disaster nursing nclin 411 transition to professional practice
Post on 21-Dec-2015
214 views
TRANSCRIPT

Disaster NursingNClin 411
Transition to Professional Practice
Research Professor Schools of Nursing
and Public Health and Community Medicine
Randal Beaton, PhD, EMT
Faculty Northwest Center for
Public Health Practice University of Washington

Relevant Clinical Experience• Volunteer EMT
• Counseled victims of 9/11 who lostco-workers
• “Psychological casualties” of Nisqually earthquake (2001)
• Stress management for First Responders – mostly firefighters and paramedics – in private practice

Objectives
To differentiate between emergency and disaster nursing
To identify key skills sets needed to practice disaster nursing (safely and sanely)

To examine some psychosocial implications of chemical and bioterror threats and events
To analyze adaptive and maladaptive psychological and behavioral responses to disaster scenarios
The degree and effectiveness of preparedness often spell the
difference between emergency
and disaster.
Disaster Principles:

Emergency Nursing – (usually) involves the provision of nursing care for patient or patients with acute injuries or life threatening illnesses. (Usually) care is provided at ED, Urgent care, Trauma unit and/or ICU/CCU

Disaster Nursing – involves response to (and preparedness for) natural or man-made events that affect an entire community or communities. (Usually) involve massive numbers of casualties and extensive property damage.


Mental Health: Are we ready?

Ancient History
• Pre 9/11 – NBC = Nobody Cares
(http://www.leaveittobeaver.org/)
World Trade Center in the aftermath of the terrorist attacks on September 11, 2001,
Flight 175 Approachesthe WTC South Tower
911911
(© AP or Reuters from September 11, News.com)
Mind-set Circa March 2005
• Where are we now?• “Somewhere between mindless
complacency and all consuming paranoia.”• Dr. P. K. Carlton, Air Force General,
Retired, Texas A&M • (worked at the Pentagon on the morning of
September 11, 2001)
“You’re a target too!”“You’re a target too!”• First words uttered by a New Jersey nurse who
witnessed the 9/11 attacks and collapse of the WTC Towers
– when I told her “I’m from Seattle”
US Public Perspectives on the Mental Health Effects of
TerrorismDecember, 2003 (n = 750)
Major Findings:More than 90% of Americans agree that the
primary goal of a terrorist attack is to generate fear and distress.
Almost 90% agree that the threat of terrorism, in and of itself, creates public fear and distress.

2003 US Public Survey Findings (cont’d)
• More than 4 out of 5 (85%) of Americans say it is likely that the US will experience a terrorist attack in the near future.
• The single most important cause of terrorism-related anxiety was “fear of the unknown”.
Major Survey Findings (cont’d)
• More than 80% of Americans want federal programs to help them and their families to better cope with terrorist threats.
• A majority would like more than instructions to just “stay resolute”.
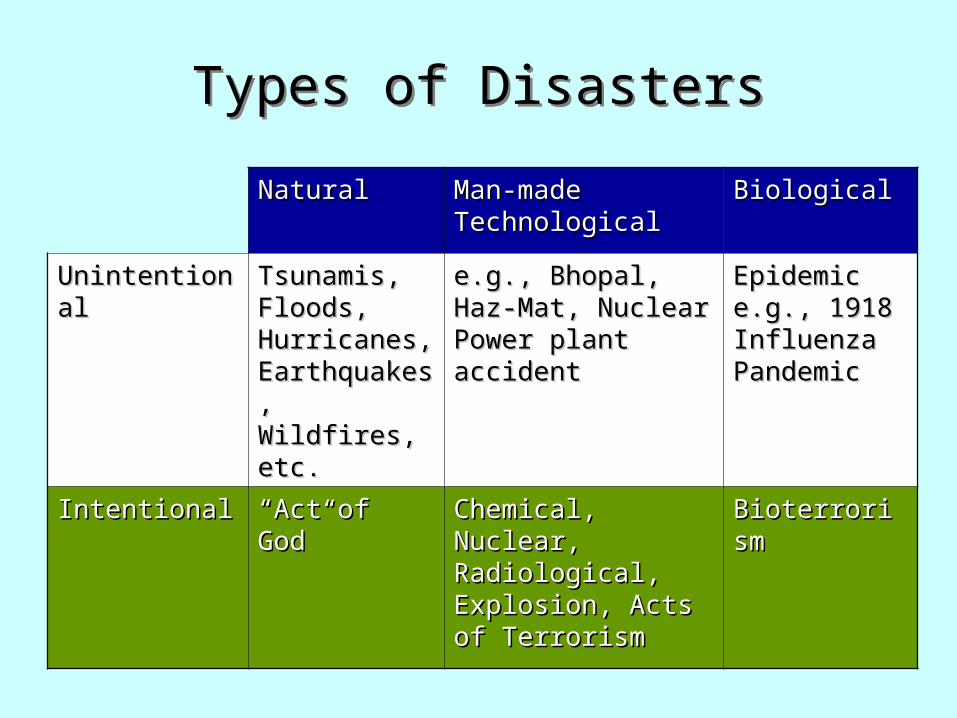
Types of DisastersTypes of Disasters
NaturalNatural Man-made Man-made TechnologicalTechnological
BiologicalBiological
UnintentionalUnintentional Tsunamis, Tsunamis, Floods, Floods, Hurricanes, Hurricanes, Earthquakes, Earthquakes, Wildfires, etc.Wildfires, etc.
e.g., Bhopal, Haz-Mat, e.g., Bhopal, Haz-Mat, Nuclear Power plant Nuclear Power plant accidentaccident
Epidemic e.g., Epidemic e.g., 1918 Influenza 1918 Influenza PandemicPandemic
IntentionalIntentional ““Act of God”Act of God” Chemical, Nuclear, Chemical, Nuclear, Radiological, Radiological, Explosion, Acts of Explosion, Acts of TerrorismTerrorism
BioterrorismBioterrorism
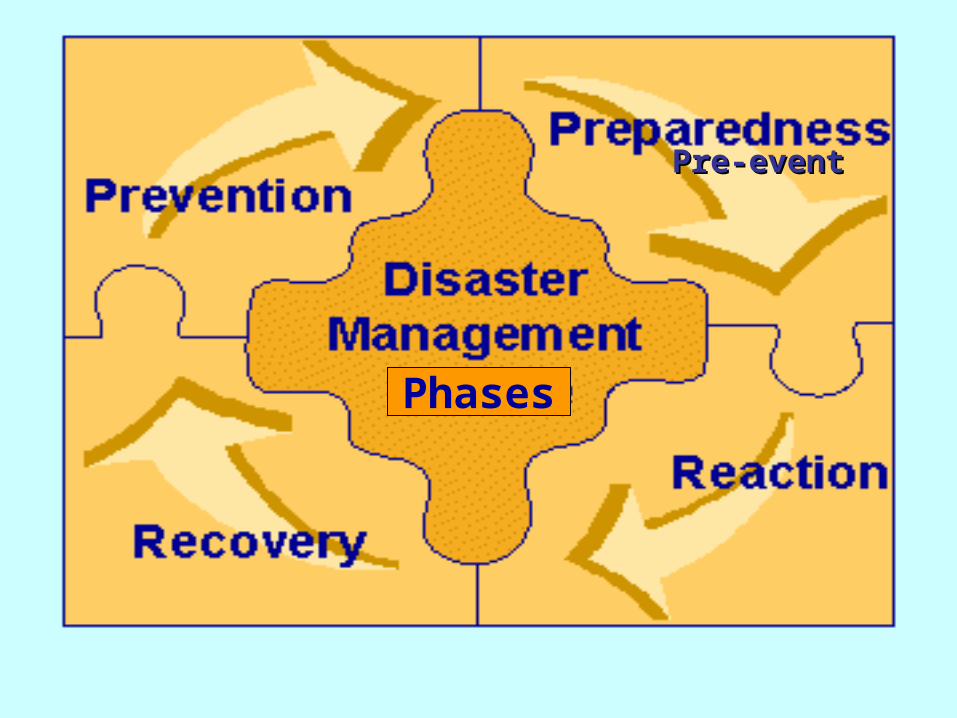
Phases
Pre-eventPre-event
The Aum Shinrikyo “Doomsday Cult”
Neurotoxin Attack on Tokyo Subway System AM Rush HourMarch 20, 1995

Sarin Gas Attack on Tokyo Subway highlights several
important issues!A covert attack may occur anywhere at
anytime.Generally, “worried well” outnumber
primary victims.“Walk-ins” and worried well may overwhelm
health care systems and providers.

TERRORIST THREATS AND ACTUAL TERRORIST EVENTS
Will have tremendous psychological and behavioral effects
May outweigh the direct impact of the chemical and biological events
Tend to completely ignore orAssume “the worst” – everyone will freak,
panic and the ensuing chaos will lead to breakdown of society

Panic Myth
True panic is relatively rare, preventable and largely circumstantial
Historically, people and communities respond cooperatively and adaptively in most natural and manmade disasters: e.g. evacuation of the WTC towers on 9/11/2001

Lessons from Influenza Pandemic of 1918 (from Barry, 2004)
Deadliest plague in historyHit the US hard 675,000 fatalitiesThough health care systems were strained,
widespread panic and the breakdown of social fabric did not occur
Lessons from 9/11
Resilience is commonOf those who exhibit acute
symptoms, most recover
Bonano, 2004

After Bonanno (2004)
0
10
20
30
40
50
60
70
80
90
100
Event
Dis
rup
tion
s
Resilience

After Bonanno (2004)
0
10
20
30
40
50
60
70
80
90
100
Event 2 Years
Dis
rup
tion
s ResilienceAcute/Recovery
FIRE FIGHTERS’ SECONDARY POSTTRAUMA SYMPTOMS
FOLLOWING 9/11
Randal D. Beaton, L. Clark Johnson, Shirley A. Murphy, and Marcus Nemuth (2004)
This project was supported by Grant R-18-OHO3559 from the National Institute for
Occupational Safety and Health of the Centers for Disease Control

Assumption
Terrorist attacks on the World Trade Center in NYC on Sept. 11, 2001 left 343 NYC fire fighters dead.
The assumption is that the “fire service family” is very close-knit.
The rationale for the current study is based on the hypothesis that secondary trauma was a potential outcome for fire fighters across the U.S.

The Current Study
Study participants were 261 urban fire fighters employed in a Pacific Northwest state.
Fortuitously, the respondents were participating in a NIOSH-funded longitudinal study and provided pre-9/11 and post-9/11 self-report data on PTSD, physiologic symptoms and coping.

Data Collection
Data were obtained from five “temporal groups”:
The day before 9/11, n = 241 or 2 days after 9/11, n = 52One week after 9/11, n = 93Two weeks after 9/11, n = 21One month after 9/11, n = 54

Impact of Events Total Score
5421935224N =
Time w/ reference to 9/11/01
1 mth After
2wk After
1wk After
1-2days After
Day Before
95
% C
I P
TS
D C
ase
Pre
vale
nce
.6
.5
.4
.3
.2
.1
0.0
-.1

So far the community outcome data from 9/11, the survivors of the Sarin Gas attack on the Tokyo Subway and other disasters are heartening and underline the resilient
nature of the human ‘spirit’ psyche.
Resilience is common and perhaps the norm Most survivors with acute distress adjust and
accommodate or recover within weeks or months Clinically significant chronic mental disorders affect a
minority of victims 10-30%

After Bonanno (2004)
0
10
20
30
40
50
60
70
80
90
100
Event 2 Years
Dis
rupt
ions
ResilienceAcute/RecoveryAcute/ChronicDelayedCyclic

Can emotional coping skills to deal with emergent disasters be taught? –
doubtful, but some hints.Stay focused on dutiesStay professionalSort out family/nurse roles/conflicts ahead
of timeDrill, drill, drillSelf-talk – should promote self-efficacyImportance of social support – especially in
aftermath

Psychological “First Aid”
Traumatic Incident Stress: Information for Emergency Workers:
NIOSH Guidelines
http://www.cdc.gov/niosh/unp-trinstrs.html

Scenario # 1
You are a nurse assisting with the mass dispensing of a life saving antibiotic/antidote following a chemical or biological terrorist attack. A patient who did not have a “credible exposure” is told that they will not receive the medication. They become hysterical and refuse to leave the dispensing site without this medication. Other patients waiting for their medication are starting to become more distressed and anxious watching this individual “lose it”.

Scenario # 2
The International Tsunami disaster of December 26, 2004 caused an enormous number of fatalities as well as large numbers of casualties and property damage in ten different national (representing even a greater number of distinct cultural groups and religious beliefs).

Scenario # 3
Senator Bill Frist, MD has recommended in his 2002 text When Every Moment Counts that all American’s disaster supply kits should now also include N95 respirators for each family member (A N95 mask only filters out 95% of the microscopic - .3 micron – sodium chloride particles in NIOSH tests.)

Scenario # 4
As a volunteer nurse working with the Red Cross, you are dispatched to a southern state to work in a shelter with community residents displaced following a series of hurricanes. What are some of the psychosocial issues that might arise for the following vulnerable populations and what are some potential remedies? Psychological triage: Who is your first priority?