disclosures sonographic cervical length for the prediction...
TRANSCRIPT

1
Sonographic Cervical Length for
the Prediction of Preterm Birth:
Standardization of the Technique
and Pitfalls
Sonia S. Hassan, M.D.
Edgar Hernandez Andrade, M.D.
Roberto Romero, M.D., D.Med.Sci. Wayne State University
Perinatology Research Branch, NICHD/NIH/DHHS
Disclosures
Presenter Name: Sonia S. Hassan, M.D.
Relevant Financial Relationships: None
Hassan, Hernandez, Romero
Learning Objectives
After completing the presentation, learners will be able to discuss:
1. The definition of a sonographic short cervix
2. The gestational age at which a cervix should be examined
3. Additional ultrasound parameters to assess preterm birth risk
4. The correct technique for the measurement of cervical length
in pregnancy
5. Amniotic Fluid sludge
6. Treatments for a sonographic short cervix
7. Future methods to assess the cervix in pregnancy
Hassan, Hernandez, Romero
Lecture Outline• The definition of a sonographic short cervix
• Gestational age at which a cervix should be examined
• Additional ultrasound parameters to assess the risk of
preterm birth
– Cervical Funnel
– Dynamic Change
– Amniotic Fluid Sludge
• The correct technique and pitfalls for the measurement of
cervical length in pregnancy
• Interventions to prevent preterm birth in women with a
sonographic short cervix
• Future methods to assess the cervix in pregnancy Hassan, Hernandez, Romero
Detroit Medical Center/Photo taken at Hutzel Women’s Hospital, copyright cannot be transferred
Preterm Birth is the Leading
Cause of Infant Mortality
Hassan, Hernandez, Romero
Preterm Birth Results in…
• Respiratory distress syndrome
• Chronic lung disease
• Bowel injury/inflammation
• Long-term mental disabilities
• Cerebral palsy
Bull World Health Organ 2010;88:31-38Hassan, Hernandez, Romero

2
Yoon B.H. and Romero R; Seoul National University
Hassan, Hernandez, Romero
Magnitude of the Problem
• ~ 13 million preterm births
worldwide
• 500,000 in the United States
• Highest rates: Africa and North
America
Bull World Health Organ 2010;88:31-38Hassan, Hernandez, Romero
Preterm Birth Rate in the US
1990-2008
CDC/NCHS, National Vital Statistics, NCHS Data Brief Number 39, May 2010
10
2
0
12
14
8
4
6
1990 1998 2000 2002 2004 2006 2008199619941992
Preterm (<37 weeks)
Late preterm (34-36 weeks)
Early preterm (<34 weeks)
Year
Perc
en
t
Hassan, Hernandez, Romero
The Annual Societal Economic
Burden Associated with
Preterm Birth in the United
States
In excess of $26.2 billion in 2005
Institute of Medicine (US) Committee on Understanding Premature Birth and Assuring
Healthy Outcomes; Behrman RE, Butler AS, editors. Preterm Birth: Causes,
Consequences, and Prevention. Washington (DC): National Academies Press (US); 2007
Hassan, Hernandez, Romero
Epithelium
OsE
Stroma
Cervix
Extra cellularmatrix
E
M
Extra cellularmatrix
Labor
Common Pathway of Parturition
Myometriuma
Low connectivity
Connexin 43
SmoothMuscle cell
High connectivity
miR-200
Connexin 43
Labor
P4
Contraction–associated Proteins
Decidua
Labor
Adapted from Romero R, Dey SK, Fisher SJ, Science 2014; 345:760Hassan, Hernandez, Romero
Stages of Cervical Function During
Pregnancy and the Puerperium
Weeks gestation
0 8 16 24 32 40
10
8
6
4
2
0
Word RA. Semin Reprod Med 2007-25-69
SofteningRipening
Dilation
Repair
Ultrasound
assessment
Hassan, Hernandez, Romero

3
Cervical glands
Perinatology Research Branch, NICHD/NIH, Wayne State University
Sonographic Cervical Length
Hassan, Hernandez, Romero
Risk for Spontaneous Delivery at <32 Weeks According to
Cervical Length at 23 Weeks of Gestation
Heath VCF et al. Ultrasound Obstet Gynecol 1998;12:301-3.
0 10 20 30 40 50 60 70
Cervical length (mm)
0
20
40
60
80
100
Ris
k (
%)
Spontaneous Preterm Delivery Before 35 Weeks Based on
Cervical Length at 24 Weeks Measured by Ultrasound
!0 1220 40 60 80
0
0.1
0.2
0.3
0.4
0.5
Pro
bab
ilit
yo
fp
rete
rmd
elivery
Estimated probability of spontaneous
delivery before 35 weeks
Observed frequency of spontaneous
preterm delivery according to cervical
length
Iams J et al. NEJM 1996;334:567-72.
Cervical length (mm)
Risk of Spontaneous Preterm Delivery at 32 Weeks Among
Women with Measured Cervical Length Between 14-24 Weeks
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80
Cervical length
Perc
en
t ri
sk
Hassan SS et al. AJOG 2000;182:1458
Cervical length (mm)
Hassan, Hernandez, Romero
Anderson F et al. AJOG;1990:163-859
Logistic Regression Analysis of Risk of Preterm Delivery by
Cervical Length Measured by Endovaginal Ultrasonography
20 30 40 50 60 70
Vaginal Ultrasound Cervical length (mm)
0
20
30
40
50
60
Ris
k o
f P
rete
rm D
eli
ve
ry (%
)
Risk =1/(1+e (-3.31-0.13xVAGCX))
Actual PTD
Predicted Risk
A Short Cervix is the Most Powerful Predictor of
Spontaneous Preterm Birth
11mm
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
What is a Short
Cervix?
Hassan, Hernandez, Romero
Low risk
Prior preterm birth
Twins
Triplets
15 mm
25 mm
25 mm
25 mm
Definition of a Short Cervix
50% Risk for Spontaneous Preterm Delivery
< 32 - 33 weeks
Hassan, Hernandez, Romero
Cervical Length
Cervical Length 11 mm
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero

4
Low risk
Prior preterm birth
Twins
Triplets
15 mm
25 mm
25 mm
25 mm
Definition of Short Cervix
50% Risk for Spontaneous Preterm Delivery
< 32 - 33 weeks
Hassan, Hernandez, Romero
Cervical Length 22 mm
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Low risk
Prior preterm birth
Twins
Triplets
15 mm
25 mm
25 mm
25 mm
Definition of Short Cervix
50% Risk for Spontaneous Preterm Delivery
< 32 - 33 weeks
Hassan, Hernandez, Romero
Short Cervix
Congenital
(DES exposure)
Surgical
(conization)
Infection
Acute Cervical
insufficiency’
Romero R, Espinoza J, Erez O, Hassan S, Am J Obstet Gynecol. 2006 Jan; 194(1):1-9
Extracellular
matrix changesProgesterone
deficiency
Hassan, Hernandez, Romero
Intra-amniotic
infection
9%
Intra-amniotic
inflammation
22%
Hassan S, Romero R, Hendler I et al. J Perinat Med 2006;34(1):13-9
Vaisbuch E, Romero R, Erez O, et al. Ultrasound Obstet Gynecol. 2010 Oct;36(4):471-81
Frequency of Intra-amniotic Inflammation and Intra-
amniotic Infection in Patients with a Short Cervix
Hassan, Hernandez, Romero
What Gestational Age
Should the Cervix be
Examined?
Hassan, Hernandez, Romero

5
Isthmus
Cervix
First Trimester Assessment of the
Uterine Cervix
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Isthmus
Cervix
Perinatology Research Branch, NICHD/NIH, Wayne State University
First Trimester Assessment of the
Uterine Cervix
Hassan, Hernandez, Romero
Isthmus
Cervix
First Trimester Assessment of the
Uterine Cervix
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
0 10 20 30 40 50 60 70 80
Cervical length (mm)
0
0.05
0.1
0.15
0.2
0.25P
rob
ab
ilit
y
> 19-24 weeks
14-19 weeks
Hassan S, Romero R, Berry S,et al. AJOG 2000;182:1458
Probability of Preterm Delivery <32 Weeks According
to the GA at which the US was Preformed
Hassan S, Romero R, Berry S, Dang K, Blackwell SC, Treadwell MC, Wolfe HM. AJOG 2000;182:1458
Hassan, Hernandez, Romero
Additional Parameters Used
to Assess the Risk of
Preterm Birth During
Transvaginal Sonography
Hassan, Hernandez, Romero
• Cervical funnel
• Dynamic change
• Amniotic fluid sludge
Are There Additional Parameters to Assess
the Risk of Preterm Birth During
Transvaginal Sonography?
Hassan, Hernandez, Romero

6
Funnel
Shoulder of funnel
Shoulder of funnel
Perinatology Research Branch, NICHD/NIH
Wayne State University
Hassan, Hernandez, Romero
Shoulder of funnel
Funnel length
Cervix
Funnel
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Dynamic Change
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Funneling and Dynamic Change Have
no Independent Predictive Value for
Preterm Delivery After Cervical Length
is Considered
To MS et al, Ultrasound Obstet Gynecol. 2001 Sep;18(3):200-3
Owen J et al, JAMA. 2001 Sep; 286(11):1340-8
Hassan, Hernandez, Romero
How Should the Cervix be
Examined?
Techniques and Pitfalls
Hassan, Hernandez, Romero
Normal Cervical Anatomy
Hassan, Hernandez, Romero

7
Internal
Cx Os
External
Cx Os
Canal Length
Funnel
Width
Funnel
Length
Canal
Length
Gomez R, Galasso M, Romero R, et al. Am J Obstet Gynecol 1994;171(4):956-64
Hassan, Hernandez, Romero
Shoulder of funnel Funnel length
Cervix
Cervical Length is the Most Important Measurement
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
• Transabdominal
• Transperineal
• Transvaginal
Methods of Sonographic
Examination of the Uterine Cervix
in Pregnancy
Hassan, Hernandez, Romero
• Transabdominal examination requires a
full bladder
• Transabdominal cervical length is longer
than transvaginal cervical length in the
same patient
• Mean difference 5.2 mm (+/-14.3, p<0.001)
Transabdominal versus
Transvaginal Sonographic
Evaluation of the Cervix
Andersen HF, J Clin Ultrasound. 1992 Feb; 19(2):77-83Hassan, Hernandez, Romero
Transabdominal Cervical Length
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Transabdominal Cervical Length
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero

8
• Developed before transvaginal transducers
were available
• Should avoid pelvic examination before the
scan
• Allows visualization of the cervix, but it is more
difficult to interpret
Transperineal versus Transvaginal
Sonographic Evaluation of the Cervix
Hassan, Hernandez, Romero Meijer-Hoogeveen M et al. Ultrasound Obstet Gynecol 2008;32:657-62Hassan, Hernandez, Romero
• Strong correlation with transvaginal
measurements
• Failure to obtain a clear image
– 30% of mid-trimester pregnancies
– 19% of third-trimester cases
• Landmarks can be obscured by bowel gas
Transperineal Sonographic
Evaluation of the Cervix
Meijer-Hoogeveen M et al. Ultrasound Obstet Gynecol 2008;32:657-62Hassan, Hernandez, Romero
• Objective
• Reproducible
• Reliable
• Minimal discomfort
Transvaginal Sonographic
Evaluation of the Cervix
Andersen et al 1990, Am J Obstet Gynecol. 1990;163:859-67
Gomez R et al, Am J Obstet Gynecol. 1994 Oct; 171(4):956-64 Hassan, Hernandez, Romero
• Transvaginal ultrasound
• Empty bladder
• Sagittal view identified
Measurement of Sonographic
Cervical Length
Hassan, Hernandez, Romero
Endocervical Canal
External
Os
External
Os
Internal
Os
External
Os
Internal
Os
Endocervical Canal
Measurement of Sonographic Cervical
Length
Gomez R, Galasso M, Romero R, et al. Am J Obstet Gynecol 1994;171(4):956-64Hassan, Hernandez, Romero

9
1) Flat internal os or isosceles triangle
2) Observe entire length of canal
3) Symmetric image of external os
4) Equal size and density of the
anterior and posterior lips of the
cervix
Recommendations for Standardization of
Cervical Examination with Ultrasound
Burger M et al, Ultrasound Obstet Gynecol. 1997 Mar; 9(3):188-93
12
3
4
42
Hassan, Hernandez, Romero
• Three measurements – shortest length
recorded
• Examine for three minutes at minimum
• Recognition of sludge
Measurement of Sonographic
Cervical Length
Hassan, Hernandez, Romero
Full bladder
Cervical length 35 mm
Empty bladder
Cervical length 17 mm
Bladder
Avoid the Presence of a Full Bladder
B
B = bladder F = fetal head
F
F
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Avoid Excess Probe Pressure
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Avoid Unequal Distance and Density
of Anterior and Posterior Cervical Lips
Unequal
Distance
Unequal
Density
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Avoid Poor Visualization of the
Endocervical Canal
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
10
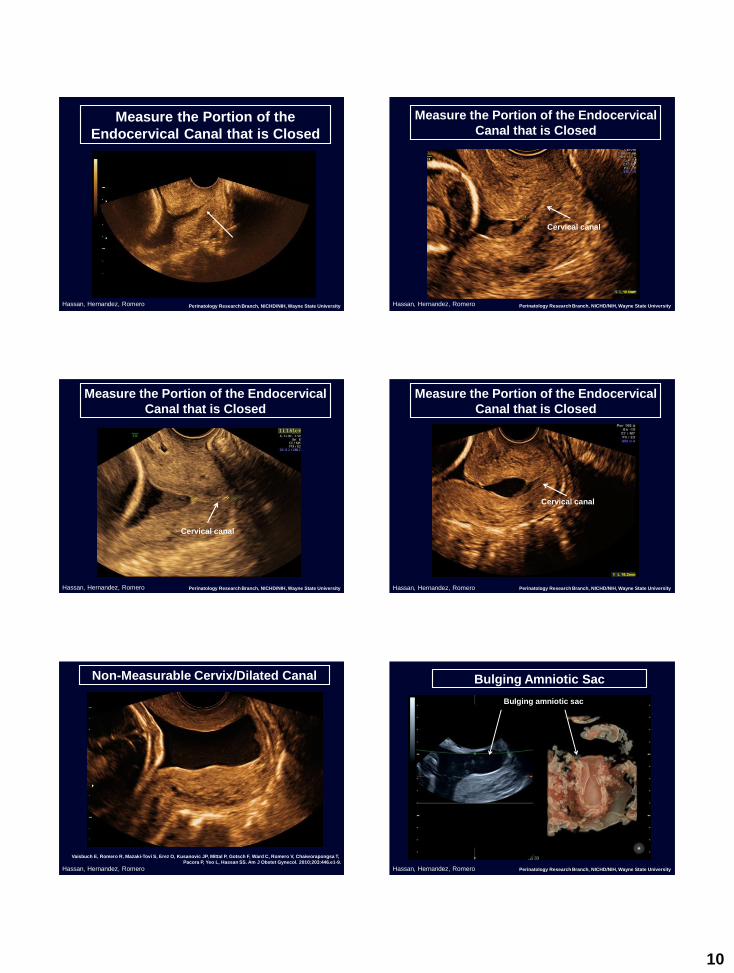
Measure the Portion of the
Endocervical Canal that is Closed
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Measure the Portion of the Endocervical
Canal that is Closed
Perinatology Research Branch, NICHD/NIH, Wayne State University
Cervical canal
Hassan, Hernandez, Romero
Cervical canal
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Measure the Portion of the Endocervical
Canal that is Closed
Measure the Portion of the Endocervical
Canal that is Closed
Perinatology Research Branch, NICHD/NIH, Wayne State University
Cervical canal
Hassan, Hernandez, Romero
Non-Measurable Cervix/Dilated Canal
Vaisbuch E, Romero R, Mazaki-Tovi S, Erez O, Kusanovic JP, Mittal P, Gotsch F, Ward C, Romero V, Chaiworapongsa T,
Pacora P, Yeo L, Hassan SS. Am J Obstet Gynecol. 2010;203:446.e1-9.
Hassan, Hernandez, Romero
Bulging amniotic sac
Bulging Amniotic Sac
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero

11
© Pat Schoff Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Cervical canalSludge
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
• Presence of dense aggregates of particulate
matter in close proximity to the internal
cervical os
Espinoza J. et al Ultrasound Obstet Gynecol 2005;25:346-52
Kusanovic JP. et al Ultrasound Obstet Gynecol 2007;30:706-714
Amniotic Fluid “Sludge”
Hassan, Hernandez, Romero
Sludge in Asymptomatic Patients at Risk
(Previous History)
• 17 % positive AF cultures vs. 0% (no sludge)
• 63% Histological chorioamnionitis
• 15% Clinical chorioamnionitis vs. 5%
• 60% spontaneous PTB (<32 wks) vs. 15%
• 37% neonates admitted to NICU vs. 16%
Kusanovic JP et al. Ultrasound Obstet Gynecol 2007;30:706-14Hassan, Hernandez, Romero
40
30
20
10
0
Frequency
<15 mm
71
Cervical length
Presence
Absence
60
50
29
50
12
15-25 mm
70
80
Frequency of Spontaneous Preterm Delivery at
<32 Weeks of Gestation According to Cervical Length
and Presence or Absence of Amniotic Fluid "Sludge”
14-24 weeks
Kusanovic JP et al. Ultrasound Obstet Gynecol 2007;30:706-14Hassan, Hernandez, Romero
Amniotic Fluid “Sludge”
Increases the predictive
value for preterm delivery
Hassan, Hernandez, Romero

12
Sludge
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero Perinatology Research Branch, NICHD/NIH, Wayne State University
Sludge
Hassan, Hernandez, Romero
Sludge
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Sludge
Amniotic Fluid “Sludge”
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
What is Sludge?
Hassan, Hernandez, Romero
Amniotic Fluid “Sludge”
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero

13
Amniotic Fluid “sludge” Sample
Romero R, Schaudinn C, Kusanovic JP, Gorur A, Gotsch F, Webster P, Nhan-Chang CL, Erez O, Kim CJ, Espinoza J,
Gonçalves LF, Vaisbuch E, Mazaki-Tovi S, Hassan SS, Costerton JW Am J Obstet Gynecol 2008;198:135.e1-5
Mycoplasma hominis,
Streptococcus mutans,
Aspergillus flavus
Hassan, Hernandez, Romero
Amniotic Fluid “sludge” Sample
Romero R, Schaudinn C, Kusanovic JP, Gorur A, Gotsch F, Webster P, Nhan-Chang CL, Erez O, Kim CJ, Espinoza J,
Gonçalves LF, Vaisbuch E, Mazaki-Tovi S, Hassan SS, Costerton JW Am J Obstet Gynecol 2008;198:135.e1-5
Mycoplasma hominis,
Streptococcus mutans,
Aspergillus flavus
Hassan, Hernandez, Romero
Romero R et al. Cover AJOG January 2008
Scanning Electron Microscopy
Biofilm:
Bacterial Cells and Exopolymeric Matrix Material
Hassan, Hernandez, Romero
Prediction
Prevention
?
Hassan, Hernandez, Romero
Treatments for a
Sonographic Short
Cervix
Hassan, Hernandez, Romero
Interventions to Prevent Preterm Birth
in Women with a short cervix
O
C
CH3
O
ProgesteroneCerclage
www.dr-arabin.de
Pessary
Hassan, Hernandez, Romero

14
Fonseca EB et al. NEJM 2007;357:462-9
Hassan SS, et al. Ultrasound Obstet Gynecol. 2011 Jul;38(1):18-31Hassan, Hernandez, Romero
Romero R, Nicolaides K, Conde-Agudelo A, Tabor A, O'Brien JM, Cetingoz E, Da Fonseca E, Creasy GW, Klein
K, Rode L, Soma-Pillay P, Fusey S, Cam C, Alfirevic Z, Hassan SS; Am J Obstet Gynecol. Feb 2012
Hassan, Hernandez, Romero
Effect of Vaginal Progesterone on the Rate
of Preterm Birth
34
28
24
20
16
12
8
4
0
<32 <33<30<28 <34
5%
11%
13%
7%
18%
10%
22%
12%
27%
16%
Weeks gestation
Perc
en
tag
e o
f p
rete
rm b
irth
Progesterone
Placebo
Romero R, Nicolaides K, Conde-Agudelo A, Tabor A, O’Brien J, Cetingoz E, DA Fonseca E,
Creasy G, Klein K, Rode L, Soma-Pillay P, Fusey S, Cam C, Alfirevic Z, Hassan S. Am J Obstet Gynecol 2011;12:003
50%
39%
42%
42%
42%
<35
30%
20%
31%ALL STATISTICALLY SIGNIFICANT
Hassan, Hernandez, Romero
Effect of Vaginal Progesterone on Neonatal
Outcomes
28
24
20
16
12
8
4
0
29%
21%
13%
6%
12%
9%
17%
10%
16%
9%
Perc
en
tag
e o
f n
eo
nata
l m
orb
idit
y
Progesterone
Placebo
RDSNICU
admission
Composite
neonatalmorbidity/mortality
Mechanical
ventilation
Birth weight
<1500g
Romero R, Nicolaides K, Conde-Agudelo A, Tabor A, O’Brien J, Cetingoz E, DA Fonseca E,
Creasy G, Klein K, Rode L, Soma-Pillay P, Fusey S, Cam C, Alfirevic Z, Hassan S. Am J Obstet Gynecol 2011;12:003
25%
52%
34%
43% 45%
32ALL STATISTICALLY SIGNIFICANT
Hassan, Hernandez, Romero
Ultrasound Obstet Gynecol. 2016; 48(3) :308-17.
Fonseca 2007
O’Brien 2007
Hassan 2011
Cetingoz 2011
OPPTIMUM 2016
Combined
24/14 39/112 29.5 0.60 (0.39-0.94)
4/12 6/19 3.5 1.06 (0.37-2.98)
28/235 46/223 35.3 0.58 (0.37-0.89)
1/4 2/4 1.5 0.5 (0.07-3.55)
33/133 38/118 30.2 0.77 (0.52-1.14)
90/498 131/476 100 0.66 (0.52-0.83)
Relative risk (fixed)
(95% CI)
Vaginal
Progesterone
(n/N)
Placebo
(n/N) Weight
(%)
Relative risk
(95% CI)
Favors placebo Favors vaginal progesterone
Study
0.05 0.1 0.2 0.3 0.5 1 2 3 5Test for heterogeneity I2 =0%
Test for overall effect Z= 3.48, P=0.0005
Hassan, Hernandez, Romero
The Next Step:
A Meta-analysis of Individual Patient Data
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol.
2017; pii: S0002-9378(17)32343-8

15
Studies included in the individual patient data meta-analysis
Study,
year
Trial enrollmentParticipants randomly assigned in
original trial
Participants
eligible for
IPDMATreatment groups Compliance
Fonseca,
2007
8 centres in the
UK, Chile,
Brazil, and
Greece
250 with a singleton or twin
gestation and a cervical length ≤15
mm
226 Vaginal progesterone 200
mg/day or placebo from 24-33
6/7 weeks of gestation
92% for the vaginal
progesterone
group and 94% for
the placebo group
O'Brien,
2007
53 centres in
US, South
Africa, India,
Czech Republic,
Chile, and El
Salvador
659 with a singleton gestation and a
history of spontaneous preterm
birth
31 Vaginal progesterone 90
mg/day or placebo from 18-22
to 37 0/7 weeks of gestation,
rupture of membranes or
preterm delivery, whichever
occurred first
100% for the
vaginal
progesterone
group and 95% for
the placebo group
Cetingoz,
2011
Single centre in
Turkey
160 with twin gestation, or
singleton gestation with previous
spontaneous preterm birth or
uterine malformation
8 Vaginal progesterone
suppository 100 mg/day or
placebo from 24-34 weeks of
gestation
100% for both
study groups
Hassan,
2011
44 centres in
US, Belarus,
Chile, Czech
Republic, India,
Israel, Italy,
Russia, South
Africa, and
Ukraine
465 with a singleton gestation and a
cervical length between 10-20 mm
458 Vaginal progesterone 90
mg/day or placebo from 20-23
6/7 to 36 6/7 weeks of
gestation, rupture of
membranes or preterm
delivery, whichever occurred
first
89% for the vaginal
progesterone
group and 93% for
the placebo group
Norman,
2016
66 centres in
the UK and
Sweden
1228 with a singleton gestation and
previous spontaneous preterm
birth, or cervical length ≤25 mm, or
a positive fetal fibronectin test
combined with other clinical risk
factors for preterm birth
251 Vaginal progesterone 200
mg/day or placebo from 22-24
to 34 weeks of gestation or
preterm delivery, whichever
occurred first
63% for the vaginal
progesterone
group and 69% for
the placebo group
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol. 2017; pii: S0002-9378(17)32343-8
Effect of vaginal progesterone on preterm birth
before 33 weeks’ gestation
Study Relative risk (fixed) 95% CI
Vaginal
progesterone
n/N
Placebo
n/N
Weight
%
Relative
risk
(95% CI)
Fonseca
200719/114 31/112 28.5
0.60
(0.36-1.00)
O’Brian
20071/12 4/19 2.8
0.40
(0.05-3.13)
Hassan
201121/235 26/223 33.6
0.55
(0.33-0.92)
Cetingoz
20110/4 1/4 1.4
0.33
(0.2-6.37)
Norman
201629/133 35/118 33.7
0.74
(0.48-1.12)
Combined 70/498 107/476 100.00.62
(0.47-0.81)
0.05 0.1 0.2 0.3 0.5 1 2 3 5
Favours vaginal progesterone Favours placebo
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol.
2017; pii: S0002-9378(17)32343-8
Outcome IPD Meta-analysis
OutcomeRR or mean
difference (95% CI)
Vaginal
Progesterone
Group
Placebo Groupp
value
NNT(95%CI
)
Pregnancy outcome
Delivery before 36
weeks0·80 (0·67 to 0·97) 28% 35% 0·02 14 (9-96)
Delivery before 34
weeks0·65 (0·51 to 0·83) 17% 26%
0·000
611 (8-22)
Delivery before 28
weeks0·67 (0·45 to 0·99) 8% 11% 0·04
27(16-
881)
Any maternal adverse
event 1·21 (0·87 to 1·69) 12% 11% 0·26 ··
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol.
2017; pii: S0002-9378(17)32343-8
Outcome IPD Meta-analysis
OutcomeRR or mean
difference (95% CI)
Vaginal
Progesterone
Group
Placebo Groupp
value
NNT(95%CI
)
Pregnancy outcome
Delivery before 36
weeks0·80 (0·67 to 0·97) 28% 35% 0·02 14 (9-96)
Delivery before 34
weeks0·65 (0·51 to 0·83) 17% 26%
0·000
611 (8-22)
Delivery before 28
weeks0·67 (0·45 to 0·99) 8% 11% 0·04
27(16-
881)
Any maternal adverse
event 1·21 (0·87 to 1·69) 12% 11% 0·26 ··
Perinatal outcome ? ? ? ?
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol.
2017; pii: S0002-9378(17)32343-8
Outcome IPD Meta-analysis
OutcomeRR or mean
difference (95% CI)
Vaginal
Progesterone
Group
Placebo Groupp
value
NNT(95%CI
)
Pregnancy outcome
Delivery before 36
weeks0·80 (0·67 to 0·97) 28% 35% 0·02 14 (9-96)
Delivery before 34
weeks0·65 (0·51 to 0·83) 17% 26%
0·000
611 (8-22)
Delivery before 28
weeks0·67 (0·45 to 0·99) 8% 11% 0·04
27(16-
881)
Any maternal adverse
event 1·21 (0·87 to 1·69) 12% 11% 0·26 ··
Perinatal outcome
Respiratory distress
syndrome0·47 (0·27 to 0·81) 5% 10% 0·007 18 (13-51)
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol.
2017; pii: S0002-9378(17)32343-8
Outcome IPD Meta-analysis
OutcomeRR or mean
difference (95% CI)
Vaginal
Progesterone
Group
Placebo Groupp
value
NNT(95%CI
)
Pregnancy outcome
Delivery before 36
weeks0·80 (0·67 to 0·97) 28% 35% 0·02 14 (9-96)
Delivery before 34
weeks0·65 (0·51 to 0·83) 17% 26%
0·000
611 (8-22)
Delivery before 28
weeks0·67 (0·45 to 0·99) 8% 11% 0·04
27(16-
881)
Any maternal adverse
event 1·21 (0·87 to 1·69) 12% 11% 0·26 ··
Perinatal outcome
Respiratory distress
syndrome0·47 (0·27 to 0·81) 5% 10% 0·007 18 (13-51)
Composite neonatal
morbidity/mortality†0·59 (0·38 to 0·91) 8% 14% 0·02 18 (12-81)
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol.
2017; pii: S0002-9378(17)32343-8

16
Outcome IPD Meta-analysis
OutcomeRR or mean
difference (95% CI)
Vaginal
Progesterone
Group
Placebo Groupp
value
NNT(95%CI
)
Pregnancy outcome
Delivery before 36
weeks0·80 (0·67 to 0·97) 28% 35% 0·02 14 (9-96)
Delivery before 34
weeks0·65 (0·51 to 0·83) 17% 26%
0·000
611 (8-22)
Delivery before 28
weeks0·67 (0·45 to 0·99) 8% 11% 0·04
27(16-
881)
Any maternal adverse
event 1·21 (0·87 to 1·69) 12% 11% 0·26 ··
Perinatal outcome
Respiratory distress
syndrome0·47 (0·27 to 0·81) 5% 10% 0·007 18 (13-51)
Composite neonatal
morbidity/mortality†0·59 (0·38 to 0·91) 8% 14% 0·02 18 (12-81)
Neonatal death 0·44 (0·18 to 1·07) 1% 3% 0·07 ··
†Occurrence of any of the following events: respiratory distress syndrome, intraventricular hemorrhage, necrotizing enterocoli tis, proven
neonatal sepsis, or neonatal death
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol. 2017; pii: S0002-9378(17)32343-8
What is the totality of the data?
Vaginal progesterone reduces the risk
of preterm birth and improves
perinatal outcome in women with a
short cervix
Vaginal progesterone is safe for use in
pregnancy
Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien J, Cetingoz E, Creasy G, Hassan Sonia, Nicolaides KH et al. Am J Obstet Gynecol.
2017; pii: S0002-9378(17)32343-8
Prior Preterm Birth and a Short Cervix:
Cerclage or Vaginal Progesterone?
Hassan, Hernandez, RomeroConde-Agudelo A, Romero R, Nicolaides K, et al. Am J Obstet Gynecol 2013;208:42.e1-18.
Hassan, Hernandez, Romero
Interventions to Prevent Preterm Birth
in Women with a Short Cervix
O
C
CH3
O
Progesterone Cerclage
www.dr-arabin.de
Pessary
Hassan, Hernandez, Romero
1) Vaginal progesterone:
• significant 53% reduction in the risk of preterm birth at <32
weeks
• 57% decrease in the risk of composite perinatal morbidity
and mortality
2) Cervical cerclage:
• significant 34% reduction in the risk of preterm birth at <32
weeks
• 36% decrease in the risk of composite perinatal morbidity
and mortality
3) Vaginal progesterone and cervical cerclage both effective
4) Surgery vs. medical
Prior preterm birth and a Short Cervix:
Cerclage or Vaginal Progesterone?
Conde-Agudelo A, Romero R, Nicolaides K, Chaiworapongsa T, O’Brien JM, Cetingoz E, Da Fonseca E, Creasy G, Soma-
Pilly P, Fusey S, Cam C, Hassan SS. Am J Obstet Gynecol. 2012 Nov 13. [Epub ahead of print].Hassan, Hernandez, Romero

17
1) Pre-cerclage 6 mm
2) Post-cerclage 14.1 mm
(1)
(2)
Cervical Length After Cerclage
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
1) Pre-cerclage 12.1 mm
2) Post-cerclage 15.7 mm
Cervical Length After Cerclage
(1)
(2)
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Cervical Length After Cerclage
1) Pre-cerclage 9.6 mm
2) Post-cerclage 18.6 mm
(1)
(2)
Cervical length After Cerclage
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero
Interventions to Prevent Preterm Birth
in Women with a Short Cervix
O
C
CH3
O
Progesterone Cerclage
www.dr-arabin.de
Pessary
Evidence for the use of a
pessary to
reduce preterm birth
in women with a short
cervix is not conclusive
Hassan, Hernandez, Romero
Twins
Perinatology Research Branch, NICHD/NIH, Wayne State UniversityHassan, Hernandez, Romero

18
O
C
CH3
O
ProgesteroneSonographic Short
Cervix
Perinatology Research Branch, NICHD/NIH, Wayne State University
13 mm
Hassan, Hernandez, RomeroR. Romero A. Conde-Agudelo W. El-refaie L. Rode M. L. Brizot E. Cetingoz V. Serra E. Da Fonseca M. S. Abdelhafez
A. Tabor A. Perales S. S. Hassan K. H. Nicolaides. Ultrasound Obstet Gynecol. In Press
Effect of Vaginal Progesterone on the Risk of
TWINS
0.05 0.1 0.2 0.3 0.5 1 2 3
9/15 4/6 8.8 0.90 (0.45-1.81)
3/5 1/1 3.5 0.78 (0.27-2.22)
50/159 62/144 100.0 0.69 (0.51-0.93)
5 Test for heterogeneity: I2 = 0%
Test for overall effect: Z = 2.44, P = 0.01
Study
Relative risk (fixed)
(95% CI)
Vaginal
progesterone
n/N
Placebo/no
treatment
n/NWeight
(%)
Relative risk
(95% CI)
Favors vaginal progesterone Favors placebo
Brizot 2015
Combined
1/5 1/2 2.2 0.04 (0.04-3.74) Cetingoz 2011
Serra 2013
3/7 5/14 5.2 1.20 (0.40-3.63)Rode 2007
3/11 7/13 9.9 0.51 (0.17-1.50Fonseca 2007
R. Romero A. Conde-Agudelo W. El-refaie L. Rode M. L. Brizot E. Cetingoz V. Serra E. Da Fonseca M. S. Abdelhafez
A. Tabor A. Perales S. S. Hassan K. H. Nicolaides. Ultrasound Obstet Gynecol. In Press
10
31/116 44/108 70.4 0.66 (0.45-0.96) El-refaie 2016
Effect of Vaginal Progesterone on the Risk of Adverse
Perinatal Outcomes
Events (n)/total n Pooled RR (95% CI)
Outcome TrialsVaginal
progesterone
Placebo/no
treatment
Assuming
independence
between twins
Adjustment for
non-independence
between twins
I2
(%)
NNT
(95% CI)
RDS 6 102/311 131/2800.67
(0.55-0.82
0.70
(0.56-0.89)0
6
(4-16)
Neonatal death 6 34/318 62/2880.50
(0.34-0.71)
0.53
(0.35-0.81)25
8
(5-19)
Perinatal death 6 43/318 72/2880.51
(0.36-0.70)
0.36
(0.39-0.84)24
7
(5-20)
Composite
neonatal
morbidity/mortality
5 23/84 28/700.57
(0.36-0.93)
0.61
(0.34-0.98)0
6
(3-109)
Birth weight <1500
grams6 48/315 73/280
0.52
(0.38-0.72)
0.53
(0.25-0.80)17
7
(5-17)
Mechanical
ventilation6 49/311 76/280
0.52
(0.37-0.71)
0.54
(0.36-0.810
7
(5-17)
R. Romero A. Conde-Agudelo W. El-refaie L. Rode M. L. Brizot E. Cetingoz V. Serra E. Da Fonseca M. S. Abdelhafez
A. Tabor A. Perales S. S. Hassan K. H. Nicolaides. Ultrasound Obstet Gynecol. 2017 Jan 9. [Epub ahead of print]
Should all Women be
Screened with Transvaginal
Ultrasound for Cervical
Length?
Hassan, Hernandez, Romero
Practical Consideration
Hassan, Hernandez, Romero

19
How Difficult and Time-Consuming is it
to Perform a Transvaginal Ultrasound?
Romero R, Hernandez-Andrade E, Hassan SS
Pain Score Indicated in the Third-trimester Group for the Different
Methods of Examining the Cervix:
Transvaginal Ultrasound, Transperineal Ultrasound, and Digital
Examination
Meijer-Hoogeveen M et al. Ultrasound Obstet Gynecol 2008;32:657-62
60
Score 5(Extremely
Painful)
0 10 20 30 40Percent 50
Score 4(Severely
Painful)
Score 3(Moderately
Painful)
Score 2(Mildly
Painful)
Score 1(Mildly
Painful)
Transvaginal ultrasound
Transperineal ultrasound Digital examination
Am J Obstet Gynecol 2012 Feb; 206(2):101-3Hassan, Hernandez, Romero
World Health Organization
Ten Principles for Good Screening Test
1. Condition = Important Health Problem
2. Available Treatment
3. Facilities Available for Diagnosis
4. Recognizable Latent Phase
5. Suitable Test or Examination
6. Test Acceptable to Population
7. Natural History of Disease Adequately Understood
8. Policy for Treatment
9. Cost of Case-Finding Economically Balanced with Care
10. Case-Finding Should be Continuing ProcessWilson JMG, Jungner G. World Health Organization 1968
Coombs, AC. Am J Obstet Gynecol 2012 Feb; 206(2):101-3
Hassan, Hernandez, Romero
Comparison of Strategies used for
Screening in Medicine
Test Number needed to screen
Pap Smear for Cervical Cancer1 1140
Mammography more than 50 years1 543
Mammography between 40 and 49 years1 3125
Prostate-specific Antigen for Prostate Cancer2 1254
Ultrasound cervical length to prevent one case of PTB
< 33 weeks (<25 mm)3357
Ultrasound cervical length to prevent one case of
neonatal morbidity/mortality (<25 mm)3218
1. Gates TJ, et al. Am Fam Physician 2001;63:513-22
2. Loeb S, et al. J Clin Oncol 29:464-467
3. Romero R, Conde-Agudelo A, unpublished.Hassan, Hernandez, Romero
Future Sonographic Methods to
Evaluate the Uterine Cervix for
the Prediction of
Preterm Birth?
Hassan, Hernandez, Romero

20
Cervical Elastography and the
Prediction of Preterm Birth
Hassan, Hernandez, Romero
Elastography
• Tissue displacement (strain) or velocity of
propagation of a mechanic stimulus within the
cervix as a ‘shear wave” can provide
information on the softness/stiffness of the
cervix
• Changes in “elasticity” are displayed in a color
elastogram
Ophir J, Cespedes I, PonnekantiH, Yazdi Y, Li X. Elastography: a quantitative method for imaging the elasticity of
biological tissues. Ultrason Imaging 1991; 13: 111–134.Hassan, Hernandez, Romero
Hernandez-Andrade E, Hassan SS, Ahn H, Korzeniewski SJ, Yeo L, Chaiworapongsa T, Romero R. Ultrasound
Obstet Gynecol 2013; 41: 152-161
Cervical Shear Wave Elastography
Hassan, Hernandez, Romero
Sagittal view of the cervix showing in red slow shear wave velocity (soft tissue) and
in blue high shear wave velocity (stiff tissue)
Cervical Shear Wave Elastography
in the internal and in the external os
Hernandez-Andrade E, Hassan SS, Ahn H, Korzeniewski SJ, Yeo L, Chaiworapongsa T, Romero R.
Ultrasound Obstet Gynecol 2013; 41: 152-161
Soft areas are displayed in red/orange
Stiff areas are displayed in blue
Transverse view of the Internal os showing in
blue high shear wave velocity (stiff tissue)
Transverse view of the external os showing in
red slow shear wave velocity (soft tissue)
Hassan, Hernandez, Romero
Color elastogram
ElastogramRegion of Interest
Averaged oscillatory displacement
Applied to the entire elastogram
Stiffness color bar
Strain or
percentage o deformation
Within the ROI
Cervical Strain Elastography in the
internal os
Hassan, Hernandez, Romero
<12 12-<16 16-<20 20-<24 24-<28 28-<30 38-<36 >360.0
0.1
0.2
0.3
0.4
0.5
0.6
Gestational age (weeks)
Str
ain
(%
)
External cervical os
Complete cervix
Internal cervical os
In Normal Pregnancies the Internal Cervical os
Becomes Softer (Increased Strain) as Gestation
Progresses
Hernandez-Andrade E, Hassan SS, Ahn H, Korzeniewski SJ, Yeo L, Chaiworapongsa T, Romero R. Ultrasound
Obstet Gynecol 2013; 41: 152-161Hassan, Hernandez, Romero

21
Increased Prevalence of Preterm Delivery <37 weeks in
Women with Strain in the Internal os >50th Percentile for
Gestational Age at 17-24 Weeks
Hernandez E, Hassan S, Chaiworapongsa T, Romero R, J. Perinat. Med. 2014; 42(2): 159–169
0
2
4
6
8
10
12
14
1614.9%c
11.5%
3.0%
8.0%
Cervical strain
%
25th 50th 75th 100th
Pregnant women with low
strain values in the internal cervical os
have the lowest risk
of preterm delivery
Pregnant women with strain values >50th
percentile in the internal cervical os
have the highest risk of preterm delivery
Hassan, Hernandez, Romero
• Sonographic cervical length is the most powerful predictor of
preterm birth
• The definition of a short cervix varies by obstetrical history
• In patients with a short cervix in the midtrimester:
• 22 have intra-amniotic inflammation and 9% have intra-amniotic infection
• The optimal time to examine the cervix is 19-24 weeks gestation
• Correct technique for cervical length examination is critical
• The cervix should be measured
• With an empty bladder by transvaginal ultrasound, in a sagittal view
Hassan, Hernandez, Romero
Conclusions (I)
• Amniotic fluid sludge increases the predictive value for preterm
delivery
• In women with a sonographic short cervix:
• Vaginal progesterone decreases preterm birth and neonatal morbidity in women
with a short cervix (singletons and twins)
• Cerclage reduces preterm birth (prior history of preterm birth and a short cervix)
• Pessary has not been definitively proven to decrease preterm birth
• It is of benefit for pregnant women to undergo a sonographic
cervical length measurement in the midtrimester to assess her risk
for preterm birth
Hassan, Hernandez, Romero
Conclusions (II) Key References
1. Burger M, Weber-Rössler T, Willmann M. Measurement of the pregnant cervix by transvaginal sonography:
an interobserver study and new standards to improve the inter-observer variability. Ultrasound Obstet
Gynecol. 1997 Mar;9(3):188-93.
2. Hassan SS, Romero R, Berry SM et al. Patients with an ultrasonographic cervical length < or = 15 mm have
nearly a 50% risk of early spontaneous preterm delivery. Am J Obstet Gynecol 200; 182:1458.
3. Hassan SS, Romero R, Vidyadhari D, Fusey S, Baxter JK, Khandelwal M, Vijayaraghavan J, Trivedi Y, Soma-
Pillay P, Sambarey P, Dayal A, Potapov V, O'Brien J, Astakhov V, Yuzko O, Kinzler W, Dattel B, Sehdev H,
Mazheika L, Manchulenko D, Gervasi MT, Sullivan L, Conde-Agudelo A, Phillips JA, Creasy GW;
PREGNANT Trial. Vaginal progesterone reduces the rate of preterm birth in women with a sonographicshort cervix: a multicenter, randomized, double-blind, placebo-controlled trial. Ultrasound Obstet Gynecol.
2011 Jul;38(1):18-31
4. Romero R, Conde-Agudelo A, El-Refaie W, Rode L, Brizot ML, Cetingoz E, Serra V, Da Fonseca E,
Abdelhafez MS, Tabor A, Perales A, Hassan SS, Nicolaides KH. Vaginal progesterone decreases preterm
birth and neonatal morbidity and mortality in women with a twin gestation and a short cervix: an updated
meta-analysis of individual patient data. Ultrasound Obstet Gynecol. 2017 Mar;49(3):303-314
5. Romero R, Conde-Agudelo A, Da Fonseca E, O’Brien JM, Cetingoz E, Creasy GW, Hassan SS, Nicolaides
KH. Vaginal Progesterone for Preventing Preterm Birth and Adverse Perinatal Outcomes in Singleton
Gestations with a Short Cervix: A Meta-Analysis of Individual Patient Data. AJOG. 2017 Nov; pii: S0002-
9378(17)32343-8.
Hassan, Hernandez, Romero
Thank You
Hassan, Hernandez, Romero