disordered gambling training - may 2015 - michele tantriella-modell and julie hynes
TRANSCRIPT
DISORDERED GAMBLINGin 2015: Trends, Implications & Services

Training Agenda• Introductions & Expectations• Overview, Definitions & Trends• Defining Disordered Gambling• Co-occurring Issues• Screening & Intervention• Problem Gambling Services• Wrap-up


Introductions & Expectations


DEFINITION:
______ something of valuein the _________________
something of greater value.hopes of obtaining
RISKING
Source: American Psychiatric Association - DSM-5 (2013).

A longhistory
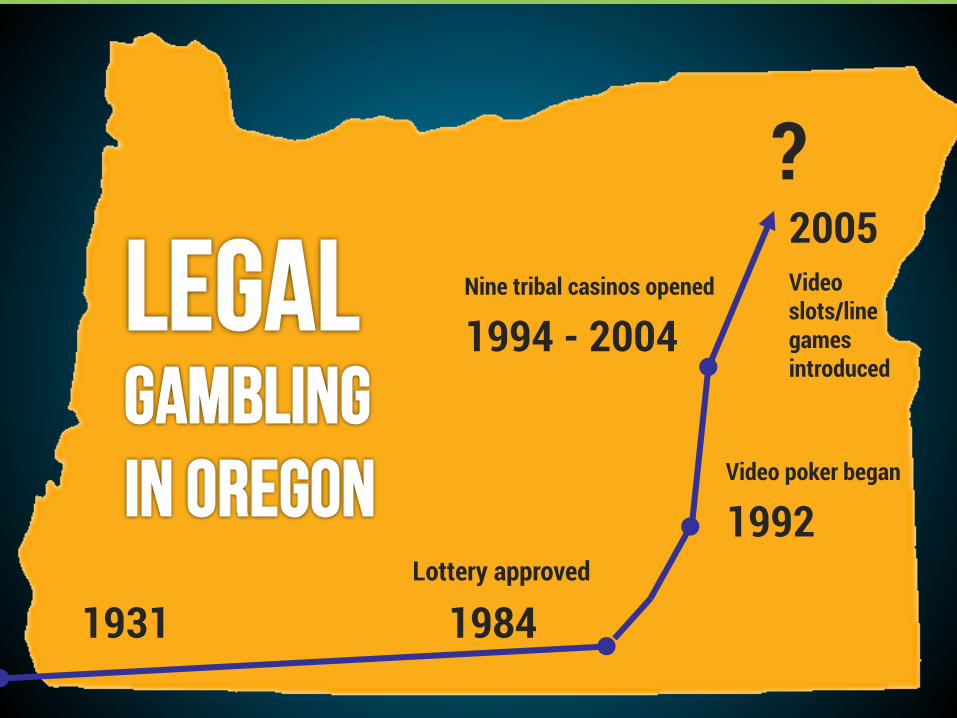
1931
Video poker began
1992
Nine tribal casinos opened
1994 - 2004
?
Lottery approved
1984

Gambling in Oregon Lottery Scratch-its Megabucks Powerball Keno Video lottery
Bingo/charitable gaming
Casino gaming
“Social gaming” (e.g., card houses)
Sports bets Horse racing Internet Office pools Poker/card nights Bets among friends Stock market (??)
Local “Social Gaming”

Image sources: Oregon Lottery, Hynes

Image sources: Oregon Lottery, Hynes

2,400 retailers in Oregon
ELECTRONIC GAMBLING:“Video Poker/Slots/Line Games”
Source: Oregon Lottery

$8.60out of
every $10 spent on lottery
Video Lottery:Video Poker / Video Slots / “Line Games”
Source: The OregonianPhoto source: Daniel Berman.

Going Mobile: Real Gambling…
16
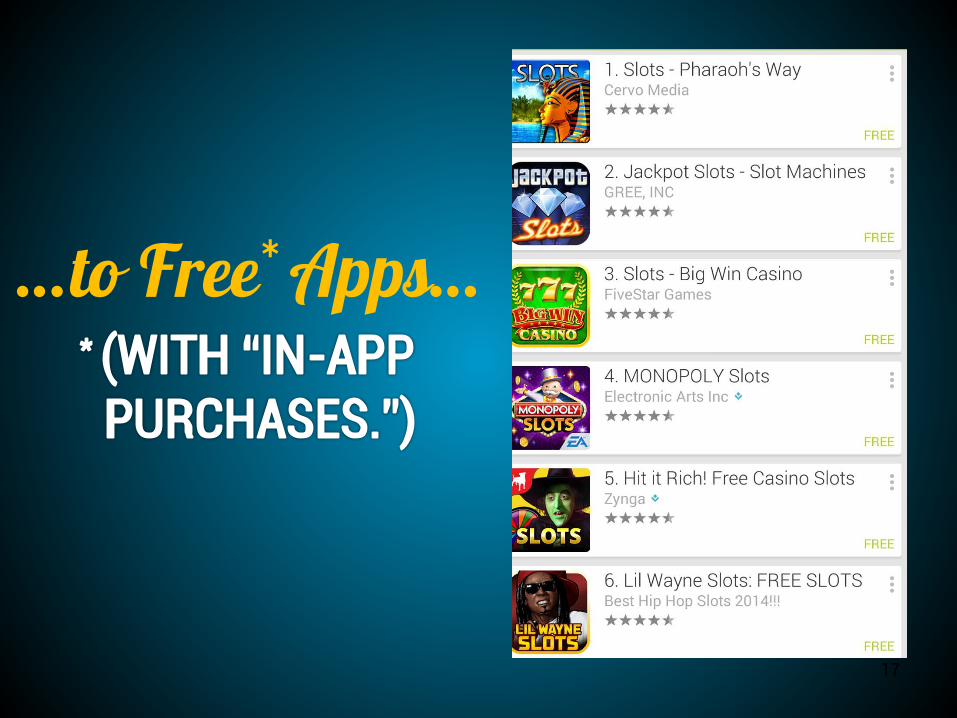
…to Free* Apps…
17

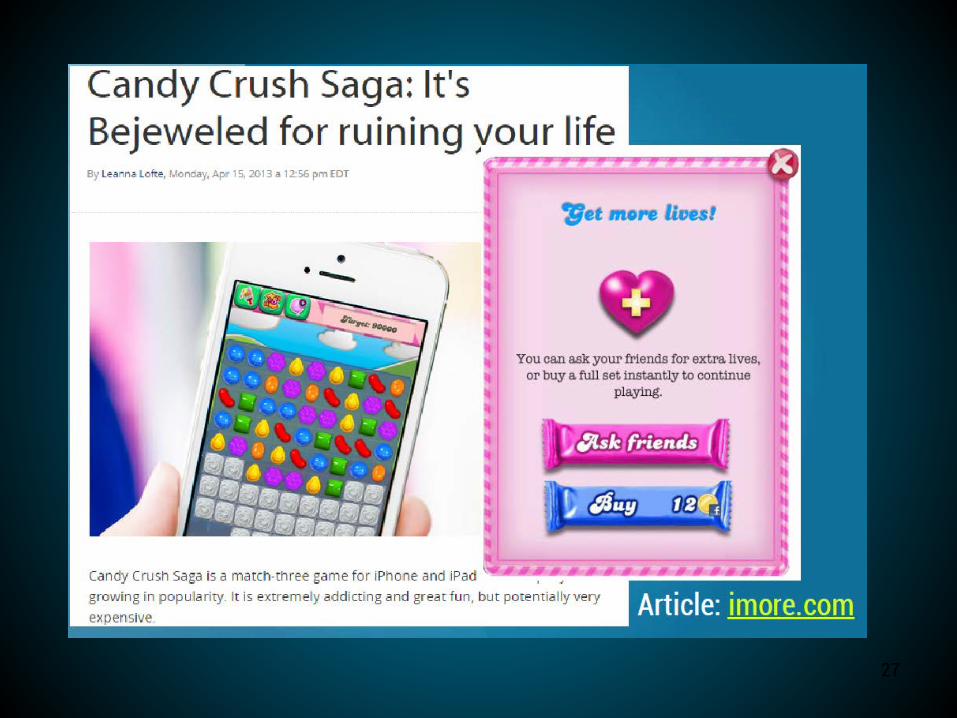
And this is where lines in 2015 start to blur…..
Gamingor Gambling?
18



21

Fantasy Sport$
22

23

2424

2525

26
27

Key
“A’s” of the Trends

AVAILABILITY.

Amygdala active
Risk-taking & impulsivity
Source: Ramoski, S., Nystrom, R. (2007). Image source: simpsons.wikia.org
age…

Acceptability.

Advertising.

Pop-up on my kid’s game, Feb 201533

2012 Oregon Student Wellness Survey, Lane County (“ESD”) and Oregon; available at http://oregon.pridesurveys.com/esds.php?year=2012
Awareness (low).
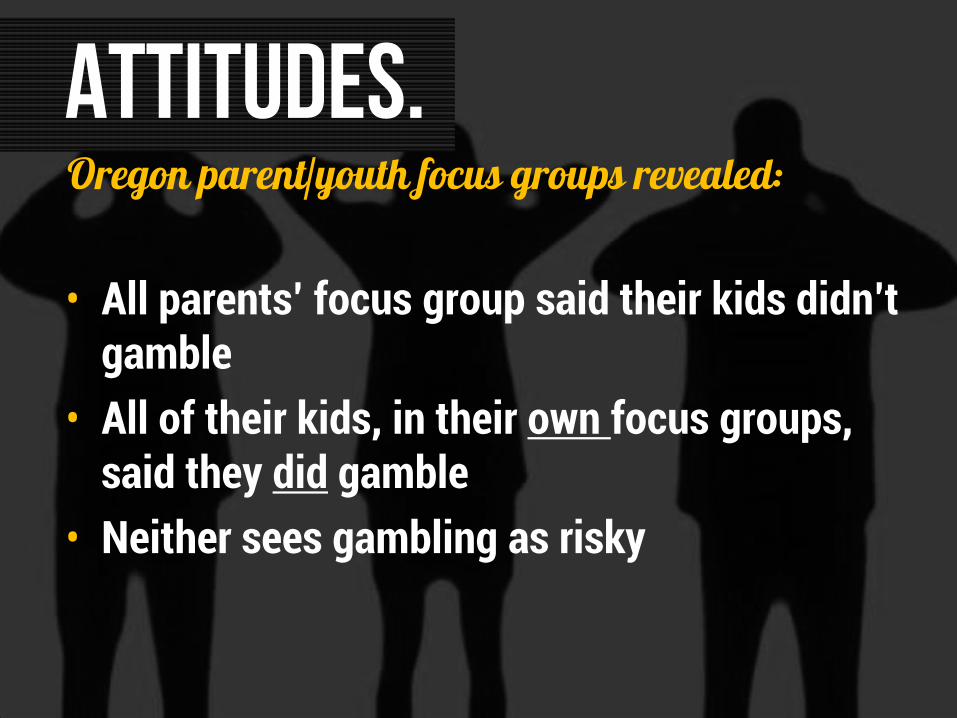
Oregon parent/youth focus groups revealed:
• All parents’ focus group said their kids didn’t gamble
• All of their kids, in their own focus groups, said they did gamble
• Neither sees gambling as risky
ATTITUDES.

More Gamblers ► More Problem Gamblers
Prevalence of gambling problems
is a function of the overall level of gambling participation

“Last Week Tonight with John Oliver” –11/9/14https://www.youtube.com/watch?v=9PK-netuhHA

disordered

PATHOLOGICAL:Persistent and recurrent maladaptive gambling behavior...results in the LOSS OF CONTROL over gambling. (DSM-IV)
Historical Definitions
New language
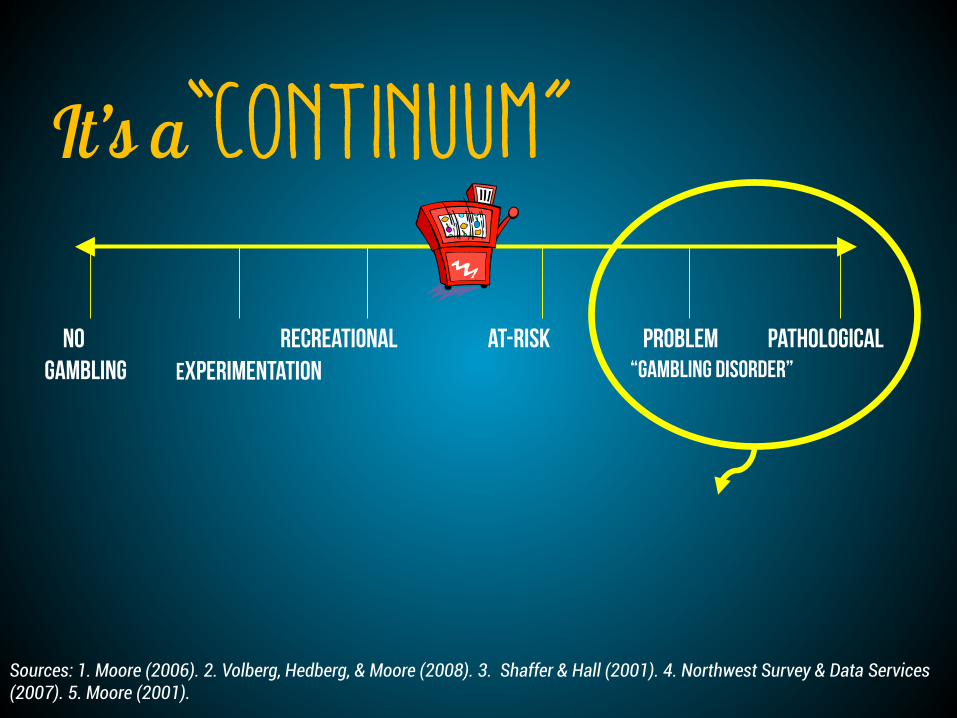
It’s a“Continuum”
No Gambling Experimentation
Recreational Problem Pathological
Sources: 1. Moore (2006). 2. Volberg, Hedberg, & Moore (2008). 3. Shaffer & Hall (2001). 4. Northwest Survey & Data Services (2007). 5. Moore (2001).
At-Risk“GAMBLING DISORDER”



Electronic Gambling
Electronic Gambling
89% Cards4%
Other7%
Oregon Gambling TreatmentGamblers' Preferences
Source: Oregon Health Authority.

The new DSM-5 (May 2013) definespathological gambling as a
“behavioral addiction,” the first of its kind.

Typical Phases of
Problem Gambling
Source: Custer, R. & Rosenthal, M.
WINNING
LOSING
DESPERATION
HOPELESSNESS

Source: http://www.oregon.gov/oha/amh/gambling/gear-workbook.pdf
THOUGHTS, FEELINGS, ANTICIPATION, FANTASY
(Gambler’s Mind, “Gambling Time/ Gambling Money”)
PLANNING(Removing obstacles
to gambling)
GAMBLING(“Winning & Losing”)
Serotonin Adrenaline
Dopamine
CRASHGuilt, Shame, Anger, Denial, Justification, Restless, Irritable, Depression, Panic or Numb, Suicidal Thoughts Dopamine
REALITY(Self with Others)“Real Time, Real Money”

$32k
85%
90%
24%
$27k$!
IS THE AVERAGE HOUSEHOLD INCOME. Range is from $0 to over $1million/year.
ARE WHITE. 4.4% Hispanic/Latino., 3.4% Asian. People of color are under-represented in treatment.
prefer ELECTRONIC GAMBLING. Video (slots/poker/line games). Cards 4.1%; scratch-its 1.3%; sports 0.9%;
HAVE COMMITTED CRIMES TO FINANCE THEIR GAMBLING. Most crimes are “white collar” (forgery, check fraud, embezzlement.)
IS THE AVERAGE INDIVIDUAL GAMBLING DEBT.
Oregonians in gambling treatment, 2012:

The “Addiction” Connection
• Loss of control• Denial• Depression/mood swings• Progressive• Tolerance• Use as an escape• Preoccupation• Similar “highs”• Self-help groups• Family involvement• Use of rituals
Differences?Similarities? Defining “use” (gambling) Behavior not attributable to
chemical ingestion No biological test More intense sense of shame and
guilt (anecdotal) Unpredictable outcome Fantasies of success /quitting is
giving up hope Easier to hide


Effects on Children• Higher abuse & neglect
• Higher levels of tobacco, alcohol & drug use, overeating & gambling among their children
Sources: 1. National opinion research center (1999). 2. Darbyshire, oster, & carrig (2001). 3. Gupta & derevensky (1997); jacobs (2000); wallisch & liu (1996). 4 volberg et al. (2008; ibid).


Some Key Risk FactorsOther
addiction issues
Starting early in life
Friends / family favorable
Community laws & norms
Mental health issues
53

People with other
addictions issues
People with other mental health issues
Military/ Veterans
Young people
Incarcerated persons
People of color
Older adults
WomenPeople of lower SES
People with history of
traumaMen
Vulnerable Populations
54

>70%are current
tobacco users
24%have current
alcohol problems
5%actually attempt
suicide
Source: Oregon Health Authority, 2013
27%experience
suicidal ideation
Use illicit drugs
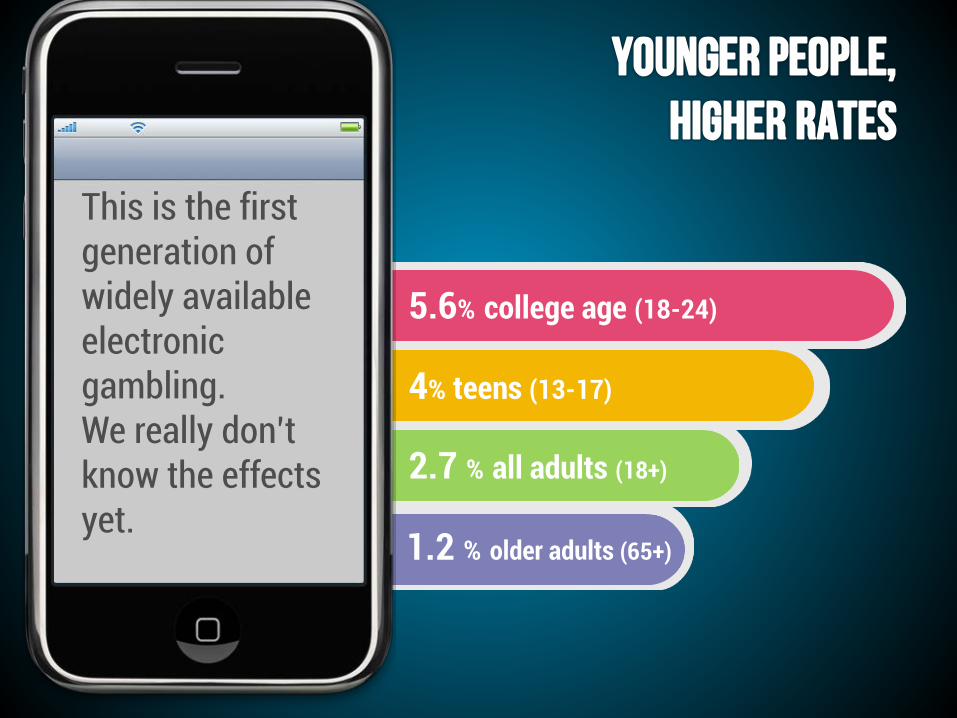
5.6% college age (18-24)
2.7 % all adults (18+)
4% teens (13-17)
This is the first generation of widely available electronic gambling. We really don’t know the effects yet.
1.2 % older adults (65+)

Adolescent Behavior & Brain Development
• Preference: ↑excitement and ↓ effort activities
• Prefer novelty• Poor planning & judgment• Minimal consideration of
negative consequences • More risky, impulsive
behaviors
Source: Grant, J (2008, October). The Adolescent Brain & Impulsive Behaviors. Healthy Brain Development: Key Impacts & Interventions Conference.

Age 65+• Rate of problem gambling lower (1.2%) 1
• BUT living close to gambling facility ↑↑risk– six times more likely to be problem
gamblers• ↑ risk factors 2
• Gambling = most frequently identified social activity 2
• Challenges in problem acceptance
Sources: 1. Moore (2001, ibid). 2. McNeilly & Burke (2000). Late life gambling: The attitudes and behaviors of older adults. Journal of Gambling Studies, 16, 393-415.
People of Color
• Higher proportion of problem gamblers (except Asians)
• Spend 2.5x more on gambling in a typical month
Source: Moore, Jadlos, & Carlson, 2000
Incarcerated Persons• One in three offenders
meet criteria for PG 1
– Highest rate in any population
• Gambling common in prison culture
• Resources limited to investigate crime & gambling 2
Sources: 1. Williams, Roysten & Hagen. (2005). Gambling and Problem Gambling Within Forensic Populations, A Review of the Literature 2. Myers, H. (2006). Organized crime in Oregon.
Military & Veterans• All four branches operate
slot machines overseas• Service members at higher
risk– Male, younger, racial/ethnic minorities– Marine corps highest rate of PG
• Alcohol & gambling connected
• Further article of interest: http://www.cnn.com/2007/US/05/22/military.gambling/index.html
Source: Department of Defense (2002). Survey of Health Related Behaviors Among Military Personnel Washington, DC: Author. Report information available at http://www.tricare.mil/main/news/dodsurvey.htm

Co-Occurrence with Mental Health & Addictions
Thought processes & distortionsNeurobiology & addiction connections
Similarities & differences

Mental Health & Addictions Connections
• Depression/mood disorders 1
– Depression – in one study, 76% of PGS had depression– Bipolar disorder – correlations with BPD & PG
• PTSD (studies of military veterans)– PTSD among problem gamblers estimated between 12.5 – 29% 2,3
• ADHD• Alcohol & other substance abuse disorders
Sources 1. Ledgerwood & Petry (2006). 2. Kausch et al. (2006). 3. Biddle et al. (2005). 4. Oregon DHS (2009).

brain

The PREFRONTAL CORTEX is the LAST PART to develop.
The brain is still
developinguntil
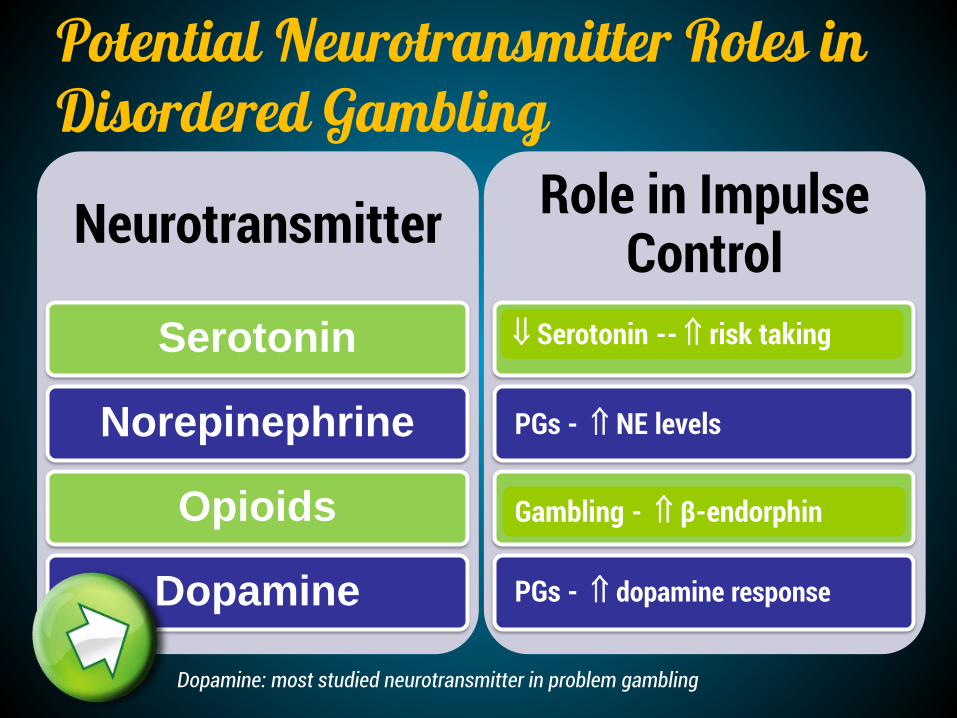
Neurotransmitter
Serotonin
Norepinephrine
Opioids
Dopamine
Role in Impulse Control
Behavior Initiation/Cessation
Arousal, Excitement
Pleasure, Urges
Reward, Reinforcement
⇓ Serotonin -- ⇑ risk taking
Gambling - ⇑ β-endorphin
PGs - ⇑ NE levels
PGs - ⇑ dopamine response
Potential Neurotransmitter Roles in Disordered Gambling
Dopamine: most studied neurotransmitter in problem gambling
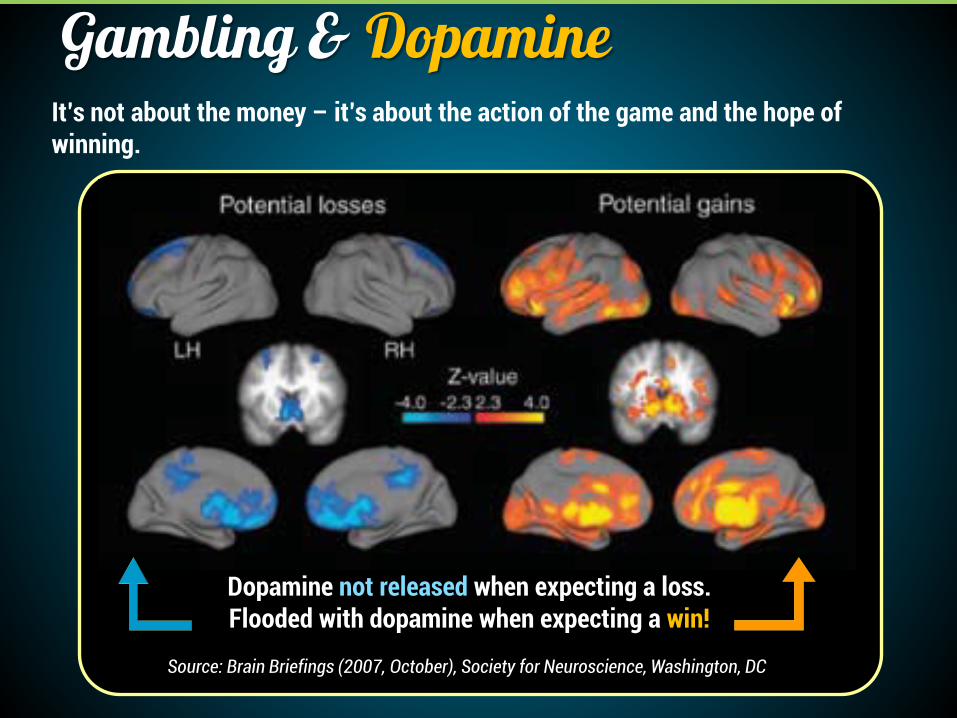
Source: Brain Briefings (2007, October), Society for Neuroscience, Washington, DC
Gambling & Dopamine
Dopamine not released when expecting a loss.Flooded with dopamine when expecting a win!
It’s not about the money – it’s about the action of the game and the hope of winning.

Image source: http://www.drugabuse.gov/pubs/teaching/largegifs/slide-2.gif
Survival Reward Pathway

Dopamine levels and behavioral pattern resulting from learned audiovisual cue (Figure from Self, 2003)
Source: Biology, Addiction & Gambling (http://www.basisonline.org/backissues/2003/vol8pdf/wager838.pdf)
"Monetary reward in a gambling-like experiment produces brain activation very similar to that observed in a cocaine addict receiving an infusion of cocaine.” -Hans Breiter, MD, co-director of the Motivation & Emotion Neuroscience Center, Massachusetts General Hospital

Sources: Tonneato, T. (1999). Cognitive psychopathology of problem gambling. Subst Use Misuse. Sep;34(11):159Anecdotal reports from problem gamblers in treatment and recovery.

Image source: Anheuser-Busch
Cognitive Distortions
• Lucky #’s• Favorite shirt• “My” machine
Superstition
Rituals/habits that are believed
to affect the outcome.

Cognitive Distortions
• Example (win): “Yeah buddy! I was just waiting on my card. I know this game inside and out.”
• Example (loss): “I would’ve won if that idiot didn’t get lucky and draw an ace.”
Biased EvaluationAttributing wins to one’s special skill or luck, while losses are blamed on external circumstances.
Image source: Anheuser-Busch
Cognitive Distortions
Forgetting about losses, only remembering wins.
Selective Memory

Cognitive Distortions
Failure to see each event as independent. Examples:• Trying to see patterns in coin flips.• “This slot machine is DUE to hit!”
Gambler’s Fallacy

Have you ever experienced a
cognitive distortion? What was the
experience like?
Reflect: cognitive distortions.


Creating conditions in families, schools, and communities that
promote the wellbeing of people
Emotional and behavioral health Physical health

Addressing the “A’s”

1. Awareness Building: Focusing on Brain Development & Technology
2. Education: Making Evidence-Based Connections with Other Problem Behaviors
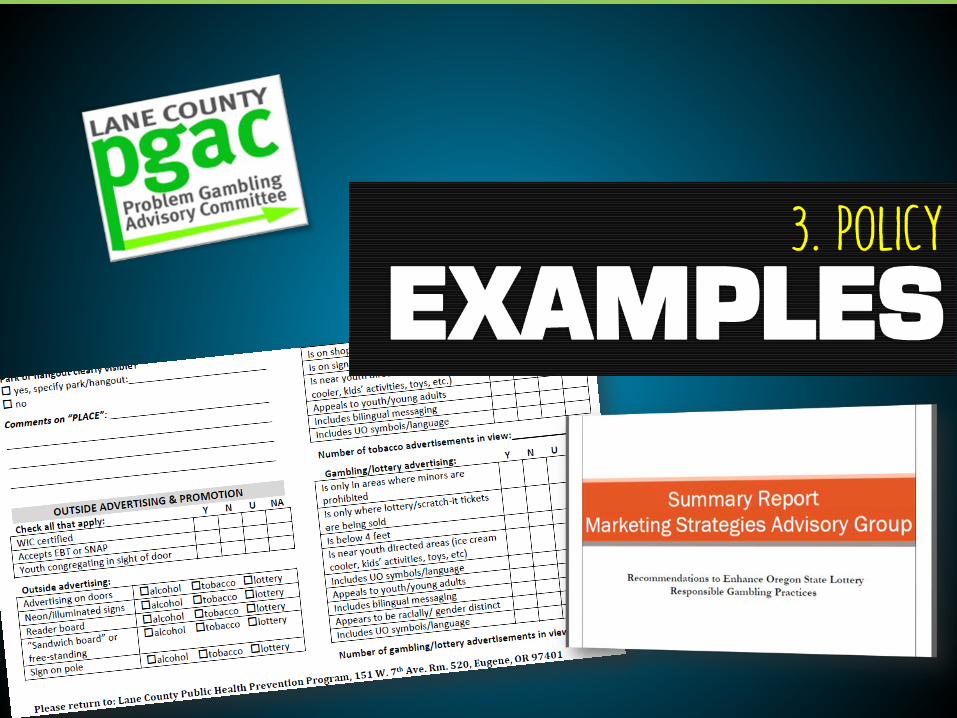
3. Policy: Systems level, implementing “Big P” & “little p”

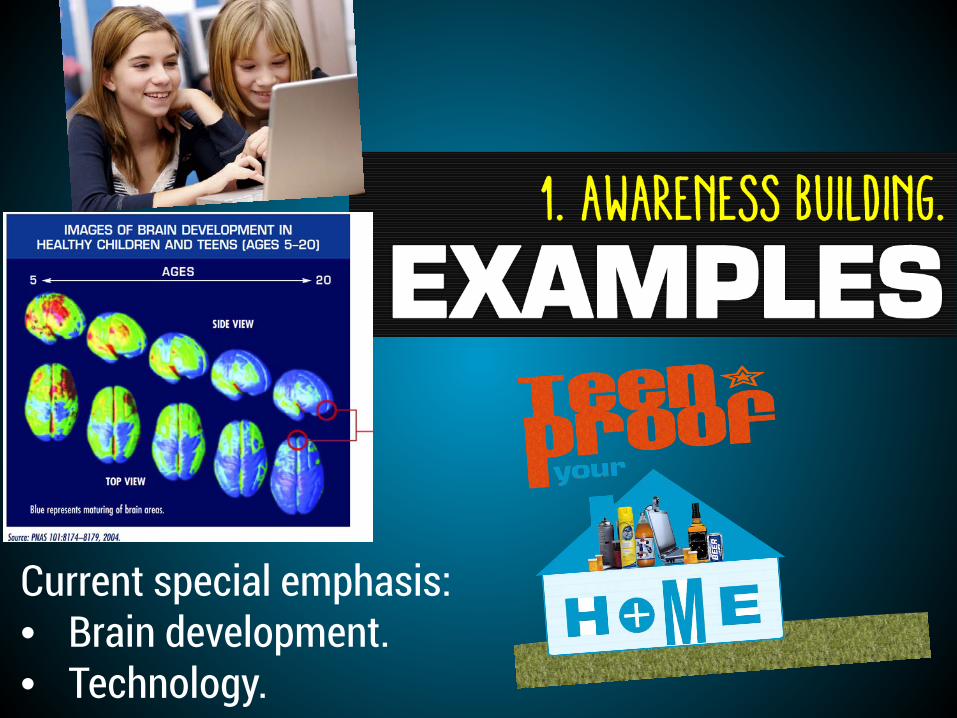
Current special emphasis:• Brain development.• Technology.

• Supporting evidence-based programs.• Curriculum integration.• Training integration.

Identification & Treatment

InterventionHelpline
emergence 24/7:
1.877.MY.LIMITReferred to provider for
assessmentFamily members come in;
later bring gambler in

Treatment Options in Oregon
• Minimal intervention: GEAR (Gambling Education and Reduction)
• Outpatient treatment (46)• Crisis respite (1)• Residential treatment (1)

Assessment Tools• “Valid and Reliable”
– DSM-V – South Oaks Gambling Screen (SOGS)
• Frequently Used– Gamblers Anonymous 20 Questions (GA-20)
Screening: The “Lie-Bet”
• Two questions to rule out pathological gambling behavior– 1) Have you ever felt the need to bet more and more
money?– 2) Have you ever had to lie to people important to
you about how much you gambled?• One or both “yes” answers indicate further
assessment needed– Further evaluation can be made by calling
1-877-MY-LIMIT (877-695-4648)

DSM Criteria Revisited1. Preoccupation with
gambling2. Increases amount of
money gambled3. Unsuccessfully tries to
quit4. Restless or irritable when
trying to cut down/stop5. Gambles as an escape
6. “Chases” losses7. Lies to others to conceal
gambling8. Has jeopardized
relationships9. Relies on others to bail
him/her out
Gambling Disorder = Four or more of above, AND: The gambling behavior is not better accounted for by a Manic Episode.
Mild (4-5) / Moderate (6-7) /Severe (8-9)

Treatment is Free IN OREGON.
24 hrs: 1-877-My-limitOnline: www.opgr.org

Emergence Gambling Treatment ProgramTreatment is gender-specific
Multimodal treatment - Individual sessions - Family therapy- Group sessions - Recreational counseling- Didactic lectures - Audiovisual education
Suggest to explore 12-step program

System Evaluation Results
• Treatment is working– 50% successful completion rate
– 64% of clients reported either no gambling or reduced gambling at 6-months post-treatment
• 97.3% of the completers at six-month follow-up and 93.9% of those at 12-month follow-up indicated strong endorsement regarding recommending the program to others
1. Oregon Health Authority, T.L. Moore (2014)

Wrapping it All Up• The lines of gaming and gambling have blurred, and
it’s become much more popular• This popularity doesn’t come without cost• Gambling problems often mimic other disorders in
manifestation, consequences, & co-occurrence• Problem gambling services are free, confidential,
available and effective• Important to assess for issue & make your clients
aware of services

Revisiting OurExpectations,Q&A
Anything lingering?

Evaluations

Thank You!!Julie Hynes
Prevention SpecialistLane County Public Health
Prevention Program
preventionlane.org
Michele Tantriella-ModellProgram Director
Emergence Meridian Gambling Treatment Program
4emergence.com