discussant: paramount: efficacy and safety of lcz696, a first-in
TRANSCRIPT

Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease
Clinical Military Hospital
Wroclaw, Poland
PARAMOUNT: Efficacy and Safety of LCZ696,
a First-in-Class Angiotensin Receptor Neprilysin Inhibitor,
in Patients with Heart Failure and Preserved Ejection Fraction:
Primary Results from the PARAMOUNT Study
Discussant
Disclosure
Consultancy fees and speaker’s honoraria from:
Novartis, Servier, Johnson & Johnson, Bayer, Pfizer,
Merck-Serono

“Heart failure with preserved ejection fraction
(HFpEF) is common, increasing in prevalence,
and causes substantial morbidity, and resource
utilization, particularly among the elderly”
Amil M. Shah and Scott D. Solomon, Eur Heart J 2012
TEMPORAL TRENDS IN THE PREVALENCE OF HEART FAILURE
Among patients hospitalized with
worsening HF 40-60% have preserved LVEF
Owan TE et al. NEJM 2006;355:251-9

Heart Failure with Preserved Ejection Fraction:
what is known ?
• epidemiology
• natural history
• disease burden
well-characterized
• diagnosis – difficult, lack of non-invasive methods
• pathophysiology – heterogeneity, poorly understood
• treatment – no effect on morbidity and mortality
PARADOX

LCZ696: first-in-class, Angiotensin Receptor Neprilysin Inhibitor (ARNI)
Why should it work in HFPEF ?
Waeber B, Feihl F. Lancet 2010

LCZ696: first-in-class, Angiotensin Receptor Neprilysin Inhibitor (ARNI)
Why should it work in HFPEF ?
Tsai EJ, Kass DA. Pharmacol Ther 2009

LCZ696: first-in-class, Angiotensin Receptor Neprilysin Inhibitor (ARNI)
Why should it work in HFPEF ?
Waeber B, Feihl F. Lancet 2010
Vasopeptidase inhibitors
(omapatrilat)
↑ risk of angio-oedema
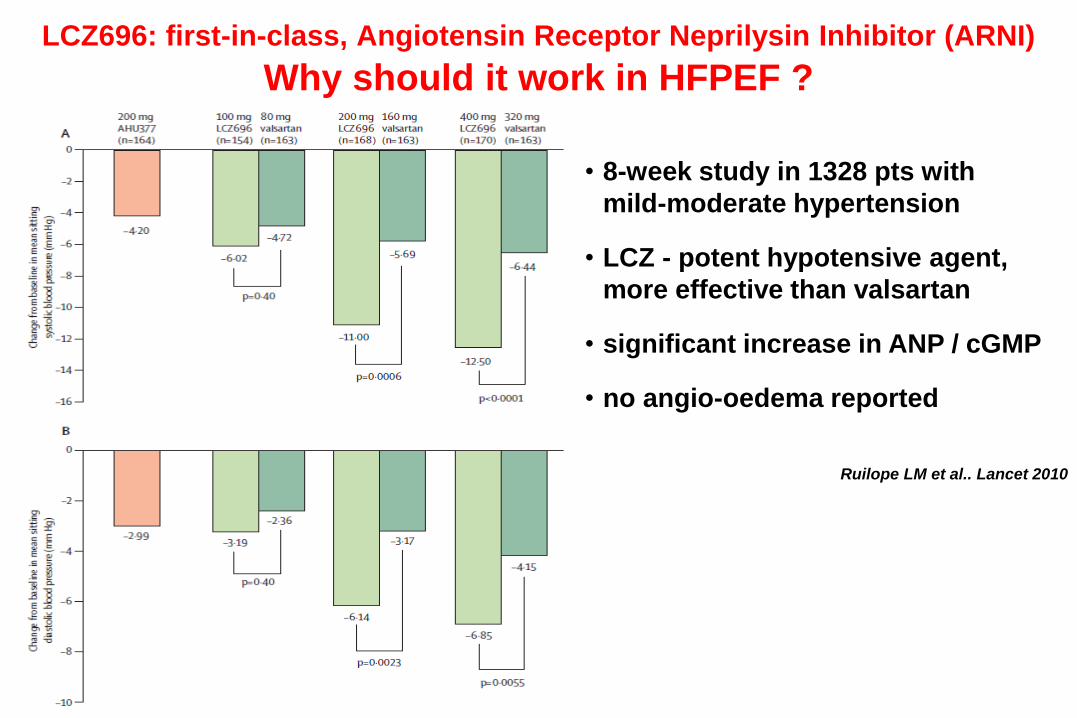
LCZ696: first-in-class, Angiotensin Receptor Neprilysin Inhibitor (ARNI)
Why should it work in HFPEF ?
Ruilope LM et al.. Lancet 2010
• 8-week study in 1328 pts with
mild-moderate hypertension
• LCZ - potent hypotensive agent,
more effective than valsartan
• significant increase in ANP / cGMP
• no angio-oedema reported

Results of PARAMOUNT trial which can be of
potential paramount importance for HFPEF patients
• Primary end-point met: significant decrease in NT-proBNP
(unrelated to changes in blood pressure, evident already after 4
weeks and sustained until week 36, visible across the whole
spectrum of the patients)
• Evidence for LA reverse remodeling (reduction in LA size)
• Trend towards improvement in symptoms (although at baseline
80% of patients in NYHA class II)
• LCZ696 therapy was safe and well-tolerated

Results of PARAMOUNT trial: open questions
• Is NT-proBNP an useful surrogate end-point in HFPEF ?
no significant difference vs valsartan at week 36
I-PRESERVE: benefit of irbesartan in patients with low NT-proBNP
Anand IS et al. Circ Heart Fail 2011

Results of PARAMOUNT trial: open questions
• Does LCZ696 favourably affect diastolic function ?
no significant difference in E/e’ and e’
Circulation 2006

Results of PARAMOUNT trial: open questions
• Why so few CV episodes ?
during 36-week follow-up: 3 (1%) deaths and 10 (3%) HF episodes
PEP-CHF MAGGIC
Cleland et al. NEJM 2007 Eur Heart J 2012

The great thing in this world
is not so much where we stand,
as in what direction
we are moving
Oliver Wendell Holmes 1841-1935