disclosures code sepsis (not now…maybe later) · •equivocal cvl use ... –within 6 hours from...
TRANSCRIPT

5/31/2014
1
CODE SEPSIS (not now…maybe later)
David Shimabukuro, MDCM Associate Professor
Medical Director, 13 ICU Physician Lead, UCSF DSRIP Sepsis Project
Disclosures
• I have no disclosures
Agenda
• Epidemiology
• The “Surviving Sepsis Campaign Bundles”
• The UCSF Experience
• Future considerations
Agenda
• Epidemiology
• The “Surviving Sepsis Campaign Bundles”
• The UCSF Experience
• Future considerations
5/31/2014
2
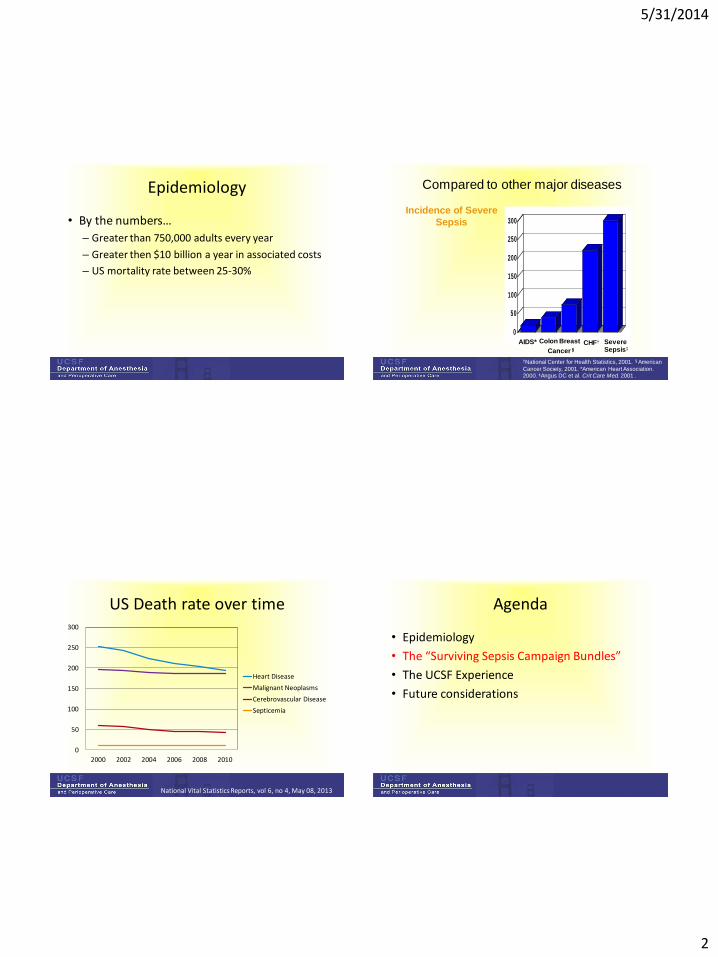
Epidemiology
• By the numbers…
– Greater than 750,000 adults every year
– Greater then $10 billion a year in associated costs
– US mortality rate between 25-30%
Compared to other major diseases
†National Center for Health Statistics, 2001. §American
Cancer Society, 2001. *American Heart Association. 2000. ‡Angus DC et al. Crit Care Med. 2001 .
0
50
100
150
200
250
300
AIDS* Colon Breast
Cancer§
CHF† Severe Sepsis‡
Ca
se
s/1
00
,000
Incidence of Severe
Sepsis
US Death rate over time
0
50
100
150
200
250
300
2000 2002 2004 2006 2008 2010
Heart Disease
Malignant Neoplasms
Cerebrovascular Disease
Septicemia
National Vital Statistics Reports, vol 6, no 4, May 08, 2013
Agenda
• Epidemiology
• The “Surviving Sepsis Campaign Bundles”
• The UCSF Experience
• Future considerations

5/31/2014
3
What is Sepsis??
• A variable condition that affects each of us differently and is initiated by an infectious insult.
• Involves the systemic activation of the inflammatory response and an unbalancing of the coagulation cascade
Septic Shock
SEVERE SEPSIS plus hypotension (Systolic
blood pressure < 90 or Mean Arterial Blood Pressure < 65) OR
Lactate > 4
Severe Sepsis
SEPSIS plus evidence
of at least one alteration in organ
perfusion
Sepsis
SIRS plus confirmed
or suspected infection
Sepsis: ACCP/SCCM Definitions
SIRS
T > 38.3 C or < 36 C
HR > 90 beats/min Tachypnea
WBC > 12K or < 4K
Severe Sepsis Definition
Crit Care Med February 2013 Volume 41 Number 2 pp. 580-637
Management of Severe Sepsis and Septic Shock
Crit Care Med February 2013 Volume 41 Number 2 pp. 580-637
5/31/2014
4
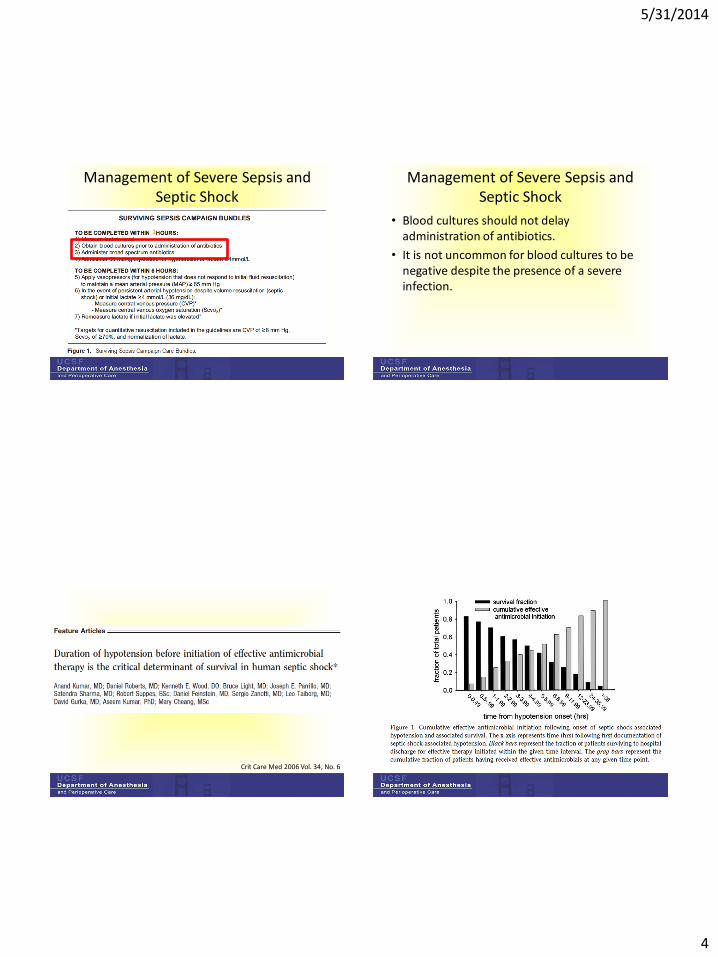
Management of Severe Sepsis and Septic Shock
1
Management of Severe Sepsis and Septic Shock
• Blood cultures should not delay administration of antibiotics.
• It is not uncommon for blood cultures to be negative despite the presence of a severe infection.
Crit Care Med 2006 Vol. 34, No. 6
5/31/2014
5
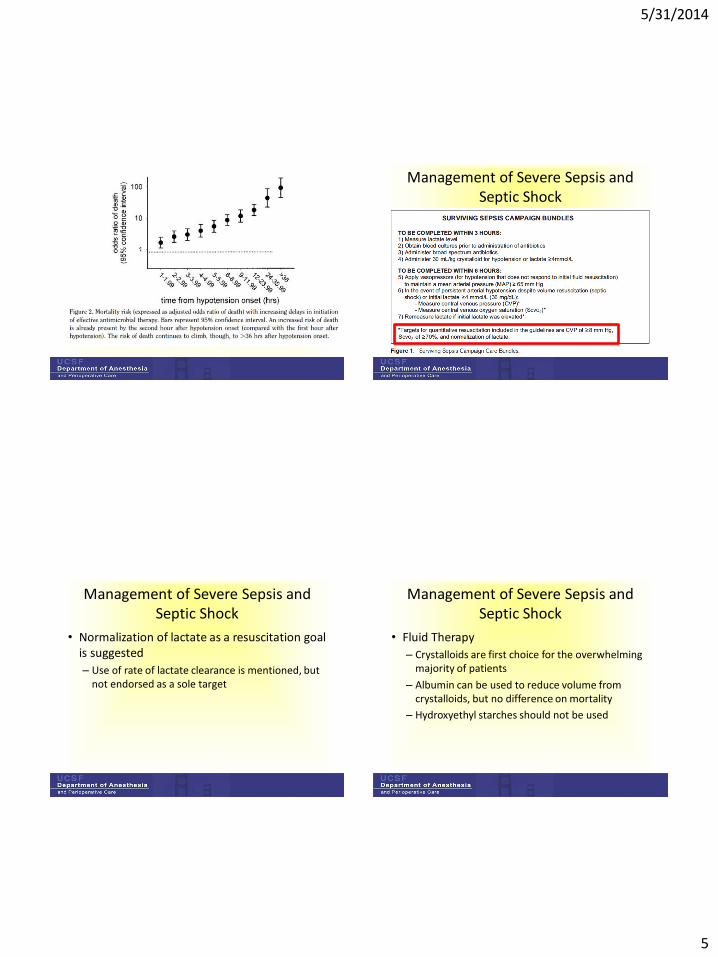
Management of Severe Sepsis and Septic Shock
Management of Severe Sepsis and Septic Shock
• Normalization of lactate as a resuscitation goal is suggested
– Use of rate of lactate clearance is mentioned, but not endorsed as a sole target
Management of Severe Sepsis and Septic Shock
• Fluid Therapy
– Crystalloids are first choice for the overwhelming majority of patients
– Albumin can be used to reduce volume from crystalloids, but no difference on mortality
– Hydroxyethyl starches should not be used
5/31/2014
6
Management of Severe Sepsis and Septic Shock
Management of Severe Sepsis and Septic Shock
• Corticosteroids
– For refractory hypotension despite fluids and vasopressors/inotropes
– Do not perform ACTH stimulation test
• Glucose
– Target level to less than 180 mg/dL
Management of Severe Sepsis and Septic Shock
• Blood Products
– HGB level 7.0 – 9.0 g/dL after hypoperfusion has resolved
– FFP not to be used unless bleeding is present or for planned invasive procedure
– PLT to be given prophylactically when <10K in absence of bleeding
Management of Severe Sepsis and Septic Shock
• More recommendations…refer to original paper
5/31/2014
7
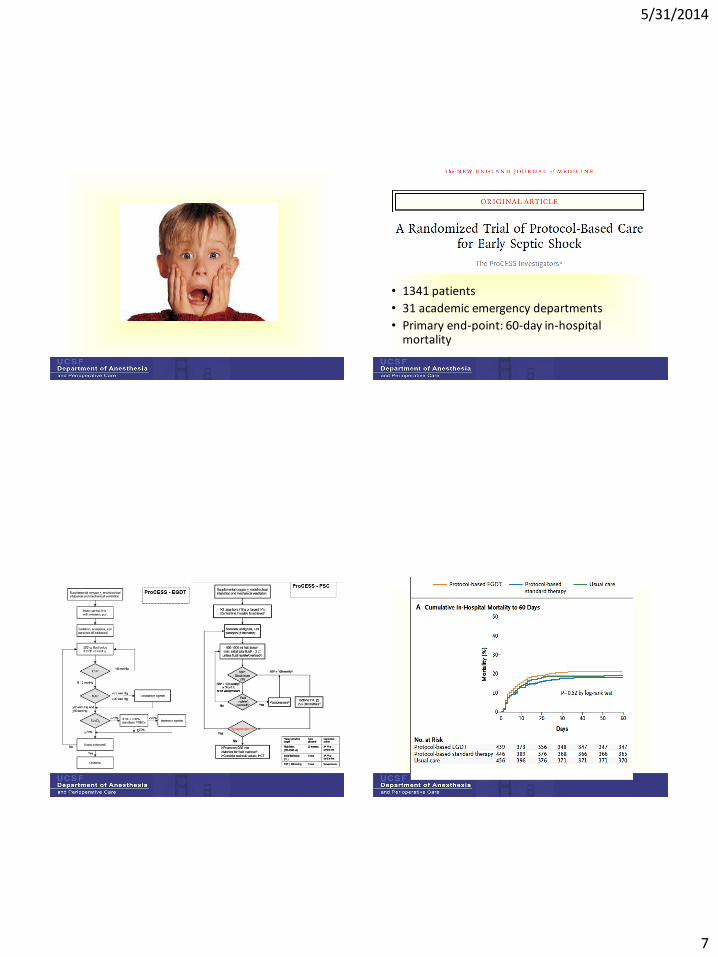
• 1341 patients
• 31 academic emergency departments
• Primary end-point: 60-day in-hospital mortality

5/31/2014
8
Major criticisms
• Academic centers
• “usual care” not defined
• Equivocal CVL use
• Antibiotic time
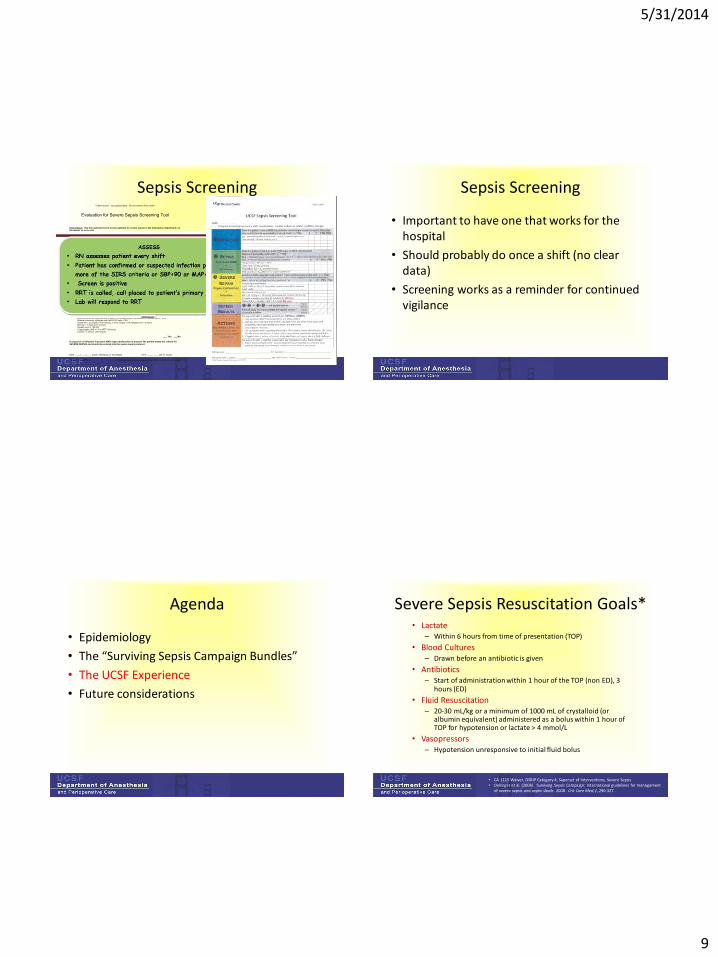
Sepsis Screening
Crit Care Med February 2013 Volume 41 Number 2 pp. 580-637
Great….but when should we do it and how should it be done!!!!
Sepsis Screening
5/31/2014
9
Sepsis Screening Sepsis Screening
• Important to have one that works for the hospital
• Should probably do once a shift (no clear data)
• Screening works as a reminder for continued vigilance
Agenda
• Epidemiology
• The “Surviving Sepsis Campaign Bundles”
• The UCSF Experience
• Future considerations
Severe Sepsis Resuscitation Goals* • Lactate
– Within 6 hours from time of presentation (TOP)
• Blood Cultures – Drawn before an antibiotic is given
• Antibiotics – Start of administration within 1 hour of the TOP (non ED), 3
hours (ED)
• Fluid Resuscitation – 20-30 mL/kg or a minimum of 1000 mL of crystalloid (or
albumin equivalent) administered as a bolus within 1 hour of TOP for hypotension or lactate > 4 mmol/L
• Vasopressors – Hypotension unresponsive to initial fluid bolus
• CA 1115 Waiver, DSRIP Category 4, Superset of Interventions, Severe Sepsis • Dellinger et al. (2008). Surviving Sepsis Campaign: International guidelines for management
of severe sepsis and septic shock: 2008. Crit Care Med,1, 296-327.
5/31/2014
10
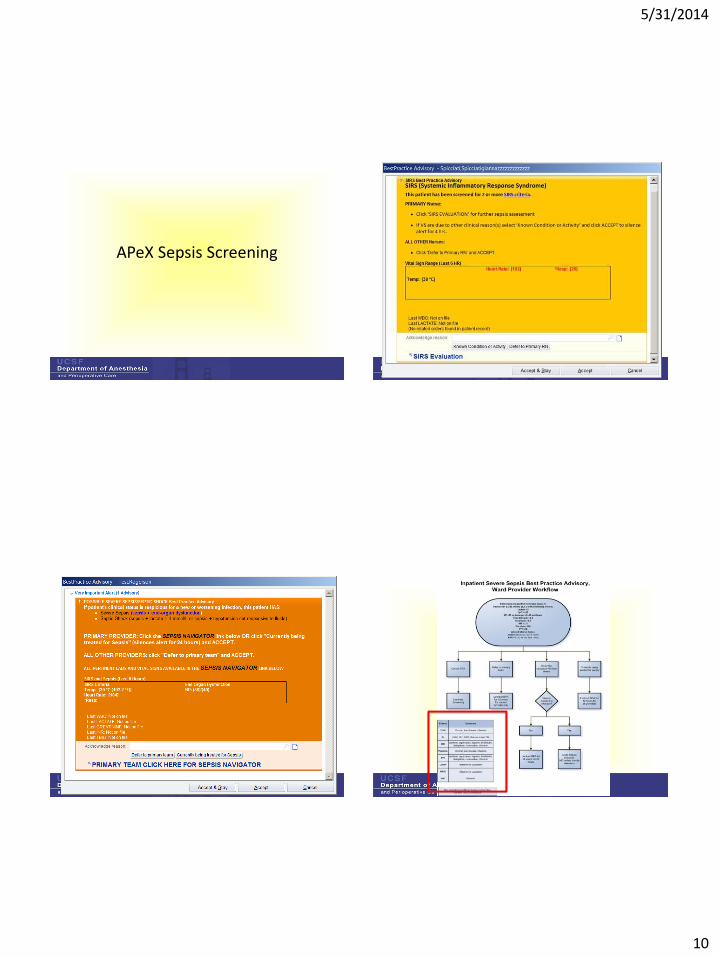
APeX Sepsis Screening

5/31/2014
11
9 ICU severe sepsis BPA analysis
33 patients total Patients with
Severe Sepsis = 15 Patients without
Severe Sepsis = 18
BPA Triggered 18 patients
True Positive (TP) = 13
False Positive (FP) = 5
Positive Predictive Value TP/ (TP+FP) = 72%
No BPA Triggered
15 Patients
False Negative (FN) = 2
True Negative (TN) = 13
Negative Predictive Value
TN / (FN+TN) = 87%
Sensitivity
TP/ (TP+FN) = 87 % Specificity
TN/ (FP+TN) = 72%
41
14 M BPA Analysis
42
73 patients total Patients with
severe sepsis = 13 Patients without
severe sepsis = 60*
BPA triggered 21 patients
True Positive (TP) = 13
False Positive (FP) = 8
Positive Predictive Value TP/ (TP+FP) = 62%
No BPA triggered 52 patients
False Negative (FN) = 0*
True Negative (TN) = 52*
Negative Predictive Value TN / (FN+TN) = 100%
Sensitivity
TP/ (TP+FN) = 100 % Specificity
TN/ (FP+TN) = 87%
Code Sepsis
What is a Code Sepsis?
– A silent alert sent by pager to a designated team that includes a Pharmacist, the RRT and the ICU Fellow
– Purpose is to expedite severe sepsis resuscitation
How is a Code Sepsis Activated?
– Sepsis Navigator via the Severe Sepsis BPA
– Pagerbox
Roles and Responsibilities
• Bedside RN
– Activates Code Sepsis & notifies Primary Team
– Presents patient conditions
– Assists with sepsis resuscitation
• Primary Team
– Responds to patient’s bedside
– Collaborate on treatment decisions
– Write orders as needed

5/31/2014
12
Roles and Responsibilities • RRT
– Validate positive screen
– Support timely blood culture collection and administration of antibiotics and fluids
– Maintain time to assure resuscitation in 60 minutes
• Pharmacist – Facilitate verification, dispensing & delivery of antibiotics
– Follow-up with primary team for subsequent dosing
• ICU Fellow – Assist with selection/ordering of antibiotics, fluids, vasopressors
– Assist with blood culture collection as needed
– Assist with determining level of care
Our data
UCSF Sepsis Bundle Compliance
Sepsis Bundle Compliance
22%
4%0%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Lactate BCx BSA Fluids Full Bundle Compliance
ED
Acute Care
ICU
14% Overall
Date of download: 8/27/2012
Copyright © American College of Chest Physicians. All rights reserved.
From: Nationwide Trends of Severe Sepsis in the 21st Century (2000-2007)National Trends of Severe Sepsis in
21st Century
CHEST. 2011;140(5):1223-1231. doi:10.1378/chest.11-0352
Frequency of admission and mortality rates due to severe sepsis, 2000-2007. Bars represent SEM.
Figure Legend:
5/31/2014
13
Agenda
• Epidemiology
• The “Surviving Sepsis Campaign Bundles”
• The UCSF Experience
• Future considerations
50
New York Times, July 11, 2012
Future Considerations
• State mandates
– New York
– California: DSRIP
• NQF
• CMS
– TJC
– Leapfrog
Summary
• A very heterogeneous disease that is difficult to diagnose in its early stages and difficult to treat in its later stages.
• Routine screening can allow for earlier identification
• Early intervention can attenuate its course, but the mainstay of treatment is supportive care.

5/31/2014
14
ORGAN DYSFUNCTION EXAMPLES:
Lactate > 2 mmol/L
Neuro: Encephalopathy,focal neurologic deficits,altered mental status
Pulm: Increased oxygenrequirement to maintainbaseline Sp02
Renal: Acute kidney injury; urine output < 30 cc/hr X2 hours; Cr > 2 mg/dL
GI: Bilirubin > 2 mg/dL
Heme: Platelet count < 100 K, INR > 1.5 or PTT > 60 secs
CV: SBP < 90 or > 40 below baseline, or MAP < 65
Sepsis Screeningand Treatment Tool
≥ 2 SIRS OR
Confirmed/SuspectedInfection
≥ 2 SIRS+
Infection
YES
NEW onsetorgan
dysfunction?
Hypotensionrefractory to
fluid boluses?
Treat for SEPTIC SHOCK
YES
Treat for SEVERE SEPSIS
Treat for SEPSISConsider SEVERE SEPSIS
InfectionOnly
If the patient screens negative, and you suspect
sepsis, then TREAT FOR SEPSIS.
START
See Next Page for Treatment Recommendations