Website of Dept. of Public Relations, GoMP.)
b) Nutrition Policy of Madhya Pradesh
Madhya Pradesh has developed and adopted a Nutrition Policy. The main objectives of
the Policy are to reduce cases of malnutrition in the state, which would be achieved by
developing a district-level work plan. The State Nutrition Policy aimed at achieving the
following objectives (by the end of year 2003):
To decrease moderate malnutrition by 15 percent and severe malnutrition by 10
percent in children less than five years of age
To decrease cases of low weight at birth by 10 percent
To eliminate blindness due to Vitamin ‘A’ deficiency
To decrease anemia among pregnant women by 20 percent
The major strategies for achieving the objectives were: inter-sectoral coordination, targeting
female adolescents for health care delivery, nutritional awareness and targeting the family
as the focal points for nutrition related programs.
6
c) Inter-sectoral convergence for program implementation
Department of Women & Child Development (DWCD) and Public Health & Family Welfare
(DPHFW) are the key departments for convergent actions at all the level. However other
departments such as:
Department of Rural Development and Panchayat: for Sanitation & Hygine, livelihood
programmes and local governenace
Department of Public Health Engineering: Providing safe water at village as well as at
AWC level
Department of Education: Adolescent anaemia and preschool componenet
Department of Tribal Welfare: For better services in vulnerable pockets of the state
Department of Food & Civil supplies: Privisioning of essentials commodity ( Wheat &
Rice) for SNP in AWCs
Department of P&T and Banks
The convergent actions with other departments play an important role for reaching out to the
most vulnerable and margilanilized community and ensuring timely availability of ICDS
services. The key points of convergence with various departments are as follows:
Implementation of ABM: A state specific Mission mode approach for improving
Nutrition services and addressing Malnutrition
Holding Regular VHNDs: A convergent forum between ICDS & Health.
Use of Mother and Child Protection Card (MCP): For better Recording & Tracking
Health Camps: For better outreach of essential services such as, Immunization,
ANC/PNC and other health Check ups.
Observation of Bal Suraksha Maah (BSM): To deliver package of Essential Nutrition
services such as VAS, Deworming, Salt testing etc.
Observing Mangal Diwas: A theme based dedicated day for providing various
services to the community in participation with PRI, SHGs, Adolescent groups and
other stakeholders
SABLA & KSY: A scheme for adolescent girls in close partnership with Health,
Education and Labour department. The programme address the life skill approach,
Nutrition component and vocational trainings
Nutrition Rehabilitation Center: The Facility based care of Severely Acute
Malnourished Children is provided by DPHFW/NRHM with active support from ICDS
for case identification, referrals and follow-ups.
Nutrition Resource Centres at State and Divisional Level: Six NRCs Established in all
the Govt. Medical Colleges to support ICDS/ABM and NRHM for regular capacity
building, planning and data utilization.
Total Sanitation Campaign (TSC): Provisioning of sanitary toilets in AWCs in
collaboration with Panchayat and Rural Development Department.
IGMSY: In close participatrion with department of P&T and Banks to facilitate
disbursement of cash benefits.
Strengthening Pre-Schools Component: following the SSA Pattern on Preschool
education as well as for child friendly buildings.
d) Nutrition and health status of women and children in MP
Health status of the people in MP has been discussed earlier (Section a.vii, page 4). The
nutritional status of women and children has been reviewed in this section.

7
A recently concluded survey on nutritional status of under five children in rural Madhya
Pradesh by the National Institute of Nutrition (NIN), Hyderabad revealed that about 52% of
the rural children below five years of age are underweight in Madhya Pradesh, with a low of
34.8% in Vidisha District and a high of 67.1% in Satna District. Similarly, 49% of them were
stunted (ranging from 34.1% in Indore and 71% in Morena) and 26% were wasted (ranging
from 15.1% in Morena and 40.2% in the district of Rajgarh). However, it is encouraging to
note that these figures are lower than those reported in the National Family Health Survey
(NFHS-3) of 2006 (underweight 62.7%; stunting 51.7%; and wasting 36%).
Trends in Children's Nutritional Status (% below -2 SD)
A similar pattern was also observed among severe acute malnourished (SAM) children as
shown in the graph below. The SAM children (having nutritional status as % below -3 SD)
shows that it is at the level of 19.8% in the state. The proportion of SAM children has
registered a decline of about 10 points from 29.3% during NFHS-3 (2006) to 19.8% as per
NIN survey (2010).

8
Trends in Children's Nutritional Status (% below -3 SD)
The NIN survey also provides prevalence of undernutrition among children by age group. It
was found that undernutrition was high among children in the age group of 1-3 years (both
underweight and stunting).
Prevalence (%) of Undernutrition among <5 yrs Children According to SD
Classification (<Median – 2SD) by Age group
The prevalence of undernutrition was found to be higher among boys than girls. The graph
below depicts that undernutrition among boys is comparatively higher than girls in all the
three categories expressed as underweight, stunting and wasting.

9
Prevalence (%) of Undernutrition among <5 yrs Children according to SD
Classification (<Median – 2SD) by Gender
This survey was conducted by NIN at the request of the Department of Women and Child
Development (DWCD), Government of Madhya Pradesh during March – August 2010. The
survey aimed to estimate the prevalence of undernutrition among under- five year rural
children and infant & young child feeding (IYCF) practices for the development of district
specific nutrition intervention strategies.
The survey also revealed that over three fourths (78.5%) of pregnant women had undergone
antenatal check-up (ANC) at least once during their pregnancy, while one third of them had
at least three ANCs (36.4%).
It is encouraging to note that the proportion of newborns that were given pre-lacteals in the
current survey was only 16.1% as against 58.7% reported in NFHS-3 survey during 2005-
2006. Although 78.4% of pregnant women received Iron Folic Acid (IFA) tablets during
pregnancy, only 20% consumed the required number of at least 90 tablets during
pregnancy. About 79% deliveries were institutional and a majority was conducted by the
Medical Officers. Birth weights were recorded for 69% infants and the prevalence of low
birth weight (less than 2.5 kg at birth) was 19% which is lower than the overall State (23.4%)
and National (21.5%) prevalence rates reported in NFHS-3.
Other encouraging results of the survey were that almost all mothers fed colostrum (first
milk) to their newborns, a fourth of the mothers initiated breastfeeding within 1 hour and
another half (49%) within 1-3 hours of delivery. However, only about one fourth of the
mothers had initiated complementary feeding at 6 months of age, which included mostly
homemade semisolids/solids. Only one third of mothers gave complementary feeds to their
children at least 3 times a day.
10
About 84% of children in the age group of 1-2 years were completely immunized during the first year of life and three quarters of children below 5 years received at least one dose of Vitamin A during the preceding year.
The survey highlights the need to impart health and nutrition education to the pregnant and lactating mothers through effective communication strategies. The existing national nutrition intervention programmes such as supplementary feeding under ICDS have to be strengthened further alongside poverty alleviation and income generating activities to improve household food and nutrition security status.
Anemia among children and women
In NFHS-3 a very high proportion (82.6%) of children between 6-35 months were found
suffering from anemia. Prevalence of anemia was higher among rural as compared to urban
children (85% and 65% respectively). In the NIN survey total 25.0 % of children between the
age group of 12-59 months were distributed IFA Tablet/Liquid
In the study conducted by National Instititute of Nutrition, Hyderabad (NIN) 2010-11, Out of
the total population surveyed 28.2% of women were registered their pregnancy before 12
weeks of gestation and 36.4% of women recived three ANC visits in comparision to 40.2 %
in NFHS -3 (2005-06), this area needs improvement. 92.8 % of women recived IFA tablets
during their pregnancy and out of which only 19.7% pregnant women consumed more than
90 IFA tablets, in comparision to 11.8 % reported NFHS -3 (2005-06). There is an increase
in 8 points but still needs improvement and its an areas of action in the present APIP.
e) History of ICDS in MP – geographical and population coverage
Launched on October 2, 1975 in thirty districts of India, ICDS program has grown as the
world’s largest early childhood development program. The program approaches child health
holistically and comprises health, nutrition, and education components for children less than
six years of age; pregnant women and lactating mothers; and adolescent girls.
ICDS Program in Madhya Pradesh
ICDS scheme was first launched in MP in 1975-76 in Baidhan, a rural block of Singrauli in
Sidhi district (Singarauli is an independent district now), and Tokpal, a tribal block of
Jagadalpur district (now in Chattisgarh state). The program was gradually expanded to
cover the entire state. Year-wise expansion of the ICDS program is shown in table E.
Currently, the ICDS scheme covers all the rural blocks and urban areas in the state. There
are 453 ICDS projects in the state. Of these, 281 are rural, 99 are tribal and 73 are urban
projects. (Annual Report, 2009-2010, Women and Child Development Department, GoMP).
In the 453 Projects, 78,929 AWCs and 12070 Mini AWCs have been sanctioned.

11
Table E. Year-wise establishment of ICDS projects and AWCs
Year ICDS
Project
Cumulative
total
Projects
AWCs Cumulative total AWCs
2004-05 - 336 - 49,258
2005-06 31 - 549 49,787
2006-07 - 367 9,537 59,324
2007-08 - - 9,914 69,238
2008-09 86 453 9,691 78,929
2009-10 There are no new projects and AWCS sanctioned in this period
2010- 11
2012-13 - - 1231 81391
Note: Mini AWCs sanctioned by GOI to MP are 12070 (including 9691 sanctioned in
Phase III)
All the AWCs, including newly sanctioned 9691 addditional AWCs and 9820 Mini AWCs are
operational. In the year 2012-13, 1231 AWCs are sanctioned by GoI. With this, the ICDS
scheme has been almost universalized throughout the state.
f) State’s financial contribution to ICDS implementation (including on supplementary
nutrition)
ICDS is a centrally sponsored scheme of GOI. The program is, however, implemented by
the state government. In MP the ICDS program is implemented under the umbrella of the
Department of Women and Child Development. The funds for the implementation of the
program are provided by GOI on a cost sharing basis.
For additional initiatives, other than covered under the GOI program, the state government
provides the required funds. For example, under the Project Shaktiman initiative of the
government, the cost of third meal and related expenses was being borne by the state
government. The state has launched in 2010 Atal Bal Mission (details are given at page 21).
Under this Mission Department of Women and Child development has been provided funds
for the welfare of women and children. Part of the funds will be made available to the ICDS
program. The state has also provided additional honorarium to AWWs & AW helpers and
Mini AWCs workers, at the rate of Rs. 1500/- per month (AWWs), Rs. 750/- per month
(AWHS) and Rs. 750/- (Min AWWs) respectively. The State also paid Rs. 631.43 lakhs
towards cost of uniform (saree) for AWWs and AWHs from its budget (sanction vide letter
No.F3-3/09-50-2 PF dt.28 Feb.2009 of GOMP).
g) Infrastructure status of AWC buildings
The Department of Women and Child Development is committed to provide adequate and
suitable accommodation for smooth functioning of the AWCs in the state. Government of
India does not give grant for construction of AWC building. The state’s own resources are
limited in this respect. But the government has made efforts to construct AWC building with
funds from BRGF and 13th Finance Commission. . Efforts are also being made to get AWCs
building constructed tapping other resources e.g. MPLAD, funds from Department of Rural
Development and Tribal Development, etc.

12
Details of AWCs sanctioned, buildings approved for construction and AWCs working in
their own building is shown in table F.
Table F: Status of AWC Building in State
District-wise number of AWCs with & without own buildings (as on 31 March 2012)
S. No
Division District Total
sanctioned AWC
Total Sanctione
d Buildings
Total Buildings constructe
d
AWC without
own building
1 Indore Alirajpur 1121 502 378 743
2 Shahdol Anuppur 1030 627 426 604
3 Gwalior Ashok Nagar 876 146 131 745
4 Jabalpur Balaghat 2294 1097 753 1541
5 Indore Barwani 1501 1050 861 640
6 Bhopal Betul 2065 1353 947 1118
7 Chambal Bhind 2022 485 242 1780
8 Bhopal Bhopal 1618 563 251 1367
9 Indore Burhanpur 725 347 169 556
10 Sagar Chattarpur 1728 1146 573 1155
11 Jabalpur Chhindwara 2636 604 442 2194
12 Sagar Damoh 1309 405 281 1028
13 Gwalior Datia 766 366 175 591
14 Ujjain Dewas 1493 339 176 1317
15 Indore Dhar 3248 1662 1128 2120
16 Jabalpur Dindori 1671 1087 999 672
17 Gwalior Guna 1125 312 258 867
18 Gwalior Gwalior 1239 311 198 1041
19 Narmadapuram Harda 574 214 139 435
20 Narmadapuram
Hoshangabad 1540 500 383 1157
21 Indore Indore 1582 296 192 1390
22 Jabalpur Jabalpur 2101 377 311 1790
23 Indore Jhabua 1606 923 430 1176
24 Jabalpur Katni 1509 687 327 1182
13
25 Indore Khandwa 1468 673 518 950
26 Indore Khargone 1857 981 684 1173
27 Jabalpur Mandla 1821 1018 771 1050
28 Ujjain Mandsaur 1499 276 210 1289
29 Chambal Morena 2058 1162 482 1576
30 Jabalpur Narsinghpur 1004 281 164 840
31 Ujjain Neemuch 880 254 158 722
32 Sagar Panna 1170 307 256 914
33 Bhopal Raisen 1379 390 290 1089
34 Bhopal Rajgarh 2010 579 420 1590
35 Ujjain Ratlam 1620 376 144 1476
36 Rewa Rewa 2791 376 265 2526
37 Sagar Sagar 2199 517 488 1711
38 Rewa Satna 2591 897 663 1928
39 Bhopal Sehore 1109 585 359 750
40 Jabalpur Seoni 1810 1182 737 1073
41 Shahdol Shahdol 1340 571 284 1056
42 Ujjain Shahjapur 1301 467 318 983
43 Chambal Sheopur 894 486 130 764
44 Gwalior Shivpuri 1850 833 492 1358
45 Rewa Sidhi 1772 886 547 1225
46 Rewa Singroli 1335 608 535 800
47 Sagar Tikamgarh 1406 951 710 696
48 Ujjain Ujjain 1888 462 328 1560
49 Shahdol Umaria 643 548 546 97
50 Bhopal Vidisha 1855 797 283 1572
TOTAL 78929 31862 20952 57977
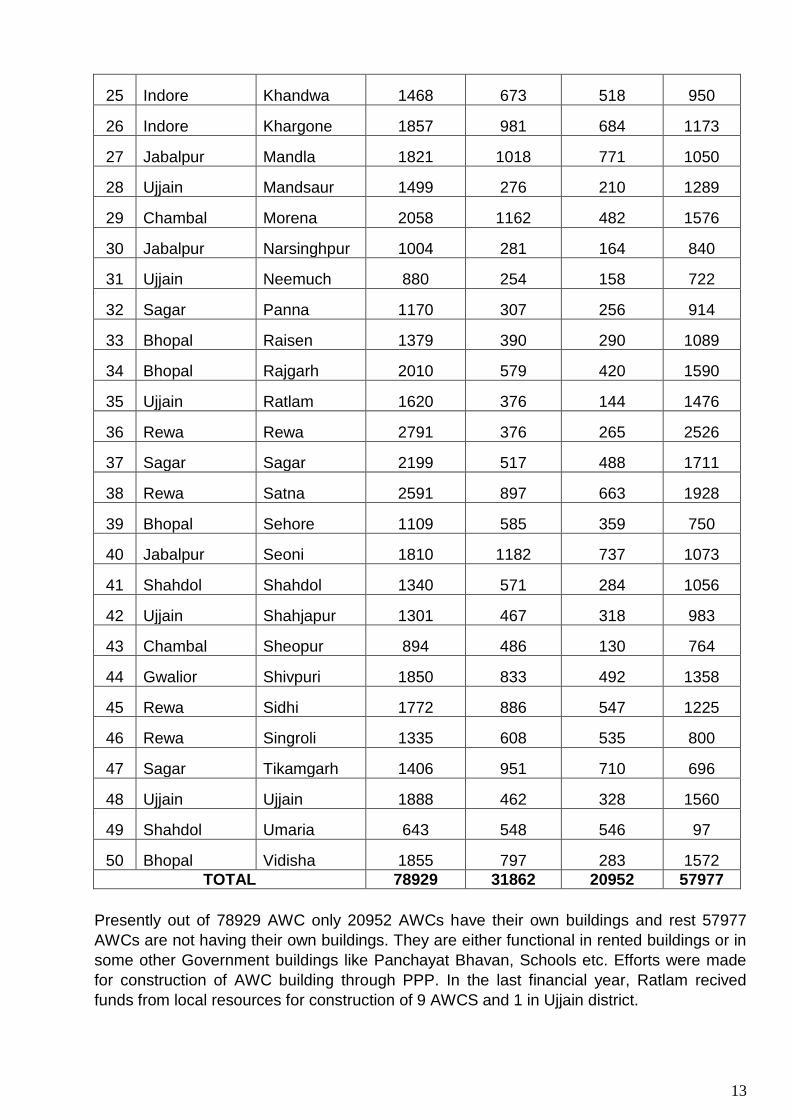
Presently out of 78929 AWC only 20952 AWCs have their own buildings and rest 57977
AWCs are not having their own buildings. They are either functional in rented buildings or in
some other Government buildings like Panchayat Bhavan, Schools etc. Efforts were made
for construction of AWC building through PPP. In the last financial year, Ratlam recived
funds from local resources for construction of 9 AWCS and 1 in Ujjain district.
14
h) Status of operationalization of Projects, AWCs and Mini-AWCs
Total number of ICDS projects and AWCs in Madhya Pradesh
ICDS program in MP operates through 453 Projects and 78,929.Anganwadi centers. District
-wise rural, tribal and urban projects and the AWCs are presented in Annexure 2. (MPR,
Nov. 2010, Directorate of Women and Child Development). With the sanction of additional
AWCs by GOI, the ICDS program has been almost universalized in the state. But, on the
State’s request for establishment of AWCs on demand, GoI has recently sanctioned 1231
AWCs but still approval of 79 projects (from 35 Districts) and 1909 AWCs is still pending
with GOI.
The state has followed the population norms given by GOI from time to time for
establishment of AWCs. The new norms of GOI (issued vide its letter No. F.14-1/2008-CDI
dt. 18 Dec.2008) in this respect are given in Annexure 3.
i) Trends in coverage of beneficiaries for supplementary nutrition and pre-school
education
Coverage under supplementary nutrition program
The beneficiaries of ICDS services are children 0-6 years, pregnant women, lactating
mothers and adolescent girls. Number of beneficiaries as per MPR March 2012 data of ICDS project in the state were 5975000 children of 0-6 year age and 1268686 pregnant & lactating Mothers.
Coverage under pre-school education
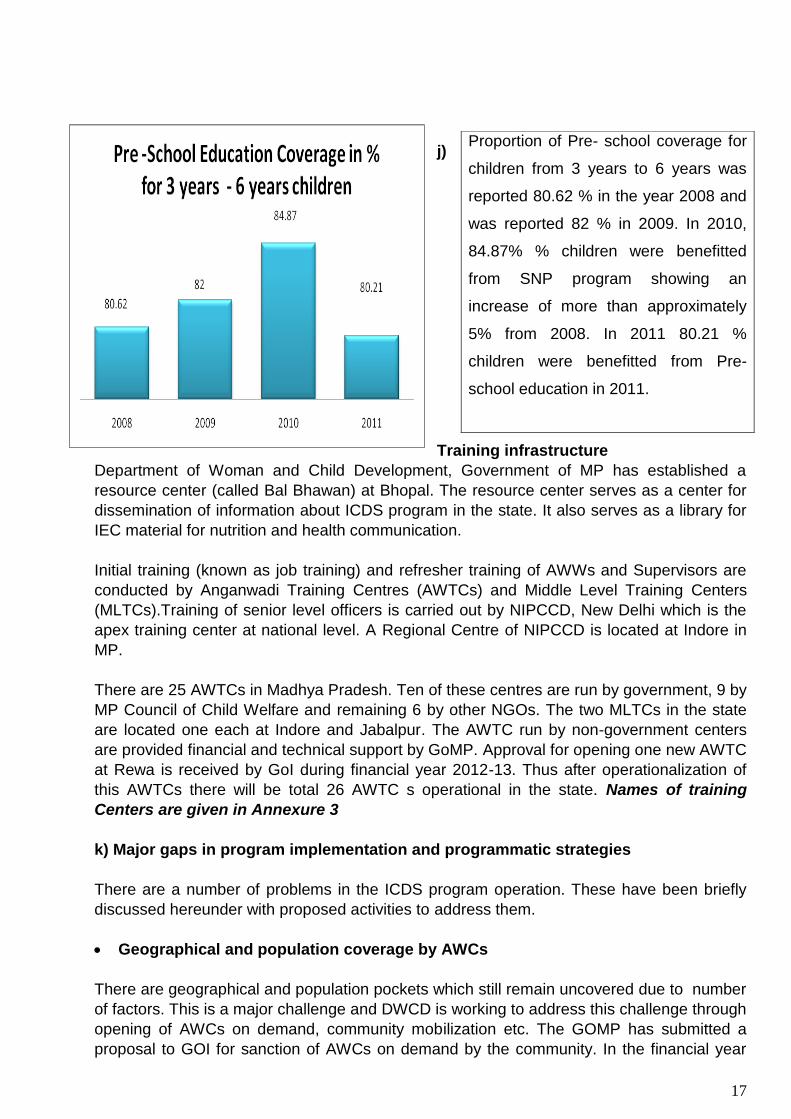
As per MPR March 2012 a total of 2734819 pre-school education beneficiaries were registered at AWCs. Of them 1388423 were boys and 1346396 were girls. The children of 3- 6yrs attending AWCs are offered informal learning through games, story telling, use of pictures, etc. AWWs are trained to conduct PSE sessions during their job training and refresher training courses.
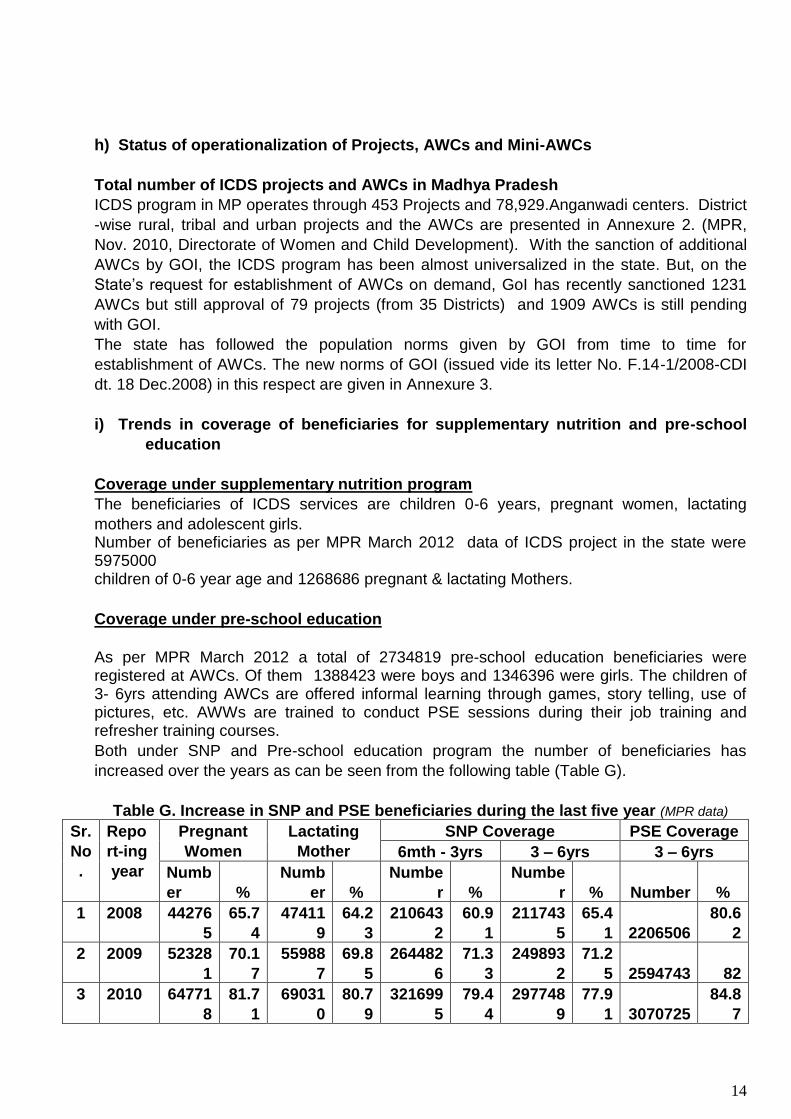
Both under SNP and Pre-school education program the number of beneficiaries has
increased over the years as can be seen from the following table (Table G).
Table G. Increase in SNP and PSE beneficiaries during the last five year (MPR data)
Sr.
No
.
Repo
rt-ing
year
Pregnant
Women
Lactating
Mother
SNP Coverage PSE Coverage
6mth - 3yrs 3 – 6yrs 3 – 6yrs
Numb
er
%
Numb
er
%
Numbe
r
%
Numbe
r
% Number
%
1 2008 44276
5
65.7
4
47411
9
64.2
3
210643
2
60.9
1
211743
5
65.4
1 2206506
80.6
2
2 2009 52328
1
70.1
7
55988
7
69.8
5
264482
6
71.3
3
249893
2
71.2
5 2594743 82
3 2010 64771
8
81.7
1
69031
0
80.7
9
321699
5
79.4
4
297748
9
77.9
1 3070725
84.8
7

15
4 2011 62821
2
94.1
1
64047
4
93.1
2
309661
2
88.8
3
287838
8
84.4
2
2734819
80.2
1
Proportion of women benefited from
Supplementary nutrition program in
year 2008 was 65.74 that increased to
70.17 in year 2009. Another increase
of 11 % has been reported in 2010. In
the year 2011 around 94.11 % women
has been benefited by the
supplementary nutrition program.
Overall a positive change of 43.15 %*
increase from baseline year of 2008 to
2011.
*
x0= % of 2008
x 1 = % of 2011
Proportion of Lactating mothers
benefitted from supplementary nutrition
program in the year 2008 was 64.23%
that increased to 69.85 in 2009. In 2010 it
increased by 11percent points and has
been reported 80.79% and in the year
2011 93.12 % lactating mothers were
benefitted from SNP. 44.97%* positive
change was reported in the SNP
coverage of Lactating Mothers from 2008
to 2011.
*
x0= % of 2008
x 1 = % of 2011
]/)[(100% 001 xxxx
]/)[(100% 001 xxxx
16
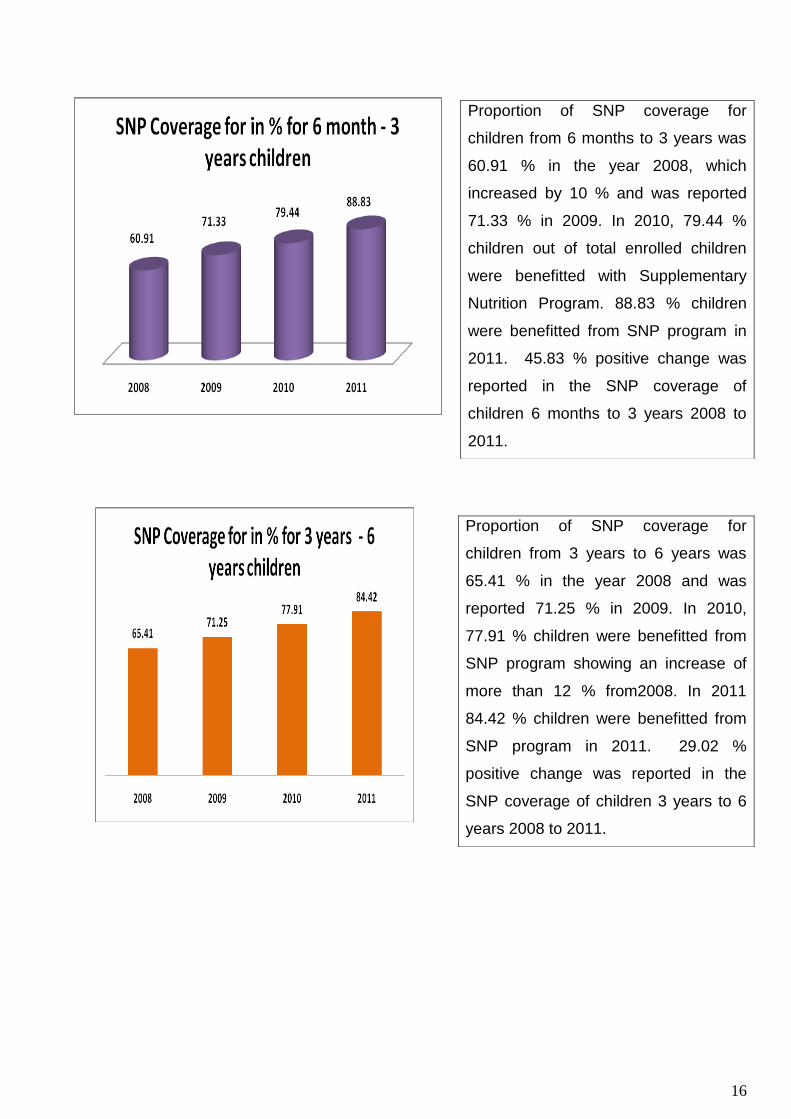
Proportion of SNP coverage for
children from 6 months to 3 years was
60.91 % in the year 2008, which
increased by 10 % and was reported
71.33 % in 2009. In 2010, 79.44 %
children out of total enrolled children
were benefitted with Supplementary
Nutrition Program. 88.83 % children
were benefitted from SNP program in
2011. 45.83 % positive change was
reported in the SNP coverage of
children 6 months to 3 years 2008 to
2011.
Proportion of SNP coverage for
children from 3 years to 6 years was
65.41 % in the year 2008 and was
reported 71.25 % in 2009. In 2010,
77.91 % children were benefitted from
SNP program showing an increase of
more than 12 % from2008. In 2011
84.42 % children were benefitted from
SNP program in 2011. 29.02 %
positive change was reported in the
SNP coverage of children 3 years to 6
years 2008 to 2011.
17
j)
Training infrastructure
Department of Woman and Child Development, Government of MP has established a
resource center (called Bal Bhawan) at Bhopal. The resource center serves as a center for
dissemination of information about ICDS program in the state. It also serves as a library for
IEC material for nutrition and health communication.
Initial training (known as job training) and refresher training of AWWs and Supervisors are
conducted by Anganwadi Training Centres (AWTCs) and Middle Level Training Centers
(MLTCs).Training of senior level officers is carried out by NIPCCD, New Delhi which is the
apex training center at national level. A Regional Centre of NIPCCD is located at Indore in
MP.
There are 25 AWTCs in Madhya Pradesh. Ten of these centres are run by government, 9 by
MP Council of Child Welfare and remaining 6 by other NGOs. The two MLTCs in the state
are located one each at Indore and Jabalpur. The AWTC run by non-government centers
are provided financial and technical support by GoMP. Approval for opening one new AWTC
at Rewa is received by GoI during financial year 2012-13. Thus after operationalization of
this AWTCs there will be total 26 AWTC s operational in the state. Names of training
Centers are given in Annexure 3
k) Major gaps in program implementation and programmatic strategies
There are a number of problems in the ICDS program operation. These have been briefly
discussed hereunder with proposed activities to address them.
Geographical and population coverage by AWCs
There are geographical and population pockets which still remain uncovered due to number
of factors. This is a major challenge and DWCD is working to address this challenge through
opening of AWCs on demand, community mobilization etc. The GOMP has submitted a
proposal to GOI for sanction of AWCs on demand by the community. In the financial year
Proportion of Pre- school coverage for
children from 3 years to 6 years was
reported 80.62 % in the year 2008 and
was reported 82 % in 2009. In 2010,
84.87% % children were benefitted
from SNP program showing an
increase of more than approximately
5% from 2008. In 2011 80.21 %
children were benefitted from Pre-
school education in 2011.
18
2011-12, a proposal of 3140 was sent to GoI to open AWCs on demand out of those 1231
AWCs has been sancioned.
Space constraints at AWCs
A major obstacle in the proper functioning of AWCs is space problem. A large number of
AWCs (about 75 percent) are still operating from improvised buildings namely rented
buildings, panchayat/ school/government buildings etc. These buildings do not provide
sufficient/suitable space for storage of supplies and equipments, organization of different
activities including pre-school education and NHED activities. . In the state out of total
78929, 20942 AWC are running in their own building, 37392 AWCs are running in rented
building and 20555 AWCs are operational in school /panchayat and other buildings. During
the financial year 2011-12 a total of 1715 AWC buildings were sanctioned for contruction
under 13th Finance Commission. The State is constatntly trying to arrange funds from
different sources e.g. BRGF, Department of Panchayat and Rural Development, etc. for
construction of new AWC buildings. Old buildings are also being renovated to make them
child friendly. This has been discussed in the next section. This has been discussed in the
next section. Proposal has sent to GoI for increasing rent of AWCs in Urban and Rural
areas, so that spacious buildings can be rented.
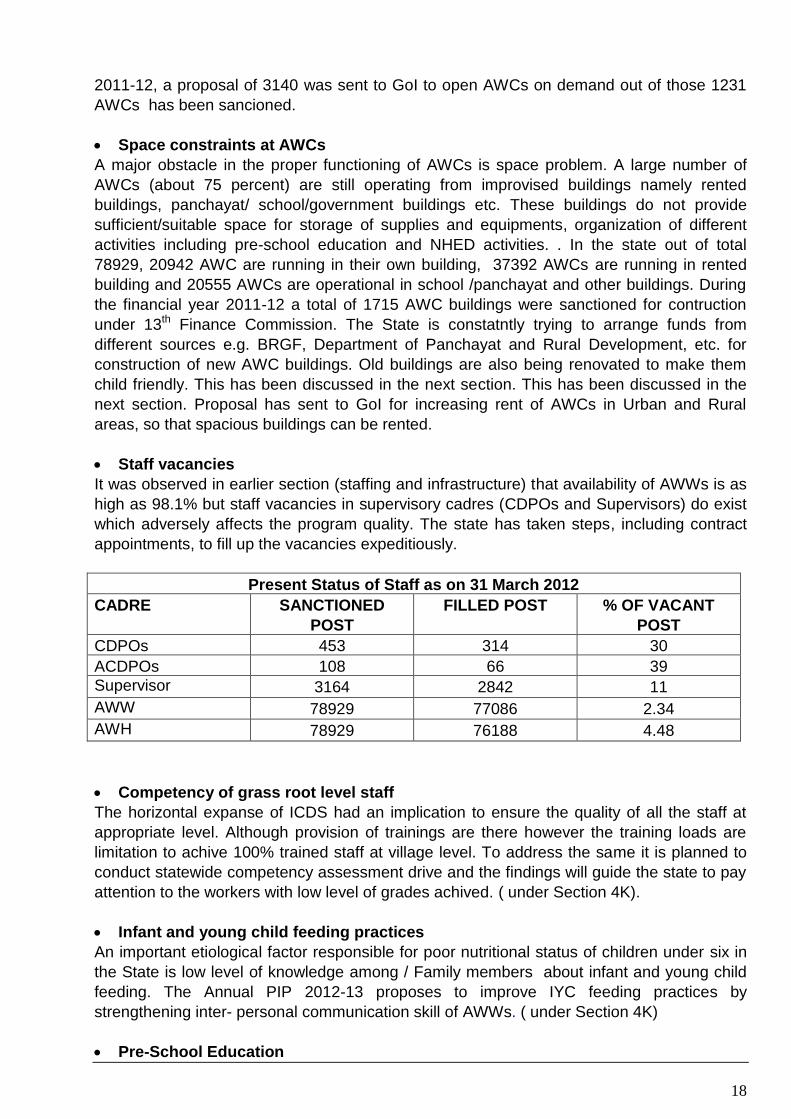
Staff vacancies
It was observed in earlier section (staffing and infrastructure) that availability of AWWs is as
high as 98.1% but staff vacancies in supervisory cadres (CDPOs and Supervisors) do exist
which adversely affects the program quality. The state has taken steps, including contract
appointments, to fill up the vacancies expeditiously.
Present Status of Staff as on 31 March 2012
CADRE SANCTIONED
POST
FILLED POST % OF VACANT
POST
CDPOs 453 314 30
ACDPOs 108 66 39
Supervisor 3164 2842 11
AWW 78929 77086 2.34
AWH 78929 76188 4.48
Competency of grass root level staff
The horizontal expanse of ICDS had an implication to ensure the quality of all the staff at
appropriate level. Although provision of trainings are there however the training loads are
limitation to achive 100% trained staff at village level. To address the same it is planned to
conduct statewide competency assessment drive and the findings will guide the state to pay
attention to the workers with low level of grades achived. ( under Section 4K).
Infant and young child feeding practices
An important etiological factor responsible for poor nutritional status of children under six in
the State is low level of knowledge among / Family members about infant and young child
feeding. The Annual PIP 2012-13 proposes to improve IYC feeding practices by
strengthening inter- personal communication skill of AWWs. ( under Section 4K)
Pre-School Education
19
Low enrolment of children in Pre-school Education (PSE) program is one of the major
challenges facing ICDS. It is realized that Right to Education cannot be achieved unless
PSE is strengthened. During 2009-10 the department of WCD carried out refresher training
of all grass root level workers (Supervisors and AWWs) in carrying out PSE. Guidance of
experts in the field was taken to design the training module. Steps have also been taken to
ensure regular supply of PSE kits to the AWCs.
Behavior Change Communication activities & resource material
Behaviour change communication is the key to improve IYC feeding and utilization of health
services by the mothers. The conventional IEC approaches (printing and distributing
posters, radio/TV jingles, wall writings, hoardings, etc) have only limited impact on bringing
about behavior change. The Annual PIP of the State proposes to strengthen inter-personal
communication skills of ICDS functionaries through training and equipping them with
suitable IEC material. (under Section 4K)
Linkages with community based organizations
Following the 73rd Constitution Amendment Madhya Pradesh was one of the first states in
the country to frame rules (Madhya Pradesh Panchayati Raj evam Gram Swaraj Adhiniyam,
1993) for implementation of Panchayati Raj system. Accordingly PRIs were created at
District, Block and Village level. Presently 21,999 Gram Panchayats are functioning in the
state. Gram Panchayats are peoples’ institutions at village level and can be potent
instruments for strengthening ICDS activities. The department of WCD proposes to orient
PRI functionaries and other opinion leaders (SHGs, Mahila Mandals, SMS, ASHA, etc)
about ICDS program. ( under Section 4K)
Monitoring and evaluation system
The department of Women and Child Development, GOMP collects a large amount of data
through monthly progress reports (Format I and II). It has developed a web enabled system
for data transfer from the field. To effectively use the data for program management the
Annual PIP has proposed staff training in MIS. ( under Section 4K)
Inter-departmental coordination/ convergence
NRHM of Department of H&FW, and Department of Women and Child Development serve
the same segment of population (women and children). Although there is some degree of
inter-departmental coordination, stillthere is scope of greater convergence for their activities
as well as other line departments have also stakes in the health and nutrition activities for
women and children. The Annual PIP, 2012-13 proposes to take initiative for convergence of
activities of line departments through conducting special workshops for the purpose. ( under
Section 4K)
l) Initiatives of the GOMP for ICDS program
Madhya Pradesh government is committed to improve the health and nutritional status of
women and children in the state. In recent years the state has taken some special initiatives
towards achieving this objective. These initiatives are briefly outlined in this section.
A. Organization of "Mangal Diwas"

20
Mangal Diwas, a unique community-based, culturally appropriate initiative has been
conceived and is being implemented by GoMP. On every Tuesday of a month a special
program is organized at AWCs in the state.
a)"Goad Bharai" is a cultural practice in many communities. It is celebrated to falicitate
pregnant women by offering them coconut fruit and other auspicious articles like bangles,
vermilion, bindi, etc. and gifts from relatives. Under ICDS initiative of GoMP Goad Bharai
celebration is performed at AWC on 1st Tuesday of every month. All newly identified
pregnant women are invited to this function. The occasion is utilized for registration of
pregnant women for antenatal care (a mother-child card is prepared), health and nutrition
education, and IFA supplementation. BPL (below poverty line) women are also provided one
time financial assistance of Rs. 500.
(b)“Anna Prashan” is also a cultural function which is observed by families to initiate the
child on semi-solid food (e.g. rice cooked in milk, porridge, etc) on attaining six months age.
Anna Prasan function is held at all AWCs on 2nd Tuesday of every month. All pregnant and
lactating women are invited to AWC to attend the function. Eligible children are given their
first solid/mushy food and offered a feeding bowl and spoon as gift. This cultural occasion is
utilized to educate mothers about infant and young child feeding and to check immunization
status of children.
(c) “Janam Diwas” program is organized at AWCs on 3rd Tuesday of every month to
celebrate birth-day of all children who were born during the month. Weight of the children
are taken and recorded on a register. Immunization status of children is checked. Children
who have not completed primary vaccination (BCG, three doses of DPT and Polio, and
Measles) are referred to NHD camps or to the nearest health institution for scheduled
immunization doses. Children whose birth day falls during the month are offered birthday
gifts.
(d). “Kishori Balika Diwas” is scheduled on the fourth Tuesday of every month. All
adolescent girls who are registered under Kishori Shakti program are invited to AWC on
Kishori Balika Diwas or Adolescent girls' day where they are educated about balanced diet,
health care and are told about economic and home making skills. Health checkup and
treatment of minor ailments, games, etc. is also organized. Adolescent girls are
administered IFA tablet for prevention of anemia.
Development Partners have extended support to the program by organizing state level
training for MLTC and AWTC staff on Mangal Diwas to build their capacity and through them
of the ICDS staff. Mangal Diwas activities are culturally in tune with the community practices
and have high acceptability. They have been successful in disseminating information,
modifying practices and eliciting community participation in different activities of AWCs. It
has provided a platform to women and adolescent girls to talk about health and welfare of
women and children. The number of beneficiaries of AWCs has shown an improvement
through these innovative programs.
21
B. Atal Bal Mission (ABM)
Taking note of the high infant mortality and under five mortality rates in the state as well as
high prevalence of malnutrition among children under six the state (MP) has decided to
launch the Atal Bal Arogya Evam Poshan Mission. The State Assembly approved setting up
of the Mission on 14th May 2010 by adopting a set of 70-point resolution The objective of
the Mission is to bring about a systematic reduction in child malnutrition and make the
State’s children healthy and happy. The dedicated Mission will experiment, pilot, replicate
and upscale ideas aimed at improving the health and nutritional status of children across
Madhya Pradesh.
The goals set out in the Mission document are:
Reduce mortality rate for children under five years (U5MR) from 94.2 to 60 per thousand
live births by the year 2015
Reduce the percentage of underweight children under five years from 60% to 40% by
2015 and further to 20% by 2020
Reduce prevalence of Severe Acute Malnutrition (SAM) less than 5 years from 12.6
percent to 5 percent by 2015 and to negligible level by 2020.
The Mission will oversee the existing nutrition and health services and will ensure that
corrective actions are taken to strengthen all components of service delivery, including
timely and appropriate utilization of financial resources and mobilization of additional
resources to achieve the set goals.
Atal Bal Mission will not be a stand alone program. Rather, it will act as an overarching
institution, a focal point to fight against child malnutrition, providing additional support-
financial and technical- to the existing programs dealing with health and nutritional services
for young children.
The Mission will specifically support the strengthening of certain specific areas e.g., effective
and regular distribution of SNP, improvements in the quality and quantity of SNP,
development of model AWCs, convergent planning. preparation of Annual District Plans,
capacity building, supportive supervision and monitoring of community based management
of moderately malnourished children and SAM children with the express purpose of
reducing child malnutrition.
The Mission will have strong political backing as its General Body will be chaired by the
Hon. Chief Minister of the state with the Ministers of Women and Child Development; Public
Health and Family Welfare; Panchayat and Rural Development as Vice-Chairpersons. The
Mission will have its own budget.
Under the Mission approach specific activities initiated supported by DFID, MP TAST &
Unicef such as:
Recruitment of ABM staff at district & Block level: By July 2013 all the 503 locations of
District & Block will be having ABM staff, and their induction training will be also
completed by August 2013 with the support of development partners.
Decentralized District Plans: Since the entire district are having different context
therefore Nutrition centric decentralized districts plans were prepared under the
leadership of each district collector. The plans were reviewed at divisional level and
accordingly allocations were made for the implementation of ABM plans
22
Technical Cell: The district staff requires constant support on technical issues, to
address the same a group of people were pooloed from International, National and
regional level to provide necessary support in the Mission activities.
Resource Centre: Further to support districts a Nutrition Resource Centres are
envisaged in the Vision document of ABM. Accordingly 6 NRC are made functional in all
the 6 Government medical college.
Traning module: For consistency of technical specification, a training module is prepared
and circulated for regular references.
C. Special survey of children through NIN to assess malnutrition
Surveys carried out by NFHS 3 recorded high prevalence (over 60%) of malnutrition among
children under six in MP. The MPR data and figures obtained from several rounds of Bal
Sanjeevani Abhiyan (where weight of children was recorded across the state), on the other
hand, reported the prevalence of underweight children to less than 50 percent.
To assess the actual prevalence of underweight children, the Department of Women and
Child Development has commissioned a study which is being carried out by National
Institute of Nutrition, Hyderabad. The study will also find out the causal factors associated
with malnutrition among children. The findings of the study will serve as the district level
baseline for nutrition prevalence and provide contours for district-level initiative to counter
malnutrition in the State. Results from NIN survey that the prevalence of underweight
children in the State is lower by 10 percent point than what was reported by NFHS-3.
(Details are at Annexure 1). Another round of NIN is proposed in the year 2013
D. Sanjha Chulha (Common Kitchen) Scheme for serving hot cooked meal to
beneficiaries
Under the Mid-Day meal program of the Panchayat and Rural Development Department
school children are served fresh cooked food prepared at school kitchen by the Self Help
Group. The Department of Women and Child Development has decided that cooked fresh
meal should also be supplied from the school kitchen for 3-6 year age children and pregnant
and lactating women covered under SNP of ICDS project. The scheme has been launched
with effect from November 1, 2009. While the food for ICDS beneficiaries is cooked and
supplied by SHG from school kitchen its distribution is done by Anganwadi Workers.
Provision for payment of transportation cost of cooked meal from school kitchen to AWC has
been made, if AWC is not located in the school premises and the school kitchen is away
from AWC. Recipes and guidelines have been provided to SHGs for preparation of food for
ICDS beneficiaries so that the daily recommended 540 calories and 14 gm protein is
provided to the beneficiaries. Of the several benefits of the scheme, an important one is
releasing the AWWs from the burden of cooking the meals. She can, therefore, now devote
more time on growth monitoring and promotion, and ECE activities.
E. Renovation of old AWCs into child friendly model AWCs
Rajya Shiksha Kendra provided Rs.10, 000/- per AWC for 88 AWCs in each district of MP
for developing the centers into Model AWC based on BaLA (Building as Learning Aid)
concept. Altogether 4400 AWCs (88 x 50) have been developed as model centers across
the state. In Ujjain district during the financial year 2011-12 a sum of Rs. 143599, in Ratlam
Rs. 114800, Rs. 37000 in Dewas and Rs. 150350 in Shahjapur has been recieved by
donation and was used for painting work in all projects and AWC in the districts.
F. Expansion of Nutrition Rehabilitation Centre

23
Since mortality rate among severely malnourished children is high (about 20%) the
Department of H&FW decided to develop a strategy to provide them prompt medical
treatment and nutritional rehabilitation. The children are admitted to NRC (established in
medical college, district and CHC hospitals) which have trained health personnel (doctors
and nursing staff) and facilities for management of severely malnourished children.
G. Use of new WHO Growth standards
Since the inception of ICDS in 1975 the nutritional status of children from birth to 5yrs has
been assessed using IAP classification based on Harvard standards (modified). WHO came
up with new standards in 2006 after a long study started in 1997 in 6 countries, including
India. MWCD organized a National Workshop on New WHO Growth Standards in New
Delhi on 8-9th February 2007. Based on the recommendations of the workshop MWCD &
MHFW, GOI took a policy decision to use WHO growth standards. Accordingly, in August
2008 Secretary, WCD and Secretary Health and Family Welfare, GOI wrote to all states for
adoption of New WHO Growth Standards in NRHM and ICDS programs.
In MP, two orientation workshops were organized in July 2009 for all the district and
selected block officials of PHFW, and WCD of all 50 districts. On the basis of the material
provided to the core trainers during their orientation in Hyderabad and those modified by
NIPPCD, state specific modules and training plans were prepared and provided to all the
state & divisional level master trainers, and Joint Directors, WCD. This was followed by a
series of divisional level & district level trainings for rolling out New WHO Growth standards
up to grass root level in all 50 districts of the state. Altogether 75853 grass root workers,
majority from DWCD, have been oriented till March 2010 on New Growth standards ans is
an ongoing activity for the last financial year.
MP is the first state in India to roll out the implementation of new WHO growth standard
across the state. This has helped in mapping the nutritional status of the children and made
it easier for the AWW to plot the nutritional status of children
H) Monitoring & Evaluation:
a. Web enabled MIS system
DWCD in collaboration with DFID/ TAST developed a web enabled MIS system to reduce
the problems associated with manual data transmission and support correct and timely
reporting. The software was piloted and tested in the year 2009/10 and in the year 2011 it
was upscaled to the entire state, supported by TAST. The MIS greatly supported the MPR
system for monitoring of the program of ICDS. There is a provision in the system to get
online information about 0-6 year children, pregnant women, adolescent girls, projects and
AWC level directory profile, etc. so that necessary monitoring and evaluation can be done.
The details of the system have been given under section “Monitoring and Evaluation”.
b. Third party Concurrent assessment: Third Party Supportive supervision is a very important for improving existing MIS but needs
to be worked out very carefully. This needs involvement of civil society organizations,
technical institutes, and experts. Setting up of a technical cell at the state level which has
coordinative role, would be necessary for concurrent assessment. However it will be
ensured that such supervision is not outsourced to one single organization/institute having
commercial interest. Commissioning a State Level Evaluation Study/Social Audit etc. to
assess the impact of ICDS on development of Children and women.

24
I) Breast feeding promotion
IYCF program in Madhya Pradesh has been scaled up in the past few years. Initially this
was initiated by Development partners by creating a pool of state & National level trainers.
Later in, a pool of middle level trainers was created across the state.
Also a cadre of CDPO and Supervisors were trained on IYCF & other Nutrition intervention
starting from High burden district. This activity was supported by DFID / TAST
To Support Nutrition intervention and to provide technical inputs to the districts 6 Nutrition
Resource Centres are made functional in close collaboration between DWCD, ABM, DME,
Medical Colleges and DFID/TAST.
ICDS in MP is working through different strategies for the promotion of appropriate breast
feeding practices. These include three in one IYCF counseling skills training, radio publicity,
periodic release of information magazine , cinema slides, mothers’ meeting and counseling,
distribution of IEC material to AWCs , organizing competitions, organizing group meetings
and awareness camps, counseling of mothers and service providers for early initiation of
Breast feeding within 1hr, colostrums feeding, exclusive breast feeding up to 6 months and
optimal feeding up to 2yrs.etc.
As a result of joint efforts of DWCD, DH&FW, Medical Colleges, local NGOs and
Development partners improvement in IYCF practices is visible as can be seen from the
following graph:
The above graph on IYCF practices shows an improvement. The data for children breastfed
with one hour of birth for rural areas was reported 13.13% in NFHS-3 which increased upto
26.4 % in NIN study 2010. In NFHS-3 the data for children who were exclusively breatfed for
6 months was reported 21.5% which increased by almost 50 % and was reported 71 % in
NIN study 2010.
J) Universal Salt Iodization
Iodine deficiency disorder is most commonly seen among poor, pregnant women and
preschool children. It results in stunted physical and mental growth of young children.
According to Coverage Evaluation Survey 2005-06 , only 33% households in MP consumed
adequately iodized salt which was reported that 48 % families were using iodized salt ≥15
25
ppm as per NIN study. The availability and consumption of un-iodized salt by the masses in
tribal and many interior pockets of the state is very high.
K) Trainings & Capacity Building: Learning from the initiative supported by DFID/ TAST to
train CDPO & Supervisors from High burden district. Similar activitiy will be carried out for all
staff in high burden districts. Also upgradation of softskills of all MLTC & AWTC staff based
on the available modules on Communications, Training skills and Computer skills.
Another approach of regular trainings will start by:
(i) Setting up of a training cell at the state level and computerized data base about the
training requirements. This cell will be responsible for preparation of Annual Training
Plan, implementation of the same, deputing trainees for various programmes.
(ii) Upgrading the infrastructure of least 5 AWTCs and 1 MLTC of the State.
(iii) Identifying specific training needs of ICDS functionaries and arrange for the training in
the same.
(iv) Development of theme specific training modules for ICDS functionaries.
(v) Cross State Learning Visits of ICDS functionaries at all levels (At least ten such visits
during one year can be propsed).

26
SECTION 2: VISION STATEMENT
Madhya Pradesh has launched an ambitious project, which will work in a mission mode, to
address the problem of malnutrition and poor health status of children. The Atal Bal Aroogya
and Poshan Mission (called in short Atal Bal Mission) was endorsed by the State Assembly
in May 2010. The Mission will work in an integrated and coordinated manner to bring about
an improvement in the nutrition and health status of children in the state.
The goal of the Mission is to:
Reduce mortality rate for children under five from 94.2 to 60 per thousand live birth
Reduce the percentage of underweight children under five years from 60% to 40% by
2915 and further to 20% by 2020
Reduce prevalence of Sever Acute Malnutrition (SAM) under five years from 12.6
percent to 5% by 2015 and to negligible level by 2020
The overall objective of the Mission is to render an enabling environment and mechanism
for prevention and reduction of malnutrition and under five mortality rates in the children of
the State through coordinated and concerted efforts.The Mission will also oversee the
existing nutrition and health services programs and will ensure that corrective actions are
taken to strengthen all components of service delivery, including timely and appropriate
utilization of financial resources and mobilization of additional resources to achieve the set
goals.
The Mission will not work as a stand alone organization but will provide additionality. The
support of the Mission to the existing programs would be budgetary as well as technical,
using the expertise from within and outside the state.
The state government has already released the first tranche of the funds to the Mission.
The Department of WCD has adapted the Atal Bal Mission priorities, objectives, goals and
targets for its ICDS program.
27
SECTION 3: ORGANIZATIONAL STRUCTURE OF ICDS PROGRAM MANAGEMENT
IN M.P.
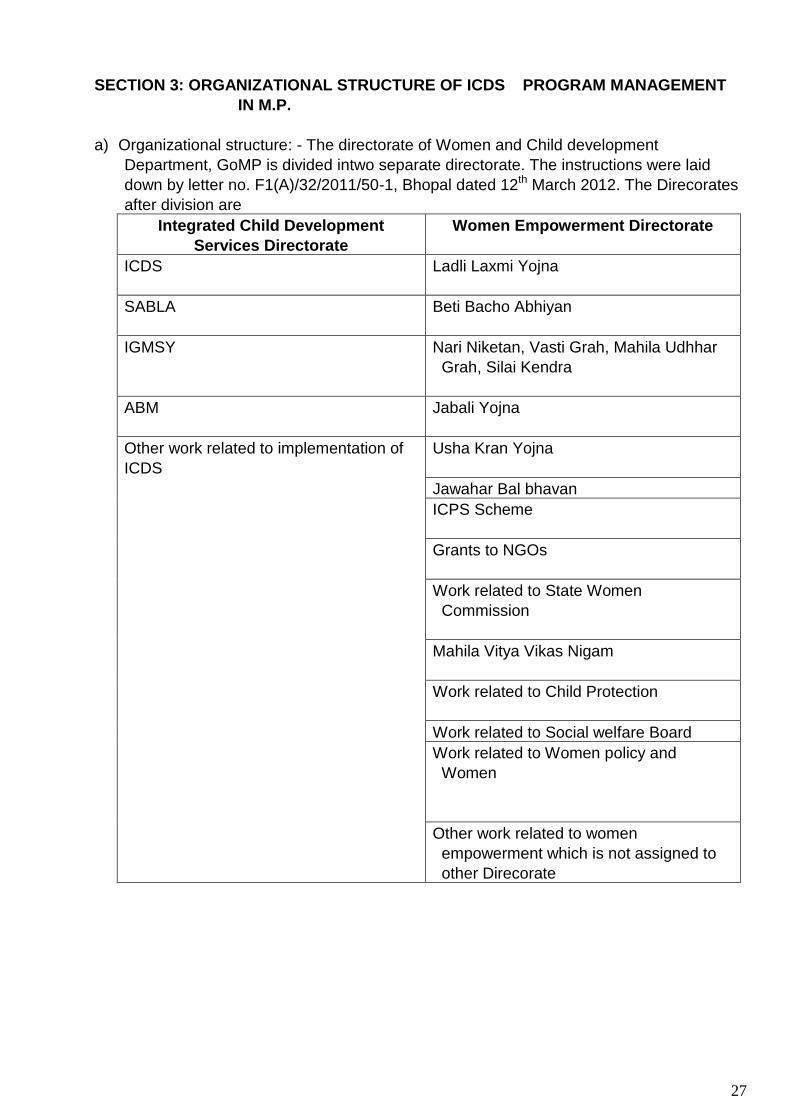
a) Organizational structure: - The directorate of Women and Child development
Department, GoMP is divided intwo separate directorate. The instructions were laid
down by letter no. F1(A)/32/2011/50-1, Bhopal dated 12th March 2012. The Direcorates
after division are
Integrated Child Development
Services Directorate
Women Empowerment Directorate
ICDS Ladli Laxmi Yojna
SABLA Beti Bacho Abhiyan
IGMSY Nari Niketan, Vasti Grah, Mahila Udhhar
Grah, Silai Kendra
ABM Jabali Yojna
Other work related to implementation of
ICDS
Usha Kran Yojna
Jawahar Bal bhavan
ICPS Scheme
Grants to NGOs
Work related to State Women
Commission
Mahila Vitya Vikas Nigam
Work related to Child Protection
Work related to Social welfare Board
Work related to Women policy and
Women
Other work related to women
empowerment which is not assigned to
other Direcorate

28
Organizational framework of the both the Directorate is shown in chart below:

29
Division Level
District Level
District Level Block Level
Assistant
Director Bal
Bhavan
(6)
Child Development & Project Officer
(453)
Assistant Statistical Officer (369)
Assistant Child Development &
Project Officer (109)
Joint Director (10)
District
Programme
Officer
(DPO) (50)
Chief
Instructor
AWTC
(10)
District
Women &
Child
Development
Officer
(DWCDO)
(34)
Instructors
(20)
Supervisors (1998 Regular &
1166 Contract appointments)
Anganwadi
Workers
(78,929)
+1231 New
ly
sanctioned
AWC )
Anganwadi
Helper
(78,929)+
1231 Newly
sanction
AWC
Mini
Anganwadi
Workers
(12,070 )

30
Table I. Revised Population Norms for establishing AWCs under ICDS program
Old Revised
CDPO Block 30,000 to 1,00,000 – 1/project
A unit for sanction of an ICDS
project in Rural/tribal
irrespective of villages &
population
For blocks with >2lac population,
state could opt for more than one
project on one per 1lac. In the
later case staff could be suitably
strengthened.
Sector Supervisor 20,000 to 30,000 – 1/sector 25,000 – 1/Sector
AWC Rural/ urban one AWC on a population of
500-1500
400 to 800 – 1 AWC
800 to 1600 – 2 AWC
1600 to 2400 – 3 AWC
In multiples of 800/AWC
Mini AWC 150 to 500 – 1 Mini AWC 150 to 400 – 1 Mini AWC
AWC tribal 300 to 1500 – 1 AWC
150 to 300 – 1 Mini AWC
300 to 800 – 1 AWC
150 to 300 – 1 Mini AWC
In MP, ICDS program functions under the Department of Women and Child Development. It
has a separate Directorate headed by a Director/Commissioner. In the district the
organization is headed by the District Program Officer (DPO). In larger districts he is
supported by DWCDO (District Woman and Child Development Officer). At the block level,
the program is managed by Child Development Project Officer (CDPO) assisted by
Assistant Statistical Officer and Assistant Project Officer. At the village level each AWW has
two honorary workers viz. Anganwadi Worker (AWW) and Anganwadi Helper (AWH). For
every 25 AWCs a Supervisor has been provided. The area covered by the Supervisor is
known as a sector.
b) Office infrastructure at state, district and block level
As mentioned earlier the Department of DWC has recently moved in a new building of its
own. At the district level, most offices of DPOs are housed in rented buildings with a few
exceptions where DPO offices are located in the district collector building or some other
government building. Out of 313 Block offices, headed by CDPO, 165 have their own
building while the remaining is in rented building.
c) ICDS program in MP is headed by a Commissioner who is an IAS officer
d) Committee/ Task Force on ICDS
The State has constituted a Core Group under the chairmanship of Director, Department of
Women and Child Development for preparation of Annual PIP. Joint Directors (ICDS and
WCD), District Program Officers of DWCD, representatives from Partner organizations
(DEVELOPMENT PARTNERS, DIFD, etc) are members of the Core Group.
Representatives from Department of Panchayat and Rural Development, BRGF, Public
Health Engineering are also invited to the Core Group meetings. The Core Group provides
guidance for preparation of the Annual PIP.
GOMP has also constituted a Steering Committee for implementation of Annual PIP. The
Steering Committee is chaired by the Principal Secretary, WCD. Principal Secretary/
Secretary of line departments e.g. Department of Planning, Public Health Engineering,
Public Health and Family Welfare, Panchayat and Rural Development are members of the
Steering Committee. Representatives of GOI, NIPCCD and Collectors of selected districts

31
are other members of the Steering Committee. The Steering Committee will ensure that the
activities proposed under Annual PIP of ICDS are implemented effectively.
e) Devolution of powers at the state/ district/block levels
Government orders have been issued for decentralization of functions and devolution of
power for smooth functioning of the ICDS activities. For example, appointment of AWW is
done by CDPO with recommendations of the respective Gram Sabhas. Similarly,
procurement of Pre- School kits and other supplies, etc. have been entrusted to the district
and block level officers. Planning of annual activities of ICDS is carried out in consultation
with community at the grass root level. PRI representatives at Panchayat, block and district
level are associated with program planning and review. Further details are given in section
4-I. “Community Participation & Involvement of PRIs” (page 66).

32
Section 4
ANNUAL ACTION PLAN- PROGRAM COMPONENTS
4A. HUMAN RESOURCES
a. State’s recruitment process The Human Resource Policy of Madhya Pradesh follows the qualifications and other norms prescribed by GOI for recruitment of staff. The process of recruitment and promotion are briefly described below:
i) Recruitment of AWWs The minimum qualification prescribed by GOI for selection of AWWs is Matriculation. But few AWWs, recruited earlier, do not possess the minimum prescribed qualification. Classification of AWWs as per their qualifications is as below:
Table 4A.1: Classification of AWWs as per their educational qualifications
Illiterate V
standard or less
VI- VIII standard
IX -XII standard
pass Graduate
Post –graduates
Total
5959 6790 14709 35461 10946 4991 78856
Majority (44.97%) of AWWs belong to IX to XII education group. About 34.82% AWWs hold less than the recommended educational qualification. This includes 16.17% AWWs who are either illiterate or have education up to fifth standard only. This has implications for programme implementation as well trainability of the workers. In tribal and difficult areas, women with required educational qualifications are often not available for selection. There is a provision of relaxation of educational qualifications’ norms in such cases. Honorarium of AWWs as per their educational qualifications and experience is listed in the table below:
Table 4.A.2 Honoraria scale of AWWs in accordance with their education and experience
S.N. Qualification & experience of
AWW Honorarium (Rs) (w.e.f. 01.04.08)
Honorarium (Rs) (w.e.f. 01.04.11)
1 Non-Matriculate 1438 2938
2 Non-Matriculate with 5 years of work
1469 2969
3 Non-Matriculate with 10 years of work
1500 3000
4 Matriculate 1500 3000
5 Matriculate with 5 yrs honorary work 1531 3031
6 Matriculate with 10 yrs honorary work
1563 3063
7 Aanganwadi Helper 750 1500
8 AWW of Mini AWC 750 1500
Selection of AWWs is made by CDPO on the recommendation of Gram Sabha. For selection of AWW, it is essential that she should be a resident of the local village.
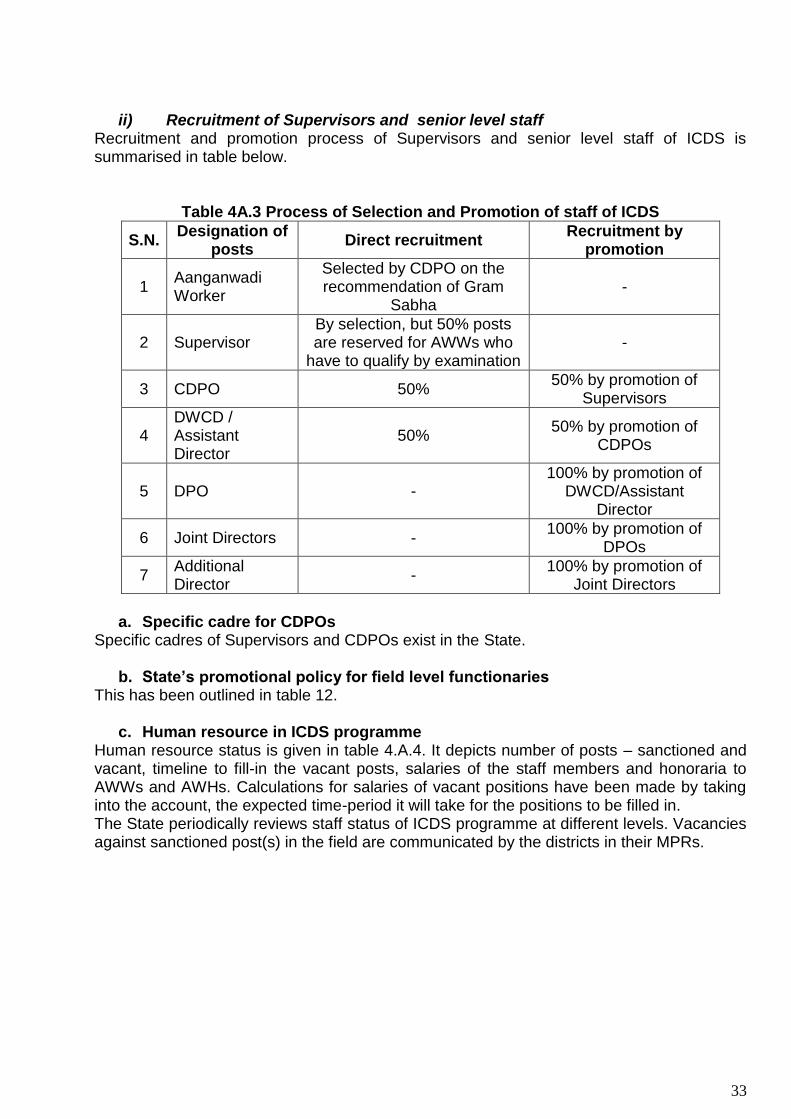
33
ii) Recruitment of Supervisors and senior level staff Recruitment and promotion process of Supervisors and senior level staff of ICDS is summarised in table below.
Table 4A.3 Process of Selection and Promotion of staff of ICDS
S.N. Designation of
posts Direct recruitment
Recruitment by promotion
1 Aanganwadi Worker
Selected by CDPO on the recommendation of Gram
Sabha -
2 Supervisor By selection, but 50% posts are reserved for AWWs who
have to qualify by examination -
3 CDPO 50% 50% by promotion of
Supervisors
4 DWCD / Assistant Director
50% 50% by promotion of
CDPOs
5 DPO - 100% by promotion of
DWCD/Assistant Director
6 Joint Directors - 100% by promotion of
DPOs
7 Additional Director
- 100% by promotion of
Joint Directors
a. Specific cadre for CDPOs
Specific cadres of Supervisors and CDPOs exist in the State.
b. State’s promotional policy for field level functionaries This has been outlined in table 12.
c. Human resource in ICDS programme Human resource status is given in table 4.A.4. It depicts number of posts – sanctioned and vacant, timeline to fill-in the vacant posts, salaries of the staff members and honoraria to AWWs and AWHs. Calculations for salaries of vacant positions have been made by taking into the account, the expected time-period it will take for the positions to be filled in. The State periodically reviews staff status of ICDS programme at different levels. Vacancies against sanctioned post(s) in the field are communicated by the districts in their MPRs.

34
Table 4 A.4: Human resource status in ICDS programme
Designation Sanctione
d Posts In
Position
Timeline for
filling-up vacancie
s
Salary/Honoraria per month
Estimated budgetary requirement for the FY 12-13
(Rs.; Lakhs)
State Level
Commissioner / Director 1 1
37400+67000+10000= 98276 11.79
Additional Director/Joint Director 2 2
37400-67000+8700= 96222 23.09
Joint Director/ Finance Advisor 12 12
37400-67000+7600=94484 136.06
Deputy Director 4 4 15600-39100+ 6600 25.75
Assistant Director 8 8 15600-39100+ 5400 49.68
Account Officer 1 1 15600-39100+ 5400 6.21
Superindendent 1 1 9300-34800+3600 4.86
Senior Auditor 1 1 9300-34800+3600 4.86
Astt. Supdtt. 1 1 9300-34800+3200 4.79
ASO 6 6 9300-34800+3600 2.92
Stenographer grade 1 2 2 9300-34800+4200 9.95
Stenographer grade 2 2 2 9300-34800+3600 9.73
Stenographer grade 3 6 6 5200-20200+2800 17.63
Asstt. Grade 1 6 6 5200-20200+2800 17.63
Data Entry Operator 4 4 5200-20200+2400 11.45
Assistant Grade 2/ accountant 7 7 5200-20200+2400 20.04
Assistant Grade 3 / Steno Typist 14 14 5200-20200+1900 38.76
Peon/Watchman/Sweeper/Cleaner 10 10 4440-7440+1300 13.73
Driver 10 10 5200-20200+1900 27.68
TOTAL 98 98 436.62

35
District Level Position
Designation Sanctioned
Posts In
Position
Timeline for filling-
up vacancies
Salary/Honoraria per month
Estimated budgetary
requirement for the FY
12-13 (Rs.; Lakhs)
DPO 48 30 3rd Qtr 55300.00 258.80
ASO 20 09 3rd Qtr 53641.00 93.34
Office Superintendent 14 03 3rd Qtr 39500.00 40.29
UDC 32 21 3rd Qtr 23700.00 75.37
LDC/Typist 41 30 3rd Qtr 23700.00 100.96
Peon 41 30 3rd Qtr 9480.00 40.38
Driver 30 30 - 23384.00 84.18
Chowkidar 5 5 - 27492.00 16.50
Total 231 158 709.82
Block level
CDPO 453 269 QIII 41080.00 1779.59
ACDPO 108 103 Dying cadre 39500.00 488.22
Assitant/Statistical Assitant 258 153
QIII 39500.00 974.07
Supervisor 3157 2728 Q III
2012-13 23700.00
8368.47
Clerk/typist 380 363 2012-13 23700.00 1056.55
Asstt. Grade I 241 153 2012-13 23700.00 435.13
Asstt. Grade II 296 143 2012-13 23700.00 406.69
Peon 562 503 Dieying cadre
9480.00 605.77
Driver 375 282 Dieying cadre
23384.00 791.31
Total Block level 5830 4697 - 14905.80
AWC Level
AWW* 80160 77086 2012-13 3000.00 28580.94
AWW (Mini) 80160 76188 2012-13 1500.00 14250.06
AWH* 12070 12070 2012-13 1500.00 2172.6
Total 172390 165344 - 45003.6

36
State’s additional contribution for honoraria of AWWs and AWHs The State’s HR policy is worker oriented. The AWWs and AWHs are paid additional honoraria by the State Government from its own budget. The AWWs are paid additional Rs 1000 per month; thus, raising their total honorarium to Rs. 2500 from Rs. 1500 paid under ICDS norms. Similarly, the AWHs are paid additional honoraria of Rs. 500 per month. Time for filling of different vacant posts has been shown in the table 14: Time Line of Activities (2012-13) at page 73. Detailed calculation of the salary/ honorarium has been given in Annexure 9.
a. LIC coverage for AWWs and other welfare measures Government of India introduced ‘Social Group Insurance Scheme of LIC of India for AWWs’, with effect from October 1, 2004. The scheme covers all AWWs and AWHs, on voluntary basis on their part. The name of the scheme is ‘AWWs Group Insurance Scheme’. The Government of MP accepted to implement the scheme and issued instructions to all District Collectors to implement the scheme (vide letter no. WCD/2004/F-3-18/04/50-2 dated 23.09.2004) with immediate effect.
f) LIC coverage for AWWs and any other welfare measures
Government of India introduced Social Group Insurance Scheme of LIC of India for AWWs
with effect from 1st Oct 2004. The scheme covers all AWWs and Anganwadi Helpers on a
voluntary basis. The name of the scheme is AWWs Group Insurance Scheme. The
government of MP accepted to implement the scheme. It issued instructions to all the
District Collectors to implement the scheme vide letter no. WCD/2004/F-3-18/04/50-2 dated
23.09.2004 with immediate effect.
2010-2011 2011-2012
Lodged Settled Amount
disbursed
Lodged Settled Amount
disbursed
No. of claims by AWWs and Helpers
Natural death 48 48 1400000.00 62 62 1860000.00
Accidental death 6 6 45000.00 7 7 525000.00
Critical illness 1 1 20000.00 1 1 20000.00
Scholarship 532 532 324000.00 1273 1273 763800.00
4B: Procurement of Materials and Equipments
a) Status of supply of equipments
No. and percentage of blocks with functional computers and printers
There are 453 Projects in the state. In the financial year 2012-13, budget is being
allotted to all the projects (453), DPOs(50), JDs office (07) and Government owned
Aaganwadi workers Training Centres (10), to procure computer and accessiories that
includes Desktop, CPU, Printer, UPS, Inverter and Borad band connections (Rs. 1000
per month / per office is allotted.
No. and percentage of District offices having functional computers/ printers

37
Functional computers are available at all the fifty District cells. In the financial year
budget is allotted to all the DPOs to make replacement of computers and
accessaries.
Functional vehicles at state, district and block level
Out of 453 CDPO offices 272 have vehicles in running condition. Remaining 181
offices hire vehicles for program activities. Further, out of 50 District cells 36 have
vehicles in working condition while the remaining 14 district cells are using hired
vehicles. At the state level there are 30 owned vechiles and 11 Private Vechiles.
No .of functional AWCs having baby and adult weighing machines-
Out of 78,929 AWCs in the state 33226 AWCs had baby weighing scales out of
which 28373 machines are in working condition (for newborns) and 60422 Salter
scales are vailable at AWCs out of which 56593 in working condition and 42022
Adult weighing machines are available at AWCs out of which 34675 are in working
condction. (MPR, March, 2012.). The requirement of baby weighing scale is 51787
and Salter scale is 23537 and adult weighing machine 45485 is required during
current financial year which included weighing machines for newly sanctioned 1231
AWCs too and demnd for 19729 MUAC tape is being placed by district to the state
for financial year 2012-13.
Table 4.B.1: List of material and equipment, and their costs, to be procured
Items
No. available
in working
condition
No. to be procured
during the year
Estimated budgetary
requirement(Rs.)
Timeline of supply
during FY (Tentative
date)
Means of Verification (MPRs/UCs)
State level
Computer with Printer+UPS
12 10 5.0 lakhs
@ Rs. 50,000 3rd Quarter 5.00 lakhs
Photocopier - 2 2.0 lakhs
@ Rs. 1,00,000 3rd Quarter 2.00 lakhs
Scanner 3 1 0.2 lakhs
@ Rs. 20,000 3rd Quarter 0.2 lakhs
Laptops 8 4 2.4 lakhs
@ Rs. 60,000 4th Quarter 2.4 lakhs
Water Cooler with RO
- 3 0.75 lakh
@ Rs. 25,000 2nd Quarter 0.75 lakhs
AC Split 1 2 0.70 lakhs
@ Rs. 35,000 2nd Quarter 0.70 lakhs
AC Window - 6 1. 5 lakh
@ Rs. 25,000 2nd Quarter 1.5 lakhs
Steel Almirah 15 10 1.0 lakh
@ Rs. 10,000 2nd Quarter 1.0 lakhs
Total procurement for state cell 13.55 lakhs

38
Items
No. available
in working
condition
No. to be procured
during the year
Estimated budgetary
requirement(Rs.)
Timeline of supply during FY (Tentative
date)
Means of Verification (MPRs/UCs)
District Level (total 50 districts)
Computer cum Printer
50 10 need
replacement
5.0 lakhs @ Rs. 50,000
3rd Quarter
5.0 lakhs
Equipment / Furniture, etc.
50 Districts 25.0 lakhs
@ Rs. 50,000 2nd
Quarter 25.00 lakhs
Total procurement at district level 30.0 lakh
Block Level (total 453 Projects)
Computer cum Printer/ UPS
253 200 need replaceme
nt
100.0 lakhs @ Rs. 50,000
3rd Quarter
100.0 lakh
Other equipment, furniture, etc.
453
Projects 226.5 lakhs
@ Rs. 20,000/project 3rd/ 4th
Quarter 226.50 lakh
Total procurement at Blocks level 326.50 lakh
AWC Level
PSE Kit 80160 801.6 lakhs
@ Rs. 1000/AWC/year
2nd Quarter
801.6 lakhs
PSE Kit mini AWC
12070 @ Rs
500.00/AWC/Year 2nd Qtr 60.35 lakhs
Medicine Kit 80160 480.96 lakhs
@ Rs. 600/AWC/year 2nd
Quarter 480.96 lakhs
Medicine Kit Mini AWc
@ Rs 300.00 /AWC/Year
2nd Qtr 36.21 lakhs
Weighing Scales Baby Weighing Scales Salter Weighing scales
28373
56593
51787
23537
@Rs.10000.00
@ 750
2nd Quarter
517.87 lakh
176.52 lakh
Adult weighing scales
29849 available
45485 required
@ Rs. 1000/AWC 2nd
Quarter 454.85 lakh
Items
No. available
in working
condition
No. to be procured
during the year
Estimated budgetary
requirement(Rs.)
Timeline of supply during FY (Tentative
date)
Means of Verification (MPRs/UCs)
Storage boxes, other equipments
- For 51231
AWCs @ Rs. 5000/ AWC
2nd & 3rd quarter
2561.55 lakhs
Total for AWCs 508.91 lakhs
Total procurements at state, district, block & AWC level 5419.05 lacs
i. Requirement during the FY (2011-12)
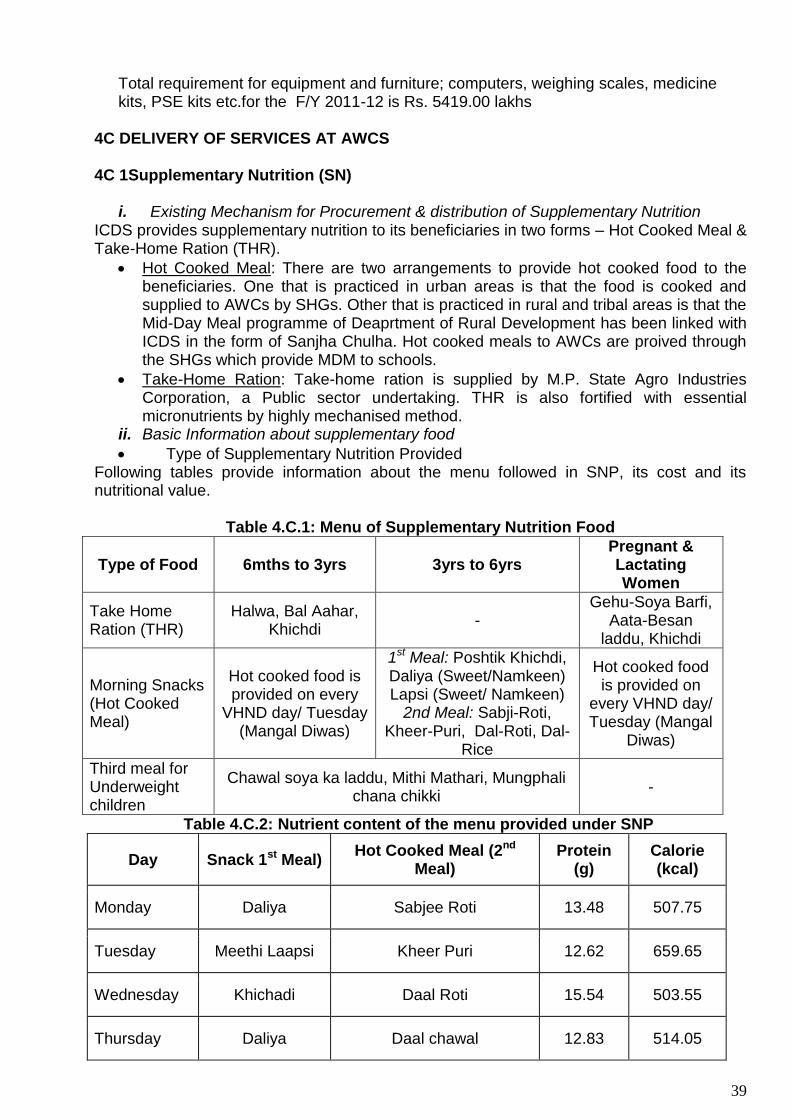
39
Total requirement for equipment and furniture; computers, weighing scales, medicine kits, PSE kits etc.for the F/Y 2011-12 is Rs. 5419.00 lakhs
4C DELIVERY OF SERVICES AT AWCS
4C 1Supplementary Nutrition (SN)
i. Existing Mechanism for Procurement & distribution of Supplementary Nutrition ICDS provides supplementary nutrition to its beneficiaries in two forms – Hot Cooked Meal & Take-Home Ration (THR).
Hot Cooked Meal: There are two arrangements to provide hot cooked food to the beneficiaries. One that is practiced in urban areas is that the food is cooked and supplied to AWCs by SHGs. Other that is practiced in rural and tribal areas is that the Mid-Day Meal programme of Deaprtment of Rural Development has been linked with ICDS in the form of Sanjha Chulha. Hot cooked meals to AWCs are proived through the SHGs which provide MDM to schools.
Take-Home Ration: Take-home ration is supplied by M.P. State Agro Industries Corporation, a Public sector undertaking. THR is also fortified with essential micronutrients by highly mechanised method.
ii. Basic Information about supplementary food
Type of Supplementary Nutrition Provided Following tables provide information about the menu followed in SNP, its cost and its nutritional value.
Table 4.C.1: Menu of Supplementary Nutrition Food
Type of Food 6mths to 3yrs 3yrs to 6yrs Pregnant & Lactating Women
Take Home Ration (THR)
Halwa, Bal Aahar, Khichdi
- Gehu-Soya Barfi,
Aata-Besan laddu, Khichdi
Morning Snacks (Hot Cooked Meal)
Hot cooked food is provided on every
VHND day/ Tuesday (Mangal Diwas)
1st Meal: Poshtik Khichdi, Daliya (Sweet/Namkeen) Lapsi (Sweet/ Namkeen)
2nd Meal: Sabji-Roti, Kheer-Puri, Dal-Roti, Dal-
Rice
Hot cooked food is provided on
every VHND day/ Tuesday (Mangal
Diwas)
Third meal for Underweight children
Chawal soya ka laddu, Mithi Mathari, Mungphali chana chikki
-
Table 4.C.2: Nutrient content of the menu provided under SNP
Day Snack 1st Meal) Hot Cooked Meal (2nd
Meal) Protein
(g) Calorie (kcal)
Monday Daliya Sabjee Roti 13.48 507.75
Tuesday Meethi Laapsi Kheer Puri 12.62 659.65
Wednesday Khichadi Daal Roti 15.54 503.55
Thursday Daliya Daal chawal 12.83 514.05

40
Friday Meethi Laapsi Daal Roti 15.51 541.20
Saturday Khichadi Sabjee Roti 13.48 507.75
Table 4.C.3: Third meal, and its nutrient content, for children between 6 months
and 6 years
Day Recipe Protein Calorie
Monday Chawal soya ka laddu 13.48 507.75
Tuesday Mithi Mathari 12.62 659.65
Wednesday Mungphali chana chikki 15.54 503.55
Thursday Mithi Mathari 12.83 514.05
Friday Mungphali chana chikki 15.51 541.20
Saturday Chawal soya ka laddu 13.48 507.75
iii. Cost (per unit) of supplementary nutrition
Table 4.C.4: Per unit cost of supplementary nutrition
Target Group
Rates per beneficiary (in Rs.) (Per beneficiary per day)
Pre – revised Revised
Children 6 months to 6 yrs 2.00 4.00
Severely undernourished children
2.70 6.00
Pregnant women and Nursing mothers
2.30 5.00
Note: Fifty percent of the cost of supplementary nutrition is met by the state government
iv. Adherence to calorific norms as prescribed by GOI and quantity per child/women per day
The rates and calorie and protein content of the SNP provided to pregnant, lactating
mothers & children 6 months to 6 years by ICDS were revised in 2009 (State Government’s
circular number F 3-2/09/50-2, dated 28.2.2009). The revised norms are mentioned in the
table below:
Table 4.C.5: Revised nutrient content of SNP food
Target Group
Pre-revised (per beneficiary per day)
Revised (per beneficiary per day)
Calories (kcal)
Protein (g) Calories
(kcal) Protein (g)
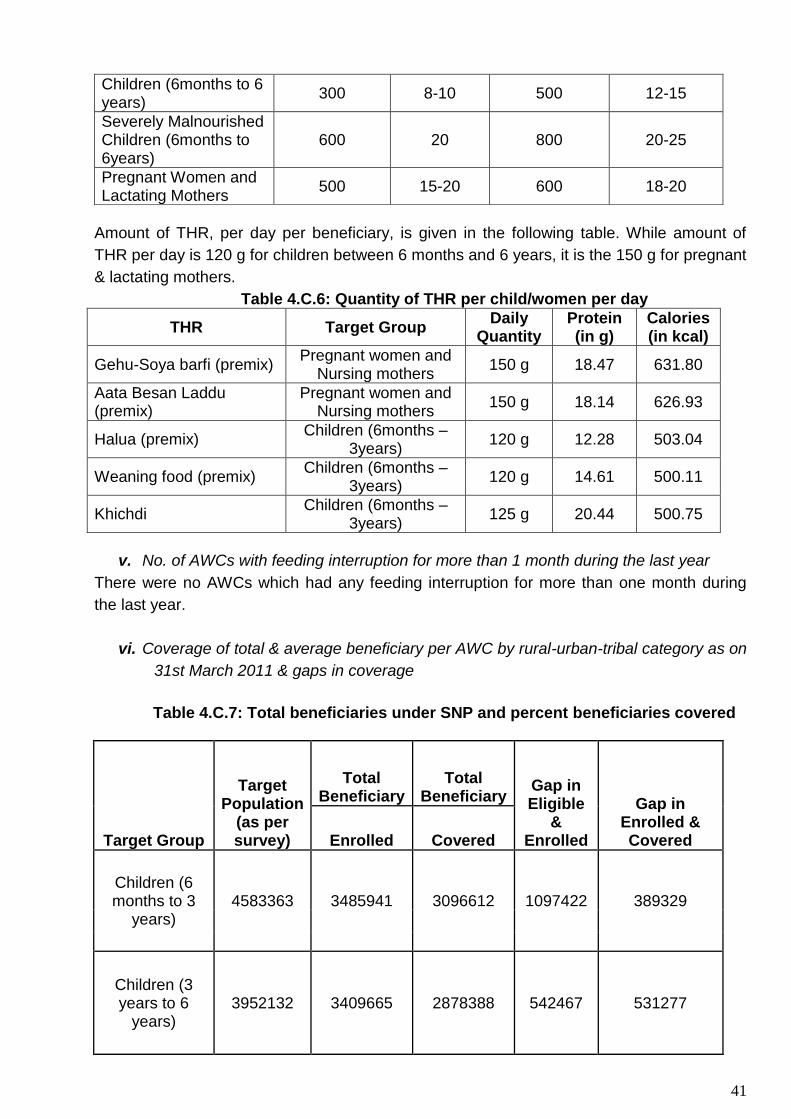
41
Children (6months to 6 years)
300 8-10 500 12-15
Severely Malnourished Children (6months to 6years)
600 20 800 20-25
Pregnant Women and Lactating Mothers
500 15-20 600 18-20
Amount of THR, per day per beneficiary, is given in the following table. While amount of
THR per day is 120 g for children between 6 months and 6 years, it is the 150 g for pregnant
& lactating mothers.
Table 4.C.6: Quantity of THR per child/women per day
THR Target Group Daily
Quantity Protein (in g)
Calories (in kcal)
Gehu-Soya barfi (premix) Pregnant women and
Nursing mothers 150 g 18.47 631.80
Aata Besan Laddu (premix)
Pregnant women and Nursing mothers
150 g 18.14 626.93
Halua (premix) Children (6months –
3years) 120 g 12.28 503.04
Weaning food (premix) Children (6months –
3years) 120 g 14.61 500.11
Khichdi Children (6months –
3years) 125 g 20.44 500.75
v. No. of AWCs with feeding interruption for more than 1 month during the last year
There were no AWCs which had any feeding interruption for more than one month during
the last year.
vi. Coverage of total & average beneficiary per AWC by rural-urban-tribal category as on
31st March 2011 & gaps in coverage
Table 4.C.7: Total beneficiaries under SNP and percent beneficiaries covered
Target Group
Target Population
(as per survey)
Total Beneficiary
Total Beneficiary
Gap in Eligible
& Enrolled
Gap in Enrolled & Covered Enrolled Covered
Children (6 months to 3
years) 4583363 3485941 3096612 1097422 389329
Children (3 years to 6
years) 3952132 3409665 2878388 542467 531277

42
Pregnant women
671818 667541 628212 4277 39329
Lactating women
741367 687816 640474 53551 47342
i. Special strategy for cut off area planning during monsoon In Madhya Pradesh, THR is supplied from MP Agro. On the basis of demands received from districts, MP Agro supplies THR from Bhopal and Indore, maintaining rotation cycle of one month. During rainy season, several villages in the State get cut-off from the district headquarter, mainly because of affected roads. Approximately, 8-10% of total AWCs get affected during monsoons. Districts know of these villages by experience. To ensure there is no disruption in the supply of SNP in such villages, districts sanction stock of SNP for two to three months in advance.
ii. Differential strategy for tribal & rural areas in collaboration with department of Tribal development
Since the inception of ICDS programme, different mechanisms for preparation & distribution of supplementary nutrition have been adopted for effective implementation of the programme. After the introduction of new Nutrition Policy in February 2007, a standard reference list of menu and revised cost along with revised calorie-protein values has been provided to all the districts (vide letter number F3-1/07/50-2of dated 15.2.2007). Earlier, preparation of supplementary nutrition at Anganwadi centers required a lot of preparation and consumed considerable time of AWWs. The AWWs are supposed to provide six services including daily organization of preschool education for children aging 3-6years, In view of this constraint, ICDS linked supplementary nutrition program with MDM program of department of tribal development. This arrangement is named as Sanjha Chulha. It is effective from 1st November 2009. As per the Sanjha Chulha initiative the SHG who was preparing food for school children prepares supplementary nutrition in the same kitchen for anganwadis as well. The SHG provides the food to the AWCs as per the fixed weekly Menu & cost following the revised norms of ICDS. Distribution of food to the beneficiaries is done by the AWW. The AWWs collects the cooked food from the Sanjha Chulha kitchen. Where Sanjha Chulha kitchen is at a distance from AWC, SHG delvers the food to the centre. In this case transportation cost is paid from administrative budget head by the CDPO. The norms for the transportation cost are: if the distance of AWC from the MDM kitchen is within 100mts then no transportation cost is paid. On the other hand, for distance between 101 to 500mts Rs. 250/month and for distance between 501 to 1000mts Rs. 500/month is paid as transportation cost to SHG. The SHG prepares food daily for all the children aged 3-6years. But on Tuesdays the pregnant & lactating mothers and 6months to 3years children coming to AWC are also served nutrition supplement. Revised guidelines were issued by the department on 27.8.2009 for implementation of Sanjha Chulha scheme. Along with the regular supplementary nutrition to all the beneficiaries, a special provision of third meal has been introduced by the State for all severely underweight children. As per the guidelines provided wide letter no.F3-2/09/50-2 dt. 10th November 2009, all the severely underweight children of age 6months to 6years are provided food with 800 kcal and 20-25gms of protein. The following table explains the third meal cost & nutritive value recommended & currently in practice for children 6 months to 3 years who are getting THR.
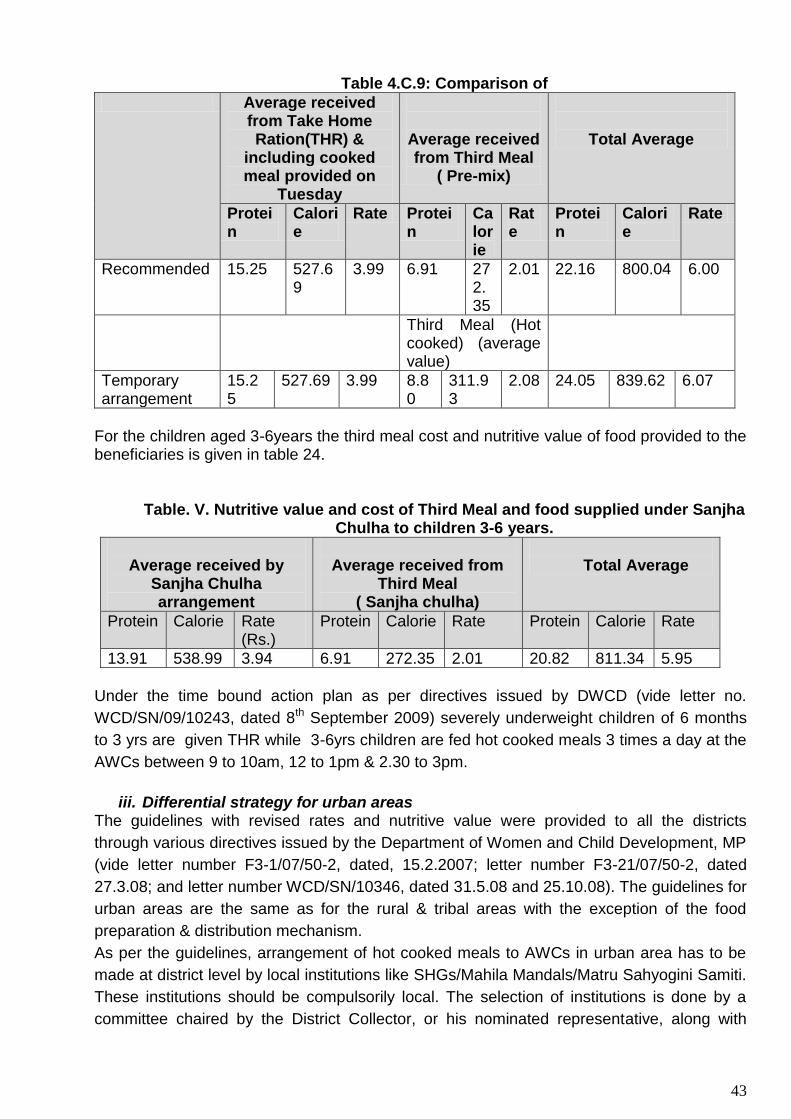
43
Table 4.C.9: Comparison of
Average received from Take Home Ration(THR) &
including cooked meal provided on
Tuesday
Average received from Third Meal
( Pre-mix)
Total Average
Protein
Calorie
Rate Protein
Calorie
Rate
Protein
Calorie
Rate
Recommended 15.25 527.69
3.99 6.91 272.35
2.01 22.16 800.04 6.00
Third Meal (Hot cooked) (average value)
Temporary arrangement
15.25
527.69 3.99 8.80
311.93
2.08 24.05 839.62 6.07
For the children aged 3-6years the third meal cost and nutritive value of food provided to the beneficiaries is given in table 24.
Table. V. Nutritive value and cost of Third Meal and food supplied under Sanjha Chulha to children 3-6 years.
Average received by
Sanjha Chulha arrangement
Average received from
Third Meal ( Sanjha chulha)
Total Average
Protein Calorie Rate (Rs.)
Protein Calorie Rate Protein Calorie Rate
13.91 538.99 3.94 6.91 272.35 2.01 20.82 811.34 5.95
Under the time bound action plan as per directives issued by DWCD (vide letter no.
WCD/SN/09/10243, dated 8th September 2009) severely underweight children of 6 months
to 3 yrs are given THR while 3-6yrs children are fed hot cooked meals 3 times a day at the
AWCs between 9 to 10am, 12 to 1pm & 2.30 to 3pm.
iii. Differential strategy for urban areas
The guidelines with revised rates and nutritive value were provided to all the districts
through various directives issued by the Department of Women and Child Development, MP
(vide letter number F3-1/07/50-2, dated, 15.2.2007; letter number F3-21/07/50-2, dated
27.3.08; and letter number WCD/SN/10346, dated 31.5.08 and 25.10.08). The guidelines for
urban areas are the same as for the rural & tribal areas with the exception of the food
preparation & distribution mechanism.
As per the guidelines, arrangement of hot cooked meals to AWCs in urban area has to be
made at district level by local institutions like SHGs/Mahila Mandals/Matru Sahyogini Samiti.
These institutions should be compulsorily local. The selection of institutions is done by a
committee chaired by the District Collector, or his nominated representative, along with
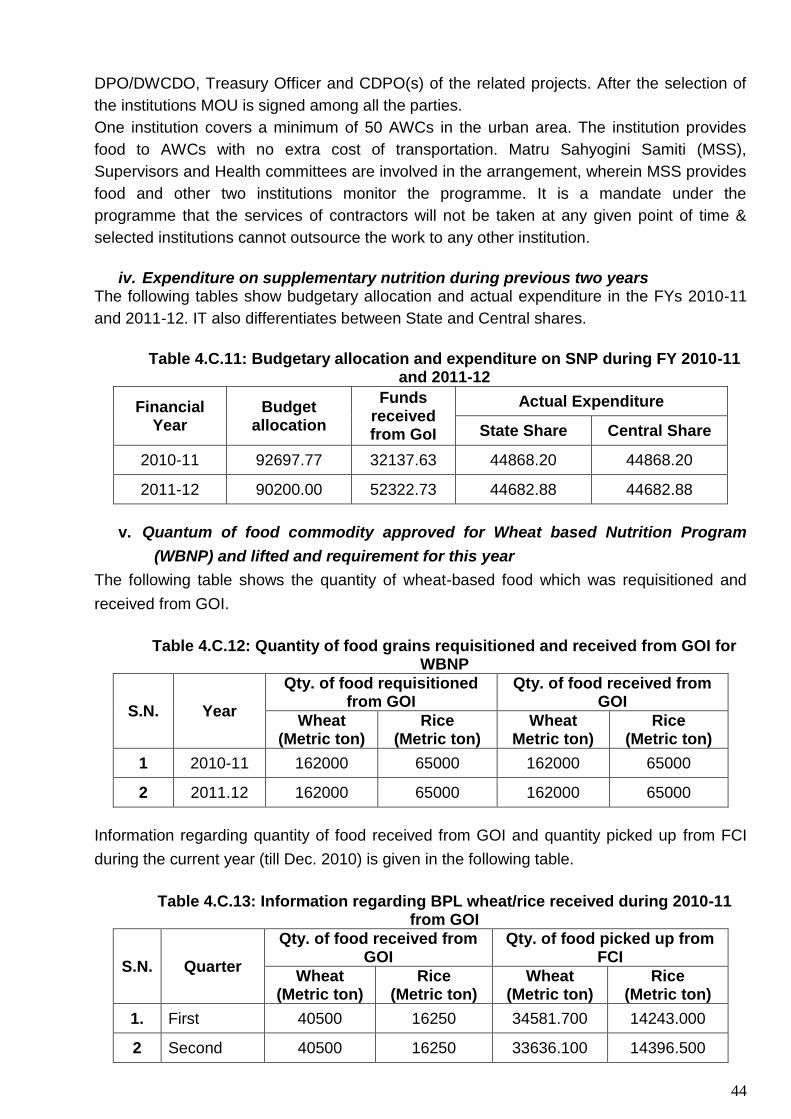
44
DPO/DWCDO, Treasury Officer and CDPO(s) of the related projects. After the selection of
the institutions MOU is signed among all the parties.
One institution covers a minimum of 50 AWCs in the urban area. The institution provides
food to AWCs with no extra cost of transportation. Matru Sahyogini Samiti (MSS),
Supervisors and Health committees are involved in the arrangement, wherein MSS provides
food and other two institutions monitor the programme. It is a mandate under the
programme that the services of contractors will not be taken at any given point of time &
selected institutions cannot outsource the work to any other institution.
iv. Expenditure on supplementary nutrition during previous two years
The following tables show budgetary allocation and actual expenditure in the FYs 2010-11
and 2011-12. IT also differentiates between State and Central shares.
Table 4.C.11: Budgetary allocation and expenditure on SNP during FY 2010-11
and 2011-12
Financial Year
Budget allocation
Funds received from GoI
Actual Expenditure
State Share Central Share
2010-11 92697.77 32137.63 44868.20 44868.20
2011-12 90200.00 52322.73 44682.88 44682.88
v. Quantum of food commodity approved for Wheat based Nutrition Program
(WBNP) and lifted and requirement for this year
The following table shows the quantity of wheat-based food which was requisitioned and
received from GOI.
Table 4.C.12: Quantity of food grains requisitioned and received from GOI for
WBNP
S.N. Year
Qty. of food requisitioned from GOI
Qty. of food received from GOI
Wheat (Metric ton)
Rice (Metric ton)
Wheat Metric ton)
Rice (Metric ton)
1 2010-11 162000 65000 162000 65000
2 2011.12 162000 65000 162000 65000
Information regarding quantity of food received from GOI and quantity picked up from FCI
during the current year (till Dec. 2010) is given in the following table.
Table 4.C.13: Information regarding BPL wheat/rice received during 2010-11
from GOI
S.N. Quarter
Qty. of food received from GOI
Qty. of food picked up from FCI
Wheat (Metric ton)
Rice (Metric ton)
Wheat (Metric ton)
Rice (Metric ton)
1. First 40500 16250 34581.700 14243.000
2 Second 40500 16250 33636.100 14396.500

45
3 Third 40500 16250 38181.500 14477.028
4 Fourth 40500 16250 33170.000 14215.000
Total 162000 65000 139569.300 57331.528
The Department of WCD has submitted to GOI a demand of 162000 metric tonnes of wheat and 65000 metric tonnes of rice for WBNP scheme for the FY 2011-12.
vi. Estimated budgetary requirements for the FY (2011-12) The table given below summarises the budgetary requirement for the year 2012-13.
Table 4.C.14: Budgetary requirement for FY 2012-13
Beneficiaries
Population as per AWW’s survey register (March 2012)
No. of beneficiaries
(as on March 2012)
Target for
current year
Unit cost (Rs.)
Budgetary requireme
nt for current FY
(Rs.; Lakh)
Means of verification (MPRs/UCs)
Children (6m-3y) 4583363 3096612 4500000 4 54000 MPR Mar 13
Children (3y-6y) 3952132 2878388 4000000 4 48000 MPR Mar 13
Pregnant Women 671818 628212 670000 5 10050 MPR Mar 13
Lactating Mothers 741367 640474 740000 5 11100 MPR Mar 13
Severe Underweight children 187599 187599 187599 6 3376.78 MPR Mar 13
Total 126526.78 -
xii) Growth Monitoring & Promotion:
No. and percentage of AWCs using WHO New Growth Charts:
After March 2010 most of the AWCs started using New WHO Growth Standards for
growth monitoring of children. But proper recording and reporting to Directorate of WCD
could start from December 2010 onwards only. Grading of nutritional status of children
as per the new standards will be reflected in MPR from next F/Y.
Percentage of AWCs using New Mother & Child Health Cards/any other tools for
counseling:
New MCP Card was launched by the Hon. Chief Minister of MP in 2007. The card was
jointly printed by the DWCD and Department of Health and Family Welfare.
DEVELOPMENT PARTNERS state office of MP also shared the printing expenses of
MCP cards.
Growth monitoring/ Promotion and Children’s Nutritional status:
The state has started using WHO New Growth Standards since 2010 onward. Distribution of
nutritional status of children using weight for age criteria (MPR March 2012) is shown in the
following graph.

46
Graph showing overall nutritional status of children from birth to 5yrs
(Using WHO New Growth Standards)
4 C2. Pre-school Education (PSE)
a) State Policy/guidelines/curricula for Pre-school Education & Pre-School Kits in ICDS:
The pre-school education component under ICDS Scheme is an important component of the
package of services envisaged under the scheme. It aims at school readiness and
development of positive attitudes towards education. Strengthening of pre-school education
would also supplement the effort in achieving the national goal of universal primary
education. It is to be noted that right to education, which has been accepted by the
government as a national policy cannot succeed without PSE.
The Pre-School Education in Anganwadi centers is provided through non-formal and play
way methods by joyful learning. The age group of 3-6 years can be termed as school
preparatory stage where the emphasis should be on development of cognitive processes
along with motor & muscular development: The child can be guided to develop pre-number
concepts such as differences between more & less, thick & thin, far & near etc. During this
age concept formation and language development also need to be facilitated by organizing
activities like pre-conversation, story telling, rhyming songs, vocabulary building etc.
Emotional and social developments are other areas which need careful intervention.
As per the guidelines issued wide letter no. 4-4/2008-CD-II dated 11th May 2009 by Ministry
of Women & Child Development, GOI Pre-School Kits are provided each year for all
operational Anganwadi Centers in the State @ Rs.1000/-, per AWC per annum. M.P. opted
for providing more than one kit having age appropriate TLM (Teaching & Learning
Material).Two kits were designed one each for less than 3years, and more than 3 years
children. The items in the kit were multiple in terms of possible play activities & concepts,
durable, safe for children (non-toxic & without sharp edges), culturally and environmentally

47
relevant, cost-effective, easy to maintain, handle and store, conducive to creativity and
problem solving.
The Pre-school Education program in terms of content, curriculum, duration, etc follows
MOWCD, GOI guidelines. In the past, PSE program had not received adequate attention
under the ICDS program due to a number of reasons. The scene has changed considerably
in recent years. There is now greater awareness among the community to enroll children for
pre-school education. The recent initiative of the state to increase the working hours of AWC
by offering additional honoraria to AWW and AWH as well supply of pre cooked food under
its Sanjha Chulha initiative has resulted into sufficient time to AWW to devote to joyful
learning activities.
b) Number & percentage of AWCs (against total operational) having received PSE
kits during the previous year:
AWCs have been supplied Pre-school Education kits for teaching learning of children
between 3-6 years attending AWCs. Each AWC is supplied one kit on annual basis. Since
2000, procurement of the kits has been done by the state government as per the decision of
MOWCD, GOI. Guidelines provided by the Ministry for procurement of PSE kits are followed
by MP. The cost of the kit has been raised from Rs 500 to Rs 1000 by GOI. The State
government has now decentralized procurement of PSE kits to the districts thus ensuring
timely supply to the AWCs. The directives for procurement of the PSE kits for the year 2010-
11 were issued to all the districts vide letter no. WCD/ICDS/2010/3611 dated 3.05.2010. The
Directorate of WCD has also printed and supplied to the AWCs calendars which outline the
subjects and pictorial material for training of the pre-school children. Total number of PSE
kits issued to AWCs during the last financial year was 78929 which is 100 percent of the
total operational AWCs. Procurement of PSE kits have been decentralized during the
current financial year. Districts have been authorized to procure the kit at their level,
following the GOI guidelines.
c) Specific interventions on preschool education made during recent years
Rajya Shiksha Kendra, DWCD & DEVELOPMENT PARTNERS jointly organized 5 days
training on pre-school education component in 2010 for all WCD supervisors. To start with
75 Master Trainers were trained. The Master Trainers trained 2500 ICDS Supervisors in
PSE and training technique at state level as resource persons. The Supervisors in turn
conducted training of AWWs. MLTC Indore and MLTC Jabalpur were used as training
centres for Supervisors’ training. The Supervisors were also supplied training modules for
training of AWWs. In the first phase in each district 200 villages were identified where
enrolment of children in primary school was low. To develop AWCs in these villages as
model centres funds were released to procure teaching learning material.
The state, with the technical and financial support from State Education Centre (Rajya
Shiksha Kendra), trained 69,240 AWWs. With effect from November 2009 pre-school
education has been developed into Anganwadi Nursery Centers.
Along with this the department has also taken steps to develop 88 model anganwadi centers
in each district of MP. These AWC will be made child friendly based on BaLA concept.
Under the guidance of national experts curriculum for pre-school education has been
designed and provided to AWCs. The curriculum includes games, story telling, song and
drama, language, cognitive and creative skills. On last Saturday of every month Children’s
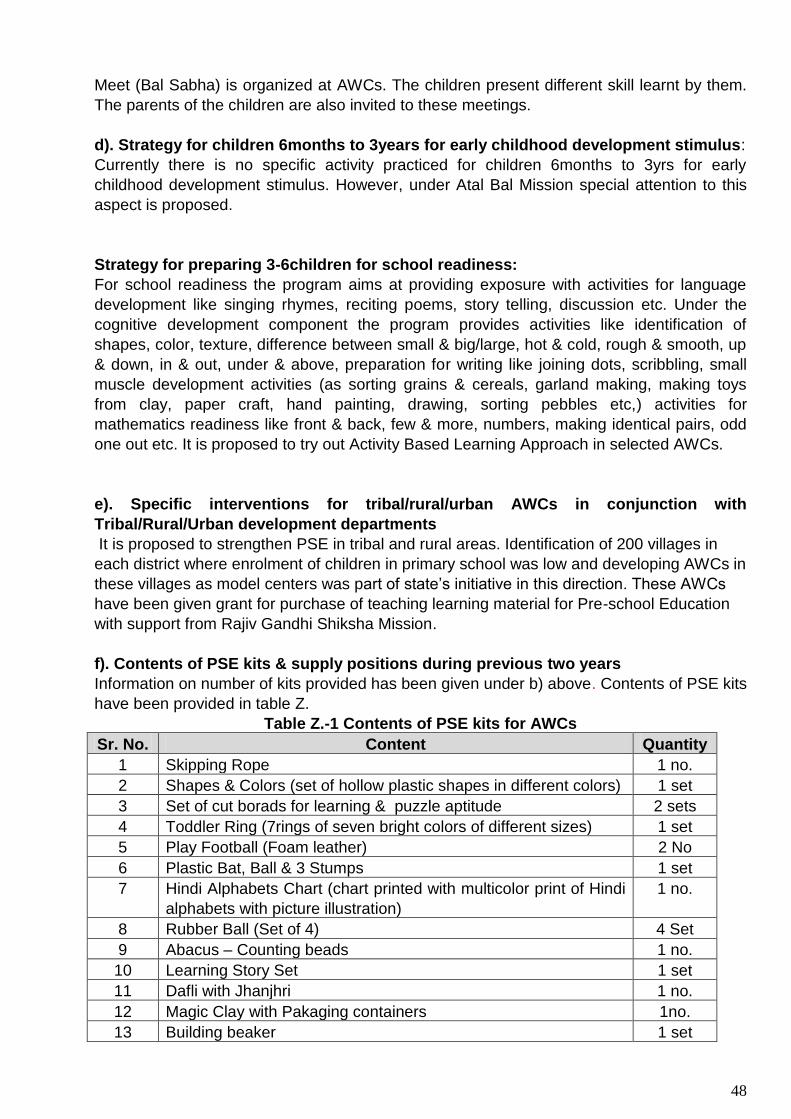
48
Meet (Bal Sabha) is organized at AWCs. The children present different skill learnt by them.
The parents of the children are also invited to these meetings.
d). Strategy for children 6months to 3years for early childhood development stimulus:
Currently there is no specific activity practiced for children 6months to 3yrs for early
childhood development stimulus. However, under Atal Bal Mission special attention to this
aspect is proposed.
Strategy for preparing 3-6children for school readiness:
For school readiness the program aims at providing exposure with activities for language
development like singing rhymes, reciting poems, story telling, discussion etc. Under the
cognitive development component the program provides activities like identification of
shapes, color, texture, difference between small & big/large, hot & cold, rough & smooth, up
& down, in & out, under & above, preparation for writing like joining dots, scribbling, small
muscle development activities (as sorting grains & cereals, garland making, making toys
from clay, paper craft, hand painting, drawing, sorting pebbles etc,) activities for
mathematics readiness like front & back, few & more, numbers, making identical pairs, odd
one out etc. It is proposed to try out Activity Based Learning Approach in selected AWCs.
e). Specific interventions for tribal/rural/urban AWCs in conjunction with
Tribal/Rural/Urban development departments
It is proposed to strengthen PSE in tribal and rural areas. Identification of 200 villages in
each district where enrolment of children in primary school was low and developing AWCs in
these villages as model centers was part of state’s initiative in this direction. These AWCs
have been given grant for purchase of teaching learning material for Pre-school Education
with support from Rajiv Gandhi Shiksha Mission.
f). Contents of PSE kits & supply positions during previous two years
Information on number of kits provided has been given under b) above. Contents of PSE kits
have been provided in table Z.
Table Z.-1 Contents of PSE kits for AWCs
Sr. No. Content Quantity
1 Skipping Rope 1 no.
2 Shapes & Colors (set of hollow plastic shapes in different colors) 1 set
3 Set of cut borads for learning & puzzle aptitude 2 sets
4 Toddler Ring (7rings of seven bright colors of different sizes) 1 set
5 Play Football (Foam leather) 2 No
6 Plastic Bat, Ball & 3 Stumps 1 set
7 Hindi Alphabets Chart (chart printed with multicolor print of Hindi
alphabets with picture illustration)
1 no.
8 Rubber Ball (Set of 4) 4 Set
9 Abacus – Counting beads 1 no.
10 Learning Story Set 1 set
11 Dafli with Jhanjhri 1 no.
12 Magic Clay with Pakaging containers 1no.
13 Building beaker 1 set
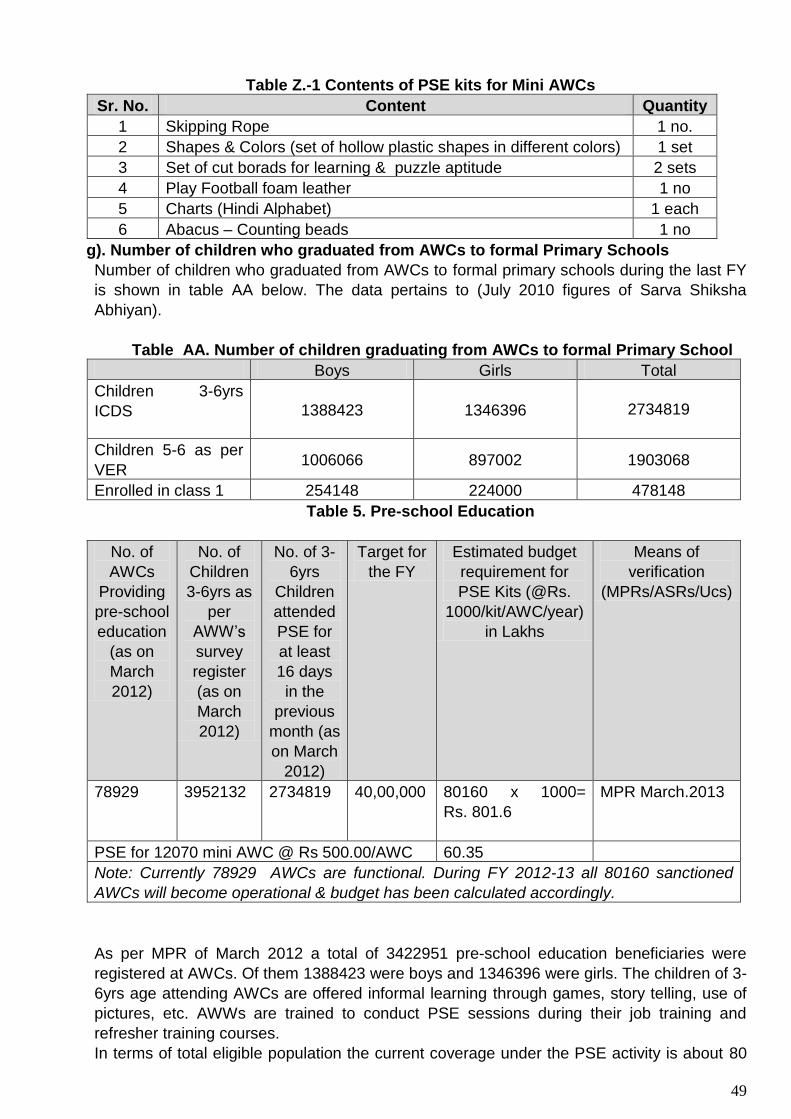
49
Table Z.-1 Contents of PSE kits for Mini AWCs
Sr. No. Content Quantity
1 Skipping Rope 1 no.
2 Shapes & Colors (set of hollow plastic shapes in different colors) 1 set
3 Set of cut borads for learning & puzzle aptitude 2 sets
4 Play Football foam leather 1 no
5 Charts (Hindi Alphabet) 1 each
6 Abacus – Counting beads 1 no
g). Number of children who graduated from AWCs to formal Primary Schools
Number of children who graduated from AWCs to formal primary schools during the last FY
is shown in table AA below. The data pertains to (July 2010 figures of Sarva Shiksha
Abhiyan).
Table AA. Number of children graduating from AWCs to formal Primary School
Boys Girls Total
Children 3-6yrs
ICDS 1388423 1346396
2734819
Children 5-6 as per
VER 1006066 897002 1903068
Enrolled in class 1 254148 224000 478148
Table 5. Pre-school Education
No. of
AWCs
Providing
pre-school
education
(as on
March
2012)
No. of
Children
3-6yrs as
per
AWW’s
survey
register
(as on
March
2012)
No. of 3-
6yrs
Children
attended
PSE for
at least
16 days
in the
previous
month (as
on March
2012)
Target for
the FY
Estimated budget
requirement for
PSE Kits (@Rs.
1000/kit/AWC/year)
in Lakhs
Means of
verification
(MPRs/ASRs/Ucs)
78929 3952132 2734819
40,00,000 80160 x 1000=
Rs. 801.6
MPR March.2013
PSE for 12070 mini AWC @ Rs 500.00/AWC 60.35
Note: Currently 78929 AWCs are functional. During FY 2012-13 all 80160 sanctioned
AWCs will become operational & budget has been calculated accordingly.
As per MPR of March 2012 a total of 3422951 pre-school education beneficiaries were
registered at AWCs. Of them 1388423 were boys and 1346396 were girls. The children of 3-
6yrs age attending AWCs are offered informal learning through games, story telling, use of
pictures, etc. AWWs are trained to conduct PSE sessions during their job training and
refresher training courses.
In terms of total eligible population the current coverage under the PSE activity is about 80

50
% ( March data). To increase enrolment of 3-6 year children to the Pre-school Education
activity is a major programmatic challenge for ICDS program.
Table AB. No. of 3-6 years children enrolled with AWCs for PSE Program
Indicators Boys Girls Total
Eligible population 2033994 1925093 3959087
Enrolled under PSE 1749397 1673554 3422951
% enrollment 86.01 86.93 86.46
PSE beneficiaries 1388423 1346396 2734819
% beneficiaries out
of enrolled children
79.37 80.45 79.90
4C3. Nutrition and health education
i. Strategy on Nutrition and Health Education Community education on nutrition issues has received high priority in MP. Every year breast-feeding week is observed to promote breast feeding. The activities are organised in collaboration with the Department of Public Health and Family Welfare, professional bodies like Indian Association of Paediatrics, Family Planning Association of India, Voluntary Health Association, BFPNI, etc. Education for breast feeding is also imparted to mothers of new-borns who come for institutional delivery. Norway India Partnership Initiative (NIPI) also promotes breast-feeding by its volunteers who are posted at the health institutions. An important initiative of the State to promote breast-feeding is appointment of trained counsellors in the hospitals for educating women delivering at health institutions under Janani Suraksha Yojana. Nutrition and health education of the mothers is carried out through Mangal Diwas events as well. These have already been described earlier in section 1 (page 20). SABLA programme which has been launched in 15 districts further strengthens this community, through adolescent girls.
ii. Status of implementation of national guidelines on Infant & Young Child Feeding Practices
National guidelines on Infant and Young Child feeding are being followed in the state. Breast-feeding is almost universal in MP; the challenge is to promote correct breast-feeding (i.e. feeding colostrums, exclusive breast feeding up to six months and introduction of semi-solids at age 6 months). The activities to promote breast feeding have been outlined in the section above. Because of the efforts made in this direction level of knowledge about early breast feeding, exclusive breast feeding, weaning at six months and breast feeding during sickness has shown an upward trend as reported by NFHS 3 and DLHS 3 data. Also refer to graph at page 24.
Existing mechanism for counselling of mothers on nutrition and health issues by AWW/Supervisor during home visit: Pregnant and lactating women are given counselling on nutrition and health issues by AWWs, Supervisors, ANMs, LHVs during home visits. Members of Matri Sahayogini Samiti have also been trained to provide counselling to mothers. NHED kits for counselling are not available but IEC material developed by DWCD and DHFW on different health and nutrition issues is used during home visits. Efforts made under NHED have paid results as can be seen by improved health behaviour of women. For example, the prevalence of breast feeding within one hour and exclusive breast feeding for six months have almost doubled from DLHS II to III; the respective figures being 43% and 21% for breast feeding within one hour and 52% and 29% for exclusive breast feeding.
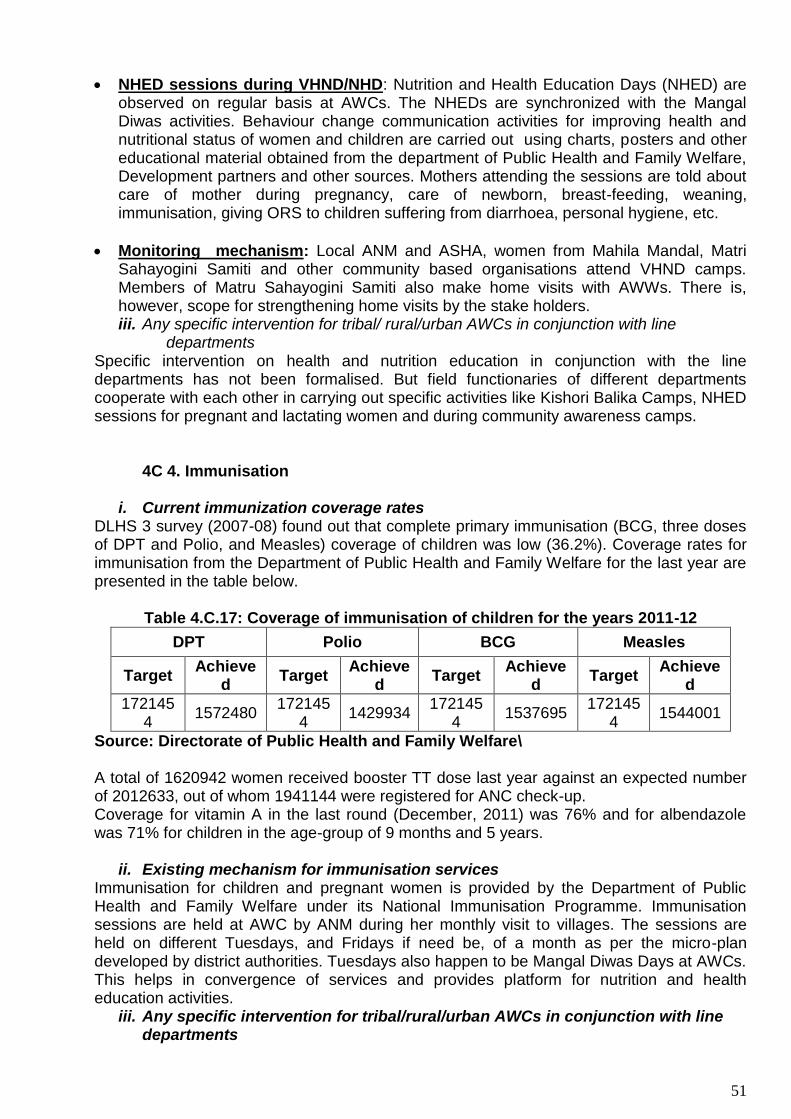
51
NHED sessions during VHND/NHD: Nutrition and Health Education Days (NHED) are observed on regular basis at AWCs. The NHEDs are synchronized with the Mangal Diwas activities. Behaviour change communication activities for improving health and nutritional status of women and children are carried out using charts, posters and other educational material obtained from the department of Public Health and Family Welfare, Development partners and other sources. Mothers attending the sessions are told about care of mother during pregnancy, care of newborn, breast-feeding, weaning, immunisation, giving ORS to children suffering from diarrhoea, personal hygiene, etc.
Monitoring mechanism: Local ANM and ASHA, women from Mahila Mandal, Matri Sahayogini Samiti and other community based organisations attend VHND camps. Members of Matru Sahayogini Samiti also make home visits with AWWs. There is, however, scope for strengthening home visits by the stake holders. iii. Any specific intervention for tribal/ rural/urban AWCs in conjunction with line
departments Specific intervention on health and nutrition education in conjunction with the line departments has not been formalised. But field functionaries of different departments cooperate with each other in carrying out specific activities like Kishori Balika Camps, NHED sessions for pregnant and lactating women and during community awareness camps.
4C 4. Immunisation
i. Current immunization coverage rates
DLHS 3 survey (2007-08) found out that complete primary immunisation (BCG, three doses of DPT and Polio, and Measles) coverage of children was low (36.2%). Coverage rates for immunisation from the Department of Public Health and Family Welfare for the last year are presented in the table below.
Table 4.C.17: Coverage of immunisation of children for the years 2011-12
DPT Polio BCG Measles
Target Achieve
d Target
Achieved
Target Achieve
d Target
Achieved
1721454
1572480 172145
4 1429934
1721454
1537695 172145
4 1544001
Source: Directorate of Public Health and Family Welfare\ A total of 1620942 women received booster TT dose last year against an expected number of 2012633, out of whom 1941144 were registered for ANC check-up. Coverage for vitamin A in the last round (December, 2011) was 76% and for albendazole was 71% for children in the age-group of 9 months and 5 years.
ii. Existing mechanism for immunisation services
Immunisation for children and pregnant women is provided by the Department of Public Health and Family Welfare under its National Immunisation Programme. Immunisation sessions are held at AWC by ANM during her monthly visit to villages. The sessions are held on different Tuesdays, and Fridays if need be, of a month as per the micro-plan developed by district authorities. Tuesdays also happen to be Mangal Diwas Days at AWCs. This helps in convergence of services and provides platform for nutrition and health education activities.
iii. Any specific intervention for tribal/rural/urban AWCs in conjunction with line departments
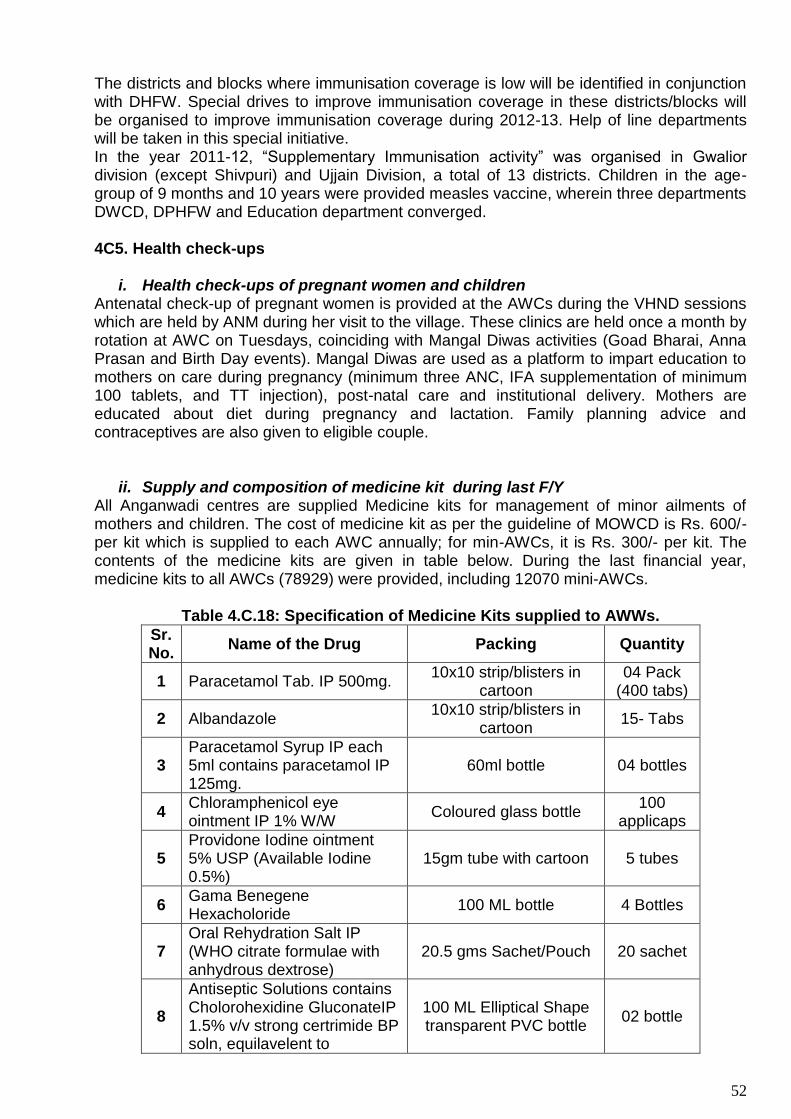
52
The districts and blocks where immunisation coverage is low will be identified in conjunction with DHFW. Special drives to improve immunisation coverage in these districts/blocks will be organised to improve immunisation coverage during 2012-13. Help of line departments will be taken in this special initiative. In the year 2011-12, “Supplementary Immunisation activity” was organised in Gwalior division (except Shivpuri) and Ujjain Division, a total of 13 districts. Children in the age-group of 9 months and 10 years were provided measles vaccine, wherein three departments DWCD, DPHFW and Education department converged. 4C5. Health check-ups
i. Health check-ups of pregnant women and children Antenatal check-up of pregnant women is provided at the AWCs during the VHND sessions which are held by ANM during her visit to the village. These clinics are held once a month by rotation at AWC on Tuesdays, coinciding with Mangal Diwas activities (Goad Bharai, Anna Prasan and Birth Day events). Mangal Diwas are used as a platform to impart education to mothers on care during pregnancy (minimum three ANC, IFA supplementation of minimum 100 tablets, and TT injection), post-natal care and institutional delivery. Mothers are educated about diet during pregnancy and lactation. Family planning advice and contraceptives are also given to eligible couple.
ii. Supply and composition of medicine kit during last F/Y All Anganwadi centres are supplied Medicine kits for management of minor ailments of mothers and children. The cost of medicine kit as per the guideline of MOWCD is Rs. 600/- per kit which is supplied to each AWC annually; for min-AWCs, it is Rs. 300/- per kit. The contents of the medicine kits are given in table below. During the last financial year, medicine kits to all AWCs (78929) were provided, including 12070 mini-AWCs.
Table 4.C.18: Specification of Medicine Kits supplied to AWWs.
Sr. No.
Name of the Drug Packing Quantity
1 Paracetamol Tab. IP 500mg. 10x10 strip/blisters in
cartoon 04 Pack
(400 tabs)
2 Albandazole 10x10 strip/blisters in
cartoon 15- Tabs
3 Paracetamol Syrup IP each 5ml contains paracetamol IP 125mg.
60ml bottle 04 bottles
4 Chloramphenicol eye ointment IP 1% W/W
Coloured glass bottle 100
applicaps
5 Providone Iodine ointment 5% USP (Available Iodine 0.5%)
15gm tube with cartoon 5 tubes
6 Gama Benegene Hexacholoride
100 ML bottle 4 Bottles
7 Oral Rehydration Salt IP (WHO citrate formulae with anhydrous dextrose)
20.5 gms Sachet/Pouch 20 sachet
8
Antiseptic Solutions contains Cholorohexidine GluconateIP 1.5% v/v strong certrimide BP soln, equilavelent to
100 ML Elliptical Shape transparent PVC bottle
02 bottle
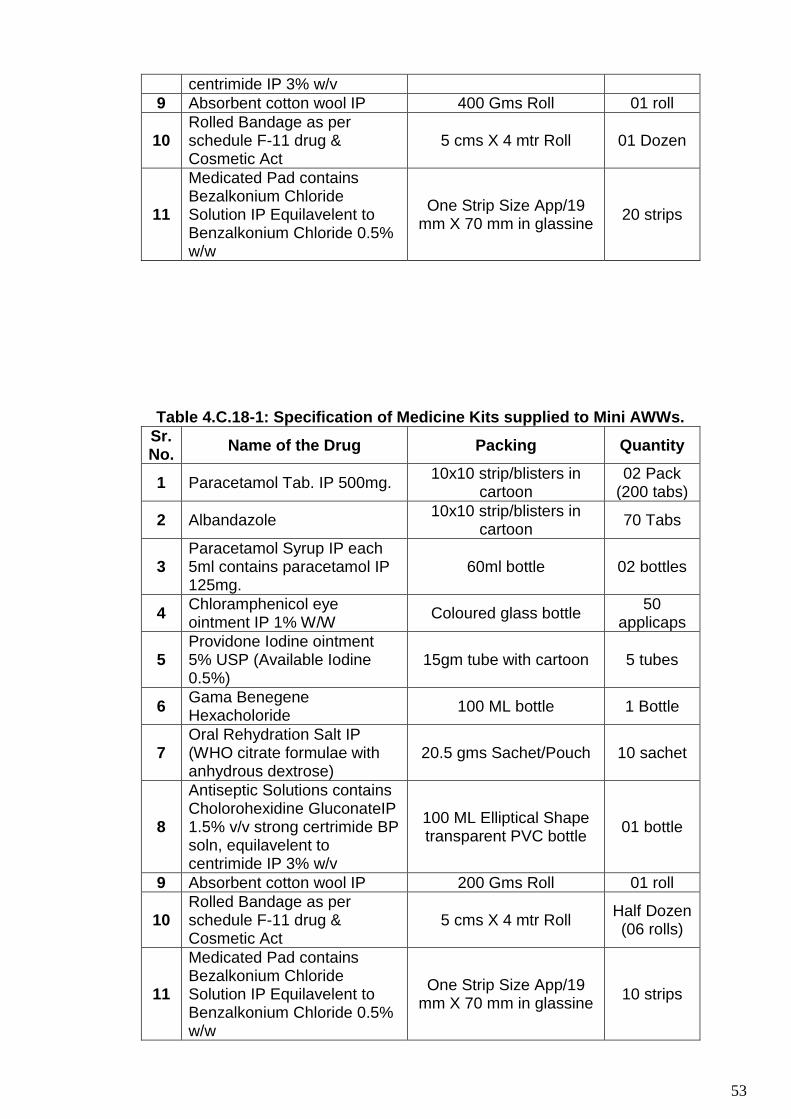
53
centrimide IP 3% w/v
9 Absorbent cotton wool IP 400 Gms Roll 01 roll
10 Rolled Bandage as per schedule F-11 drug & Cosmetic Act
5 cms X 4 mtr Roll 01 Dozen
11
Medicated Pad contains Bezalkonium Chloride Solution IP Equilavelent to Benzalkonium Chloride 0.5% w/w
One Strip Size App/19 mm X 70 mm in glassine
20 strips
Table 4.C.18-1: Specification of Medicine Kits supplied to Mini AWWs.
Sr. No.
Name of the Drug Packing Quantity
1 Paracetamol Tab. IP 500mg. 10x10 strip/blisters in
cartoon 02 Pack
(200 tabs)
2 Albandazole 10x10 strip/blisters in
cartoon 70 Tabs
3 Paracetamol Syrup IP each 5ml contains paracetamol IP 125mg.
60ml bottle 02 bottles
4 Chloramphenicol eye ointment IP 1% W/W
Coloured glass bottle 50
applicaps
5 Providone Iodine ointment 5% USP (Available Iodine 0.5%)
15gm tube with cartoon 5 tubes
6 Gama Benegene Hexacholoride
100 ML bottle 1 Bottle
7 Oral Rehydration Salt IP (WHO citrate formulae with anhydrous dextrose)
20.5 gms Sachet/Pouch 10 sachet
8
Antiseptic Solutions contains Cholorohexidine GluconateIP 1.5% v/v strong certrimide BP soln, equilavelent to centrimide IP 3% w/v
100 ML Elliptical Shape transparent PVC bottle
01 bottle
9 Absorbent cotton wool IP 200 Gms Roll 01 roll
10 Rolled Bandage as per schedule F-11 drug & Cosmetic Act
5 cms X 4 mtr Roll Half Dozen (06 rolls)
11
Medicated Pad contains Bezalkonium Chloride Solution IP Equilavelent to Benzalkonium Chloride 0.5% w/w
One Strip Size App/19 mm X 70 mm in glassine
10 strips

54
iii. Status of three antenatal coverage of pregnant women during last year ANC services are provided by ANM during the monthly visits to AWCs by rotation. The ANC checkups are generally done at the AWCs. The AWWS assist the ANM in mobilising the mothers and in conducting ANC clinic. According to data of DHFW, ANC registration in MP was 96%, while 3 ANC visits were paid to 77% pregnant women in FY 2011-12.
iv. Supply of IFA tablets to pregnant women through RCH IFA tablets, large and small, are supplied to all Sub-Health Centres by the DHFW under the RCH II program. The ANMs, in turn, supply IFA tablets to the AWCs for distribution to women and children. IFA tablets were distributed to 80% of pregnant women in the State during April 2010 to Jan 2011 (www.mp.gov.in. health bulletin). During the period under reference, all AWCs were supplied IFA tablets. There is provision for purchase of IFA tablets by DWCD, in case there is supply break down from DHFW. Control of adolescent anaemia is also a component under SABLA program.
v. Strategy to improve health check up during the FY Coordination between the departments of WCD and HFW will be further strengthened to improve health checkup of mothers and children during the financial year. Greater role of PRI to motivate the community and community monitoring of the program will be attempted. Emphasis on inter-personal communication will be given in IEC activities .
vi. Specific intervention for tribal/ rural/urban AWCs in conjunction with Tribal/ Rural/Urban development department
No specific intervention for tribal/rural and urban groups to improve health check-up in coordination with the line departments was planned during the last financial year. The possibility of improved inter-sectoral coordination between the concerned departments will be explored during the next financial year.
vii. Linkage with AYUSH : No linkage can be done with AYUSH
4C 6. Referral services
i. Existing mechanism for referral services AWWs refer pregnant women and children requiring medical advice/care to local ANM during her monthly village visit or to Sub Health Centre. But women/children who need special advice are referred to Primary Health Centre/Community Health Centre and District Hospital in the area. As per MPR data March 2012 21599 pregnant and lactating women were referred to higher health facilities that includes PHC/CHC/DH ( out of 21599, 18673 were referred for normal delivery, 1564 were referred due to complication and 1362 were reffered for other services from AWCs). During the same reference period 54036 children were referred by AWWs to various helath facilities, out of which 27452 children were referred for Pheumonia, Dirrehea and Fever, 17221 severely underweight children were also referred.
ii. Constraints in effective referral There is no effective system of referral of clients between AWCs and the health facilities. This is a great constraint in the referral system. Absence of a referral card in the Anganwadi Centres is also a constraint.
iii. Strategy to improve this component during the F/Y
It is proposed to develop and supply referral cards to the AWCs for referral of clients to higher centres. Efforts will also be made to discuss the problem with the local ANM/Block

55
MO to evolve a robust referral system so that the clients referred are received at the referred centre promptly and given appropriate services. Allocation for printing of referral cards @ Rs. 10 per AWW = Rs 10 x 80,000 = 8, 00,000 it is proposed to include this under ABM.
4D Observance of Village Health and Nutrition Day
a) Mechanism for observance of monthly Village Health and Nutrition Day
MOHFW guidelines describes the importance of conducting monthly Village Health Nutrition
Days, which defines the required relevant procedures and logistics; the role of each cadre of
health worker including supervisors; and the various activities that should be conducted on
the day. Under NRHM the Village Health and Nutrition Day is planned to provide
comprehensive Maternal and Child health and nutrition services, ensure early registration,
identification and referral of high risk children and pregnant women.
The department of WCD actively participates in Village Health and Nutrition Days organized
by the department of HFW. VHNDs held once a month in the villages covered under sub
health centre area by rotation. Women and children, particularly pregnant and lactating
women, in the village are mobilized for attending the meeting. Village Health and Sanitation
Committee members, members of Matri Sahayogini Samiti, Mahila Mandals, SHG, and
other community based organizations are also contacted to extend support for VHNDs.
a) Summary of activities that are taken up
during the Village health and Nutrition
day
VHND activities are jointly carried out by health
staff (ANM/LHV), AWWs and ASHA. AWWs play
important role in community mobilization besides
helping in organizing the activities. VHNDs are
generally held at sub health centre or AWCs.
Pregnant women are registered for antenatal care,
and health check up of women is done. Two doses
of tetanus toxoid vaccine are administered and IFA
tablets (total 100 tablets) are given. Children who attend VHND are given health check up.
Primary immunization (BCG, 3 doses of DPT and Polio each, and Measles) is administered
to children and Vitamin A supplement is also given. Mother and Child card is used to record
the services provided to the beneficiaries. IEC activities on nutrition of pregnant/ lactating
women and children, importance of immunization, family welfare methods, and personal
hygiene form important aspect of VHND activities
The different activities are organized at VHND like Health and Nutrition Education,
immunization,
PNC, Exhibitions etc. The MIS reveals that AWW imparted Health and Nutrition Education in
98 % sessions and organized exhibitions in 89% of session out of total they attended.
b) Support received from community/ PRIs for observance of NHD
Support is sought from community/ PRIs for observance of Nutrition and Health days. The
support is extended by way of participation in the event, community mobilization, publicity,
use of PRI resources including Panchayat Bhavan) to organize the events. PRI members
were present in 91% of VHNDs organized in the state.
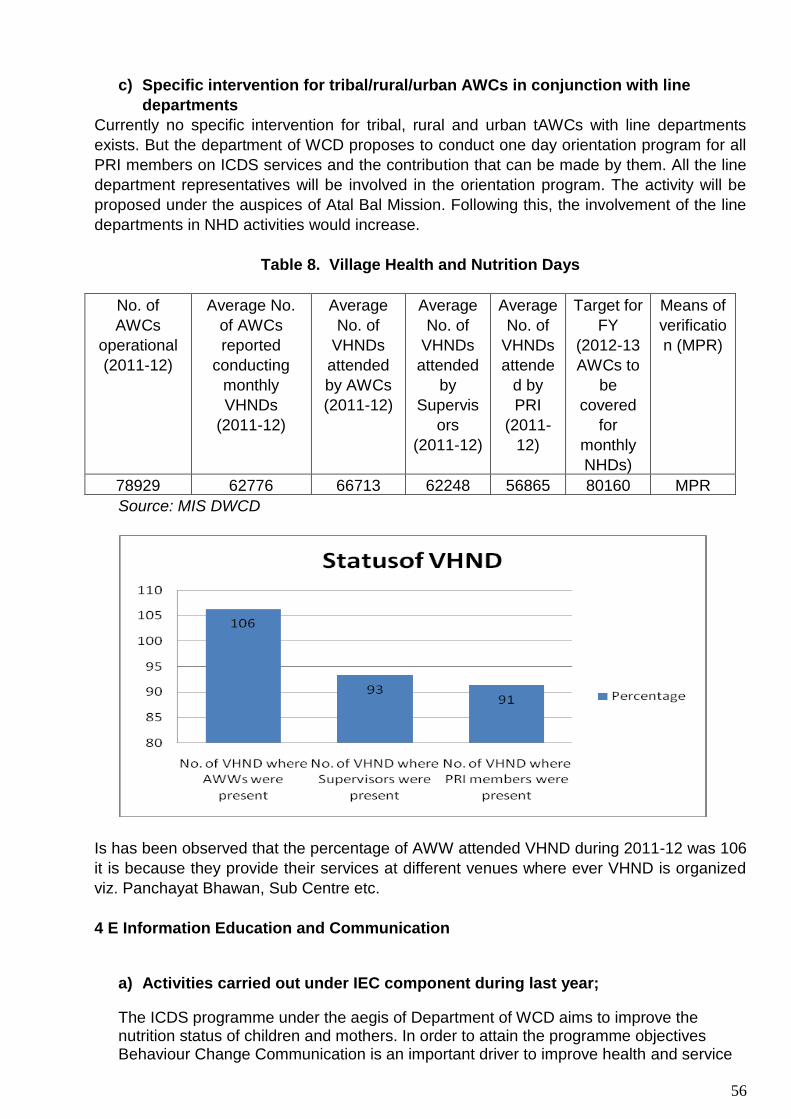
56
c) Specific intervention for tribal/rural/urban AWCs in conjunction with line
departments
Currently no specific intervention for tribal, rural and urban tAWCs with line departments
exists. But the department of WCD proposes to conduct one day orientation program for all
PRI members on ICDS services and the contribution that can be made by them. All the line
department representatives will be involved in the orientation program. The activity will be
proposed under the auspices of Atal Bal Mission. Following this, the involvement of the line
departments in NHD activities would increase.
Table 8. Village Health and Nutrition Days
No. of
AWCs
operational
(2011-12)
Average No.
of AWCs
reported
conducting
monthly
VHNDs
(2011-12)
Average
No. of
VHNDs
attended
by AWCs
(2011-12)
Average
No. of
VHNDs
attended
by
Supervis
ors
(2011-12)
Average
No. of
VHNDs
attende
d by
PRI
(2011-
12)
Target for
FY
(2012-13
AWCs to
be
covered
for
monthly
NHDs)
Means of
verificatio
n (MPR)
78929 62776 66713 62248 56865 80160 MPR
Source: MIS DWCD
Is has been observed that the percentage of AWW attended VHND during 2011-12 was 106
it is because they provide their services at different venues where ever VHND is organized
viz. Panchayat Bhawan, Sub Centre etc.
4 E Information Education and Communication
a) Activities carried out under IEC component during last year;
The ICDS programme under the aegis of Department of WCD aims to improve the nutrition status of children and mothers. In order to attain the programme objectives Behaviour Change Communication is an important driver to improve health and service

57
seeking behaviour alongside the service delivery. The key focus areas of the ICDS programme are-
Infant and Young Child Feeding (IYCF) practices
Immunization
Growth monitoring
Pre-school education
The department uses a mix of traditional and modern media to reach out to the target audiences. There is a lot of focus on inter personal communication activities through AWWs. In order to create mass awareness on schemes, issues and to connect with the AWWs a number of publications are published. Last year (on October 6, 2011) Chief Minister of Madhya Pradesh launched “Beti Bachao Abhiyan”, for which the DWCD is the nodal department.
A summary of the IEC activities carried out are as follows:
Publications Radio Observation of special days
Inter Personal Communication
Community platforms
Other channels
AnaganwadiSamacharika A monthly news letter to disseminate information to AWWs about new guidelines and activities
Radio has been used effectively last year to generate awareness on ICDS program and specific issues.
Focused dissemination of messages around specific themes through observance of special days
AWWs are the primary channel of IPC ensuring maximum reach to the beneficiaries
Engage Community Based Organizations to conduct community mobilization (Mahila Mandal, Matri Sahayogini Samiti, Self Help Group)
To enhance reach and impact a mix of mid media channels have also been used last year
Calendar Depict success stories on women empowerment and prevention of female foeticide
Channels Use of 12 centers of All India Radio and Vividh Bharti program in MP
Women focused International Women’s Day-March 8 Safe Motherhood Day- April 11 World Breastfeeding week-1-7August Adolescent focused National Girl’s Day-January 24
Area of concern Lack of job aids for effective IPC and counseling sessions
-Nutrition Health and Education Day -Village Health and Nutrition Day (with NRHM)
-Exhibitions -Street shows -Cinema slides -Rallies -Workshops -Seminars -Painting competition -Mangal Diwas

58
Adolescent Girls week- July 25-31 Stop Child Marriage campaign-throughout the week with focus around Akshay Tritya Others ICDS day- October 2 Children’s day- November 14 Nutrition week September 1-7
Badhte Kadam Behtar Kal (marching towards better tomorrow)
Programmes Stories Radio drama Songs Talks and Discussions Jingles Radio spots Phone in facility
Information booklet on Ladli Laxmi and IGMSY
Key focus areas Breast feeding Immunization Complementary feeding
Folders, booklets, pamphlets, posters Increase awareness on nutrition, health, immunization, breast feeding
b) List of IEC materials that have been developed
IEC material developed by the department has been outlined in the previous section.
Posters have been supplied to AWCs. During last financial year Public Address
systems were procured and supplied to all 453 Projects and 7 Divisional Bal
Bhavans.
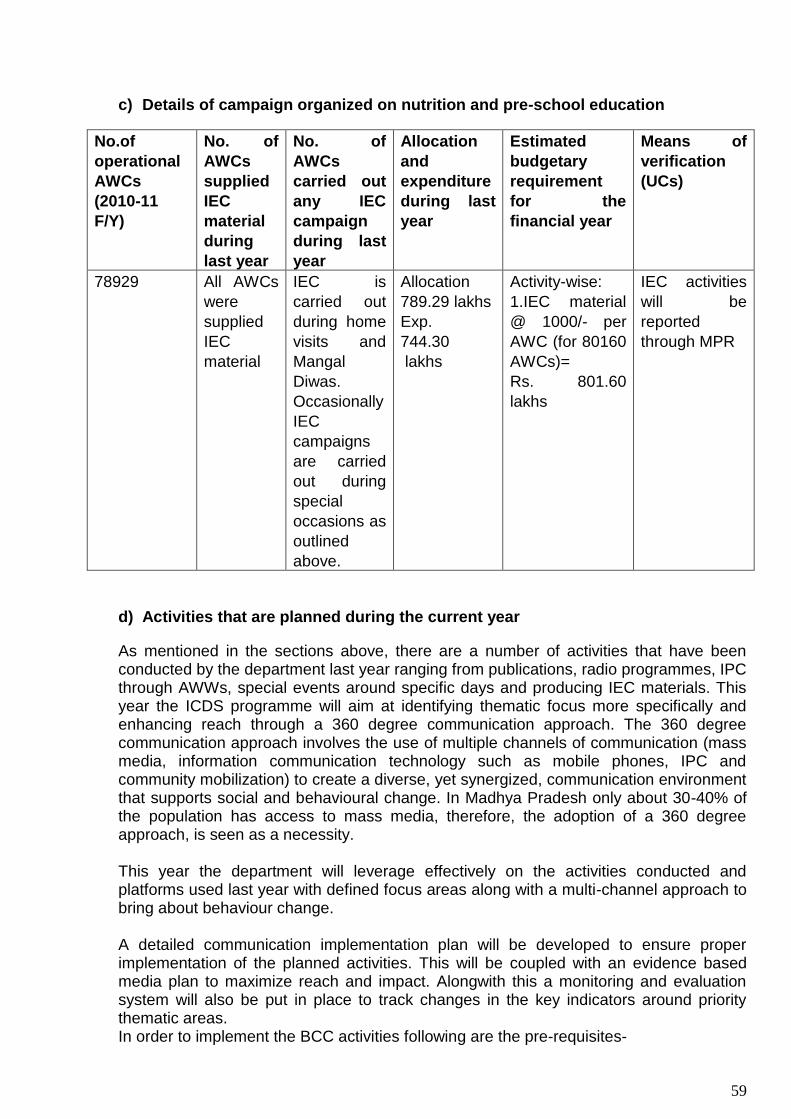
59
c) Details of campaign organized on nutrition and pre-school education
No.of
operational
AWCs
(2010-11
F/Y)
No. of
AWCs
supplied
IEC
material
during
last year
No. of
AWCs
carried out
any IEC
campaign
during last
year
Allocation
and
expenditure
during last
year
Estimated
budgetary
requirement
for the
financial year
Means of
verification
(UCs)
78929 All AWCs
were
supplied
IEC
material
IEC is
carried out
during home
visits and
Mangal
Diwas.
Occasionally
IEC
campaigns
are carried
out during
special
occasions as
outlined
above.
Allocation
789.29 lakhs
Exp.
744.30
lakhs
Activity-wise:
1.IEC material
@ 1000/- per
AWC (for 80160
AWCs)=
Rs. 801.60
lakhs
IEC activities
will be
reported
through MPR
d) Activities that are planned during the current year
As mentioned in the sections above, there are a number of activities that have been conducted by the department last year ranging from publications, radio programmes, IPC through AWWs, special events around specific days and producing IEC materials. This year the ICDS programme will aim at identifying thematic focus more specifically and enhancing reach through a 360 degree communication approach. The 360 degree communication approach involves the use of multiple channels of communication (mass media, information communication technology such as mobile phones, IPC and community mobilization) to create a diverse, yet synergized, communication environment that supports social and behavioural change. In Madhya Pradesh only about 30-40% of the population has access to mass media, therefore, the adoption of a 360 degree approach, is seen as a necessity. This year the department will leverage effectively on the activities conducted and platforms used last year with defined focus areas along with a multi-channel approach to bring about behaviour change. A detailed communication implementation plan will be developed to ensure proper implementation of the planned activities. This will be coupled with an evidence based media plan to maximize reach and impact. Alongwith this a monitoring and evaluation system will also be put in place to track changes in the key indicators around priority thematic areas. In order to implement the BCC activities following are the pre-requisites-

60
Capacity strengthening of IEC officials across various levels (Technical
Assistance to be provided by BBC-World Service Trust through DFID support)
IPC skill strengthening of Aanganwadi Workers (Technical Assistance to be
provided by BBC-World Service Trust through DFID support) Details are provided
in the capacity building section
Creating communication outputs (Technical Assistance to be provided by BBC-
World Service Trust through DFID support)
4F. Monitoring and evaluation
a) Existing monitoring and supervision mechanism at different level
The main tool of monitoring of ICDS program in the State is monthly progress report data
received from the field starting at AWCs and reaching the state monitoring cell. Although
huge amount of data is collected through this system, currently it is not put to effective use
for management purposes. It is realized that the data is neither complete (because of
different number of AWCs reporting in a given month), nor accurate. Accuracy of data is not
ensured because the AWWs are not fully trained (particularly those whose literacy levels are
low) to maintain records and fill up the MPR forms. They also are not aware of the
importance of the MPR for program management. The supervisors also do not check the
data for its accuracy and completeness. At the state level the team handling the data is not
trained for its collation, analysis and interpretation for management purposes. The
department has recently put in place a web enabled system for data collection from the
periphery to the state headquarter and, once fully operational, is expected to improve
monitoring of the ICDS program activities more effectively. Training of the staff will be
undertaken in use of new web enabled monitoring system at all levels.
The state proposes to introduce and establish a system of data verification through
independent third party audit. This will be done on a regular basis so that all the 50 districts
and 313 blocks are covered in a year. The Department with the support of MPTAST has
recently completed a data verification study on routine MIS. The findings and
recommendations suggested by the study would be adopted for improving the quality of
data.
In addition, concurrent monitoring system would be implemented to evaluate and assess the
performance of various activities at regular intervals. This concurrent monitoring system will
provide ifnromation on key parameters of the program and will serve as guide for taking mid-
course corrections to improve the programme activities for achieving the desired outcomes.
b) Constraints in monitoring and supervision (human resources, capacity building
and mobility of functionaries)
Supervision of the program is undertaken by supervisory level functionaries/ officers at
different levels i.e. sector level, project level and district level. A unique, initiative was taken
last year by the Hon. Minister of WCD and the Commissioner / Director of the department by
personally visiting the AWCs and checking the program implementation including SNP.
.However, the need for a strong and formal system of supervision and monitoring cannot be
over-emphasized. Capacity building of staff for monitoring has already been highlighted in
the above paragraph. Lack of mobility of supervisory staff at different levels is also an
important constraint
61
d) Assessment/ evaluation studies undertaken
No assessment or evaluation study has been undertaken by the department in the last two
years. But the study by National Institute of Nutrition (ICMR), Hyderabad which has been
commissioned by the state to assess the level of malnutrition among children and the
underlying factors will provide district-wise baseline information and epidemiological
determinants of malnutrition. The data will be used for district-level planning of activities to
control malnutrition
e) State has rolled out revised MIS as prepared by MWCD
The State has not yet rolled out revised MIS system prepared by MWCD. But it will be
incorporated in the web enable monitoring system early next financial year.
f) State’s strategy to improve the existing MIS
State proposes to introduce revised MIS developed by MWCD on the web enabled platform
to improve MIS for ICDS program activities. Along with the introduction of the new MIS
system, training of staff at different level will also be undertaken to develop capacity of staff
to use the new information system.
In addition, it is proposed that a nutrition surveillance system will be designed and
developed in the state to identify high risk pockets and also to understand the causal factors
along with social-cultural attributes associated with prevalence of malnutrition in the state.
The nutrition surveillance system will be interfaced with the existing web-enabled MIS so
that data synchronization can take place in a systematic manner.
The nutrition surveillance system will provide regular information at micro and macro level
on issues of malnutrition and its level. The information would be helpful in identifying the
SAM children and would be utilized in tracking malnourished children at micro level.
This will be further supplemented by innovative use of mobile phone technology for
improving the MIS system and tracking of SAM children. The use of mobile phone
technology will also be used for supportive supervision and improving feedback
mechanisms at field level. The state propose to pilot such innovations using ICT tools (such
as mobile phone/PDA technology) for improving the MIS system as well as in better
management of SAM children through real time data analysis and tracking of children and
other beneficiaries.
g) Community monitoring mechanism
DEVELOPMENT PARTNERS is running a community monitoring system in one of the
districts (Guna) of the state. Based on the experiences gained, community monitoring
system will be gradually scaled up in other districts as well.
h) Structured feedback mechanism
Although some feed back is provided to the functionaries at the ground and middle level by
the supervisory staff there is as yet no structured feedback system in place. Supervisors do
provide feedback to the AWWs during their supervisory visits. A structured feed back format
and system will be incorporated in the training of staff at all levels which is being proposed
as part of introduction of new MIS of MWCD and web enabled reporting system.

62
Table 10. Monitoring and Evaluation
No. of
operational
AWCs as
in March
2012
No of
AWCs
having
revised
records
and
registers
No. of
blocks
using IT
for MIS
No. of
review
meetings
held at the
state level
during
past year
Allocation &
Expenditure
during last
year
Estimated
budgetary
requirement
for FY
(Rs. 500
per AWC
Means of
verification
78929 Currently
using old
records
and
registers
All 453
Blocks are
using IT
for MIS
Review
meetings
held as
part of
piloting
web-
enabled
reporting
system
Allocation
200.00
lakhs
--------------
Exp.
173.42
lakhs
80160
AWCx Rs.
500/ AWC
=400.8
lakhs
MPR
4G Training and capacity building
a) State Training Action Plan
State Training Action Plan is prepared by the State annually and submitted to the MOHFW.
The training cycle of the workers is fixed. The annual training load is calculated on the basis
of new recruits requiring training (induction training) and the number of workers who need
refresher and job training during the year under reference. Training backlog of the workers is
calculated on the basis of number of staff undergone training during the previous year.
Induction training of new AWWs sanctioned by MWCD is currently under progress.
Training of AWWs and supervisor is carried out by AWTCs and MLTCs. Training of senior
level staff is undertaken by NIPCCD for which programs are designed and communicated to
the State. As yet, there is no computerized record of workers undergone training and
requiring training. But this will be achieved by developing a suitable software and linking it to
the web of ICDS program.
b) Training needs assessment ICDS functionaries
No formal TNA has been carried out by the state. But training needs assessment is
informally assessed by discussion with the supervisory staff and communicated to the
higher level. Additionally, results of evaluation of ICDS program which has been conducted
under ODISHA project is taken into account while conducting training of workers by AWTC
and MLTC.
c) Available training resources in the state (AWTCs, MLTC and SRCs)
There are 10 AWTCs run by DWCD while another 15 are run by NGOs. During the financial
year 2012-13 a new AWTC has been sanctioned by GoI at Rewa. The AWTCs run by the
NGOs are financed by the government. The two MLTCs in the State are run by the
government. The list of AWTC and MLTC is given in annexure 3. The State Resource
Centre is located at Bhopal.

63
d) Detailed training calendar
Detailed training calendar for all the training institutions is prepared annually. A copy of the
training calendar is placed at annexure 5. The state training calendar is based on the
training calendars submitted by different training institutions.
e) Monitoring and supervision mechanism
The training activities are monitored through the information submitted by the training
institution after completion of each training conducted by them. Information is also collected
from the training institutions as and when required.
f) Review of the performance during the last two years as per QPR
Review of the capacity of the training centers has not been undertaken during the current
financial year. But performance review is carried out during annual planning meeting of the
Principals of the AWTCs and MLTCs. The last meeting of the Principals of training centers
was held on 19th March 2012 where training activities were reviewed and the Annual
Training Plan was discussed and finalized. . Information from the centers is also collected
periodically as per the need.
g) Proposal for other training activity
Training programs have been proposed under different program heads, besides the regular
training activities conducted by AWTCs and MLTC.
State has developed web based MIS system and proposes Rs 1753.95 lacs for training all
the functionaries ( AWW, Supervisor, CDPOs’ DPOs, DWCDPOs’, DDs, etc) on online
MPR.
For the year 2012-13 State has proposed two study tour one each at Maharashtra
and Andhra Pradesh which will amount to Rs. 10.00 Lacs
h) Financial requirements
(details on Annexure5)
i) Induction training, Job training and refresher training by AWTC/MLTC
DWCD vide its letter No. WCD/583/Trg/2012 dated 25 April 2012 has submitted a proposal
to MWCD, GOI for annual training activity for the F/Y 2012-13. (Details are placed at
annexure 5). A budget of Rs. 947.54 lakhs has been proposed by the state for carrying out
induction training, job training, refresher training and establishing new Aganawdi Training
Centre in Rewa, MP. during the financial year 2012-13. The state also prosposes to train
12070 mini AWH which will cost Rs. 162.81 Lacs
4 H. Convergence with line departments
a) Existing mechanism for convergence and coordination with line departments
Core committee for Annual PIP for ICDS has been constituted. A Steering Committee under
the chairmanship of the Principal Secretary, DWCD has also been constituted. The Core
Committee and Steering Committee will not only provide guidelines for preparation of
Annual PIP but would review its progress and of the ICDS annual program.
Several activities of the Department of WCD and HFW e. g holding of VHND, NHD,
antenatal, immunization sessions, Mangal Diwas at the village level are held jointly by the

64
functionaries of the two departments. Sanjha Chulha program is an example of coordination
between departments of WCD, Education and Panchayat & Rural Development. Training of
AWWs in PSE with financial and technical support of District Education Centre is yet
another example of the interdepartmental coordination. Construction of AWCs with BRGF
funds of department of Panchayat and Rural Development has been similarly undertaken as
joint effort between the two departments to promote health and nutritional status of women
and children.
Consultations are also held between different line departments, particularly Public Health
and Family Welfare, for implementation of ICDS activities. Area and activities of
convergence between the WCD and HFW departments have been detailed under section on
situation analysis (page 6) of this document. The inter-department convergence will be
further strengthened with the launch of Atal Bal Mission which will serve as the umbrella
organization for reviewing and supporting activities of the two departments for the purpose
of promotion of health and nutrition in their various dimensions. The new SABLA program
creates platform for interdepartmental coordination and convergence for improving health
and nutrition of adolescent girls.
a) Status of joint planning with health at district, block and village level
The Department of WCD has been participating in the preparation of Annual Plan of Action
for National Rural Health Mission at State and district levels. Similarly, for the preparation of
Annual PIP of the Department of WCD consultations were held with the department of
health and other line departments at village, block and district level for decentralized
planning.
b) Joint visits /review with health and other departments
Joint visits, as per program requirement are made by the officers at the district and block
level to the AWCs in connection with program activities and occasionally for supervisory
purpose. The number of joint visits undertaken by the middle level and grass root
functionaries of the DWCD and DHFW during the last year is shown below.
Table 11. Convergence
No. of blocks that
have developed
micro plans for
VHNDs with
health
No. of districts/blocks
having integrated ICDS
plans with
NRHM/TSC/NRDWP/SSA
plans
Average No. of
AWCs reported
conducting
monthly VHND
with participation
of ANMs during
previous year
Means of
verification
(Review reports/
Field visit reports)
All Done All 78929 AWCs
conducted monthly
VHND meetings
with ANMs
MPR (March 2013)
No. of sector
meetings attended
by health staff
No. of blocks that have
organized convergence
meeting of ICDS, health,
PRI and other line
departments.
No. of districts that
have organized
convergence
meeting of ICDS,
health, PRI and
MPR (March 2013)
65
other line
departments
13564 sector
meetings were
attended by health
staff
Information not available Information not
available
MPR (March 2013)
Budget: An amount of Rs. 50 lakhs (Rs. 1 lakh per district) has been proposed for
convergence meetings and workshops for all line departments.
4I Community participation and involvement of PRIs
a) Existing mechanism for community participation
The role of PRI is very important in the implementation of ICDS program. PRIs are involved
in a number of ways to support ICDS program activities. For example, AWWs and AWHs
are selected by CDPOs on the recommendations of Gram Sabha. Selection of the site for
construction of AWC building is also done by Gram Sabha. In fact, Gram Sabha provides
land to the department of WCD for construction of the AWC building. Involvement of PRI,
however, depends to a large extent on the rapport between the AWW/ Supervisor of the
area and the PRI members and, therefore, varies from village to village. The support of PRI
may range very widely. In two districts viz. Damoh and Sidhi, Janpad Panchayat (Block
Panchayat) are running ICDS projects. This is an example of PRI owning the program.
Similarly, two NGOs are managing ICDS projects.
The PRIs extend support to AWW for mobilization of community support, motivating mothers
to attend health check up, immunization sessions, conducting Mangal Diwas, observing
special days e,g. Breast Feeding Day, etc. Village Health and Sanitation Committees have
been formed in all the villages of the state. These committees are part of Village Panchayat
and are responsible for planning and implementation of health and nutrition related
activities. The scope for PRI involvement in a larger and intensive way so that the program
is owned by the peoples’ institutions is as yet limited. To increase it, the department of WCD
proposes to conduct one day orientation on ICDS for Sarpach, and Mahila members of the
Panchayat and members of VHSC.
b) Percent of AWCs participated in at least one Gram Sabha meeting during last year
Gram Sabha meetings are supposed to be held monthly. But very few Gram Sabhas meet
on monthly basis. The Department of Panchayat and Rural Development mandates that
Gram Sabhas meet at least four times a year on Republic day (26 Jan), Independence Day
(15 Aug.), 2nd October (Gandhi Jayanti) and 14 April (Baba Saheb Ambedkar Jayanti). All
the adult members of the village are members of Gram Sabha. AWW of the village, being a
resident of the village, is a member of Gram Sabha and participates in the meetings as and
when the meetings are held.
c) Percent of AWCs received support fom Panchayat/ CBO (SHGs, etc)
All AWCs receive support from PRI in different form as discussed under a) above.
c) Percent of monthly Gram sabha meetings attended by AWWs
Department and Panchayat and Rural Development mandate that AWWs attend meetings
of Village Health and Sanitation Committee. This committee is one of the several

66
committees of Village Panchayat and looks after health and nutritional related activities in
the village; Data on percent of Gram Sabha meetings attended by AWWs is not available.
d) Percent of monthly Panchayat Samiti meetings attended by ICDS staff
This information is currently not available.
e) Number of districts where Zila Parishads have reviewed ICDS program
Swasthya and Mahila Bal Vikas Samiti is a special committee of Zila Parishad. It meets
bimonthly and reviews ICDS program implementation in the district.
Budget: An amount of Rs. 665.0 lakhs has been proposed for orientation of PRI
members in ICDS program ( Key initiatives, page 68)
4 J Financial management and fund flow mechanism
a) Fund flow mechanism from State to Districts/ Block
Funds are transferred from the state to the district for program implementation. The
allocation is given as per the norms of the GOI and is demand base. Funds for honoraria of
AWWs and AWH and salary of staff are transferred to the project directly. Funds for SNP
are, on the other hand, transferred to District Pancahat. The district Panchayat, in turn
makes allocation to the Janpad Panchayat for Sanjha Chulha. (for supply of hot cooked
meal through SHGs which are contracted for the purpose). State government has issued
detailed guideline about the contents of the meal, its nutritional value and cost. The SNP
program is supervised by the department functionaries for food quality and regularity.
The POL, contingency funds and rental of AWC building (if they are housed in rented
accommodation) are also passed on to the CDPO as per the government of India norms.
PSE kit budget has been decentralized as recommended by GOI and given to the districts.
The Districts are now authorized to purchase PSE kits as per the standard contents
recommended by GOI.
b) Steps taken to ensure timely payment of honoraria of AWWs/ AWHs
The budget for payment of honoraria has been transferred to the Block level (CDPO office,
the lowest office which has accounts assistant to manage budget and accounts). CDPO is
the Drawing and Disbursing Officer at Block level for ICDS activities.There is, therefore, no
delay in payment of honoraria to AWWs and AWHs. Similarly the SNP funds have been
given to Janpad Panchayat (Block Panchayat) for smooth functioning of nutrition
supplement program.
c) State’s plan for establishing Society structure under ICDS set up
Society structure has been set up under Atal Bal Mission. Currently the society has been set
up at state level. But district level society structure is envisaged. Once the Society at the
district level is established under Atal Bal Mission the government may consider bringing the
functioning of ICDS under Atal Bal Mission Society frame work.
d) Detailed minor head-wise break-ups of allocation for different program activities
Head-wise break up of allocation is detailed in table 13.
e) Statement of expenditure (SOE) of previous year
Statement of Annaul expenditure of previous year (2-11-12) is enclosed at annexure 8.

67
4 K New Initiatives to Strengthen ICDS Program during 2012-13
Over the last more than four decades, ICDS program in MP has expanded considerably,
both in content of services and geographical and population coverage. The progress of the
program to achieve its objective of improvement of nutritional and health status of the
children under five has been successful to a large extent.. Yet a lot of ground remains to be
covered as nearly half of the children in the state are underweight.
In the year 2010 the State launched the Atal Bal Mission with the explicit objective of
lowering of the mortality rate among children under five and reduction of prevalence of
malnutrition, particularly Sever Acute Malnutrition (SAM). The Mission document outlines the
strategies and activities to achieve these goals.
The DWCD has reviewed the performance of the program while documenting Annual PIP,
2012-13. The document has followed the guidelines provided by GOI while preparing the
PIP. Yet the Department (WCD) feels that additional thrust is required to address some
state specific problems and to strengthen program activities. The strategy and planned
activities to strengthen the program activities have been outlined in the following pages.
1. Orientation for Community Participation in ICDS program
Rationale:
Programs like ICDS, which has people as its target, cannot succeed without their informed
participation. Involvement of community, PRIs, CBOs and village level opinion leaders, in
the activities of ICDS and ultimately its ownership of the program is thus essential for its
success. At present, community sees, by and large, ICDS as a government program. This
has to be changed to people accepting that ICDS is their own program for the benefit of their
own children.
Activity proposed to improve community participation
As a first step the community needs to be informed about the activities of ICDS program
(and health) and its importance for the health and nutritional wellbeing of children, and
pregnant and lactating women and adolescent girls. The aim of the present initiative is to
create awareness about the program and their involvement in micro planning of its activities
and community monitoring. It is proposed to organize one day orientation program on ICDS
for community leader, PRI, VHSC members, etc. In each of about 55,000 villages in the
state five to six persons will be oriented on ICDS program.
Outcome-
Awareness of community leaders about ICDS and through them the community increased.
Indicator
No. of villages covered under orientation program and in each village number of persons
oriented.
Timeline-
II, III and IV quarter of 2012-13
68
Budget:
i). Training of PRI, CBOs, VHSC members etc- 55,000 villages x 6= 3,30,000 @ Rs. 150,
per participant (travel, food, stationery, payment to trainers, etc) = 495.0 lakhs
ii) Resource material and information booklet @ Rs 50 per participant & trainer i.e.3, 40,000
x 50 = 170 lakh
Total i) and ii) = Rs.665 lakhs
1. Appointment of additional AWWs in selected AWCs
Rationale:
There are about 11,000 AWWs in the state who are illiterate (4556) or have less than V
standard educational status (6394). It is unrealistic to expect that these educationally
handicapped women will be able to undertake growth monitoring, maintain records and
registers, submit MPR data or carry on PSE activities.
Activity
It is proposed to appoint additional AWWs in these AWCs and/ or those where the problem
is acute because of other reasons. The department of HFW, for example, has appointed
additional ANMs under its NRHM program to strengthen the sub health centres where there
is a need to do so. The new AWWs will be given honorarium permissible to AWWs of Mini
AWC (i.e. Rs. 750/- per month) and will help existing AWWs in performing their duties more
effectively. The CDPOs will be asked to appoint the additional AWWs on the
recommendations of Gram Sabha.
Outcome
AWCs strengthened by appointment of additional AWWs in selected AWCs.
Indicator
No. of additional AWWs appointed, trained and posted at identified AWCs
Time line
II, II, IV quarters
Budget:
i) Induction training of 11,000 AWWs at AWTC (20 trainees per batch i.e. total 550 batches.
Training cost per batch @ Rs.27,000 per batch as per GOI norm)
Total training cost = 27,000 x 550 batches = Rs. 148.5 lakhs
ii) Honoraria to additional AWW @ Rs. 750 p.m. / AWW for six months during 2012-13 =
Rs 495 lakhs.
Total of i) and ii) = Rs. 643.50 lakhs
2. Training of AWWs in Inter-personal communication
Rationale:
Conventional IEC approach i.e. communication through print or electronic media are not
very effective in changing the behavior of mothers about breast feeding, supplementary
feeding, health seeking behaviour for immunization and in case of illnesses of the children,
additional diet during pregnancy and lactation, iron supplementation etc. These issues are
69
related to their personal knowledge, attitudes and practices. Inter-personal communication is
best suited to bring about behaviour change among women and influencers. BBC-World
Service Trust through DFID support will be providing Technical Assistance to DWCD for
designing the IPC training component along with Job aid and will assist in implementing the
training through the proposed model in a phased manner.
Activity:
It is proposed to hold training of AWWs in inter-personal communication so that they can
bring about behavior change in mothers and influencers. The training will be done in a step
ladder manner as follows:
IPC experts will train 60 selected CDPOs as Master Trainers in the technique of IPC.
The CDPOs will be selected from all the CDPOs based on their interest and existing
skills. The training will be at State HQ or some other suitable place. The training will
be of two day duration.
Each team of two CDPOs (Master Trainer) will train Supervisors in batches of 20
Supervisors. Total five batches will be trained by every team. (Thus training load on
each CDPO team will be 100 Supervisors in five batches of 2 day each). MT can
stagger the training @ one or two training per week so that her own work does no
suffer.
The Supervisors will act as Trainer of AWWs for their respective clusters, covering
25 AWWs each. The training may be of two sessions of half day each or one full day
session. The Supervisor will hold half day refresher training every month to reinforce
the skills of AWWs in IPC.
(a) Suitable training modules will be developed for use of Master Trainers and Supervisors.
(b) Also job aids will be designed and printed for the use of AWWs in the community during
home visits, NHED sessions, during visit of women to AWC etc. Hands on training in the use
of the flip books will be imparted by Supervisors to AWWs in live situations.
(c) The training will be supported by Development Partner working in state and having
experience of imparting training on the issue.
Outcome-
Skill of AWWs and Supervisors in IPC improved
Indicator-
No. of AWWs and Supervisors trained in IPC technique and no. of them started IPC during
different sessions (home visit, AWC visit, NHED sessions, etc).IPC training will also be
monitored by number of Supervisors holding refresher training for AWWs every month.
Time line-
II.II and IV quarter of 2012-13..
Budget-
i) Training of 60 Master Trainers (CDPOs) by experts in IPC
(Including fee of experts) = Rs. 1.0 lakhs
ii) IPC training of Supervisors by Master Trainers CDPOs)
3000 Supervisors x 150 = Rs. 4.5 lakhs
iii) Honoraria to CDPO – Rs 150 / batch x 5 batches per Master Trainer = 750.0
70
Total honoraria to 60 Master Trainers= 750 x 60 = Rs 45,000
iv) Training of AWWs in IPC by Supervisors Rs. 100 per AWW/ day
80,000 AWWs x 100 = Rs. 80.0 lakh
v) Honoraria to Supervisors for training AWW (Rs. 200) for two trainings
Total honoraria to Trainers (Supervisors) – 3000 x 200 = 6.00 lakhs
vi) Expenditure on training modules, stationery, etc. (Rs. 20 per participant x 80,000) =
16 lakh
vii) Development and printing of job aids for AWWs – 80,000 x 200 = 160 lakhs
Total of i) to vii) above= Rs. 267.95 lakhs
3. Mobile tracking system for program activities and malnourished childrenSAM
children
At present, ICDS programme activities are monitored through MPR. Monitoring by MPR has
several shortcomings because apart from incomplete and inconsistent data the information
reaches the program management after several weeks. Timely action on the basis of field
data is not possible. To monitor the services being provided by AWCs and to track the
status of severly malnourished children on real time basis is a challenging task. It is,
therefore, proposed to introduce a system of mobile tracking of AWC services.
Activity
Under the scheme it is proposed to utilize existing private call centres / mobile telephone
sevices to receive daily information from the AWWs. The sector supervisors will collect the
information about functioning of AWCs, distribution of SNP meals/ THR, attendance of
children in PSE program, home visits made, VHND held, etc. A fixed time will be used to
contact the AWW who will be available with the required information. The Supercisor, in
turn, will pass on the collated information to the Block/ District units. Close monitoring of the
activities of AWCs will be possible by this system. Wherever necessary (such as AWCs not
opening, SNP not being distributed, etc) prompt action will be possible by the management
on receiving information from the field.
Outcome
Information about the AWC activity and surveillance of malnourished children is
strengthened.
Indicator
Number and percentage of AWWs contacted through mobile tracking system
Timeline
II, III, IV quarters of 2012-13.
Budget:
Rs.5.00 per day x 300 days for each AWC=Rs 1500 x 80160 = Rs.1202.4 Lakhs
4I. Special request for better Services
4I.1. Budget for construction of AWC Buildings:

71
There 37392 AWC are running in rented building, 20595 in other building and 1231 AWC
are newly sanctioned. Hence state proposes requirement of Rs. 2416.13 Crores for
construction of 41231 new Anganwadi Building.
4I.2. Increase in rent of AWC and Project Office
The rent for urban AWC is Rs. 750.00 per month and for rural AWC is 200.00 which is quite
less for the required space to run all the activities at AWC. Hence we propose increase in
rents for urban to 1000.00 and rural to 500.0 . Similarly, the project offices are functioning
either from Government building or rented building, in rented building there is a constraint
bof space for storing THR in the present rent rate . Hence we propose rent for 268 project
office cum godown @ Rs 3000.00 per month. The total budget required for AWC and
project office rent will be Rs. 28.12 Crores.
4I.3. Uniform for children
Like primary school and private schools have uniform for their children, so to bring uniformity
in the children who come to AWC we propose to provide them a set of uniform to chidren
between 3 to 6 years of age group. There are 40lakhs children who fall in the age group of
3- 6 years the budget required will be Rs. 100.00 Crores (@Rs.250.00)
4I.4.Transportation of THR from CDPO office to AWCs
The unit cost for SNP is Rs. 4 which includes the cost of transportation also, but this
amount is not sufficient for providing SNP excluding transportation, Hence we propose
addition budget for transportation of SNP from CDPO to AWCs - 80160*2Quintal*50* 12 =
Rs 9.61 Crores.
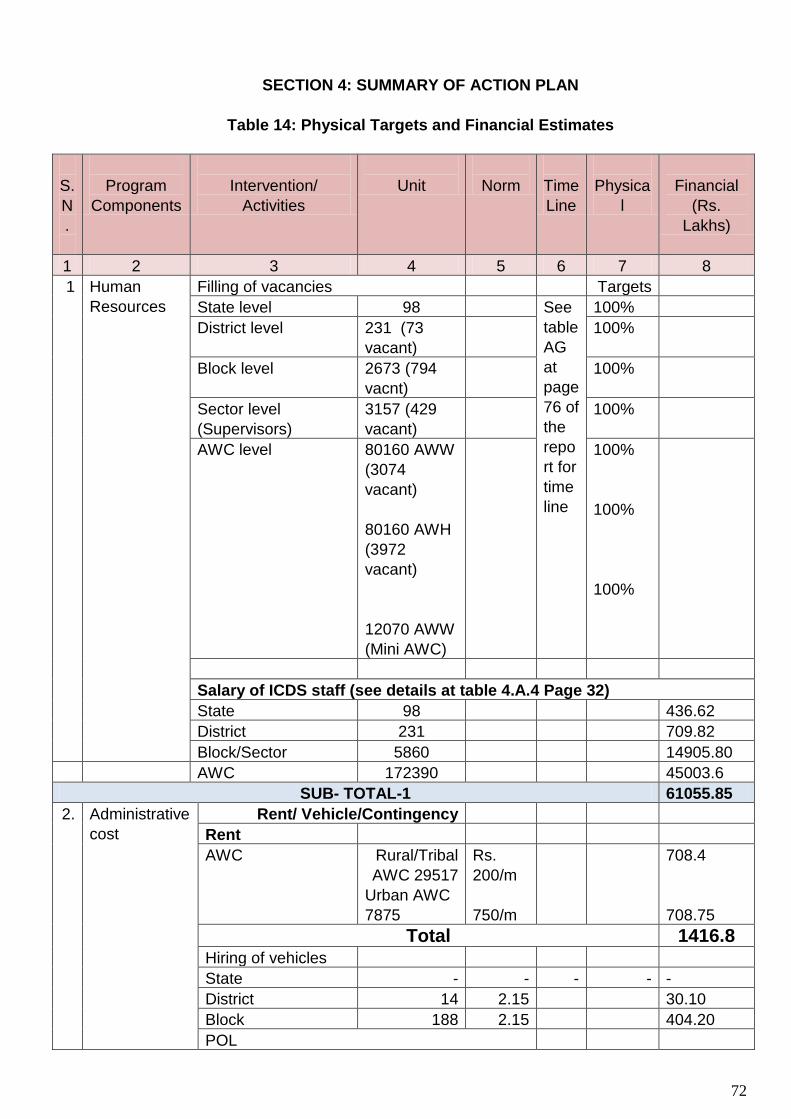
72
SECTION 4: SUMMARY OF ACTION PLAN
Table 14: Physical Targets and Financial Estimates
S.
N
.
Program
Components
Intervention/
Activities
Unit
Norm
Time
Line
Physica
l
Financial
(Rs.
Lakhs)
1 2 3 4 5 6 7 8
1 Human
Resources
Filling of vacancies Targets
State level 98 See
table
AG
at
page
76 of
the
repo
rt for
time
line
100%
District level 231 (73
vacant)
100%
Block level 2673 (794
vacnt)
100%
Sector level
(Supervisors)
3157 (429
vacant)
100%
AWC level
80160 AWW
(3074
vacant)
80160 AWH
(3972
vacant)
12070 AWW
(Mini AWC)
100%
100%
100%
Salary of ICDS staff (see details at table 4.A.4 Page 32)
State 98 436.62
District 231 709.82
Block/Sector 5860 14905.80
AWC 172390 45003.6
SUB- TOTAL-1 61055.85
2. Administrative
cost
Rent/ Vehicle/Contingency
Rent
AWC Rural/Tribal
AWC 29517
Urban AWC
7875
Rs.
200/m
750/m
708.4
708.75
Total 1416.8 Hiring of vehicles
State - - - - -
District 14 2.15 30.10
Block 188 2.15 404.20
POL

73
State 10 1.2 12.0
District 36 1.2 43.20
Block 265 1.25 331.25
Total 820.75
Contingency
State level 1 2.0 2.0
District level 50 1.0 50.0
Block level 453 0.40 181.20
AWC 80160 0.006 480.9
Total 714.1
SUB-TOTAL- 2 2951.65
3. Supplementary
Nutrition
Supply of SN to children, P & L
women and AGs
Children 6
months- 6 yrs
85,00,000 Rs. 4 x
300
102000 .00
P & L women 1410000 Rs. 5x
300
21150.00
Severe
malnourished
children
1.87,599 Rs. 6 x
300
3376.78
SUB- TOTAL -3 Note: 50% of cost of SNP to be borne by State 126526.78
4. Procurement Supply of material & equipments (see table 4B.1 at page 37)
PSE kit 80160 0.01 lakh/ kit 801.60
Medicine kit 80160 0.006 lakh/ kit 480.96
PSE kit (Mini
AWC)
12070 0.005lakh/kit 60.35
Medicine kit (Mini
AWC)
12070 0.003lakh/kit 36.21
Weighing scales
Salter scale
23537 0.0075 / scale 176.52
Baby weighing
scale
51787 0.01 lakh /
scale
517.87
Adult weighing
scale
45485 0.01 lakh /
scale
454.85
Computers/ Printers and UPS
State level 10 0.50 5.0
District level 10 0.50 5.0
Block level 200 0.50 100.0
Almirah/ Storage
box/ Utensils,
equipment, etc
See table 4B.1 details
State level 8.55
District level 50 districts 0.50 25.0
Block level 453 Blocks 0.20 90.6
AWC level@ 0.05
lakhs for furniture
51231 AWC 0.05 2561.55
SUB- TOTAL – 4 5324.06
5. Training and Regular training See 1110.35

74
capacity
building
(induction/ job/
Refresher
annexure 5
MPR /MIS training
for ICDS staff
1753.95
Exposure Visit 10.0
SUB – TOTAL- 5 2874.3
6. IEC Mangal Diwas 80160
AWCs
0.025 2004.0
IEC per AWCs /yr 80160
AWCs
0.01 801.60
SUB - TOTAL- 6 2805.6
7. Monitoring &
Evaluation
Routine
monitoring
through MPR
80160
AWCs
0.005 400.8
Register, records
etc. (80160
+12070 mini
AWC)
.005 461.15
SUB-TOTAL-7 861.95
8 Others Uniform to
AWW/AWH
80160
AWCs
+80160
AWHs+1207
0 Mini
AWWs /
=172390
Rs. 425
/
worker
681.36
Convergent
workshops
50 districts 1.0 lakh
/ distric
50.0
Flexi Fund for the
AWCs
92230 0.01 922.3
Travel 2297.0
Office expense 620.0
Special initiatives :
See details at item 4 K at page 60 of the report.
1.Orientation workshops for PRI Members 665.0
2.Appointment of additional AWWs at 11000 AWCs 643.50
4. Training of AWWs and Supervisors in Inter-personal
communication
267.95
5. Mobile tracking system for program activities 1202.4
SUB- TOTAL-8 7349.51
GRAND TOTAL 209749.70
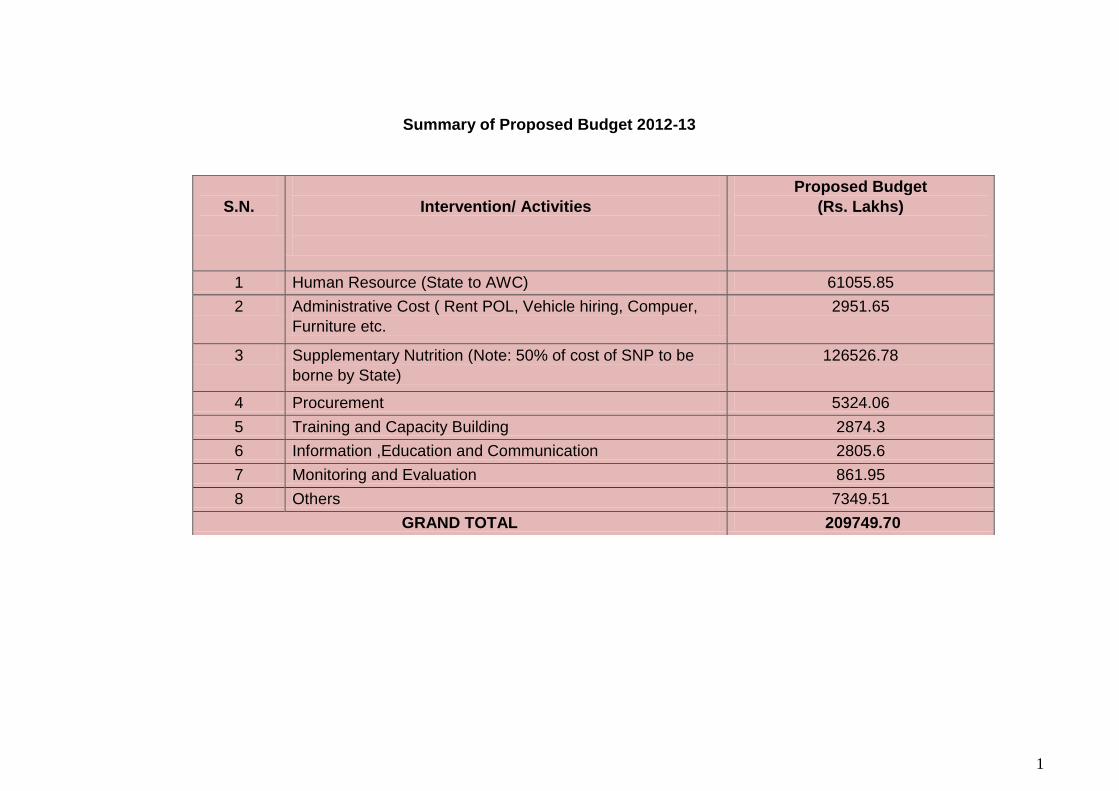
1
Summary of Proposed Budget 2012-13
S.N.
Intervention/ Activities
Proposed Budget
(Rs. Lakhs)
1 Human Resource (State to AWC) 61055.85
2 Administrative Cost ( Rent POL, Vehicle hiring, Compuer,
Furniture etc.
2951.65
3 Supplementary Nutrition (Note: 50% of cost of SNP to be
borne by State)
126526.78
4 Procurement 5324.06
5 Training and Capacity Building 2874.3
6 Information ,Education and Communication 2805.6
7 Monitoring and Evaluation 861.95
8 Others 7349.51
GRAND TOTAL 209749.70
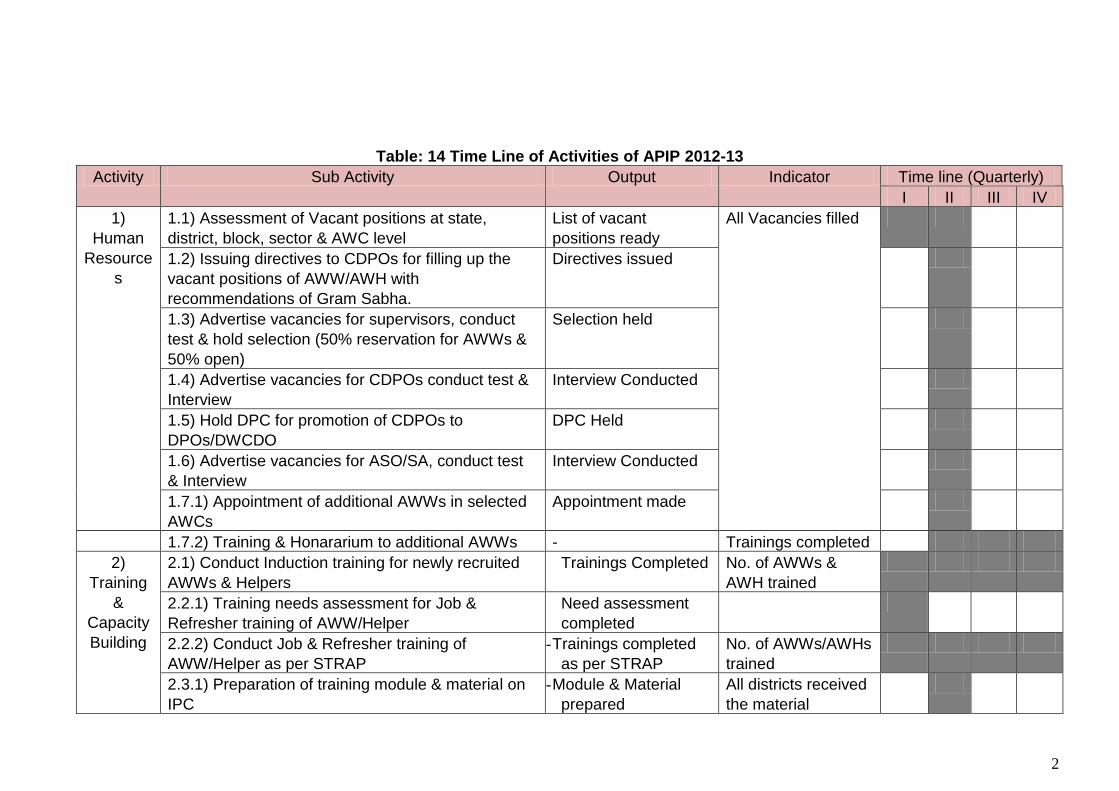
2
Table: 14 Time Line of Activities of APIP 2012-13
Activity Sub Activity Output Indicator Time line (Quarterly)
I II III IV
1)
Human
Resource
s
1.1) Assessment of Vacant positions at state,
district, block, sector & AWC level
List of vacant
positions ready
All Vacancies filled
1.2) Issuing directives to CDPOs for filling up the
vacant positions of AWW/AWH with
recommendations of Gram Sabha.
Directives issued
1.3) Advertise vacancies for supervisors, conduct
test & hold selection (50% reservation for AWWs &
50% open)
Selection held
1.4) Advertise vacancies for CDPOs conduct test &
Interview
Interview Conducted
1.5) Hold DPC for promotion of CDPOs to
DPOs/DWCDO
DPC Held
1.6) Advertise vacancies for ASO/SA, conduct test
& Interview
Interview Conducted
1.7.1) Appointment of additional AWWs in selected
AWCs
Appointment made
1.7.2) Training & Honararium to additional AWWs - Trainings completed
2)
Training
&
Capacity
Building
2.1) Conduct Induction training for newly recruited
AWWs & Helpers
Trainings Completed No. of AWWs &
AWH trained
2.2.1) Training needs assessment for Job &
Refresher training of AWW/Helper
Need assessment
completed
2.2.2) Conduct Job & Refresher training of
AWW/Helper as per STRAP
- Trainings completed
as per STRAP
No. of AWWs/AWHs
trained
2.3.1) Preparation of training module & material on
IPC
- Module & Material
prepared
All districts received
the material
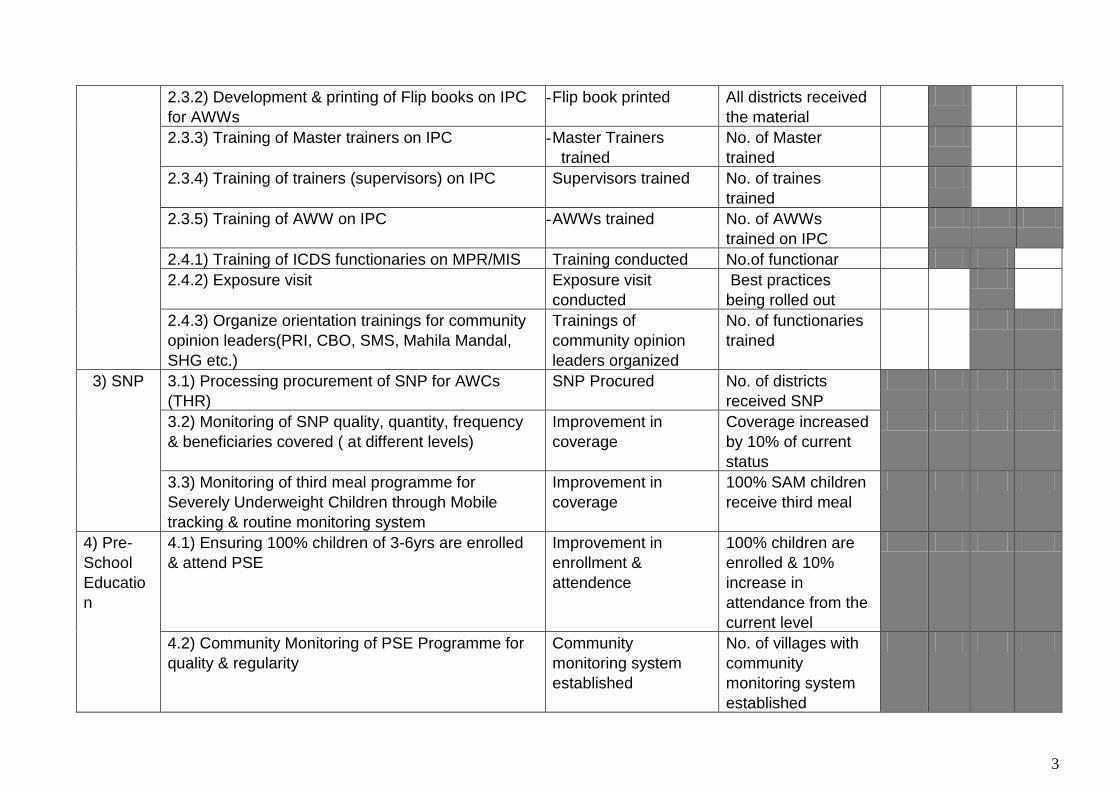
3
2.3.2) Development & printing of Flip books on IPC
for AWWs
- Flip book printed All districts received
the material
2.3.3) Training of Master trainers on IPC - Master Trainers
trained
No. of Master
trained
2.3.4) Training of trainers (supervisors) on IPC Supervisors trained No. of traines
trained
2.3.5) Training of AWW on IPC - AWWs trained No. of AWWs
trained on IPC
2.4.1) Training of ICDS functionaries on MPR/MIS Training conducted No.of functionar
2.4.2) Exposure visit Exposure visit
conducted
Best practices
being rolled out
2.4.3) Organize orientation trainings for community
opinion leaders(PRI, CBO, SMS, Mahila Mandal,
SHG etc.)
Trainings of
community opinion
leaders organized
No. of functionaries
trained
3) SNP 3.1) Processing procurement of SNP for AWCs
(THR)
SNP Procured No. of districts
received SNP
3.2) Monitoring of SNP quality, quantity, frequency
& beneficiaries covered ( at different levels)
Improvement in
coverage
Coverage increased
by 10% of current
status
3.3) Monitoring of third meal programme for
Severely Underweight Children through Mobile
tracking & routine monitoring system
Improvement in
coverage
100% SAM children
receive third meal
4) Pre-
School
Educatio
n
4.1) Ensuring 100% children of 3-6yrs are enrolled
& attend PSE
Improvement in
enrollment &
attendence
100% children are
enrolled & 10%
increase in
attendance from the
current level
4.2) Community Monitoring of PSE Programme for
quality & regularity
Community
monitoring system
established
No. of villages with
community
monitoring system
established

4
4.3) Organization of Parent-AWW meet every month
for creating awareness about PSE
System of Parent
AWWs meet
established
No. of AWCs which
started organizing
regular meeting with
parents
5)
Procurem
ent
5.1) Procurement of PSE kit by DPOs as per
purchase rules
Kits procured No. of AWCs
received PSE kit
5.2) Procurement of Medicine kit by DPOs as per
purchase rules
Kits procured No. of AWCs
received Medicine
kit
5.3) Place orders for procurement of Computers &
Printers through LUN after finalizing the
specifications at DWCD
Orders placed No. of districts
/blocks received
supplies
5.4) Procurement of furniture & office equipments as
per purchase rules
Procurement done No. of districts
/blocks received
supplies
5.5) Assessment of requirement of serving utensils,
boxes, dari, furniture etc for AWCs
Assessment of
requirement made
No. of districts from
where assessment
received
5.6) Procurement of serving utensils, boxes, dari,
furniture etc for AWCs as per purchase rules
Procurement done No. of AWCs
received supplies
6) IEC 6.1) Strengthen Mangal Diwas Programme Mandal Diwas
strengthened
No. of AWCs where
all four Mangal
Diwas are held
regularly
6.2) Assess IEC needs & develop strategies &
material
IEC strategy
document developed
-
7)
Monitorin
g &
Evaluatio
n
7.1) Linking of Mobile tracking monitoring system &
referral of SAM children
7.2) Development & Printing of New MPR formats,
Checklist, Registers
Material developed No. of districts
started using new
MPR & formats
5
8) Others 8.1) Procurement of Sarees & badges to AWW &
AWH
Procurement made No. of AWWs &
Helpers received
Sarees & badges
8.2) Organizing Convergence workshops for
improved interdepartmental coordination with
health, RD, Education, Tribal departments
Convergence
workshops for
interdepartmental
coordination initiated
No. of districts
started organizing
convergence
workshops
8.3) Strengthen NHED sessions in convergence
with health department
NHED sessions
strengthened
No. of NHED
sessions organized
as per the protocols
6
Section 5: Additional Information
Support Received from Development Partners in ICDS
III) MP Health Sector Reform Programme (MPHSRP) supported by DFID
The MPHSRP has been jointly designed by GoMP and DFID within the broader context of MP Health Sector Strategy. The Departments of Public Health and Family Welfare, (DoPH&FW) and Women & Child Development (WCD), Government of Madhya Pradesh (GoMP) have been implementing a DFID supported (2007-15 ) Madhya Pradesh Health Sector Reform Program (MPHSRP). This includes financial and technical assistance of £120m with total fund allocation to DWCD of £35m: of which £16m has been disbursed till 2011-12. The goal of MPHSRP is to improve the health status of people in Madhya Pradesh - especially the poorest, and thereby accelerate the state's progress towards the MDGs. The purpose is to increase use of quality health services especially by the poorest people and in underserved areas. This program provides a unique opportunity for the government to prioritize the use of its limited resources and to help address the critical shortcomings in the public health system. The main objectives of this program are reduction in: infant mortality, maternal mortality, total fertility rate, making health outcomes and utilization of services more equitable, addressing malnutrition among children and reducing morbidity and mortality from common communicable diseases such as malaria, leprosy and tuberculosis. Key Reform Dimensions To achieve these objectives, the program supports the following five dimensions of reforms: 1. Improve availability of quality public and private health, sanitation and nutrition services,
particularly in the underserved districts, 2. Improve availability of more and better trained staff, in particular in the underserved districts, 3. Strengthen financial management and procurement systems, 4. Bring about increased demand for nutrition, health and sanitation services; and 5. Strengthen M&E Systems. These outputs are in turn co-related with a host of agreed milestones, the achievement of which is facilitated by the MP TAST under the Technical Cooperation component of the MP HSRP. The MPHSRP support for the DWCD/ICDS over 2007 -2012 includes the following: Design of State nutrition mission (AtalBal Mission) and a PMU set up by MPTAST within
AtalBalMissions Implementation of state nutrition mission (ABM) supported in 5 districts of Sagar Divisions. TA team has supported the training of 156 ICDS Supervisors and also trained Block officials
(CDPOs) from all the 134 projects in 15 high burden districts for supportive supervision and building correct knowledge about core nutrition interventions.
Develop monitoring and Evaluation framework for ICDS Established M&E unit - 2 people placed in the department from TAST support Revised MPR as per needs of the State and GOI and Develop Web enabled MIS –online as
well as offline system for data entry.ilot conducted on revised MPR and ONLINE MIS system in 50 blocks (one block from across the state
IT enabled MIS for ICDS is now scaled up all over the state, with a dedicated URL created for MIS: mpwcdmis.org. 3409 ICDS functionaries were trained during the process with DFID TA support. Registers have been designed keeping in view the revised on-line MPR format and the needs of the GOI. Number of registers was reduced from 9 to 7.
DFID TA also funds the CRISP (web management services) to support A large scale BCC campaign and IPC is being designed under MPHSRP to promote IYCF,
hand washing and toilet use

7
DFID TA has supported roll out of SABLA and IGMSY in 2 districts. DFID TA also funds the CRISP (web management services) to maintain web based MIS
system for the department.
DFID TA support over 2012 onwards will focus on: ABM district and block staff training and supervision
Direct implementation support of ABM in 11 districts
All district plans will be monitored quarterly at state level.
Supervisors & CDPOs training will be continued as well as training of AWW as needed.
Facilitate state level convergence with NRLM and Tejaswani and work with community groups/SHGs/Volunteers.
Sabla: TAST will support Sabla in 2 districts and develop linkages to strengthen the life skills and vocational/skill development.
Behavior Change Communication; the BCC consortium – BBCWST and Care – is now in place and help implement BCC activities.
MIS strengthening:
Training of CDPOs and Supervisors on use and analysis of MPR data
Concurrent monitoring of outcomes and processes to be started (every quarter 8-10 districts to be monitored with quantitative and qualitative surveys)
NIN survey to be repeated in 2013 to track progress
II) Support by UNICEF
Technical support on promotion of infant and young child feeding practices including the use of WHO child growth standards at state, division and district level
Technical support in development of vision and strategy document for Atal Arogya and Bal Poshan Mission and development of district level strategy document. Technical support in operationalization of the mission at state, division and district level.
Provide technical support for planning, implementation and monitoring of State Government’s initiatives and schemes like SABLA,
Streamlining the timely identification, referral of SAM children to NRCs
Unicef is also extending financial and technical support Such as Gap filling supply for ICDS quality improvement (Salter Scale, Growth Registers, Monthly weight registers, IYCF Flip book & Flash Cards), Supply to NRCs - Electronic weighing scale, Length Board, Camera, MUAC Tape, Bed sheets, Feeding & Protocol Panels.
II) Support by Micronutrient Initiative(MI)
MI support mainly for strengthening the vitamin A supplementation in routine immunization & along with deworming during the Bal Suraksha Maah rounds
MI provides training & organize workshops for capacity building of officials & staff of different line departments at different levels on vitamin A supplementation.
IEC activities & printing of reporting formats for the Bal Suraksha Maah is also one of the major activities supported by MI.

8
Names of Key Officers of DWCD and Their Telephone Numbers
Department of Women and Child Development
Vijaya Raje Vatsalya Bhavan, Arera Hills, Bhopal, M.P.
Names, Addresses and Contact Numbers of Key Officers
Name Address Telephone Nos.
Office Residence
Shri B.R. Naidu, Principal Secretary
C-2/ 8, Char Imli, Bhopal
0755- 2550894 0755-2559692, 9425602333
Shri D. D. Agarwal, Commissioner
0755-2550909
Shri H.C. Agrawal, Additional Director
86-A, Janaki Nagar, Bhopal
0755-2550940 8109210060, 9424468226
Shri Akshaya Shrivastava, Jt. Director
109/12, Shivaji Nagar, Bhopal
0755- 2550928 e-mail:
9424410467
Shri. Pankaj Mohan 0755-2550916 9425155066
Shri R.P. Singh, Joint Director
HIG-3/135, Bag Mugalia, Bhopal
0755-2550922 9827227727
Shri R.C. Shukla, Deputy Director
G-2/103, 1100 Quarters
9425026630
Shri Harish Khare, Deputy Director
F-91/ Tulsi Nagar 0755- 2550936 94255614440
ICDS Website URL : www.mpwcd.nic.in
Names, Addresses and Contact Numbers of District level Program Officers
Indore Division Address Telephone
1 Mr. Vishal Nadkarni District Program Officer
Department of Women & Child Development, Room no.107, Collectorate Campus, Moti Tabela, Indore, Dist Indore.
Ph: 0731-2366058, 9425103731
2 Mr. N.S. Tomar District Program Officer
Department of Women & Child Development Collectorate Campus, Dhar , District Dhar
Ph: 07292-2235066, 9425942401
3 Ms. Jaywant Verma District Program Officer
Department of Women and Child Development, Asha Gram Road, Barwani, District Badwani
Ph.07290- 224445 94254 08498
4 Mr. L.N. Kandwal District Program officer
Women and Child Development Office , Indore Road, Near TAFE Tractors Khargone, Dist. Khargone,
Ph: 0728-2232596, 94251 91303
5 Mr. Rajesh Gupta District Program Officer
Office of Women and Child Development Department, Khandwa District Khandwa (M.P.)
Ph: 0733-2223794, 9425355652

9
6 Mr. R.S. Jamra District Program Officer
Office of Women and Child Development Department Tanki Ground, Umrali Road, Alirajpur, District Alirajpur (MP)
Ph: 07394-234350, 9993109030
7 Mrs. Neelu Bhatt, District Program Officer
Office of Women and Child Development Department, Jhabua District Jhabua (M.P.)
Ph: 07392-244397, 9425061658
8 Ms. Shweta Raghav District Program Officer
Office of Women and Child Development Department Renuka Mata Mandir Road Near Shikarpura Thana, Burhanpur (MP) District Burhanpur (M.P.)
Ph: 07325-251931, 99779 19111
Ujjain Division
9 Ms. Nishi Singh District Program Officer
Department of Women & Child Development 38. Prashasnik Kshetra, Sector Wing D, Mahendra Bhatnagar Marg, Near Iskon Temple, Ujjain (MP)
Ph: 0734-2511658, 9827350147 Email: [email protected]
10 Mr. D.S Meena District Program Officer
Office of Women and Child Development Department Old Kendriya Vidyalaya Katju Nagar, District Ratlam (M.P.)
Ph:- 07412-270433, Joshi acct:9424047811
11 District Women & Child Development Officer,
Office of Women and Child Development, Old Kendriya Vidyalaya, Ratlam
Ph:- 7412- 270433, 267876
12 Mrs. Relam Baghel District Program officer
Department of Women and Child Development Women and Child Development Office Nayi Abadi District Mandsaur (M.P)
Ph:- 07422-242543, 9424892032
13 Ms. Sunita Yadav District Program Officer
Office of Women and Child Development Department Collectorate Campus Lalghati, District Shajapur (M.P.)
Ph: 9425065313, 07364-226639
14 Mrs. Sushma Bhadoria District Program Officer
Office of Women and Child Development Department Collectorate, District Neemuch (M.P.)
Ph: 9425980823, 07423-231020
15 Ms. Tripti Tripathi District Program Officer
Department of Women & Child Development Collectorate Campus District Dewas
Ph: 07272-250117, 98931 21587
Bhpal Division
16 Ms. NakiJahan Qureshi District Program Officer
Office of Women and Child Development Department, B-Block, Old Secretariat, Collectorate Campus District Bhopal (M.P.)
Ph: 9425083175, 0755-2548599

10
17 Mr. Brajesh Shivhare District Program Officer
Office of Women and Child Development Department District Sehore (M.P.),
Ph:- 0756-2222752, 9407273520, 94250 39265
18 Ms. Rama Mukati District Program Officer
Office of Women and Child Development Department Collectorate Campus District Rajgarh (M.P.)
Ph: 9 94258 89970 0737-2255083
19 Mr.D.S. Meena District Program Officer
Office of Women and Child Development Department Collectorate Campus District Raisen (M.P.),
Ph:- 07482-222132, 989375413
20 Mr. Sanjay Tripathi District Program Officer
Office of Women and Child Development Department Commissioner Building District Hoshangabad (M.P.)
Ph: 94257 25653, 07574-253254
20 Mr. Devendra Sundaryal District Program Officer
Office of Women and Child Development Department Behind Collectorate Office Collectorate Campus District Vidisha (M.P.)
Ph: 9479879741, 0759-2232986
21 Mr. Lalit Dehariya District Program Officer
Office of Women and Child Development Department Near Sunrays school, Pandey Compound, District Harda (M.P.)
Ph: 94251 75811, 07577-225973
22 Mr. Pradeep Rai District Program Officer
Office of Women and Child Development Department Near Bus Stand, District Betul (M.P.)
Ph: 07141-230305, 9926377522
Sagar Division
23 Mr. Brijesh Tripathi District Program Officer
Department of Women & Child Development Near Police line Road District Chhattarpur
Ph: 07682- 243590, 9425362263
24 Mr. Sanjay Singh District Program Officer
Office of Women and Child Development Department Tehsili Compound District Sagar (M.P.)
Ph: 07582-223510; 9424439925
25 Mr. B.L. Prajapati District Program Officer
Office of Women and Child Development Department Collectorate Campus District Tikamgarh (M.P.)
Ph: 07683-242257; 9425141901
26 Mr. Yogendra Yadav District Program Officer
Office of Women and Child Development Department Old Collectorate Building District Damoh (M.P.)
Ph: 07812-222473, 94254-38991
27 Mr. Nayan Singh District Program Officer
Office of Women and Child Development Department Collectorate Office, Opposite Ram Jankin Mandir, District Panna (M.P.)
Ph: 07732-252159, 9424762973
Chambal Division
28 Mr. D.K.Sidharth District Program Officer
Office of Women and Child Development Department Collectorate Campus District Morena (M.P.)
Ph: 9425635752, 07532-223379

11
29 Ms. Kalpana Bohre District Program Officer
Office of Women and Child Development Department Collectorate, District Bhind (M.P.)
Ph: 98263-62417, 07534-230427; Accountant: Maujiram ji:- 9754517996
30 Mr.Sourabh Singh District Program Officer
Office of Women and Child Development Department Collectorate Campus District Sheopur (M.P.)
Ph: 07530-222088, 9425131721
Gwalior Division
31 Mrs. Seema Sharma, District Program Officer,
Office of Women and Child Development Department Moti Mahal, Gwalior
, Ph: 07512-446217, 9425114265
32 Mr. D.S. Jadon District Program Officer
Office of Women and Child Development Department Collectorate Campus District Datia (M.P.)
Ph: 942540 07197, 07522-233724
33 Mr. R.C. Tripathi District Program Officer
Department of Women & Child Development Cantt Area, District Guna (MP)
Ph: 94254-72915, 07542-250168
34 Mr.Sajan Aluna District Program Officer
Department of Women & Child Development Collectorate Campus District Shivpuri (MP)
Ph: 94254 36991, 0749-2234704
35 Mr. Akhilesh Jain District Women & Child Development Officer
Office of Women and Child Development Department Nehru Degree College, District Ashoknagar (M.P.)
Ph: 94250 51653, 07543-220306
Rewa & Shahdol Division
36 Ms. Usha Solanki District Program Officer
Office of Women and Child Development Department Shilpi Plaza, A- Block 3rd Floor, District Rewa (M.P.)
Ph: 07662-256857, 94251-84993
37 Mrs. Saurabh Singh District Program Officer
Office of Women and Child Development Department District Collectorate Campus, District Satna (M.P.)
Ph: 94251 31721, 07672-224182
38 Mr. M.L. Mehra District Program Officer
Office of Women and Child Development Department Old Collectorate Building District Shahdol (M.P)
Ph: 07652-241538, 9425184228
39 Ms. Laxmi Dhurve District Program Officer
Office of Women and Child Development Department Near Collectorate Campus District Annupur (M.P.)
Ph: 07659-222672, 222287, 9407091821
40 Ms. Leekha Shivedi District Program Officer
Office of Women and Child Development Department Collectorate Campus District Dindori (M.P)
Ph: 9826736833, Ph. 07644- 234965, 234364
41 Mr. Gautam Adhikari, District Program Officer
Office of Women and Child Development Department, District Sidhi,
Ph. 07822-250302, 9425472915
12
42 Mrs. Subhadra Manikpuri District Women & Child Development Officer
Office of Women and Child Development Department Collectorate Campus District Umaria (M.P.)
Ph: 07653223397, 9407855295
43 Ms. Pratibha Pandey, District Program Officer
Office of Women and Child Development Department, District Singrauli (M.P.)
Ph:- 9425470883
Jabalpur Division
44 Mr. H.K. Sharma District Program Officer
Office of Women and Child Development Department Collectorate Campus District Jabalpur (M.P.)
Ph:, 0761-2609545, 94258-49111
45 Ms. Swarnima Shukla District Program Officer
Office of Women and Child Development Department Collectorate Campus District Chhindwara (M.P.) P
Ph: 94250-51420, 07162-243421
46 Ms. Shanti Bele District Program Officer
Office of Women and Child Development Department Collectorate Campus District Narsinghpur (M.P.)
Ph: 07792-230512, 94250-40632
47 Mrs. Shashi Uike District Program Officer
Office of Women and Child Development Department Near Smarak Chouraha District Mandla (M.P.)
Ph: 07642-252373, 993092532
48 Ms. Neelima Tiwari District Program Officer
Office of Women and Child Development Department, District Balaghat,
Ph:- 07632-241637, 94254-47851
49 Mr. Manish Seth District Program Officer
Office of Women and Child Development Department, District Katni
Ph:- 07622-224623, 9425159633
50 Mr. Bharat Singh Rajput District Program Officer
Office of Women and Child Development Department, District Seoni
Ph:- 07692-228191, 9009220758

13
ANNEXURES
Annexure- 1
Nutritional Status Of Children Up to 6 Years By SD Classification
Districts
Under Nutrition among 0-5 Yr Children (< Median – 2sd)
Current survey (2010-11)
Underweight Stunting Wasting
Alirajpur 60.8 52.9 32.6
Anuppur 55.8 45 28.9
Ashokngar 49.9 55.6 20
Balaghat 48.1 40.7 23.6
Barwani 65.1 58 34.8
Betul 43.2 38.1 21.1
Bhind 55.1 63.5 16.0
Bhopal 55.8 47.7 24.6
Burhanpur 55.4 48.6 26.7
Chhatarpur 48.3 45.9 21.9
Chindwara 48.8 44.3 27.3
Damoh 42.9 39.5 26.6
Datia 59.6 66.7 21.1
Dewas 40.9 38.2 22.5
Dhar 54.4 46.9 33.2
Dindori 61.7 50.3 31.6
Guna 50 48.4 25.3
Gwalior 56.6 65.2 21.1
Harda 53.7 47.6 23.5
Hoshangabad 38.4 37.6 24.8
Indore 34.9 34.1 21.7
Jabalpur 45.7 39.1 24.2
Jhabua 57 50.3 31.5
Katni 55.5 51.5 27.4
Khandwa 56.9 45.1 29.8
Khargone 58 50.6 30.8
Mandla 56.5 47.3 29.6
Mandsaur 52.5 45.1 27
Morena 53.2 15.2 15.2
Narsimhapur 46.1 49 16.9
Neemuch 48.1 36 24.1
Panna 50.3 42.1 29
Raisen 36.3 38.8 19.3

14
Rajgarh 56.5 46.6 40.2
Ratlam 49.1 42.1 29
Rewa 53.7 58.3 22
Sagar 48.3 61.5 19.2
Sathna 67.1 66.3 29.5
Sehore 40.5 41 21.2
Seoni 52.9 40.3 29.8
Shadol 56.5 42.1 32.6
Shajapur 51.7 43.3 30.1
Sheopur 52.3 64.6 17.9
Sidhi 54.5 52 25.4
Singrauli 58.8 51.8 34.3
Shivpuri 55 62 25.7
Tikamgarh 49.7 45.7 23.1
Ujjain 45 39.9 26.7
Umaria 66.6 60.3 32.9
Vidisha 34.7 50.8 16.3
Pooled 51.9 48.9 25.8
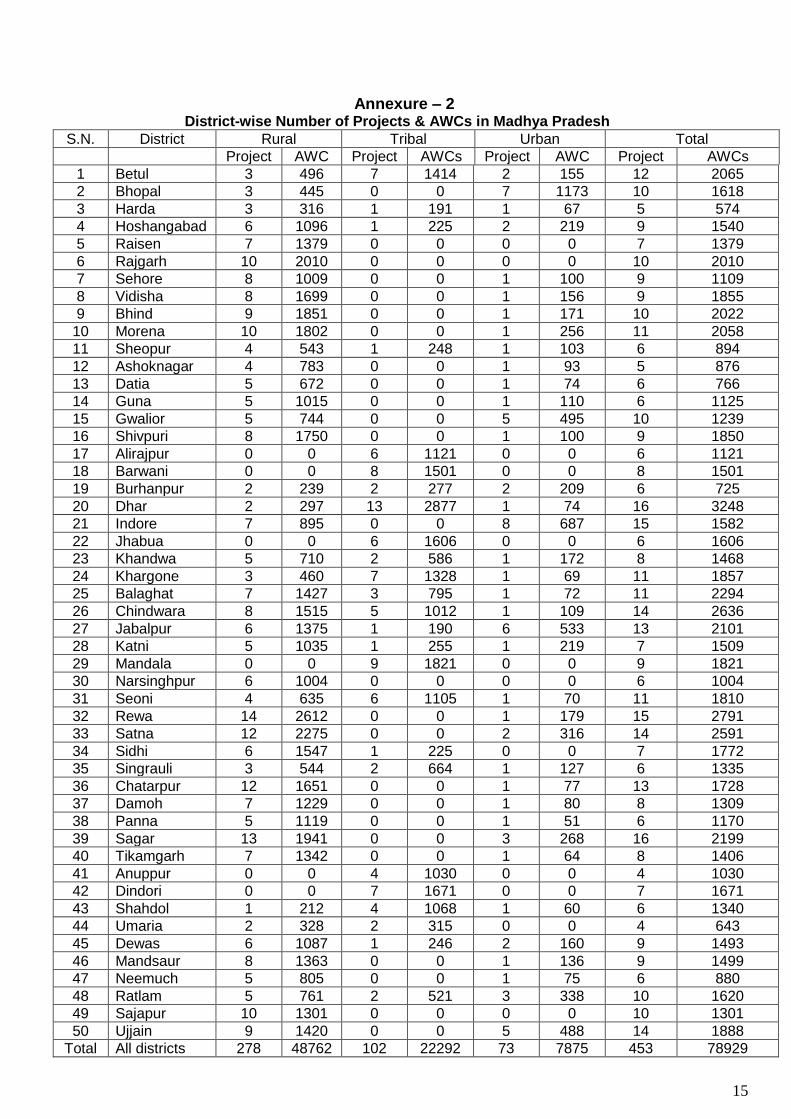
15
Annexure – 2 District-wise Number of Projects & AWCs in Madhya Pradesh
S.N. District Rural Tribal Urban Total
Project AWC Project AWCs Project AWC Project AWCs
1 Betul 3 496 7 1414 2 155 12 2065
2 Bhopal 3 445 0 0 7 1173 10 1618
3 Harda 3 316 1 191 1 67 5 574
4 Hoshangabad 6 1096 1 225 2 219 9 1540
5 Raisen 7 1379 0 0 0 0 7 1379
6 Rajgarh 10 2010 0 0 0 0 10 2010
7 Sehore 8 1009 0 0 1 100 9 1109
8 Vidisha 8 1699 0 0 1 156 9 1855
9 Bhind 9 1851 0 0 1 171 10 2022
10 Morena 10 1802 0 0 1 256 11 2058
11 Sheopur 4 543 1 248 1 103 6 894
12 Ashoknagar 4 783 0 0 1 93 5 876
13 Datia 5 672 0 0 1 74 6 766
14 Guna 5 1015 0 0 1 110 6 1125
15 Gwalior 5 744 0 0 5 495 10 1239
16 Shivpuri 8 1750 0 0 1 100 9 1850
17 Alirajpur 0 0 6 1121 0 0 6 1121
18 Barwani 0 0 8 1501 0 0 8 1501
19 Burhanpur 2 239 2 277 2 209 6 725
20 Dhar 2 297 13 2877 1 74 16 3248
21 Indore 7 895 0 0 8 687 15 1582
22 Jhabua 0 0 6 1606 0 0 6 1606
23 Khandwa 5 710 2 586 1 172 8 1468
24 Khargone 3 460 7 1328 1 69 11 1857
25 Balaghat 7 1427 3 795 1 72 11 2294
26 Chindwara 8 1515 5 1012 1 109 14 2636
27 Jabalpur 6 1375 1 190 6 533 13 2101
28 Katni 5 1035 1 255 1 219 7 1509
29 Mandala 0 0 9 1821 0 0 9 1821
30 Narsinghpur 6 1004 0 0 0 0 6 1004
31 Seoni 4 635 6 1105 1 70 11 1810
32 Rewa 14 2612 0 0 1 179 15 2791
33 Satna 12 2275 0 0 2 316 14 2591
34 Sidhi 6 1547 1 225 0 0 7 1772
35 Singrauli 3 544 2 664 1 127 6 1335
36 Chatarpur 12 1651 0 0 1 77 13 1728
37 Damoh 7 1229 0 0 1 80 8 1309
38 Panna 5 1119 0 0 1 51 6 1170
39 Sagar 13 1941 0 0 3 268 16 2199
40 Tikamgarh 7 1342 0 0 1 64 8 1406
41 Anuppur 0 0 4 1030 0 0 4 1030
42 Dindori 0 0 7 1671 0 0 7 1671
43 Shahdol 1 212 4 1068 1 60 6 1340
44 Umaria 2 328 2 315 0 0 4 643
45 Dewas 6 1087 1 246 2 160 9 1493
46 Mandsaur 8 1363 0 0 1 136 9 1499
47 Neemuch 5 805 0 0 1 75 6 880
48 Ratlam 5 761 2 521 3 338 10 1620
49 Sajapur 10 1301 0 0 0 0 10 1301
50 Ujjain 9 1420 0 0 5 488 14 1888
Total All districts 278 48762 102 22292 73 7875 453 78929

16
Annexure –3
List of Anganwadi Training Centres & Middle Level Training Centres in MP
S.N. Name of training Centres District
Government training centres
1 Government AWTC , Pawarkheda Hoshangabad
2 Government AWTC, Rajgarh Rajgarh
3 Government AWTC, Obaidullagunj Raisen
4 Government AWTC, Jabalpur-1 Jabalpur
5 Government AWTC, Jabalpur 2 Jabalpur
6 Government AWTC, Satna Satna
7 Government AWTC, Nogaon Chatarpur
8 Government AWTC, Shivpuri Shivpuri
9 Government AWTC, Dhar Dhar
10 Government AWTC, Tikamgarh Tikamgarh
Non-Government AWTC
1 AWTC, MP Council of Child Welfare, Bhopal Bhopal
2 AWTC, MP Council of Child Welfare, Gwalior Gwalior
3 AWTC, MP Council of Child Welfare, Seoni Seoni
4 AWTC, MP Council of Child Welfare, Shahdol,
Shahdol
5 AWTC, MP Council of Child Welfare, Mandla Mandla
6 AWTC, MP Council of Child Welfare, Ratlam Ratlam
7 AWTC, MP Council of Child Welfare, Jhabua Jhabua
8 AWTC, MP Council of Child Welfare, Ujjain Ujjain
9 AWTC,MP Council of Child Welfare, Chindwara
Chindwara
10 AWTC, Indore Indore
11 AWTC, Mahila Chetana Manch, Bhopal Bhopal
12 AWTC, Institute of Regional Analysis, Betul Betul
13 AWTC, Savya Sanchi Centre, Sidhi Sidhi
14 AWTC, Shri Ram Shankar Samiti, Morena Morena
15 AWTC, Matr Shakti Seva Kendra, Guna Guna

17
Annexure-4
District-wise number of NRC established in MP and Children Treated
(April 2011- March 2012) Source :- NRHM
Sr.
No.
District Name Fully Functional
NRCs
Partially Functional
NRCs
Total
NRCs
1 ANOOPPUR 4 - 4
2 ASHOKNAGAR 3 - 3
3 BALAGHAT 2 - 2
4 BARWANI 3 1 4
5 BETUL 5 - 5
6 BHIND 2 2 4
7 BHOPAL 3 1 4
8 BURHANPUR 3 - 3
9 CHHATARPUR 5 - 5
10 CHINDWARA 4 - 4
11 DAMOH 5 - 5
12 DATIA 3 2 5
13 DEWAS 4 - 4
14 DHAR 7 1 8
15 DINDORI 3 - 3
16 GUNA 3 2 5
17 GWALIOR 4 - 4
18 HARDA 3 - 3
19 HOSHANGABAD 5 1 6
20 INDORE 5 2 7
21 JABALPUR 6 - 6
22 JHABUA 4 - 4
23 ALIRAJPUR 2 - 2
24 KATNI 6 - 6
25 KHANDWA 5 - 5
26 KHARGONE 7 1 8
27 MANDLA 3 - 3
28 MANDSAUR 7 - 7
29 MORENA 5 - 5
30 NARSINGHPUR 2 1 3
31 NEEMUCH 3 - 3
32 PANNA 4 2 6
33 RAISEN 3 2 5
34 RAJGARH 2 1 3
35 RATLAM 2 3 5
36 REWA 5 2 7
37 SAGAR 3 3 6
38 SATNA 3 3 6
39 SEHORE 2 3 5
40 SEONI 2 - 2
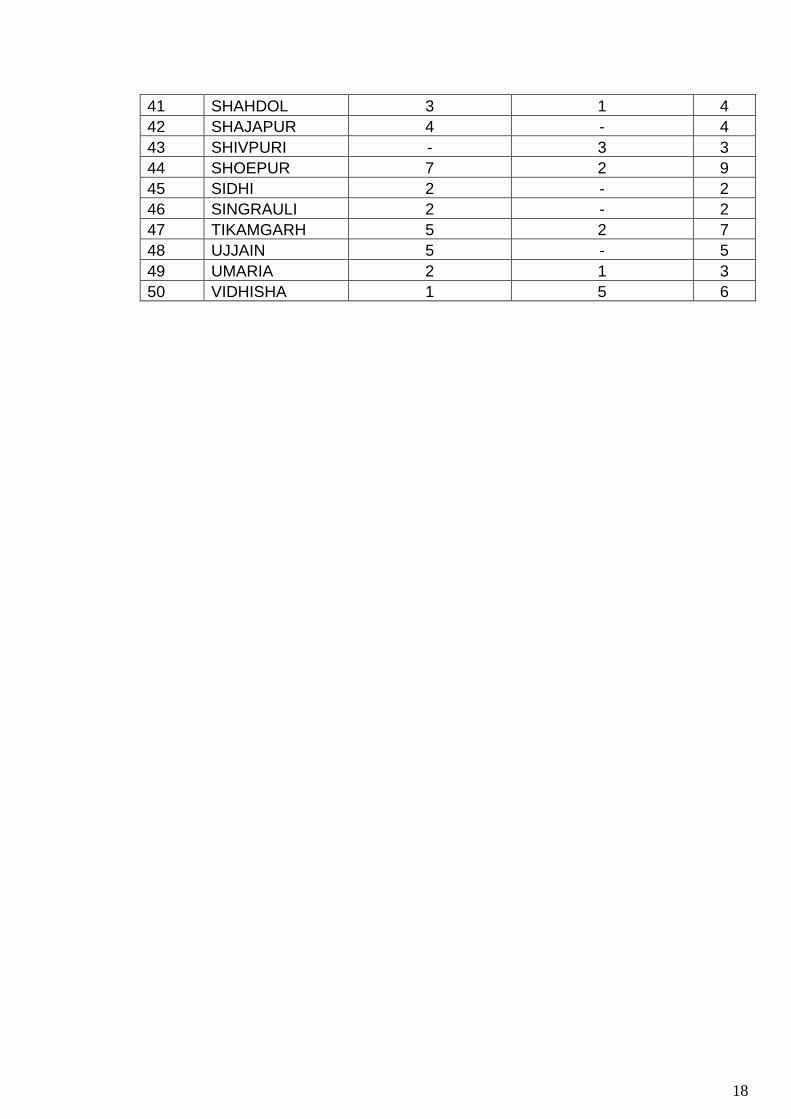
18
41 SHAHDOL 3 1 4
42 SHAJAPUR 4 - 4
43 SHIVPURI - 3 3
44 SHOEPUR 7 2 9
45 SIDHI 2 - 2
46 SINGRAULI 2 - 2
47 TIKAMGARH 5 2 7
48 UJJAIN 5 - 5
49 UMARIA 2 1 3
50 VIDHISHA 1 5 6

19
Annexure 5
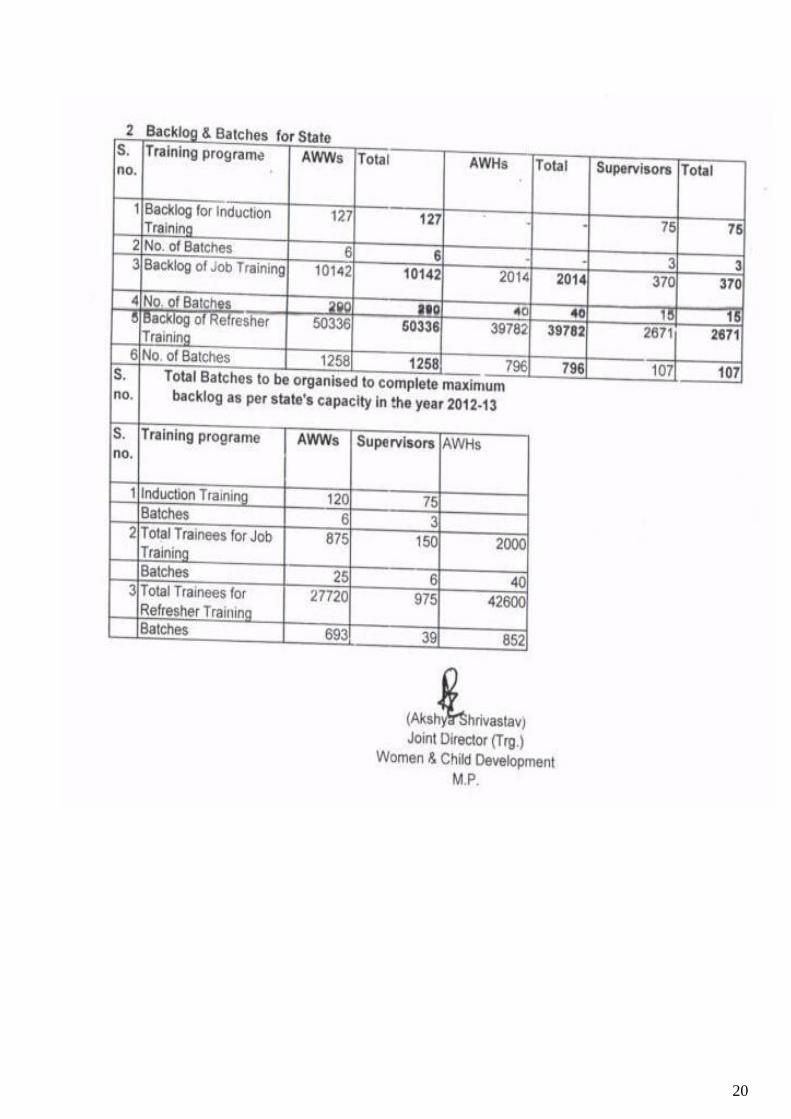
20

21

22

23

24
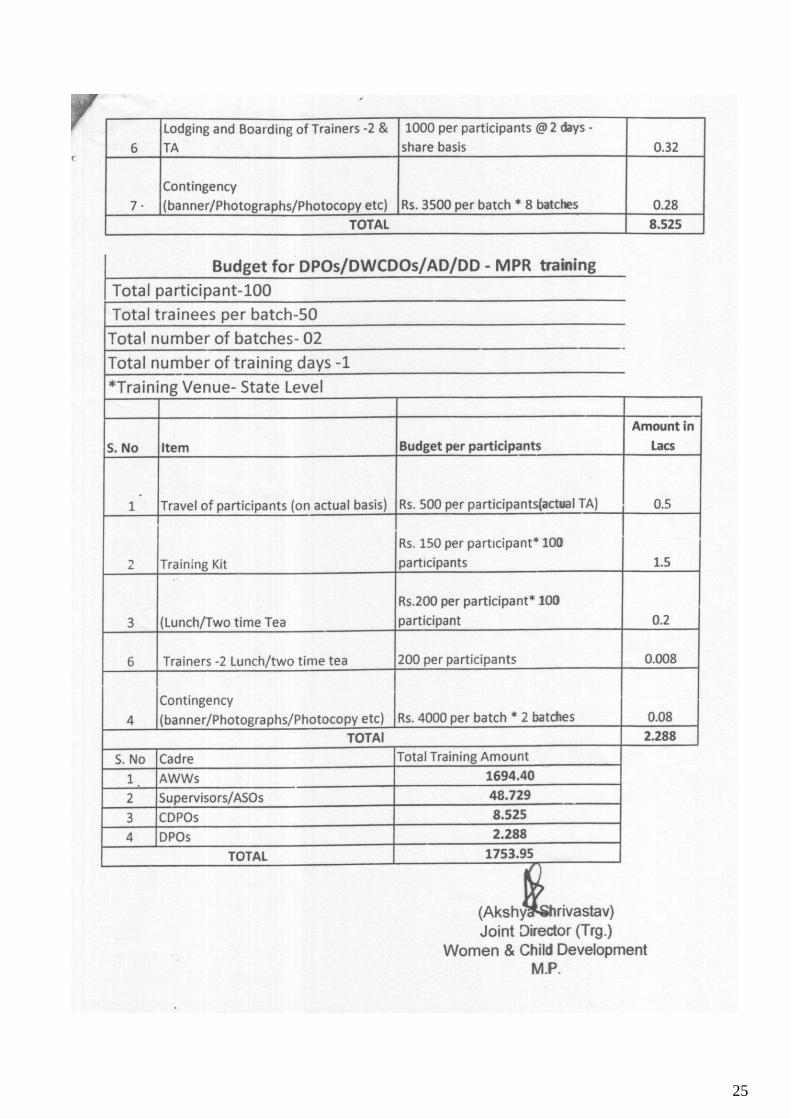
25