division of cerebrovascular diseases, department … p. adams jr, m.d. division of cerebrovascular...
TRANSCRIPT

Harold P. Adams Jr, M.D. Division of Cerebrovascular Diseases, Department of Neurology Carver College of Medicine UIHC Stroke Center University of Iowa

o I adjudicate events in clinical trials sponsored by Merck and I serve on the DSMB for a clinical study funded by Medtronic. I am a consultant to Pierre Fabre (France)
o I receive grant support from NINDS and St Jude Medical
o I will discuss therapies for treatment of stroke that are not approved by the FDA

o A leading cause of death and disability among Americans o Approximately 800,000 new strokes annually o Affects men, women, and children of all ages o More common in Blacks, Hispanics
o A leading cause of long-term disability o The most common acute neurological illness
o Leading neurological reason for hospitalization o The frequency of stroke is increasing
o Aging of the American population o Survival of high-risk patients with heart disease

Iowa Stroke Registry Design Project 4

o 4th most common cause of death – 1,627 deaths o 5 Iowans die from stroke every day o 3rd most common cause of death among women o 14% of the men dying of stroke are < 65 o The mortality rate from stroke has been declining
o In 2009, 8140 admissions for stroke in Iowa hospitals
o In 2008, average inpatient costs for stroke were $9282
o Total inpatient hospital costs are $78.2 million



¡ Number of patients =14,483
¡ Source of data § IHA Discharge Data
SAH, 176, 1% ICH, 546,
4% Other ICH, 314, 2%
Occlusion Precerebral, 4281, 30%
Occlusion Cerebral, 2871, 20%
TIA, 1413, 10% Acute, 21,
0%
Other, 1362, 9%
Late, 3499, 24%

o Important issue in Iowa o Approximately 25% of Americans
o Rural areas or small communities o Risk of stroke is 1.34 greater than urban areas
o Elderly, poor, minorities o Outcomes among rural patients
o Relative increase in mortality – 18% o Many problems not unique to rural America
o Suburban and non-‐academic hospitals o Non-‐availability of technology/expertise

o Large distances to hospitals o Hospitals – limited resources
o Critical access hospitals o Limited experience with stroke
o Non-availability of stroke specialists o Neurology o Interventional
o Interventions used in this setting o Time in transfer to medical center


o Current approach to early treatment of ischemic stroke o Change attitude of the public and health care system o Increase the number of persons treated o Core message
o Stroke is a life-‐threatening or life-‐changing disease o Stroke is an emergency o Stroke may be successfully treated and outcomes
improved o Time is brain
o Public education to recognize stroke and best responses
o Organize medical resources to treat stroke

o Public recognition of symptoms o Sudden onset of neurological symptoms o May not be recognized by patient, observers are key o Family, friends, neighbors, co-‐workers
o Response – immediately seek medical attention o Do not wait for symptoms to resolve o Call 911 or brought to the hospital o Arriving by EMS expedites early hospital care o If not stroke, many be another serious neurological
disease

o Treatment of stroke modeled on treatment of MI o Vascular events secondary to arterial occlusion o Need rapid treatment to limit organ injury o Treatment centers on reperfusion o Best managed in specialized centers o Most important early treatment occurs in the community
o Emergency cardiac care system is well-‐developed o Need to think of stroke in the same way and add
stroke care to the emergency cardiac care system

o Most patients are not treated with reperfusion therapy
o Most patients arrive too late for treatment or their strokes are considered to be mild
o Overall impact of intravenous thrombolysis is limited
o Impact of intra-arterial interventions is very small

o 4750 hospitals with 495,000 patients with ischemic stroke o 64% of hospitals had not treated a single patient o 0.9% of hospitals had treated 10 or more patients
o Low utilization of rtPA o Smaller (< 95 beds) hospitals o Less densely populated areas in South and Midwest o Areas that involve 40% of the American population
Kleindorfer et al, Stroke, 2009; 40: 3580

o Ischemic stroke is a common and serious disease o Potential for death or severe incapacity o Affects patient and family
o An approved therapy of proven value is available o Intravenous thrombolysis is approved by the FDA
o Success is linked to early treatment o Guidelines provide recommendations for care
o Improve safety and efficacy of treatment o Failure to follow guidelines associated with poorer
outcomes

o Not treating a patient may violate the rule of “doing no harm”
o The primary legal issue is not prescribing rtPA o Need a well-documented reason for not treating o Clearly state reasons in the medical record
o Medication may be prescribed by any physician o Neurological consultation helps comfort levels of primary
care or emergency medicine physician o Plans for consultation should have these plans in place
o The size of the hospital is not a defense o Expected to have a plan for emergency treatment of
stroke

o Organize emergency medical services o Certification of stroke centers
o Primary stroke centers o Comprehensive stroke centers
o Time goals for emergency treatment o Development of regional stroke programs
o Hub-and-spoke system o Drip-and-ship strategy o Use of technologies to increase availability of
neurological expertise o Get With The Guidelines

o First step in stroke management o The time the stroke is most “acute” o Meets the need of early intervention o Matches the approach for MI
o More than just assessment – start treatment o Guidelines proved recommendations
o General emergency care o Hemorrhage or infarction

o 100% use of validated pre-hospital screening tools o Compare to final diagnoses o Use to improve first responder and EMS training o Complete minimum of 2 hours of training/year o Use stroke history checklists
o Assure that response time is < 9 minutes o Dispatch time < 1 minute, travel time same as
for MI o Assure pre-arrival notification of hospitals o Protocols for transfer of patients from non-
stroke hospitals to stroke centers Jauch et al, Stroke 2013

o Assess and manage ABCs o Do not treat hypertension unless directed by physician
o Initiate cardiac monitoring o Provide O2 to maintain O2 saturation > 94% o Establish IV access with saline
o Do not give excess volume of fluid o Do not administer glucose-containing fluids unless patient has
hypoglycemia o Check blood glucose and treat accordingly o Determine time of onset of stroke o Obtain family information, preferably a cell phone
Jauch et al, Stroke, 2013

o Diversion of patients to hospitals that can treat stroke o Emergency medical services o Hospitals that are not ready to treat stroke are bypassed
o Regulations that route patients with acute stroke to primary stroke centers or stroke-ready hospitals o Initiated in 2000 in Alabama and Texas o End of 2010: 16 states and regional areas in 3 additional states
o Covered population o 2000 4,471,933 1.5% o 2010 164,705,389 53%
o Efforts continue to expand this system Song & Saver, Stroke, 2012; 43: 1975

o Recognize the wide range of EMS programs in the state of Iowa o Full-time paramedics o Part-time, unpaid volunteers
o Levels of expertise and experience vary o Reflect numbers of patients with stroke seen
o Develop programs that will provide core information to EMS directors and personnel
o Key features o Recognition of stroke manifestations o Early stabilization and obtain key history o Prompt notification and transport to stroke-ready hospital

o Recognize the common neurological findings o FAST – face, arm, speech
o Obtain key historical information o FAST – time of onset of symptoms (last normal) o Medications or other recent illness o Cell phone # of next-of-kin or family member
o Stabilization o As with other critically ill people
o Emergency transport o Bypass a hospital that cannot treat patient
o Notification of stroke ready hospital – Code Stroke Jauch et al, Stroke, 2013

o Hospitals that have the capability to give emergency stroke care o Focus on care in emergency department o Communication closely linked to EMS o Rapid evaluation and treatment of stroke o Administration of intravenous thrombolysis o Communities across the United States
o Protocols in place o Certified by Joint Commission or states o Another group of hospitals – stroke capable

o Integrated between smaller and larger hospitals o Hub-and-spoke system
o Increase availability of neurological expertise o In person, telephone consultation, telemedicine
o Develop protocols that can be used in community hospitals o Emergency evaluation o General emergency treatment o Administration of intravenous rtPA o Drip and ship (emergency transfer to larger hospital)
o Increase the number of patients treated with rtPA

o Develop stroke care protocols for the network o Used at both the hub and spokes o Emergency diagnostic studies and therapies o Indications for evacuation to the hub o Returning the patients back to the community
o Professional educational programs o Physicians and hospital personnel o Emergency medical services personnel
o Public educational programs o Coordinate research

o Emergency Medical Services o Treat stroke as a level 1 emergency o Dispatchers and rescue services o Emergency assessment, transportation and notification
o Primary Stroke Centers or Stroke-Ready Hospitals o Protocols for emergency management of stroke o Potential collaboration with comprehensive center o Community outreach programs o Public education, health screening and stroke prevention o Maintaining continuity of care

o Limited neurological coverage in most small to medium sized communities o Non-availability of a neurologist o Even less availability of a vascular neurologist
o Develop close links with a comprehensive stroke center o Crucial time lost during transfer to center o Treatment started locally
o Choices o Telephone consultation o Teleradiology o Telemedicine (telestroke)

o Nationwide inpatient sample o 22,243 patients treated with IV thrombolysis o 4,474 patients treated using drip-and-ship approach
o 81% referred to teaching hospitals o 7% had subsequent endovascular treatment
o States using drip-and-ship had higher rates of use of thrombolytic therapy o 5.4% vs. 3.3% (p < 0.001)
o Outcomes (home and self care) o Drip-and-ship vs. primary emergency department o Odds ratio 1.198 (95% CI 1.019-1.409, p = 0.028)
Tekle et al, Stroke, 2012; 43: 1971

o Hospital plan to respond to a patient with acute stroke o Coordinate emergency assessment and treatment o Emergency alerts to the code stroke team o Emergency department is usual site for treatment
o Development of a code stroke toolbox o Initial assessment including orders and laboratory
supplies o Screening assessment for stroke and rtPA o General emergency management o Stroke-specific management and availability of rtPA

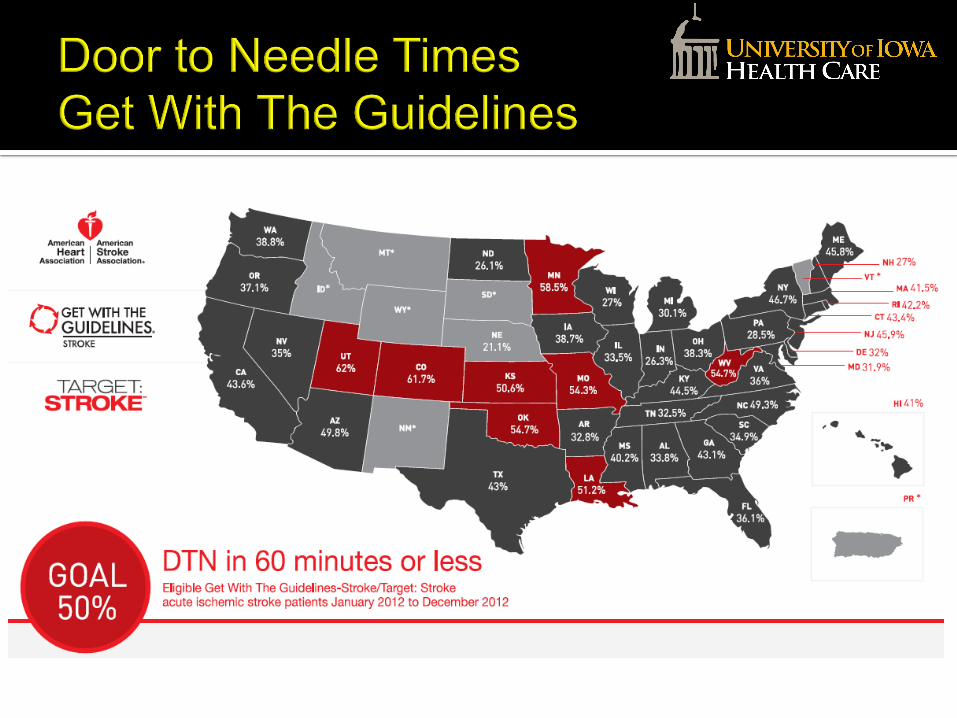
o Based on Brain Attack Recommendations o Door-to-needle time 60 minutes
o First contact in the emergency department o Clinical assessment and diagnosis o Results of diagnostic studies o Decisions about treatment o Starting bolus dose of rtPA
o Results of diagnostic studies 45 minutes o Time of arrival to hospital o CT, laboratory, and ECG

o Are the neurological symptoms due to stroke?
o Is the stroke hemorrhagic or ischemic?
o Are there acute medical or neurological complications that affect early treatment?
o Is the patient eligible for intravenous thrombolytic treatment?

o Hemorrhagic stroke o Seizures with post-ictal signs o Migraine (may or may not have headache) o Metabolic disorder
o Hypoglycemia o Occult trauma o Intracranial mass
o Subdural hematoma o Tumor
o Somatization disorder

o Sudden onset of focal neurological symptoms o Usually maximal at onset o May wax and wane or slowly progress
o Signs should fit within a defined vascular territory o Cerebral hemisphere – hemiparesis, sensory loss, visual
field defect, aphasia, neglect o Brainstem/cerebellum – ataxia, cranial nerve palsy,
dysarthria, bilateral motor signs, crossed signs o Rarely associated with loss of consciousness o Approximately 20% of patients have headache o Nausea and vomiting occur with brainstem or
cerebellar infarction

Consciousness 0 - 3 Orientation 0 - 2 Commands 0 - 2 Gaze 0 - 2 Visual fields 0 - 3 Facial paresis 0 - 3 Arm motor (x2) 0 - 4 Leg motor (x2) 0 - 4 Limb ataxia 0 - 2 Sensory 0 - 2 Language 0 - 3 Dysarthria 0 - 2 Inattention 0 - 2
Brott et al, Stroke. 1989; 20: 864-70.

0%10%20%30%40%50%60%70%80%90%
100%
0-3 points n = 170
4-6 points n = 409
7-10 points n = 323
11-15 points n = 205
16-22 points n = 103
23+ points n = 059
excellentgoodpoordead
Adams Jr HP, et al. Neurology. 1999;53:126.
Impact of NIHSS Scores on Outcomes

o Brain imaging o May be either CT or MRI o CT generally more readily available in community
hospitals o Quick, non-invasive, and relatively inexpensive o Gives key information for emergency care
o Electrocardiogram o Complete blood count and platelet count o INR and aPTT o Cardiac enzymes, renal studies, glucose o Pulse oximetry


o Similar to other acutely and seriously ill patients o ABC of life support
o Airway protection if decreased consciousness or brainstem dysfunction
o Oxygen supplementation not needed unless hypoxic o Monitor vital signs and neurological status o Intravenous access with normal saline o Treat fever and look for source of fever o Treat serious cardiac arrhythmias o Symptomatic treatment – pain, nausea,
agitation

o Elevations in blood pressure common – underlying risk factor, stress, physiological response for perfusion
o Management is controversial because of lack of clinical trial evidence
o Aggressive lowering of blood pressure is not recommended because of risk of worsening of stroke
o Need to lower blood pressure to treat rtPA o IV administration of short-acting medications
o Labetalol, nicardipine, apresoline, sodium nitroprusside
Jauch et al, Stroke, 2013

o Approved medical therapy for treatment of carefully selected patients with acute ischemic stroke
o Engine that is driving acute stroke care o Improve neurological outcomes o May “cure” patients o Efficacy is time-linked o Cannot be given with impunity – does cause
bleeding o Effective therapy of limited usefulness because
too few patients are being treated

Pooled analyses of clinical trials
Time Odds of Favorable Outcomes < 90 minutes 2.55 (1.44 – 4.52) 91 – 180 minutes 1.64 (1.12 – 2.40) 180 – 270 minutes 1.34 (1.06 – 1.68) 270 – 360 minutes 1.22 (0.92 – 1.61) Lees et al, Lancet, 2010; 375: 1695

o IV administration of rtPA is recommended o 0.9 mg/Kg (maximum dose is 90 mg) o 10% as bolus, remainder infused over 1 hour
o Carefully selected patients < 3 (4.5) hours o Can be associated with side effects
o Overall risk of bleeding is 6%, higher with severe strokes
o Does not increase mortality o Uncommon risk of angioedema
o Success in clinical settings is similar to that achieved in trials
o Success is linked to compliance with guidelines Jauch et al, Stroke, 2013

o Goal remains to treat as quickly as possible o Expansion of time window from 3 to 4.5 hours o This expansion in time not approved by FDA
o Require a similar study in the US o Dosage of rtPA and ancillary care similar o Some differences in criteria for treatment (3 – 4.5
hours) o Age less than 81 o Maximum NIHSS score – 25 o Diabetes and history of prior stroke o Warfarin use (regardless of level of INR)
Del Zoppo et al, Stroke, 2009; 40: 2945 & Jauch et al, Stroke, 2013

o Impact on the numbers treated is relatively small o Approved by European Regulatory Authorities o Not approved by FDA
o Did not find the data compelling o Requested another study in the US o Such a study is not likely to be done
o Marketing of the medication for this indication o Influence CMS decisions about reimbursement for
treatment in time window o Guidelines continue to recommend the
administration of rtPA up to 4.5 hours after onset of stroke
Wechsler and Jovin, Stroke, 2012; 43: 2517

o Did the stroke happen in the last 3 – 4.5 hours? o Stroke upon awakening or unwitnessed stroke o Minor symptoms with subsequent worsening o TIA followed by a second (new) event
o Remember the difference in criteria for those treated < 3 hours and those treated 3 – 4.5 hours
o If the stroke is > 3 hours but < 4.5 hours o Age must be < 81 for treatment in 3 – 4.5 hours o No age restriction for treatment < 3 hours

o Any co-morbid disease or recent illness that could be associated with a high risk of bleeding complications? o History of prior cerebral hemorrhage o Recent stroke or myocardial infarction o Recent major trauma or surgery o Recent major bleeding
o Is the patient taking oral anticoagulants? o If taking warfarin, do not treat in 3 – 4.5 hours o If taking warfarin, treat in < 3 hours if INR is < 1.8 o Aspirin, clopidogrel, dipyridamole, ticlopidine o Safety with use of thrombin or direct Xa inhibitors is
not known. Interim plan: not to treat if drug was given < 48 hours

o Are baseline coagulation tests normal? o Primary issue is anticoagulant use or a history of bleeding o Abnormal coagulation tests preclude treatment o Tests take time to perform and may treat in some instances if
tests are delayed o Finger stick test for INR o Prolonged aPTT as a marker for dabigatran effect
o Is the patient a diabetic and has a history of a previous stroke? o May treat < 3 hours but not in 3 – 4.5 hour time period
o Is the patient taking an ACE-inhibitor? o Not a contraindication o May be associated with increased risk of angioedema

o What is the score on the NIH Stroke Scale? o No minimum score for treatment o Mild stroke may worsen subsequently o Composition of score may influence decision o A patient may be disabled despite a low score
o No maximum score for treatment < 3 hours o Use caution with very severe stroke o Higher risk of bleeding complications o No increase risk in mortality
o Maximum score for treatment in 3 – 4.5 hours o NIHSS score < 25

o What are the findings on brain imaging? o Presence of a hemorrhage – contraindication o Stroke appears to be older than 3 – 4.5 hours o Very large ischemic lesion is detected o Presence of a dense artery sign – usually a severe stroke
o Are the patient/family aware of risks of treatment? o Overall risk of symptomatic bleeding is approximately 6% o Hemorrhagic transformation of infarction or hematoma o Risk of bleeding greater in patients with severe strokes o FDA approved therapy and guidelines available

o A number of variables have identified those patients at the highest risk for bleeding following intravenous thrombolysis o Elderly, severe strokes, elevated glucose, serious
comorbid diseases, cardioembolism o None of these variables is an absolute
contraindication to treatment o Many of these variables also portend a poor
outcome without treatment o The presence of multiple “risk factors” for a
hemorrhagic complication should lead to a careful discussion with the patient and family about the risks and benefits of treatment

o Close observation and monitoring during first hours o Neurological status o Blood pressure and vital signs
o Aggressively treat arterial hypertension o If systolic > 180 mm Hg or diastolic > 110 mm Hg o Parenterally administered, short-acting medications
o Delay placement of devices associated with bleeding o Nasogastric tube o Bladder catheter o Central venous line

o Stroke now is being treated as the emergency it is o Requires coordination and collaboration
o Public o All components of the health care system o Government and third-party payers
o Need to address hurdles to early treatment o Each community or region has its own issues to address o Overcome these hurdles with careful and proactive
planning

o Likely will have new interventions for treating stroke
o Combinations of interventions o Thrombolysis and neuroprotective agents o Intravenous and intra-arterial interventions o Adjunctive use of antithrombotic agents
o Improved selection of patients for specific therapies o Treatments that could be started in ambulance or
helicopter o Regardless of advances, the success of future
stroke treatment will remain time-linked and time-limited