doctors in training - sma physics dr shaun ho shares why he was drawn to the specialty 30 dummies’...
TRANSCRIPT

On the Shoulders of Giants
Dummies’ Guide to Residency
Residency Programme – Hits and Misses
Vol. 47 No. 7 July 2015
MCI (P) 154/01/2015
Doctors in Training

CONTENTSVol. 47 No. 7 2015
Editorial
4 A Residency in TransitionDr Jonathan Tan introduces the issue
FEaturE
5 On the Shoulders of Giants Prof P Balasubramaniam continues to impart knowledge
PrEsidENt’s Forum
8 Developing Good Habits in Clinical Practice – Part OneDr Wong Tien Hua discusses the importance of starting right
CouNCil NEws
10 Creating Global ConnectionsDr Benny Loo attends the World Medical Association and Junior Doctors Network meetings
12 SMC’s Response to SMA’s Email Query
iNtErViEw
13 Viewpoints on ResidencyFrom those in the GMEC
ExECutiVE sEriEs
18 Workplace Stress Management for DoctorsA/Prof Calvin Fones looks into the matter
oPiNioN
22 To Through-Train or Not? Dr Tan Li Feng writes about the perks of the residency system
24 Residency Programme – Hits and Misses Dr Tan Ming Yuan touches on the impact and challenges
26 From FM Residency to Sports MedicineDr Wang Mingchang reveals his path to sports medicine
28 Radiation Oncology – A Merging of Biology and PhysicsDr Shaun Ho shares why he was drawn to the specialty
30 Dummies’ Guide to ResidencySK Warrior provides some tips
GP mattErs
32 When Doctors SufferDr Leong Choon Kit speaks about the hardships of being a GP
sma Charity FuNd
34 Running for a Good Cause Relive the exhilaration of Pocari Sweat Run 2015
35 Achieving More TogetherSMACF continues to serve the community
ProFEssioNalism
36 Guide to End-of-life Decision MakingDr Anantham Devanand offers advice on how to view this delicate matter
iNdulGE
38 A Journey through Amsterdam and PragueBryan Koh brings us along for the marvels of his holiday
aNNouNCEmENt
21 Inter-Professional Games 2015
40 MCA Online Training Module - Assessment of Mental Capacity under the Mental Capacity Act
CalENdar
41 SMA Events August – October 2015
aiC says
42 One Patient, One Health RecordGPs, read on!
Opinions expressed in SMA News reflect the views of the individual authors, and do not necessarily represent those of the editorial board of SMA News or the Singapore Medical Association (SMA), unless this is clearly specified. SMA does not, and cannot, accept any responsibility for the veracity, accuracy or completeness of any statement, opinion or advice contained in the text or advertisements published in SMA News. Advertisements of products and services that appear in SMA News do not imply endorsement for the products and services by SMA. All material appearing in SMA News may not be reproduced on any platform including electronic or in print, or transmitted by any means, in whole or in part, without the prior written permission of the Editor of SMA News. Requests for reproduction should be directed to the SMA News editorial office. Written permission must also be obtained before any part of SMA News is stored in any retrieval system of any nature.
EDITORIAL BOARD
Editor
Dr Tan Yia Swam
Deputy Editors
Dr Tina Tan
Dr Tan Tze Lee
Editorial Advisors
A/Prof Daniel Fung
A/Prof Cuthbert Teo
Dr Toh Han Chong
Members
Dr Jayant V Iyer
Dr Natalie Koh
Dr Leong Choon Kit
Dr Jipson Quah
Dr Jonathan Tan
Dr Jimmy Teo
EX-OFFICIOSDr Wong Tien Hua
Dr Daniel Lee Hsien Chieh
EDITORIALOFFICE
Senior Manager
Sarah Lim
Editorial Executives
Sylvia Thay
Donna Cheong
ADVERTISING AND PARTNERSHIP
Li Li Loy
Denise Jia
Tel: (65) 6223 1264
Email: [email protected]
Publisher
Singapore Medical Association
2 College Road
Level 2, Alumni Medical Centre
Singapore 169850
Tel: (65) 6223 1264
Fax: (65) 6224 7827
Email: [email protected]
URL: http://www.sma.org.sg
UEN No.: S61SS0168EPhotosiStock: 24, 30, 31; Shutterstock: 1, 22, 32, 36

7EDITORIAL
By Dr Jonathan Tan, Guest Editor
“the world is changed…”The merits of the residency programme were the subject of much debate when it was first proposed and
implemented. Would these shorter training programmes with controlled working hours lead to less clinical exposure
and less proficient specialists? Were these new-fangled trainee evaluation forms and feedback sessions truly
necessary? There was much skepticism at first, but one should not judge a tree before seeing its fruits. Perhaps now,
with most of the residency systems in full swing and the first batches of senior residents coming off the production
line, we can take stock of the brave new world of postgraduate medical education in Singapore, a system in transition.
“i feel it in the water. i feel it in the earth. i smell it in the air.”To truly understand a new country, one needs to get one’s boots on the ground. In this edition, we speak to two
groups of people: those who have moulded and nurtured the new residency programmes and the first products
of this far-eastern graft of the Accreditation Council for Graduate Medical Education. I had the privilege to
practise in the departments of the four professors interviewed in this edition and they have kindly agreed to share
their views on their past experiences, the present changes they have effected and their hopes for the residency
programme in the future. I would like to thank Asst Prof Alfred Kow, A/Prof Shirley Ooi and A/Prof Raymond Goy
for so graciously sharing their thoughts, and needless to say, it was a great privilege to interview my programme
director, A/Prof Joseph Thambiah.
We also invited three senior residents to share their personal views as they transitioned to the next stage of
their professional training. They are Dr Tan Li Feng, a medical student who became a resident directly who is now
both a mother and senior resident, Dr Tan Ming Yuan a former basic specialist trainee in general surgery and now a
chief resident and Dr Wang Mingchang, who is completing his family medicine training and is now setting up a new
sports medicine centre.
“much that once was is lost.”To the casual reader, the single institution centeredness of this edition is immediately apparent, and I apologise
for it. Before the residency system, trainees had the opportunity to rotate to various hospitals around the island,
but in this day and age, I doubt I will have much opportunity to see how orthopaedics is practised outside of the
west of Singapore, and I hope this will in some way explain the lack of interviewees from the other clusters.
The last trainees of the old basic specialist training/advanced specialist training trainees are rapidly exiting, and
soon all will be residency. Or maybe not. Dr Shaun Ho describes to us the training that radiation oncology trainees
undergo, one of the last few specialties not part of the residency programme.
“For none now live who remember it”The Chinese have a saying that one who teaches for a day, is like a father for life. Just as our behaviour reflects
our upbringing, our professional life is a reflection of the training we received. When one watches a surgeon
operate, with every quirk and step, one can hear the echoes of mentors past. In the end, it is my opinion that it is the
people and not the system that makes a good training programme. We should never forget the teachers that make
it all possible. Every specialty has its icons and giants, and perhaps in this time of transition, it would do us good
to speak to someone of great experience, who even after retiring from active practice two decades ago has been
active in educating orthopaedic surgeons in Singapore and the region. A tutorial with Prof P Balasubramaniam
has been the stepping stone to passing the FRCS and MMED for many orthopaedic trainees, and his thoughts on
medical education are well worth hearing.
I hope that as we move into the future with the residency programme, we do not forget the past and those who
have helped brought us to where we are today.
Jonathan Tan is currently an orthopaedic resident at the National University Health System. A dwarf in a department of giants, his hobbies include falling asleep while studying, resubmitting rejected journal articles and trying to not stutter during morning teachings. He is grateful for the opportunity to pursue his dreams and hopes to become a good orthopaedic surgeon and help educate future trainees. He is thankful for the love and support of his parents and fiancée without which none of this would be possible.
A Re
siden
cy in
Tra
nsiti
on
4 • sma News July 2015

7 thE First reaction of orthopaedic
trainees, when faced with the
challenges of passing the MMed
(Orthopaedics) and FRCS (Orth), is to
seek a master to prepare them for the
test ahead.
Prof P Balasubramaniam completed
his training in the UK in 1966, and
then joined the University of Malaya
where he was professor and head
of the orthopaedics department. He
joined the then Singapore University
Department of Orthopaedic Surgery in
1981 and was promoted to professor
in 1984. He served as Vice-Dean of the
Faculty of Medicine, Deputy Chairman
of Medical Board and Director of
Medical Affairs, and retired in 1994 at
the age of 65.
Prof Bala’s retirement marked the
beginning of an annual pilgrimage of
orthopaedic trainees to his home for
tutorials. For the next two decades,
successive batches of trainees would
sit around his dining table, moulded
and hardened for the battles ahead.
Even at 86, Prof Bala is still an
oracle of orthopaedic knowledge; a
tutorial with him is a tour de force
through the breadth of orthopaedics,
leaving the trainees wiser but
chastened by the gaps in their own
knowledge. In this era of Accreditation
Council for Graduate Medical
Education (ACGME) and residency,
Prof Bala is unique, separate from the
structured training programmes; he
has taken it upon himself to educate
the next generation of orthopaedic
surgeons.
on teachingDr Jonathan Tan – JT: When did you
first start teaching?
Prof P Balasubramaniam – PB: I began
teaching when I was 19, after the
completion of my A-levels in Sri Lanka.
I worked as a relief teacher in Botany
and Zoology for nine months before
starting medical school. It was my most
memorable teaching experience, since
it was my first teaching assignment.
I started teaching medical students
while I was a medical officer. My boss,
who was too busy to teach, had told me
to stand in for him. That was back in the
1950s where there were no computers
or PowerPoint slides, and lessons were
conducted with “chalk and talk”.
JT: What is your philosophy on
teaching?
PB: My philosophy on teaching is that
every trainee can be trained. To begin
with, every trainee must be a bright
student, one has to be, to pass medical
school and enter higher orthopaedic
training, and I respect that. My style
of teaching has always been to impart
knowledge; the trainees do not need to
know anything at first, but if you impart
your knowledge and set them on the
right track, they will eventually become
good orthopaedic surgeons.
I believe in imparting three things
to my trainees: knowledge, skills and
attitude. I do not just teach from a
textbook, but I also teach based on
my personal experience and what is
important for the trainees in their daily
practice. Training programmes can
change, but they must impart adequate
knowledge to the trainees to enable
them to function in their daily practice.
[At this point, Prof Bala opened one of his notebooks to show me the handwritten notes and illustrations he had prepared beforehand. I could not help but be impressed by the dedication it took to update and compile this set of notes every year for a new batch of trainees.]
I place equal importance on all
clinical skills – at the bedside, in the
clinic and in the operating theatre.
Maintaining proper clinical records
is as important as good clinical work,
because it allows you to learn from
your mistakes and to evolve as a
clinician.
Attitude is part of the unspoken
syllabus, something that you impart
FEATuRE
On the Shoulders of Giants – An interview with Prof P BalasubramaniamConducted by Dr Jonathan Tan, Guest Editor
July 2015 sma News • 5

by personal example to your trainees.
Orthopaedics is not just cutting and
doing.
[Every department has its unspoken culture and some elements of Prof Bala’s influence still permeate mine, even 20 years after he has left. In the same way, the surgical style of each consultant silently reveals his or her past mentors. My department’s culture too speaks of the time when he was still a part of it.]
surgery and orthopaedicsJT: What do you think is the best
way to teach someone to be a good
surgeon?
PB: I believe that surgical trainees
need to operate at least twice a
week. When I was operating, I used
to operate on one side of the spine
and let the trainee operate on the
other. As their experience increases,
I allowed them to work on more and
more of the case. Eventually, I let
them operate alone while I remained
outside the operating theatre, so
that they could consult me if they
needed help.
[A/Prof J Thambiah, my programme director, still speaks fondly of how, at the end of every spinal operation, Prof Bala would instruct him to draw by hand the
vertebrae that he had operated on and colour in the areas that he had removed. It made him a better surgeon and artist, too!]
JT: What do you think is the biggest
change in orthopaedics since you first
started practicing?
PB: In orthopaedics, the volume of
knowledge has increased to such
an extent that most surgeons are
unable to cope. Orthopaedic surgeons
are increasingly subspecialised
and interested only in their areas
of subspecialisation. However, I
maintain a broad interest in the
whole body; it is difficult to do so, but
if one understands the whole body,
one is able to see how the different
subspecialties meet and thus better
understand the patient.
Personally speakingJT: What have you gained from your
years as a teacher?
PB: The most important thing I have
gained is the personal satisfaction of
being able to pass on knowledge to my
students, being able to influence them,
change the way they practise and
ready them for their profession.
JT: Do your students still keep in
touch with you?
PB: Yes, they do! Occasionally, one of
them would call up or invite me out
for a meal. However, I have lost touch
with some of them as their practices
and families grow.
JT: Besides teaching, what do you do
in your free time?
PB: I enjoy going for walks to the
market or shopping centre. These
walks give me much pleasure, as
I enjoy looking at new faces and
watching people interact.
In my younger days, I used to
enjoy cooking. I used to tell my wife
to give me a free day so that I can
cook. Of course, she was a much
better cook then I. When she passed
away, I woke up every morning to
cook for my children, so that lunch
would be ready when they returned
from school, but my maid does not
like it when I interfere in the kitchen,
so I have stopped cooking.
[Prof Bala’s wife, Ratnadevi Desilva, had a reputation for being an excellent cook. The prospect of a good meal was something every trainee looked forward to after spending hours re-editing a manuscript with Prof Bala. She passed away in 1984, and since then, Prof Bala has balanced the responsibilities of being a professor of orthopaedics and both a father and a mother to his three children. He is now a grandfather and his children have pursued successful careers overseas in the medical and educational fields.]
some thoughtsIt has been a great privilege
for me to interview Prof Bala and
to hear his thoughts on educating
orthopaedic surgeons. It has been
said that teaching is one of the paths
to immortality, as those who inspire
and educate are never forgotten. As
we move into the brave new world
of residency and ACGME, it would
behove us to remember the giants on
whose shoulders we stand.
Prof Bala celebrating his birthday with a group of students
6 • sma News July 2015

LIFE IN PIXELSSMA NEWS PHOTO COMPETITION
The winner of each theme will take home $50 in CapitaVouchers, a Crumpler camera bag and a Canon Digital Ixus lanyard
with 16GB thumbdrive. The winning photos will also be featured in the pages of SMA News and on the Life in Pixels website.
What’s more, winners of each theme are eligible for a finale readers’ voting contest and stand to win the grand prize, a DSLR
EOS100D Kit sponsored by Canon!
Wait no more and send us your best photos along with your name and MCR/matriculation number at lifeinpixels@sma.
org.sg, with the name of the theme as email subject. All images must be in JPEG format, and sized to at least 2,480 x 3,508
pixels. Include a short descriptive legend (maximum 20 words) with each picture.
This contest is open to SMA members in good standing only. Before submission, check out the contest details at
https://www.sma.org.sg/lifeinpixels.
Calling all photography enthusiasts! To celebrate Singapore’s 50th year of independence, we have released a series of themes which reflect the richness of life on this little red dot.
theme* Closing date release of results
1. “Singapore by Night” – capture the bright lights of our city after the sun goes down
13 September End September
2. “Nation Building” – a play on words: members of the pioneer generation and buildings of historical significance
15 November End November
*SMA will be holding relevant photo workshops in conjunction with each theme. For more info, go to http://goo.gl/6Wg3mv.
In celebration ofOrganised by Imaging partner

PRESIDENT’S FORuM
iN this issue, we focus on doctors in
training. The term “doctors in training”
is interesting to me because, in my
view, doctors never really stop training.
Constant learning and relearning is a
lifelong habit that we develop to keep
ourselves abreast of the changes and
advances in medicine. As doctors,
we want to achieve excellence in our
clinical practice, which is impossible
if we stop learning just because we
have completed a prescribed training
programme.
Aristotle wrote: “We are what we repeatedly do. Excellence, then, is not an act, but a habit.”
Our lives are regulated by habitual
actions, the things that we keep doing
over and over again until they become
automatic. Every morning, we get out
of bed from the same side and stumble
to the washroom to begin our routine.
The amount of toothpaste we use, the
sequence of brushing of teeth, even
the amount of water we fill in the
rinsing cup is more or less consistent.
A cafe manager once told me that the
regular customers who patronise his
establishment typically order the same
item on the menu every time and that
most people like their morning coffee
or tea prepared in a specific way with
very little variation.
Habits are, therefore, very useful
patterns of behaviour that our brains
have developed over time to save
“processing power” and energy. The
term “automaticity” is the ability of
humans to do things without having
to occupy the mind with low-level
details, and we sometimes call this the
“autopilot mode”. In clinical practice, we
often hear doctors commenting that
they carry out their tasks at a “spinal
level”, which means that it has been
repeated so often that the action, akin
to a reflex arc, does not seem to pass
through the brain.
Driving a car is a good example of
automaticity since driving is a very
complex task involving coordination
of sensory and motor function. I recall
my first few driving lessons, where I
struggled in remembering to adjust
the rear view mirror, fasten the seat
belt, ensure that the seat is correctly
positioned and check that the gear
shaft was disengaged – all before even
starting the car. Parking the car was
also a difficult and highly complex
Developing Good Habits in Clinical Practice – Part One
By Dr Wong Tien Hua
Illustration: Dr Kevin Loy
8 • sma News July 2015

process, requiring presence of mind to
note the surrounding traffic conditions
and a sense of direction of the car’s
movement as it reverses into the
parking lot. If the brain is unable to
adapt and develop an automatic neural
pattern to driving, then every driving
trip will be as stressful and emotionally
draining as the first. Thankfully, this
is not the case because we are able to
drive with relative ease, especially on
familiar routes, while listening to the
radio at the same time.
the good, the bad and the uglyAs doctors, we constantly develop
habits in our daily clinical practice.
Some examples of routine tasks
include:
• Communication – Eliciting a clinical
history from patients, addressing
their ideas, concerns and
expectations, and building rapport.
• Clinical examination – Performing
a focused examination and picking
up clinical signs without missing
important information.
• Medical records – Keeping good
and detailed medical records.
• Medical procedures – These include
performing venepuncture, ECG and
infection control procedures such
as proper handwashing.
Good habits can help us work more
efficiently and effectively. The fact that
doctors are able to excel in every test
and examination, leading to a medical
degree, testifies to our good habits of
discipline, determination and effective
time management.
Good habits in communication
help to establish rapport with patients
and maintain an effective doctor-
patient relationship. Maintaining a
high standard of hygiene and infection
control is a good habit that has a
direct impact on patient safety and
public health. A seasoned medical
officer who can insert an intravenous
cannula smoothly into a neonatal vein
seemingly without thinking is only able
to do so through repeated practice and
the forming of habitual reflexes.
Bad habits, on the other hand, are
professional landmines lying in wait to
sabotage our practice even when we
have the best intentions.
Seemingly innocuous bad habits
such as poor handwriting may lead
to errors that can have serious
consequences to patient safety and
clinical care. In prescribing medicine,
a wrongly placed decimal mark
translates to an incorrect dosage
by a factor of at least ten times. Bad
habits in communication can lead to
misunderstandings with patients and
consequently, dissatisfaction with
the consultation process. We know
the importance of maintaining eye
contact and practising active listening
in patient communication, but the
realities of a busy clinical environment
with computers, phones and other
equipment competing for our attention
can be distracting for the doctor.
Habits form not only in individuals
but also within teams and larger
organisations. For example, as doctors
we work in teams that are part of larger
medical departments or units within a
hospital. How an individual interacts
with others often forms habitual
patterns and result in what we call
“organisational culture”. When there
is poor teamwork or safety culture,
or when team leaders foster a hostile
work environment, communication
may break down, and this can cascade
into catastrophic events that end up as
horror stories in the newspapers. The
accumulation of collective bad habits
can thus snowball into something
rather ugly.
Two recent Singapore Medical
Council cases of wrongful
administration of drugs highlight the
importance of individual responsibility
and the role of teamwork. The first case
was that of a young medical officer
who was censured for administering
chemotherapy intrathecally instead
of intravenously because she failed to
check the route of administration at the
bedside. Such an error could have been
avoided if the steps of administration
were followed and hardwired into
a mental routine. The second case
was that of a cardiothoracic surgeon
who gave undiluted cardioplegic to a
patient. He was initially convicted of
willful neglect, but a court of appeal
later overturned the ruling. The
judges noted that in this case, there
was systemic failure at play, which
contributed to the error. In the above
examples, communication within the
team had broken down and bad habits
were allowed to snowball.
starting rightFor every clinical activity, there is
thus the potential of developing either
good or bad routines. Unfortunately,
our brains do not seem to be able to
distinguish between them; it is as easy
to pick up good habits as it is bad ones,
depending on our frame of mind.
Medical training should not be
confined only to the notion of technical
skill training and accumulation of
medical knowledge. During the course
of our instruction, we are also training
ourselves to develop good habits in
clinical practice. Therefore, we need
to consciously learn good clinical habits
before bad habits seep in and establish
themselves in our subconscious
behaviour. There is no better time to
inculcate a culture of good clinical
habits than at the beginning of one’s
professional career. Senior doctors
have an important role to play as role
models and in setting the standards for
good clinical practice.
For those of us who are keen to
improve our behaviour, change is only
possible if we are aware of how our
habits are formed, as well as what
triggers and rewards fuel them. I will
explore these factors in a separate
article. Watch this space.
Dr Wong Tien Hua is President of the 56th SMA Council. He is a family medicine physician practising in Sengkang. Dr Wong has an interest in primary care, patient communication and medical ethics.
July 2015 sma News • 9

COuNCIL NEwS
i rEPrEsENtEd SMA at the World Medical Association
(WMA) and Junior Doctors Network (JDN) meetings in
Oslo, Norway, from 15 to 18 April this year. It provided me
with a platform to learn the different postgraduate medical
education systems around the world and also speak about
Singapore’s transition to the residency programme.
more about the associationsWMA is an international organisation representing
physicians. It was founded on 17 September 1947 and has
now grown to encompass 111 national medical associations.
The organisation was created to ensure the independence of
physicians and to work for the highest possible standards of
ethical behaviour and care by physicians, at all times.
JDN is made up of junior doctors who are representatives
of the respective national medical associations or associate
members of WMA. It was formed in 2010 to provide a
forum for experience-sharing, policy discussion, project and
resource development on issues of importance to junior
doctors, such as postgraduate medical education, their well-
being and the healthcare workforce.
my experienceJunior doctors from all over the world, including
America, Canada, Spain, Brazil, Turkey, Germany, Nigeria,
Japan and Singapore attended the JDN meeting, hosted
by the Norwegian Medical Association. It was an enriching
experience where I gained insights on various training
systems and difficulties faced by the junior doctors of
the respective countries. Many of the issues raised were
surprisingly similar to those of Singapore’s training system,
such as the appropriate amount of duty hours (and the
challenge of not exceeding it), influx of foreign-trained
doctors and support of junior doctor representations in
national medical bodies (such as postgraduate training
governing groups).
I also realised that the limitations of one system could
be the ideal for another. For instance, the Singapore
system is packed with multiple examinations including
the exit examination (which is a requirement for specialist
accreditation). The lack of an equivalent examination in
more established medical systems, such as the Norwegian
one, was deemed by some to be an inadequacy in ensuring
Creating Global ConnectionsText and photos by Dr Benny Loo
10 • sma News July 2015

the good quality of specialists trained. This, however, does
not necessarily mean that poor specialists are produced as
it governs the trainees through the training programme and
constant guidance by their supervisors.
The other lesson I learnt was the luxury of being part
of Singapore’s relatively younger medical training system.
We enjoy a robust training system with the benefit (and
burden) of integrating two medical systems and we never
had to fear the collapse of the training infrastructure. The
harsh reality faced by our compatriots in Nigeria is the lack
of investment in medical training from the government and
they are constantly fighting for the survival of their residency
programme. The Nigerian delegates were duly awarded the
best country presentation after sharing with us the grim
plight of their training system.
Thereafter, for the next three days, I observed the WMA
meeting where many issues ranging from membership,
ethics, socio-welfare to education were enthusiastically
discussed. It was a great learning experience as multiple
countries came together to debate for the better cause of
mankind. Issues discussed included environmental health,
support to street children and chemical weapons – which are
fortunately not experienced in Singapore. These problems
faced by many developing, and even some developed
countries, further validated Singapore’s achievements
in 50 years. WMA has also formed closer ties with other
international bodies such as World Federation for Medical
Education and gained more impact in international health
(as evidenced during the Ebola outbreak). I believe that
Singapore will be able to play a bigger role as WMA
continues to strive for better healthcare across the globe.
This experience has broadened my mind on international
healthcare and medical training and I feel very glad to have
met many like-minded friends. I look forward to participation
in future JDN and WMA activities.
Dr Loo is currently training as a senior resident in paediatric medicine at KK Women’s and Children’s Hospital. He likes to look on the bright side of life and always strives to balance his work, family and personal duties.
Clockwise from far leftDr Loo (third from left) with participants of JDN with Dr Xavier Deau (President), Dr Mukesh Haikerwal (Chairperson of Council) and Dr Otmar Kloiber (Secretary-General) of wMADr Loo explaining the Singapore health system and residency programmePhoto taken with Dr L Kayode Obembe (President of Nigeria Medical Association) and Nigerian delegatesGroup photo with the JDN participants
July 2015 sma News • 11

SMC's Response to SMA's Email QueryoN 15 May this year, Dr Daniel Lee wrote an email query letter to the Singapore Medical Council (SMC)
Executive Secretary, on behalf of SMA, enquiring about doctors’ participation in websites that list doctors’
details and services. We herein reproduce the email query and SMC’s response in full.
15 may 2015 sma’s email to smC Executive secretary
Dear Ms Tan,
SMA has been informed by some members that
doctors’ details have been made available through websites
apparently offering appointment services (eg, https://www.
docdoc.sg/, https://www.practo.com/) whether by direct
registration, or by the site entering the details without the
doctor’s permission.
We would like to ask if SMC would consider that the
doctor has contravened the SMC Ethical Code and Ethical
Guidelines if he participates actively, or if he is merely listed
on the website without his expressed agreement.
Yours sincerely,
Dr Daniel Lee
Honorary Secretary
Singapore Medical Association
smC’s reply
Dear Mr Lee,
We refer to your email dated 15 May 2015 enclosing an
email from Dr Daniel Lee.
The email in question raises the matter of whether
there has been a contravention of the Ethical Code and
Ethical Guidelines (ECEG) by active involvement in either
of the two portals listed. As is the case with advertising on
any platform, the concern would be more on the quality
and standards of information than the availability of the
platform itself. For that reason, to the extent either portal
provides only factual information on the doctors (eg, factual
information on the specialisation of a doctor, contact
details and opening hours), this is unproblematic as the
ECEG explicitly allows factual information on doctors to
be provided to the public (Sections 4.4.1 and 4.4.2 of the
ECEG).
However, where the doctor actively provides
information that can be used in a misleading fashion, or
otherwise participates actively in any website that they
know may use such information in a manner which is
comparative in nature, or would otherwise be used in a
manner inconsistent with the principles set out in Section
4.4.1, such acts may amount to a contravention of the ECEG.
Though not exhaustive, this would include the provision of
special discounts, or gifts, or any other financial incentive
to the patient for using such platform, or involvement in
platforms where testimonials are used as part of a doctor’s
listing or advertisement. Furthermore, while paying for
advertising one’s practice is allowed, the ECEG disallows
doctors from being involved in “fee-sharing” arrangements
with third parties, including such websites.
On those fronts, it would appear to us that participation
in a directory-like structured website is not inappropriate,
while active participation in any website providing
“ranking-table” like frameworks (based on parameters
that may not be objectively based on factual matters),
where doctors can be involved in special “promotions” or
provide other inducements for use of services or where
patient testimonials are utilised, may contravene the ECEG.
As it may be inappropriate for us to make determinative
pronouncements on individual websites, especially in the
absence of a complete understanding of the website’s listing
methodologies and their financial arrangements (if any)
with the medical community, doctors may wish to consider
for themselves how the application of such principles might
apply to each of these websites.
Kind regards
Selven Sadanadom
Deputy Head (Corporate Communications),
Administration Division
Singapore Medical Council
COuNCIL NEwS
12 • sma News July 2015

it has been almost five years since the residency programme was introduced to Singapore’s healthcare
landscape. Just how different is the residency programme from the previous system and what is its impact on
the residents? We interviewed four professors who are actively involved in the Graduate Medical Education
Committee to find out more about their perspective on the programme.
a/Prof Joseph
thambiah
is a senior
consultant and
head of the
Musculoskeletal
Trauma division,
Department of
Orthopaedic Surgery,
National University Hospital (NUH).
He is both a fellowship-trained spine
surgeon and trauma surgeon. A/Prof
Thambiah is actively involved in
undergraduate and postgraduate
education, and has been the
programme director (PD) of the
National University Health System
(NUHS) orthopaedics residency
programme since its inception.
To him, medicine is more than a
profession; he currently leads bi-
monthly medical missions to Batam
and organises weekly mobile medical
clinics that provide free healthcare
to foreign workers and the elderly
poor living in one-room HDB flats.
Now that the first residents accepted into the residency programme have become
registrars, how do you feel their performance compares to that of trainees from the old system?
In my opinion, the performance
of the current senior residents is
equivalent to that of their predecessors.
“
onViewpoints INTERVIEw
Residency
A/Prof Thambiah (second from left, standing) posing at the photo booth
July 2015 sma News • 13

“
One of the pluses of the residency
programme is that we have a clear
idea of the quality of work expected
from the residents when they turn
registrars. A negative is the decreased
amount of time spent gaining
experience due to the regulation of
duty hours, though this is balanced by
a reduction in resident fatigue.
However, whether the residents
have the requisite amount of time to
gain clinical experience and are ready
for greater responsibilities is still a
concern. We try to overcome this by
getting the residents to do tag-on calls
with senior residents and registrars
six months before they become senior
residents themselves. We also make
sure that there is always an additional
level of supervision for them to turn
to. I think one trait of the old system
was that we threw the new registrars
into the deep end and allowed them
to sink or swim; more often than
not, they swam and learned from the
experience, but this is not optimal.
We aim to provide more consistent
training in the swimming process
so that they can keep their noses
above water for far longer. However,
I sometimes worry that this method
may be too much molly-coddling,
and as we all know, too much stress
shielding is not good for fracture
healing!
what do you think are the challenges faced by your residency programme?
When I first started as a
programme director, I thought I was
being punished, since I had to learn the
language of the Accreditation Council
for Graduate Medical Education
(ACGME) from scratch. I had to
complete the programme information
form and go through it word for word,
as the ACGME would fault us if even
a comma was out of place. (Thankfully
I was well trained by my mentor
Prof Balasubramaniam.) The other
challenge was getting the faculty to
accept that the paradigm had shifted
and that the ACGME is the new reality.
Another challenge we face
is contextualising the training
programme for our own national
purposes. With the replacement of the
old training programme, we may have
thrown the baby out with the bath
water, as there was much good that
we could have retained. Personally, I
see no reason why we have to slavishly
follow everything the ACGME requires
of us. We should have the confidence
as a nation to develop our own colleges
for orthopaedics. Scotland, with a
smaller population than Singapore,
has two Royal Colleges of Surgery.
Perhaps, this is what we should aim for
in the future; a national system that
combines the best of both worlds.
We may also be forcing our junior
residents to choose their specialties
too early. Perhaps, there should be a
Ministry of Health (MOH) directive
that all graduates must go through
mandatory housemanship and a year
as a medical officer (MO) before
appearing for interviews. By that time,
they may be better able to make a
sound decision concerning what will
affect them for the next 40 years of
their lives.
Similarly, medical students are
choosing their specialties far too
early. In my opinion, each cohort of
residents should have some degree
of homogeneity in their postgraduate
experience. However, when we select
residents too early on, we may end
up placing an undue amount of stress
on them to catch up with their more
experienced fellow residents. If such
an MOH directive is in place, it may
discourage the various programmes
from “poaching” medical students
early for fear of losing them to other
programmes.
asst Prof alfred Kow is
currently the Assistant
Dean of Education in
Yong Loo Lin School
of Medicine. He is
actively involved in
undergraduate education
in surgery in NUS. In
addition, he is also a core faculty
member of the NUHS general surgery
residency programme. He was
previously the associate programme
director for NHG-AHPL general
surgery residency program at Tan
Tock Seng Hospital and Khoo Teck
Puat Hospital. He is truly excited
to participate in improving surgical
education in Singapore.
Now that the first residents accepted into the residency programme have become registrars, how do you feel their performance compares to that of the trainees from the old system?
Much preparation was put in
place to ensure that the residents
are well supervised and that they
mount the learning curve safely and
smoothly. Simulation training, more
focused on-the-job training, as well
as better organised and intensive
education activities allow the senior
residents to better understand surgical
practices. We also crafted the float
systems to comply with the work
hour restriction and at the same time,
allow the residents more focused
training in emergency surgery. This
has helped them to concentrate their
learning in emergency surgeries (eg,
appendicectomies, hernias, simple
laparotomies). By the time they turn
registrars, they are well prepared
to handle the role. We have also
scheduled them to shadow registrars
on call from as early as the beginning
of the third year residency, to prepare
them to step up to the job when the
time comes. The residents are very
motivated and I am extremely pleased
with their performance. While the
younger senior residents may not be
able to handle complex operations on
their own, the faculty members are
14 • sma News July 2015

readily available to help. That is the
beauty of the training system – ease of
consultation and better supervision.
what are the benefits of the residency programme?
A structured teaching system
with focused outcome is the key to a
successful residency system. It has also
created a pro-teaching environment
for the residents to learn, instead of
a “work-oriented” routine. There is a
great paradigm shift in the mentality
of the trainers and faculty members
as well. Personalised supervision is
an important feature in the residency
system. Mentees can explore their full
potential with the faculty members
and their mentors to gain as much
as possible from the training system.
Work hours are controlled and there
are fewer issues with fatigue in the
residency system. Some may argue
that this might compromise training
quality, but I would say that, if the
system is crafted properly, it should
be a win-win situation for both the
faculty and the residents. Resident
satisfaction is very high (but I hope
it will not lead to complacency and
over-demanding behaviour from the
residents).
what do you think is the future of your residency programme?
It is still a new and evolving system.
We went through some growing pains
in the beginning, but it is now slowly
entering a stable state. The system
should get better as long as the whole
fraternity of surgeons in Singapore
(as trainers and faculty members)
put in effort to make surgical training
better for the next generation of
surgical residents. Of course, this is
only possible with the administrators
and leaders in MOH working hand-in-
hand with the faculty members on the
ground.
a/Prof shirley ooi
is a senior consultant
and former chief
of the Emergency
Medicine (EM)
Department
at NUH. She has
been the Designated
Institutional Official (DIO) of
the NUHS residency programme since
2009 and was the chairperson of the
Emergency Medicine Specialist Training
Committee from 2009 to 2011. She has
won multiple teaching and mentoring
awards, with the most prestigious being
the National Outstanding Clinician
Educator Award 2013. She was also
the winner of the National Medical
Excellence Team award in 2011.
how is the training of the current residents different from that which you received when you were a trainee?
It is definitely very different. As
one of the pioneers of EM in Singapore,
there was hardly any structured
training. Though we had guidelines
on what the relevant postings were in
order to qualify for our FRCS (A&E)
exams, we basically rotated from one
posting to another with hardly any goals
or objectives for each of our postings.
There were also no dedicated mentor
or posting supervisor to guide us during
the basic specialist training (BST) phase,
and we depended on opportunistic
learning and tutorials from our seniors
to prepare for our exams. The gaps in
our knowledge were sometimes only
revealed when we were taking the high-
stakes FRCS (A&E) exams in Edinburgh,
as there were no local exams then!
In contrast, the current EM
residency programme is well structured
and administered by a programme
director with 0.5 full-time equivalent
(FTE) protected time and a core faculty
with 0.2 FTE protected time. The
programme is externally accredited
by the ACGME-I, and has a curriculum
with clear goals and objectives. Uniform
training is in place and learning is no
longer left to the “luck” of the trainees.
Each resident has a dedicated mentor
who follows them through the full five-
year period of residency and there are
rotation supervisors as well. Formative
feedback is emphasised so that the
residents know how they are doing.
There are also annual in-training exams
to help residents identify where their
gaps in knowledge are. As the residents
belong to a sponsoring institution
(SI) under the leadership of a DIO
who oversees the Graduate Medical
Education Committee, each SI takes
ownership of its residents’ training.
Another key difference is that the
current EM residents can start their
training as early as in their house
officer (HO) year, whereas we could
“
Dr Alfred Kow and his family
July 2015 sma News • 15

“
start our training only after completing
housemanship.
Now that the first residents accepted into the residency programme have become registrars, how do you feel their performance compares to that of trainees from the old system?
To answer this question objectively,
comparison should be made between
similar scenarios. For residents who
enter the EM residency as MOs, the
product is just as good, if not better.
This is because the training that they
receive is more comprehensive and
holistic. Residents who entered the
EM programme as HOs should not be
compared with the registrars during
my time; who at the earliest would have
been in their fifth or sixth postgraduate
year. Rather, they should be compared
to their peers of
equivalent clinical
experience in the
previous system
whose performance
they definitely
surpass.
As a DIO, I
have asked senior
clinicians from
different specialties
about how they
view the current
senior residents
compared to the
registrars from the
former training system. Unanimously,
they concurred that these senior
residents, although more junior in
terms of age, are just as competent. In
fact, one senior clinician opined that
current senior residents can function
at a level that is one year ahead of
previous ASTs! They also felt that the
competence level of the residents as
a whole is more uniformed compared
to the past. Previously, there were
excellent and motivated ones who
were able to fend for themselves, but
there were also those who were very
weak even after they exited from the
training programme. They attributed
this improvement to a better selection
system, a more structured programme
and the closer monitoring given. In
addition, the senior residents have
demonstrated better pass rates in their
exams.
Therefore, despite the shorter
training period, I would still appeal to
those comparing the two systems to
remove the seniority factor from the
equation. Only then can we assess the
real impact of the residency system.
what do you think are the challenges faced by your residency programme?
In the past, trainees were virtually
guaranteed a job upon completion
of their training in a particular
department. In the current situation,
the aim of the residency programme,
as set out by MOH, is for each of the
three SIs to train specialists for the
whole country and not only for their
individual institution. Thus, residents
need to have this mindset or they may
be greatly disappointed!
Allowing residents to start training
as early as their HO year may pose
a challenge, because the experience
of life in a particular specialty as a
medical student may be different
from that as a working doctor. It is
probably better for junior doctors
to choose their specialty after
gaining some working experience. In
addition, nothing beats real clinical
experience. I think a win-win situation
would be a slightly delayed entry
into the residency programme, after
the completion of housemanship,
combined with a well-structured
residency programme. Then, we will
have the best of both worlds!
A/Prof Ooi (centre), as DIO, at her 11th run of the NuHS Residency Orientation at Outward Bound Singapore in July 2015 after completing 18 km kayaking round Pulau ubin with her residents, senior management and faculty!
a/Prof raymond Goy
was the programme
director of the NUHS
Anaesthesiology
Residency Programme
from 2010-2015. He
was awarded the NUH
Teaching Excellence Awards
for three consecutive years
(2012-2014) and the NUHS Residency
Award in 2014. A/Prof Goy firmly
believes that the ACGME-I system
(with appropriate adaptations to the
Singapore healthcare system) is the
best change our Ministry of Health
has made to our postgraduate training
in Singapore. He is passionate about
mentoring residents from all specialties.
Many residents have benefited from his
guidance or received “homework” at
the end of a day in theatre.
how is the training of current residents different from that which you received when you were a trainee?
In the past, anaesthesia trainees
were allowed to plan and dictate
their own BST rotations. This was
advantageous, as it promoted self-
guided learning. Motivated trainees
could pick rotations in hospitals where
subspecialty training was available to fill
up the gaps in their training. However,
this system had several disadvantages.
If a trainee was not cognizant of the
gaps in his training, he may not choose
the appropriate rotations and could
end up with deficiencies in his learning.
16 • sma News July 2015

A/Prof Raymond Goy (first from left) with his pioneer batch of NuHS anesthesiology residents at Outward Bound School
Furthermore, the Medical Officers
Posting Exercise (MOPEX) system
was manpower-driven rather than
education-driven. Even if the trainees
were keen to do the required rotations,
the vagaries of the manpower
requirements and administrative
divide of the different hospitals may
occasionally result in them not getting
their desired postings.
The ACGME-I residency
programme replaces the opportunistic
learning of the BST/AST system. All
subspecialty training in anaesthesia is
now uniformly administered based on
the curriculum and educational needs
of each trainee. With this system in
place, each trainee will get hands-on
experience in the full spectrum of
anaesthesia practice. The elements
of formative resident and faculty
evaluation and feedback are also
enhanced. There are also competency
milestones that the trainees have
to work towards in their route to
specialisation.
Importantly, it is no longer just
about the teaching and receiving of
information. It is also about educators
taking ownership of a resident’s
successes, challenges and professional
and ethical development.
what are the benefits of the residency programme?
The residency programme offers
numerous benefits for the learners,
educators, hospitals and Singapore, if
we are patient and allow the system to
mature.
I believe that the more structured
curriculum and the closer monitoring of
residents will enable us to consistently
produce well-rounded doctors. The
more objective system of evaluations
and feedback also ensures that the
residents are kept abreast of their
progress and allows the faculty to step
in, when needed, to assist them.
We also make sure that the
residents’ feedback on the programme
are heard and acted upon by the
faculty. I particularly enjoyed the
“Meet the Residents” sessions with
my DIO, which allowed us to identify
areas of improvement in the training
programmes, the hospital work
processes and areas that affect patient
outcomes.
what do you think are the challenges faced by your residency programme?
There are multiple challenges,
past and present. These challenges
help make our PDs more resilient and
determined to overcome them for the
sake of their residents.
Current medical students and
young doctors are entering specialty
training earlier and are thus less aware
of the rigours and demands of each
specialty compared to before. Medical
students are placed in an unnecessarily
stressful situation of having to
decide on a career track without the
opportunity of caring for patients
and becoming great doctors first; this
is the so-called “residency rat race”.
My advice to young medical students
and doctors is this – unless you are
certain of your career choice, it would
be prudent to take a step back and try
out new options before embarking on
a residency track; a career has to be
driven by passion not obligation, so take
your time to explore and embark on a
specialty that ignites your passion.
A possible solution is to allow
doctors to apply for residency training
only in the second post-graduation year
so that they would have the opportunity
to rotate through more specialties
as MOs. PDs must have the foresight
and discipline to look at the Singapore
system as a holistic national training
unit and allow applicants to mature in
their outlook before matching them
to the specialty. We must also provide
active career counselling to our medical
students to learn to be good holistic
doctors first before specialist training,
and dissuade them from joining the rat
race before they are ready.
At the same time, the increasing
number of residents in our
programme has led to fewer spaces
available for MOPEX MOs to work
in our department, preventing us
from evaluating their suitability
for residency. We overcame this
by performing swaps with our
participating sites, giving MOs from
their departments the opportunity to
work in our programme to prove their
worth, while our residents spend time
at these partner sites. We hope that
this will give MOs who are not yet
part of the residency programme the
chance to become residents.
July 2015 sma News • 17

EXECuTIVE SERIES
PraCtisiNG mEdiCiNE can
be stressful. Conversations with
colleagues invariably drift to
anecdotes that illustrate how
and why stress is inherent to our
profession. Research evidence also
suggests that doctors are vulnerable
to stress at work and that we are
highly susceptible to the ill effects of
work stress, including an increased
incidence of psychological distress and
psychiatric morbidity.
While we readily endorse its
ubiquitous presence, a simple
definition of “stress” remains
elusive. Broadly, stress refers to
the psychological and physiological
reactions that occur when we perceive
an imbalance in the level of demand
placed upon us versus the capacity to
meet that demand. In the workplace, it
refers to the times when we are simply
not sure if we have what it takes to
meet the challenges faced.
why are doctors stressed?A combination of factors
contributes to why doctors may be
especially vulnerable.
Some personality traits that make
us good as professionals (eg. obsessive,
perfectionistic, conscientious,
approval-seeking) may cause us to
be more prone to emotional distress.
Doctors like to be in control but may
harbour chronic self-doubt.
The nature of the job – long hours
and heavy patient loads – is an obvious
source of stress. At the outset of our
careers, we have learnt to deal with
difficult patients and relatives, often
in hectic and trying environments.
Dealing with issues of death, dying
and suffering may take an emotional
toll. Engaging in the “noble” mission of
Workplace Stress Management for Doctors
By A/Prof Calvin Fones
healing ostensibly makes sacrificing
personal life acceptable, or even
expected. The skewed emphasis
on work may then contribute to
poor family/social relationships and
support.
The types of stress may be
unique to the practice environments.
Doctors in public service may feel a
lack of control over factors like work
schedules or workloads, or having
to cope with a lack of resources.
Dysfunctional workplace dynamics
such as bullying or feeling undermined
or unrecognised are often cited by
doctors in training. On the other
hand, those in private practice may
face isolation, both physically and
psychologically.
Various factors pertaining to
the culture and organisation of the
workplace may also engender more
stress for the doctor working there
(Table 1).
table 1. organisational factors that affect work stress
Lack of autonomy and control
Work schedule (eg, call rosters and clinic schedule)
Work load (eg, patient load and administrative duties)
Lack of resources to work effectively and safely
Manpower constraints
Fear of mistakes and litigation
Risk management
Administrative ineptitude and bureaucratic bottlenecks
Career expectations
Uncertainty about authority and responsibilities
Balancing clinical load, administrative, research and teaching
Unclear/unrealistic targets
Career development/advancement and training opportunities
Job fit
Different personal values from the workplace environment,
(eg, generatinprofessional fees vs financial/social needs of patients)
Congruence with interests, training and skills
Dysfunctional workplace dynamics
Hierarchy
Promotions and recognition
Rivalries and peer pressure
Bullying, feeling undermined and harassment
work environment
Monotonous, routine
Chaotic and disorganised
Safety, workplace violence and risks
Organisational support
When patients complain or threaten litigation
Leave/holiday coverage
18 • sma News July 2015
why does stress matter?Stress in doctors matters because it
leads to “casualties” among colleagues,
including burnout, emotional
exhaustion, disillusionment, a lack of
personal accomplishment, depression,
anxiety and drug/alcohol abuse or
dependence.
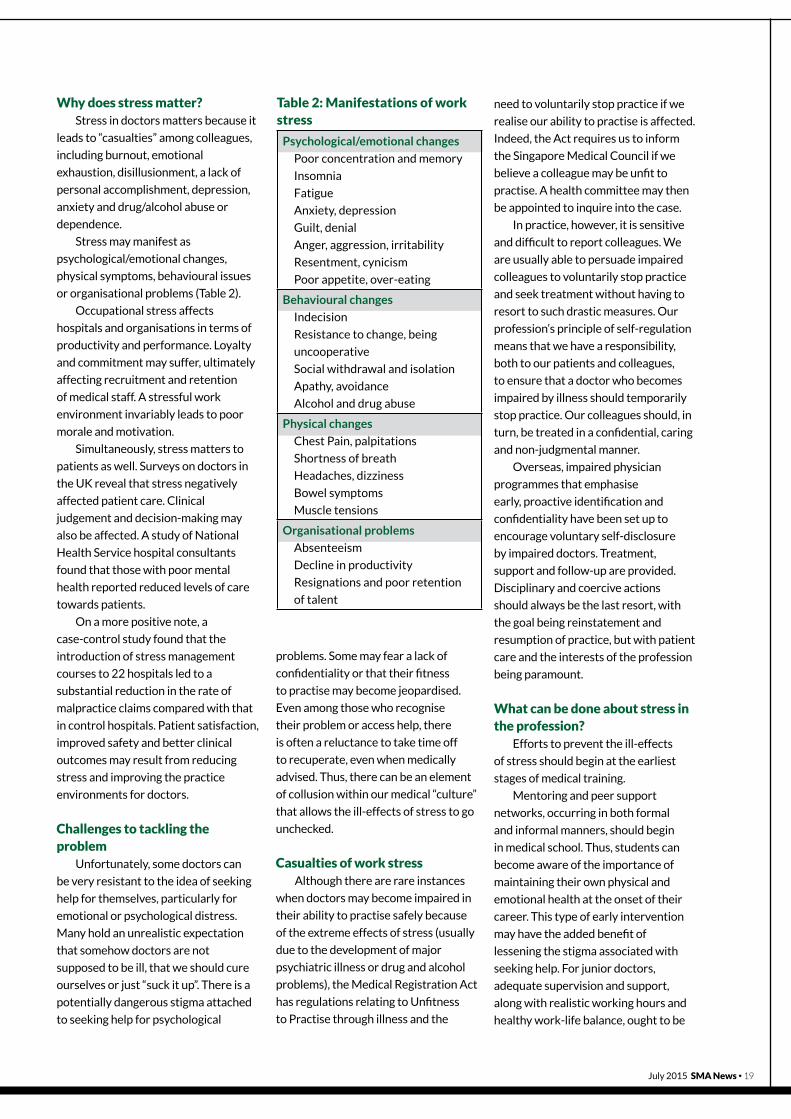
Stress may manifest as
psychological/emotional changes,
physical symptoms, behavioural issues
or organisational problems (Table 2).
Occupational stress affects
hospitals and organisations in terms of
productivity and performance. Loyalty
and commitment may suffer, ultimately
affecting recruitment and retention
of medical staff. A stressful work
environment invariably leads to poor
morale and motivation.
Simultaneously, stress matters to
patients as well. Surveys on doctors in
the UK reveal that stress negatively
affected patient care. Clinical
judgement and decision-making may
also be affected. A study of National
Health Service hospital consultants
found that those with poor mental
health reported reduced levels of care
towards patients.
On a more positive note, a
case-control study found that the
introduction of stress management
courses to 22 hospitals led to a
substantial reduction in the rate of
malpractice claims compared with that
in control hospitals. Patient satisfaction,
improved safety and better clinical
outcomes may result from reducing
stress and improving the practice
environments for doctors.
Challenges to tackling the problem
Unfortunately, some doctors can
be very resistant to the idea of seeking
help for themselves, particularly for
emotional or psychological distress.
Many hold an unrealistic expectation
that somehow doctors are not
supposed to be ill, that we should cure
ourselves or just “suck it up”. There is a
potentially dangerous stigma attached
to seeking help for psychological
problems. Some may fear a lack of
confidentiality or that their fitness
to practise may become jeopardised.
Even among those who recognise
their problem or access help, there
is often a reluctance to take time off
to recuperate, even when medically
advised. Thus, there can be an element
of collusion within our medical “culture”
that allows the ill-effects of stress to go
unchecked.
Casualties of work stressAlthough there are rare instances
when doctors may become impaired in
their ability to practise safely because
of the extreme effects of stress (usually
due to the development of major
psychiatric illness or drug and alcohol
problems), the Medical Registration Act
has regulations relating to Unfitness
to Practise through illness and the
need to voluntarily stop practice if we
realise our ability to practise is affected.
Indeed, the Act requires us to inform
the Singapore Medical Council if we
believe a colleague may be unfit to
practise. A health committee may then
be appointed to inquire into the case.
In practice, however, it is sensitive
and difficult to report colleagues. We
are usually able to persuade impaired
colleagues to voluntarily stop practice
and seek treatment without having to
resort to such drastic measures. Our
profession’s principle of self-regulation
means that we have a responsibility,
both to our patients and colleagues,
to ensure that a doctor who becomes
impaired by illness should temporarily
stop practice. Our colleagues should, in
turn, be treated in a confidential, caring
and non-judgmental manner.
Overseas, impaired physician
programmes that emphasise
early, proactive identification and
confidentiality have been set up to
encourage voluntary self-disclosure
by impaired doctors. Treatment,
support and follow-up are provided.
Disciplinary and coercive actions
should always be the last resort, with
the goal being reinstatement and
resumption of practice, but with patient
care and the interests of the profession
being paramount.
what can be done about stress in the profession?
Efforts to prevent the ill-effects
of stress should begin at the earliest
stages of medical training.
Mentoring and peer support
networks, occurring in both formal
and informal manners, should begin
in medical school. Thus, students can
become aware of the importance of
maintaining their own physical and
emotional health at the onset of their
career. This type of early intervention
may have the added benefit of
lessening the stigma associated with
seeking help. For junior doctors,
adequate supervision and support,
along with realistic working hours and
healthy work-life balance, ought to be
table 2: manifestations of work stress
Psychological/emotional changes
Poor concentration and memory
Insomnia
Fatigue
Anxiety, depression
Guilt, denial
Anger, aggression, irritability
Resentment, cynicism
Poor appetite, over-eating
Behavioural changes
Indecision
Resistance to change, being
uncooperative
Social withdrawal and isolation
Apathy, avoidance
Alcohol and drug abuse
Physical changes
Chest Pain, palpitations
Shortness of breath
Headaches, dizziness
Bowel symptoms
Muscle tensions
Organisational problems
Absenteeism
Decline in productivity
Resignations and poor retention
of talent
July 2015 sma News • 19

“The young doctor should look about early for an avocation, a pastime, that will take him away from patients, pills, and potions…” – William Osler
encouraged. Medical training should
include helping doctors recognise their
own limitations and develop skills to
better track how stress affects their
well-being and professional practice.
what can you do to help yourself?Awareness
Awareness of the sources of
stress and how one reacts to different
stressors is a crucial first step.
Individuals differ in the nature and
intensity of the stress that they are
susceptible to.
Acceptance
Coming to terms with one’s own
vulnerabilities is not always easy. The
stringent standards and rigorous nature
of medical training sometimes inculcates
a distorted message that not pushing
ourselves to the limit amounts to
personal “weakness”.
The competitive nature of medical
school and residency may spill over to
professional rivalry, and this culture of
competitiveness can be a major source
of stress. Striving to be “the best” may
demand a high emotional cost. Perhaps
an attitude more aligned with simply
doing our professional best is healthier,
both for the patients and doctors.
Attitude
Along with the inherent need to
“compete”, certain mental attitudes
serve to perpetuate workplace stress.
The notions of service, sacrifice
and putting the needs of patients
first, which are “noble” attributes of
the profession, may easily become
distorted to unhealthy proportions.
Some doctors, while appearing to
lament their extended work hours and
lengthy appointment lists, may derive
gratification from the same; their
popularity as the most widely sought-
out specialist, therefore, justifies what
is actually an imbalanced and stressful
practice.
Nevertheless, acquiring a healthy
work-life balance is not easy to achieve,
but prioritising the basics of rest,
relationships, relaxation and recreation
go a long way to preventing the ill-
effects of stress.
Stress-reduction techniques include
elements of deep breathing, muscle
relaxation, mindfulness and meditation.
Exercise and physical activity stimulate
the production of endorphins and
counter the deleterious effects that
stress has on the immune system.
Coping stylesHaving negotiated the rigours of
many years of medical education and
training, most doctors would have
developed their own repertoire of
strategies to cope with stress. Their
effectiveness depends on the type of
stressor, the particular individual and
circumstances. There are two types
of coping responses: emotion- and
problem-focused.
Emotion-focused coping
This involves trying to reduce the
negative emotional responses (eg,
fear, anxiety, depression, frustration or
embarrassment) associated with stress.
Emotion-focused coping techniques
include distraction and suppressing
emotions or experiencing them through
talking about how they feel. These
strategies may be ineffective, as they
ignore the root cause of stress or delays
the dealing of the specific problem.
However, it can be a good strategy if the
source of stress is beyond the person’s
control.
Problem-focused coping
This targets the causes of stress
in practical ways by tackling the
problem or situation that is causing
stress, consequently directly reducing
the stress level. These strategies,
which include problem-solving, time-
management and accessing instrumental
social support, aim to remove the
stressor or reduce the cause of stress.
They deal with the root cause, thus
providing a long-term solution. It is
the default strategy employed in our
professional approach to tackling our
patients’ problems. However, it is not
always possible to use these strategies
such as when dealing with loss and
bereavement, which requires emotion-
focused coping.
making the choice of less stress For some doctors, a stressful
professional life has become a
longstanding and deeply ingrained
habit. Others seem resigned to the view
that stress itself is an inevitable part
of life as a doctor. The reality is that
there are proactive choices that we can
make, especially when we realise that
negative effects have already begun
to set in. Making a decision to take the
necessary steps to better manage and
control work stress can be tremendously
empowering. Change may not come
easily, but the patience, persistence
and commitment required would be
worthwhile across all areas of life.
Dr Calvin Fones is a consultant psychiatrist in private practice who assesses patients who are stressed every day. He also listens to stressed colleagues who vent their angst in hospitals’ doctors’ lounges and occasionally helps stressed
medical colleagues in a clinical setting. Not immune to workplace stress himself, he tries to follow the advice he dispenses.
20 • sma News July 2015

Singapore Medical Association
For Doctors, For Patients
at this year’s Inter-Professional Games (IPG) from August to October!
For more than one-and-a-half decades, SMA has joined forces with five other professional bodies,
namely the accountants, architects, engineers, lawyers and surveyors to organise the annual IPG.
If you wish to find out the complete list of games and take part in IPG 2015,
please visit https://goo.gl/5AWUhX.
dr Chia yih woEi
ChairmaN
sma sPorts & GamEs CommittEE
BRING YOuR GAME ON

OPINION
or Not?
i bEloNGEd to the second last
A-Level batch that missed the much
feted through-train scheme by a
whisker. So I thought I should count it
fortuitous to be the second batch to
enter the residency “through-train”
programme.
Much like the A-Level through-
train, the residency “through-train”
has also been greeted with much
controversy. The pros and cons of
either system are bounteous. The
former system was more flexible
(or laissez-faire) and self-directed
(or unstructured); while the new
promised more structure (or greater
bureaucracy) and greater certainty (or
less flexibility).
As I had always wanted to do
geriatrics, it was not a difficult
choice for me to jump onto the kiasu
Singaporean student bandwagon to
sign up for the internal medicine (IM)
residency programme straight out of
medical school. It also helped that IM
was not a complete lock-in either, as
I knew that if I did not find geriatrics
appealing after a while, there were
many other IM subspecialties available
to choose from. In that way, I got the
best of both worlds – a guaranteed
By Dr Tan Li Feng
{
{To Through-Train
22 • sma News July 2015

Li Feng is a first year senior resident from the Department of Geriatrics, National University Health System (NUHS). She first wrote an article for SMA News in 2007 (http://news.sma.org.sg/3905/MedSoc.pdf), in her first year of medical school as
the class representative. In it, she stated that she wanted to do Geriatrics and eight years down the road that is what she is doing today.
training spot and some flexibility for
manoeuvring. I am not sure if other
specialties enjoy this advantage as
well.
However, as IM residents came
to learn soon after, there was also
a price to pay for such flexibility.
Senior residency subspecialty spots
are not guaranteed. The chances of
landing a senior residency spot seem
at times as random as the vagaries
of the wind, dependent on the year
that you are scheduled to apply in
and the competition you face in that
particular cohort. Neither was there
an option of waiting a year to apply in
a less competitive cohort. The budding
cardiologist who daily holds onto his or
her aspirations to get by every arduous
medicine call might very well end up
doing general medicine or being lost
at the end of junior residency, due to
factors that are at times beyond the
resident’s control. Some flexibility
has since been introduced to the
senior residency matching process,
but certainly the promise of turning
consultant in six years upon graduation
is unfulfilled for a selected group of
residents.
Thankfully, I did not have to go
through that disappointment as a
resident. If anything, the residency
system’s certainty and push to “churn
out” specialists helped me move on
despite having my training disrupted
by a happy bundle of joy – the birth
of my son. I am certain that without
the residency programme, I would not
have been able to keep to the schedule
of completing my junior residency
programme within the stipulated 36
months. Thanks to supportive and
enlightened programme directors who
helped mould my schedule in an “infant
residency programme”, I was able to
be matched to my senior residency
programme of choice before I had even
attempted my registrar exams. This
would have been impossible in the
old system. I passed my exams within
months of starting senior residency.
As a new mother, moving on to
senior residency sooner, rather than
later, has certain advantages and was
definitely a factor in my decision to
continue training rather than dropping
out as the light at the end of the tunnel
seems closer within reach. The only
downside so far has been that because
I never got the chance to do any
paediatrics, as breadth of training was
sacrificed for intensity and relevance,
I am no wiser when it comes to little
ailments that my infant gets.
The residency system is assuredly
not for everyone. Unlike the old system
where junior doctors were not given
dedicated guidance, the residency
system benefits some, potentially
at the expense of others, but it can
also ensnare some. It is expeditious
but should not be rashly undertaken.
Perhaps it can be likened to marriage.
If one is ready for commitment,
accommodation, loss of some
autonomy and in-laws (one big, fixed
residency family), then take the plunge.
However, if marriage is undertaken
merely to escape singlehood and not be
left on the shelf, then it is a dangerous
commitment with possibly painful
outcomes for all involved.
Not everyone is suited for marriage,
and not all would enter into one at
the same time in life. But thankfully,
residency is not marriage. It is only one
part of a doctor’s journey. Sometimes
it is a highway, other times a blip or
a detour. But in the grand scheme of
things, what does it matter if you take
six, ten or 15 years to train? It is simply
a matter of perspective – something we
doctors need in all that we do.
...the residency system benefits
some, potentially at the expense of others, but it can
also ensnare some.”
“
July 2015 sma News • 23

24 • sma News July 2015
OPINION
residency Programme – Hits and Misses
By Dr Tan Ming Yuan
loNG hours, busy calls and
punishing schedules – these are some
characteristics often associated with
general surgery training all over
the world. Nonetheless, they are a
necessary evil to achieve craft and
mastery in our field of practice. In
recent times, surgery training, as well
as the specialist training community
as a whole, has undergone a huge
change with the introduction of the
residency programme in Singapore.
What prompted the change was
the success of the US residency
programme and the need to increase
the specialist population in Singapore
to meet the demands of the future.
transitioning from old to newI am part of this transition phase
and am currently witnessing its
evolution. Upon graduation and
completion of my house officer year,
prior to serving my two-year National
Service in the Singapore Armed
Forces, I found myself on the brink of
the transition between the old and
new systems. As a pre-selected basic
specialist trainee traversing into the
new realm of residency and having
experienced both, I was able to see
the differences between these two
unique systems and how the change
has impacted local training.
{ {

Dr Tan Ming Yuan is chief resident with the NHG-AHPL General Surgery Residency. He believes that there is more to life than work and is thankful to have great friends at work, not just colleagues.
“…in order for the residency programme to reach its
full potential, an entire
generation will have to change.”
July 2015 sma News • 25
Residency is a form of graduate
medical training that originated
from the US and took root in the
19th century. Pioneered by Sir
William Osler and William Stewart
Halsted at the Johns Hopkins
Hospital, residency is a formalised
and regulated training programme
that has evolved over the years
to its current state – rigorous
and structured in its training
methodology and outcomes.
With the change from the time-
proven, “survival of the fittest”
basic specialist training/advanced
specialist training system to the
new structured, competency-
based residency system, there is
a push for the implementation of
new pedagogies and education
methods. In addition to the
workload of service provision, the
resident now faces an increase in
number of assessments, in-training
examinations and other demands,
which were hitherto given far
less attention. An all-rounded
resident is expected to perform
well in each of these realms – from
clinical medicine, operative skills to
scholarly activities and involvement
in institutional or national
administrative commitments.
Considering the challengesAlthough the concept and
eventual aim of residency is good,
many would agree that there is
much room for improvement. The
residency programme is still at its
infancy stage of development and
will continue to grow and evolve in
order to meet the challenges of the
future.
Like a cup that is already filled
with water, we cannot continue
adding more water without first
removing some, or else the cup will
simply overflow. Similarly for the
residency programme, we need to
be cognizant about what additional
tasks and aims are added, as well as
where compromises can be made
based on what is relevant and critical
for achieving what is deemed a
competent specialist of the future.
There is also a need for a
paradigm shift in the methods of
administering such a programme.
This starts with the top management
and flows down to the faculty, who
are on the ground mentoring the
new generation of trainees. We
need to rethink the methods that
have served us well in the past and
consider if they are still relevant and
efficient in achieving our targets, or
perhaps we need to embrace a new
methodology.
There has been much flak on
the concepts of restricted duty
hours, protected time for formalised
teaching and in the case of surgical
disciplines, case logs. These concepts
should be viewed not only in its
execution (which may have caused
some inconvenience to individuals
and institutions), but also the intent
and reasons they are in place.
Perhaps, with greater understanding,
these changes may be more readily
embraced.
For a long time, we have assumed
that a doctor is also a teacher, but
this may not be the case. Faculty
must be educators, not just by
chance or talent, but through
nurturing. There is now much
knowledge available on the science
of education, and we should not
ignore the necessary development
of our teachers in this regard. Thus,
the faculty for residency ought to be
trained specifically for this role.
Despite these challenges, I
remain optimistic about the future.
This transition is a good opportunity
to discard some of the preconceived
notions of what used to work, to
shape the training programme
for our future generation, and to
remind ourselves of the importance
of continual evolvement and
improvements. Certainly, there
will be some hits and misses
along the way, but in order for the
residency programme to reach its
full potential, an entire generation
will have to change. We must stay
focused on our mission, which is to
train competent future medical and
surgical specialists who will excel
and surpass their predecessors. Only
when that happens will we have truly
succeeded.

OPINION
why Fm in Nuhs?Family medicine (FM) was not
the initial choice for my first medical
officer posting exercise (MOPEX). I
had applied for anaesthesia but got
a polyclinic posting instead. Though I
struggled with the polyclinic workload,
I found myself enjoying the variety
of cases that spanned different body
systems, age groups and genders,
as well as the continuity of care and
relationships forged with patients.
After rotating through other
MOPEX postings, I realised that shift
work and overnight calls are not for
me. All things considered, I decided
on FM as a specialty. My application
under the old basic specialist training
programme in 2010 was rejected.
Fortuitously, I reapplied the following
year and was accepted into the
inaugural intake of the FM residency.
I chose National University Health
System (NUHS), as it offered a unique
programme, including block postings
to private GP clinics. I was also bowled
over by the sincerity of its faculty,
especially when the programme
director, A/Prof Tan Boon Yeow,
telephoned personally to address my
concerns point-by-point. Later on, the
faculty also supported my intention to
subspecialise in sports medicine.
Fm residency journeyThe inaugural batch of NUHS FM
residents experienced many teething
problems. The learning curve for
inpatient rotations was steep. Even
though the postings were short, the
residents were expected to get up
to speed fast and to perform like
other members of the department
in order to fulfil service needs.
Also, the style of assessment of the
Accreditation Council for Graduate
Medical Education (ACGME) and
the concept of hosting FM residents
were new to most departments,
leading to confusion on the ground
regarding how best to manage our
learning needs. In departments with
high service loads and manpower
shortages, educational needs
sometimes took a back seat and taking
time off to attend FM continuity
clinics and teaching sessions was often
difficult. In 2011, the programme
failed the ACGME audit, leading to
uncertainty over our future.
I am glad to say that all that is in
the past now. The programme has
since gone on to achieve full ACGME
accreditation. Host departments
have also become more mindful of
FM residents’ unique learning needs
By Dr Wang Mingchang
From FM Residency to Sports Medicine
26 • sma News July 2015

and are thus more accommodative
towards us. They also recognise FM
residents’ contribution to their teams,
for instance in ensuring holistic patient
care beyond the focus of a specialty on
a specific organ system or region.
why sports medicine?Having served as an instructor
in the health and fitness club during
my junior college days, I had found
it rewarding to teach about exercise
safety, to give injured students
rehabilitation advice, and to help
others meet their weight loss and
fitness goals. During my university
days, I continued to do so and
cherished the hope that I could
someday incorporate this aspect in my
career.
I first heard about sports medicine
in my second year of medical school,
and subsequently did my electives at
the Changi Sports Medicine Centre
(CSMC) and Singapore Sports Council,
and also served six months as a medical
officer at CSMC. One of the routes to
subspecialisation in sports medicine
was via the Master of Medicine in
Family Medicine examination. This was
a natural choice for me since I have
an interest in both family and sports
medicine.
meeting dr lingaraj Krishna My first rotation in National
University Hospital (NUH) in 2011 was
with the orthopaedics department. At
that time, I did not work directly with
Dr Lingaraj Krishna (current director
of NUH Sports Centre), but he had
found out about my interest in sports
medicine. Three years later, towards
the tail-end of my residency training,
Dr Lingaraj, having been tasked to set
up the NUH Sports Centre, invited me
to be a part of it and I agreed without
hesitation.
building up the serviceDr Lingaraj worked tirelessly
to engage staff within and outside
of NUH, and to put together a
multidisciplinary sports medicine
Dr Wang Mingchang is a family physician and sports medicine registrar with the NUH Sports Centre. He is hydrophobic but is trying hard to overcome this, and hopes to complete a 1.5-km open water swim someday.
and surgery
team comprising
orthopaedic surgeons,
sports physicians,
physiotherapists,
podiatrists,
radiologists, sports
scientists and others.
He also liaised with
senior management,
administrative staff
and contractors to
set up the physical
premises of the Sports
Centre, as well as
implement operational
and billing protocols.
My roles
included setting up
pre-participation
screening protocols
for events supported
by the Sports Centre
and drafting disclaimer
statements on the advice of the
hospital’s legal counsel. I also had the
opportunity to network with National
University of Singapore’s (NUS) staff
and partner institutions on projects
jointly organised with the Sports
Centre, as well as assist with article
requests from the mainstream media.
The biggest challenge was getting
NUH accredited as a sports medicine
training site. Upon rejection by the
Joint Committee for Specialty Training
(JCST) on the first attempt, we sought
the advice of other successfully
accredited sports medicine
departments, to come up with a
training programme that met JCST
training requirements. Personally, the
process was challenging as the above
responsibilities were in addition to my
pre-existing FM work commitments
at St Luke’s Hospital and the NUH
Transitional Care Team. You can
imagine the amount of free time I had
left over!
All our efforts finally came to
fruition when NUH received its
accreditation as a sports medicine
training site. As for me, I will be starting
full-time sports medicine training
from July 2015. Clinics have already
started at the Sports Centre, and we
hold regular multidisciplinary team
meetings to discuss challenging cases.
We are also collaborating with Team
NUS in looking after NUS athletes
with sports injuries and coming up
with injury prevention programmes for
high-risk sports.
Final thoughtsFrom the family medicine’s point
of view, sports and exercise play a vital
role in chronic disease management.
Knowledge of sports medicine is also
important, as more Singaporeans are
participating in exercises, resulting in
increasing rates of sports injury. As we
manage a rapidly ageing population,
physical exercise will play a key role in
functional and healthy ageing.
Above Dr wang Mingchang (right) with Dr Lingaraj Krishna, the director of NuH Sports CentreFacing Faculty and residents of NuHS FM residency programme at an orientation dinner in July 2014
July 2015 sma News • 27

what is radiation oncology?Radiation oncology has
traditionally been one of the best
kept secrets in medicine. Even
though this specialty is becoming
increasingly popular overseas, it is
still relatively unknown locally due
to limited exposure to it in medical
school, despite the important role it
plays in the treatment of cancer. It
is estimated that more than half of
all patients diagnosed with cancer
will undergo radiotherapy during the
course of their illness, whether it is in
the curative, palliative, neoadjuvant
or adjuvant setting.
Friends and family, even those
in healthcare, have little idea what
radiation oncology is about. It is often
confused with diagnostic imaging,
Text and photos by Dr Shaun Ho
OPINION
Radiation Oncology – A Merging of Biology
and Physics
interventional radiology, nuclear
medicine or medical oncology. In
radiation oncology, we use ionising
radiation in the form of photons,
electrons and even protons to treat
patients with cancer or other benign
conditions such as thyroid eye
disease, keloids, acoustic neuromas,
arteriovenous malformations and
trigeminal neuralgia.
Radiotherapy has come a long
way since its therapeutic potential
was discovered more than a hundred
years ago. It has developed rapidly,
especially over the last 20 years,
from simple 2D techniques to
3D conformal radiation therapy
(RT), to intensity-modulated RT
and stereotactic radiosurgery. As
technology continues to advance, so
does our ability to deliver radiation
to a target with greater accuracy and
higher dosage while sparing as much
normal tissue as possible.
why i chose to specialise in radiation oncology
Radiation oncology was not what
I had planned on specialising in – I
stumbled upon it unexpectedly. In
fact, I was initially drawn to surgery
because I was fascinated with its
interplay of anatomy, pathology
and technique. However, during
my surgical posting, I met a fellow
medical officer (MO) who was a
radiation oncology trainee rotating
through general surgery. That was
when I first learnt about this field
and the intriguing nature of its work,
which seemed to share similarities
with surgery minus the invasiveness.
Later, I did a posting in radiation
oncology and decided to stay put.
Radiation oncology appeals to
me in several ways. The first is our
patients – as every oncology patient
we meet in the clinic faces a serious
disease, it is a privilege to be part
of the treatment process to cure or
palliate our patients and it is also
very rewarding. Furthermore, many
consultants are able to build close
relationships with the patients and
their families because patients who
receive RT are often on long-term
follow-up after the completion of
treatment.
Another factor that draws me to
radiation oncology is the colleagues
in the department – fellow doctors,
radiation therapists, nurses, physicists
and dosimetrists – who work closely
together. From healthcare staff who
go the extra mile for patients, to
fellow trainees who help and support
each other, to senior doctors who
are always ready to provide help and
advice, everyone is passionate about
their work and caring towards the
patients.
Several incidents left a lasting
impression on me. One was a
consultant who had travelled to a
{
{

patient’s house to pass him some
medication when he found out that
the patient had significant side
effects from RT. Another colleague
recently fetched a deaf patient who
was uncontactable by phone to the
hospital because the patient’s CT scan
was suggestive of a retropharyngeal
abscess. Such colleagues who
genuinely care and go the extra mile
for their patients remind me daily why
I chose to practise medicine.
Unfortunately, radiation
oncologists are often subjected to
button-pushing witticisms due to the
perceived one dimensional nature of
our work, but nothing can be further
from the truth. Another aspect of
radiation oncology that appeals to me
is the broad knowledge base and skill
sets required in this field. Not only
do radiation oncologists need to be
familiar with reading CT scans, MRIs
and nuclear imaging, we must also
have a good understanding of surgical
procedures and anatomy, as it helps
guide target volume contouring. Due
to the many patients with terminal
disease that we manage, we also
need to have a basic understanding
of chemotherapy and the systemic
treatment options available, and be
familiar with palliative care.
A day in the clinic could involve
performing a nasendoscopy for one
patient, a vaginal examination and Pap
smear for another patient, followed
by a depot injection of goserelin for
a patient with metastatic prostate
cancer while titrating his pain
medications and having a discussion
about future care plans, and finally,
interpreting the radiological films
of another patient . While the initial
learning curve can be steep, the
multifaceted aspect of our work helps
to keep things interesting.
Radiation oncologists have
fairly predictable schedules, which
is uncommon in medicine. While
weekdays can get quite packed, we
do not have night calls and most
weekends are free. This allows for
good work-life harmony, giving us
sufficient time for our families and
hobbies.
radiation oncology trainingRadiation oncology is one of the
remaining training programmes not
yet under the residency system. It
consists of five years of seamless
training, of which one year is spent in
relevant non-radiation postings of our
choice. We work towards attaining
the UK FRCR (Clinical Oncology) or
the FRANZCR (Radiation Oncology),
the Australian/New Zealand
equivalent. The former qualifies
physicians in the UK to be clinical
oncologists who can prescribe both
chemotherapy and radiotherapy, but
it can be quite challenging to clear
the exams as we do not prescribe
chemotherapy in Singapore. Besides
clinical oncology, the exams also cover
subjects such as physics, statistics,
pharmacology, cancer biology and
radiobiology. As some of these topics
are not covered in medical school, it
takes some effort to learn them from
scratch.
To help us in our training, we have
weekly combined tutorials across
institutions. In-training assessments
are conducted through regular
mini-Clinical Evaluation Exercises,
case-based discussions and Direct
Observation of Radiotherapy
Planning Skills (DORPS). We also
have six monthly end-of-posting
assessments, comprising multiple
choice questions and vivas. During
our training, MOs and registrars
rotate through various firms in the
department to gain exposure to the
different oncology subsites such
as neuro-oncology, head and neck,
thoracic, breast, gastrointestinal,
urology, gynaecology, lymphoma,
paediatrics and sarcomas. The
department is also generally
supportive of trainees who wish to
broaden their knowledge beyond
radiation oncology.
Overall, radiation oncology is a
very interesting field, incorporating
technology and imaging with patient
care and contact. I am fortunate to
have stumbled into this field and am
thankful to be training in a specialty
that I enjoy.
Shaun is a radiation oncology registrar at National Cancer Centre Singapore. A lover of the outdoors, he can be found jogging through park connectors across Singapore on weekends. He enjoys discovering new places and learning new
things. Spending time with his friends and family brings him lots of joy and laughter.
July 2015 sma News • 29

OPINION
EVErybody KNows how to become a resident… or do
they? Good grades, publications, community service and
excellent clinical acumen are all helpful, but are they all that
matter? Are the rumours that blue blood, good looks and
medical school of origin play a part true? Are all candidates
for residency equal or are some more equal than others?
Maybe yes, maybe no, but you can’t change your parents
(although you can choose your godmother or godfather),
and in this age of Facebook, it is getting increasingly hard to
pass off your plastic surgeons’ handiwork as a makeover or
targeted weight loss/gain. But fear not, with this short guide
to basic residency requirements and specialty-specific
traits, you’ll be filling out survey forms and hounding faculty
members to complete your evaluations in no time.
basic residency requirements Knowledge
It’s difficult to get that general surgery residency if
you think the epiploic foramen of Winslow is in the brain.
Neither will you impress your endocrine consultant if you
think a sliding scale is something you use in the kitchen.
Time to stop sailing the uncharted seas and open a
book, plus even if you publish ten papers for your future
programme director, you still have to pass medical school
before you can start residency.
Clinical acumen
Appearing in the firing line at multiple morbidity and
mortality meetings does not a resident make. Clinical
acumen is an integration of knowledge, experience and
the art of medicine. The only way to get more of it is to
set out to sea more often, hopefully with a chart. For the
non-resident senior medical officer or service registrar
wandering in the desert, have faith because the time for
you to cross the river into your promised land (ie, specialty)
is at hand, especially for the good clinician. For the medical
student applying for residency, perhaps possessing clinical
acumen is a bit too much to ask, but it’s never too early to
start mastering the specialty of your choice.
Research
How do you differentiate between each candidate? For
some programmes, a PubMed search for the prospective
candidate’s publications may be a surrogate marker, but
dummies’ Guide to residencyBy SK Warrior
research
is not for
research’s
sake. If you’re
going to be doing
something for the
rest of your life, it helps
that it’s an intellectually
stimulating subject worth
investigating. But still,
you shouldn’t overdo it
and neglect your clinical
work; all the publications
in the world are of little
use if you can’t tie off that
bleeder in the middle of
the night.
Attitude
No one
wants a
resident who
pulls a long face
every time the clinic goes past 5 pm or turns off the phone
after midnight while on call. Remember you have to earn
the right to perform those total knee replacements and
cataracts, so put on your happiest smile and say, “Yes
Prof, I’m ok!” and then continue holding that retractor
throughout the rest of that Whipple procedure. Remember,
pain is weakness leaving your body. What we do in life
echoes through eternity… and the next residency interview.
Grooming
You have to look the part – if you want internal
medicine, look neat and intelligent; general surgery or
neurosurgery, look as though you’ve not slept in days.
And if you want to do a residency that begins with the
letter “O” or “D”, it’s time to buy those heels and invest
in some branded accessories; but try not to overdo it –
perfect makeup, initialed bespoke clothing, fancy shoes
and Bahasa Indonesia instead of Bahasa Melayu classes
may raise suspicions of “mountain climbing” private sector
tendencies, not kosher in residency programmes meant to
train doctors for the public sector.
30 • sma News July 2015
traits of the specialty However, those are but general
attributes of a resident. Below are some
specialty-specific traits that you must
demonstrate to get your residency.
Anaesthesiology
Be OCD! That sticker can only be
pasted lengthwise on the syringe. Helps
to have an overdeveloped hippocampus
(I think?) for all those drug dosages and
half-lives, and the nerves of a fighter pilot when the patient
crashes on you.
Internal medicine
Why have one differential when you can have 15? Refer
as needed to disprove said differentials. Be the last true
generalist in a world of subspecialists.
Geriatric medicine
Be both gentle and patient and have the ability to
move at a glacial pace. A flair for dialects is helpful but not
compulsory. After all, the caregivers of the elderly tend to
be foreign maids who can speak some basic English.
Diagnostic radiology
Love office hours and life spent in darkness. Love
shades of grey, literally. A photographic memory and the
ability to hedge help (“please correlate clinically”).
Pathology
Love office hours and a life spent staring down
microscopes. Love shades of purple and pink, literally. A
photographic memory and the ability not to hedge help.
Emergency medicine
Hate office hours and love
unpredictability. Work is like a box of
chocolates (you never know what you’re
going to get!). Save lives and be like
the Night’s Watch, overstretched and
misunderstood. Be prepared to override
your friends, as necessary, to admit
to the correct specialty (ideal, but not
compulsory).
Cardiology
Can read squiggly lines and enjoy life
at 1,000 miles per hour? Welcome!
Neurosurgery
Can read CT brains and enjoy life at 1,000 miles per
hour? Welcome!
“SK Warrior” is the alter ego in each of us who has to regularly face challenges in our work, and gracefully overcome obstacles of all forms, with a smile. May the SK warrior live on in you forever and to continue to do SK work for the betterment of your patients.
“Ours not to reason why, ours but to do and die.”
General surgery
Male: Have good hands and be able to withstand
pain and hard work. Looking good or speaking well is not
necessary.
Female: Pretend to be one of the men and be ready to
give up the best years of your life proving yourself.
Ophthalmology, otolaryngology, dermatology and plastic
surgery
Top of the class and good-looking to boot (some people
have all the luck). Let me guess, you can get
through a night call with perfect makeup, hair
and clothing, too.
Paediatrics
Chronic Dean’s lister with a deep
affinity for complex syndromes? Enjoy
calculating dosages with a calculator? Of
course, it helps if you actually enjoy working
with kids.
Obstetrics and gynaecology
Be the kind of person that women love, yet never
seen as a potential romantic rival by the husbands. Enjoy
occasional awkward conversations.
urology
Be sympathetic about leaks, unpeeled and peeled
bananas and malfunctioning machinery. Enjoy awkward
conversations.
Psychiatry
Be a father/mother figure or confidant that the patient
never had. Must be wary of erotic transference. Must enjoy
awkward conversations.
Orthopaedics
Enjoy working with power tools.
Know everything about only one thing.
Don’t be hurt if people think you know
nothing.
Family medicine
Enjoy working with people. Know
something about everything. Don’t be
hurt if people think you know nothing.
Remember Jon Snow became Lord
Commander.
July 2015 sma News • 31

i FrEquENtly receive distressed
SMSes from fellow GPs. Many of us are
solo practitioners who enjoy autonomy
as doctors and businesspeople. There
are certainly beauty and benefits in
solo practices. However, life is not
always smooth sailing; often, it springs
surprises on us in unexpected ways.
Like our patients, we face all kinds of
life challenges – personal health, family
problems, emotional issues, practice
difficulties, even perceived unfairness
and injustice. The list is endless.
Physical well-beingBeing in the frontline of the
healthcare system, GPs are constantly
bombarded with all kinds of viruses.
We are seasoned warriors against
influenza, hand, foot and mouth
disease, dengue, shingles and
chickenpox. We get knocked down,
rest a day and are back on our feet,
albeit with the loss of a day’s worth of
income.
From time to time, we hear
remotely about some new outbreaks
like the MERS. Many of us have
volunteered as Public Health
Preparedness Clinics and have
been promised supplies of personal
protective equipment and antiviral
medicines. Despite the support, we still
feel the jitters.
Some of the older GPs may suffer
from chronic diseases. A few may have
strokes. While we can still comfortably
practise as GPs, our emotional strength
and stamina would have diminished.
We may not be able to last an entire
day of clinic.
Financial well-beingMany young GPs are struggling
to make ends meet because of the
high rental of their commercial units.
They may still be servicing their study,
housing or car loan. At the other end
of the scale, patients are deterred by
the perceived higher GP fees. These
GPs are stuck between a rock and a
hard place.
“Hey, bad news! My neighbour has just rented his unit to a young, new GP.”“Hi, my landlord wants to increase my rental from $3k to $8k. How?”“Oui, the GP behind my clinic has just gotten CHAS. Should I apply too?”“Hi bro, just received a letter from a management company wanting to introduce a penalty system. How?”
All these SMSes reflect the very
dynamic and hostile environment in
which GPs operate. The bottom line is
money. At the forefront of our minds is
how to survive, or is it even worth the
effort continuing?
When Doctors Suffer
By Dr Leong Choon Kit, Editorial Board Member
“Hel
p, m
y family just left me...”
“Feeling depressed...”“I’m
so lost! ”
32 • sma News July 2015
GP MATTERS

Dr Leong Choon Kit is a GP in the private sector. He feels strongly about doctors contributing back to society. As a result, he tries to lend a voice to the silent majority in every issue he has come across, particularly those in healthcare, educational and other social concerns.
Psychological well-beingGPs undergo multiple stresses
daily, and over time, they can
certainly wear us down.
“Look, Choon Kit, being a GP can be very bipolar. If your clinic is empty, you are stressed by the fear of no income. If the clinic is too full, you are stressed by not being able to finish seeing the patients, or missing potentially life-threatening conditions and complaints from patients.”
A senior GP had warned me
when I first started my clinic. I can
understand that perfectly well now.
social well-beingI have heard of colleagues who
work so hard that they have hardly
any time to socialise. I have also
tried counselling fellow colleagues
whose spouses have left them.
To a lesser extent, I sometimes
feel stressed when my patients
ask about my children’s academic
performance, or lack thereof. I
also feel stressed when my friends
and relatives stop me in church, at
weddings or funerals to ask about
their medical conditions. It seems
rude to avoid them and it is difficult
to explain to laypersons about our
ethical obligation regarding kerbside
consultation.
where will help come from? A few years ago, while holidaying
on Phillip Island, Melbourne, my
family stopped at a quiet restaurant
by the quay for lunch. I found out
from the restaurant staff that it
is an establishment set up by a
fishermen’s co-operative to help ill
fishermen who could not go out to
sea – an interesting concept. Their
self-help spirit is admirable. The
chef, waiters and waitresses worked
tirelessly and always wore a smile.
They knew that their work supports
one another to bring collective good
to their community.
Similarly, in mission work, it
is recognised that missionaries
experience all kinds of stresses. Not
all return from the field unscathed.
Many of them need regular doses of
tender loving care, which is provided
by the member care department of
the mission agencies.
Doctors too are human – we
get bombarded by all kinds of
stresses and get wounded physically,
emotionally and psychologically.
Despite that, we are supposed to
carry out our duty to care for others
and in the name of professionalism,
hide our hurts while doing so.
It is about time that our
professional bodies look into a
formal structure to look after our
kind. We should learn from the
fishermen on Phillip Island and the
mission agencies. We should not
expect others to take pity on us or
look after our welfare, nor should we
expect a hand-out.
I am familiar with the GP scene.
Chat groups and regular meetings to
share industrial knowledge can be
therapeutic. These platforms allow
GPs to openly discuss problems
faced in the different phases of our
lives and practice, and enable us to
learn from one another.
Another useful and practical
help would be for GPs to cross
cover one another during periods
of unavailability. For smaller clinics,
employing a locum may not be
feasible. We can help to look after
patients from neighbouring clinics,
allowing our colleagues to take leave
for holidays, mission trip or medical
follow-up at hospitals.
There is so much we can do for
one another; the time to act is now…
or maybe yesterday?
“Hey, CK, do you have a moment? I’ve just received a letter from a management company and I am disturbed by the new clauses they have added in. Can you help?”
Looks like it’s time to help again.
I will share what I learn from this
friend in the next issue…
There is so much we can do for one
another; the time to act is now… or maybe yesterday?”“
July 2015 sma News • 33

By Jennifer Lee, Deputy Manager, SMA Charity Fund
thE PoCari Sweat Run 2015 was held on 12 July 2015 at
Kallang Practice Track. SMA Charity Fund (SMACF) was one
of the selected beneficiaries of the run that attracted a total of
10,000 runners, with 53 runners registered under SMA.
Dr Wong Tien Hua, President of SMA, flagged off the 10-km
run in the morning before joining the crowd as a fellow runner.
Staff from the SMA Secretariat also took part in the race to
support the SMACF.
In his speech, Dr Wong thanked Pocari Sweat Singapore and
the runners for their support towards SMACF and its causes,
which include providing financial support for future doctors
from underprivileged families. With the bursary, they will not
need to find other means to supplement their family income at
the expense of their medical education and training. Dr Wong
went on to congratulate Pocari Sweat Singapore for a successful
event, with a good turnout.
The donations received from the race will be used to fund
the SMA Medical Students’ Assistance Fund (SMA-MSAF), a
programme managed by SMACF, which provides bursaries to
needy medical students to support their living expenses so that
they can concentrate on their medical education.
Mr Yoshihiro Bando, operating officer of Otsuka
Pharmaceuticals Japan, commented, “POCARI SWEAT was
developed by Otsuka Pharmaceuticals Co. Ltd, Japan, with the
philosophy to create new products for better health worldwide.
We also recognise medical doctors as one of the key players in
creating and impacting health through their medical knowledge
and training. We are pleased to have the SMA Charity
Fund, which helps ensure that needy medical students can
concentrate in their medical training and become good medical
doctors, as one of our beneficiaries!”
Running for a Good Cause
Ph
oto
: Po
cari
Sw
eat
Sin
gap
ore
Ph
oto
: Po
cari
Sw
eat
Sin
gap
ore
Ph
oto
: Po
cari
Sw
eat
Sin
gap
ore
34 • sma News July 2015

achieving more together
Full member of National Council of social service SMA Charity Fund (SMACF) is now a full member of
the National Council of Social Service (NCSS).
NCSS is the coordinating body for some 400
voluntary welfare organisations (VWOs) in Singapore. It
is a statutory body established by an Act of Parliament
(The NCSS Act) on 1 May 1992, with the charter to
improve the lives of the disadvantaged in Singapore,
taking over the functions of the former Singapore
Council of Social Service and Community Chest of
Singapore. It works closely with many government
ministries, as well as the people and private sectors.
NCSS leads and coordinates the social service sector
in Singapore with the purpose of ensuring that every
person has the opportunity to live a life of dignity to his
or her fullest potential within society.
There are two types of membership under NCSS:
full and associate. Full membership is granted to an
organisation whose primary function is to provide a bona
fide direct social service that helps to meet the existing
needs of the community.
As the SMACF is a young charity, being awarded
a full membership is a testament to the quality of our
programmes. We can now collaborate with the council as
well as network with other VWOs to address needs that
may not have been covered, thus deepening our impact
on the medical fraternity. In addition, SMACF will also
be eligible for consideration for various funding schemes
under NCSS.
Care & share movement
SMACF has been accepted as a member of the Care &
Share Movement.
Care & Share is a national fund-raising and
volunteerism movement led by Community Chest for the
social service sector, in celebration of SG50 this year.
It aims to bring the nation together to show care and
concern for the needy, and to recognise the contributions
made by VWOs. Eligible donations raised by participating
VWOs from now till 31 March 2016 will be matched
dollar-for-dollar by the government. The matched
amount will go towards building the capabilities and
capacities of the social service sector, and supporting
social services to meet rising needs.
Your support is critical in helping us to advance our
cause, and create ripples through society. Donation to
SMACF can be made online at the SG Gives website
(https://www.sggives.org/smacf) or by cheque (donation
forms can be downloaded from our website). Donation
made this year will enjoy 300% tax deductions.
By Jennifer Lee, Deputy Manager, SMA Charity Fund
SMA CHARITY FuND
Bursary application for the SMA-MSAF is now open
for medical students from Lee Kong Chian School of
Medicine and Yong Loo Lin School of Medicine. Medical
students who are interested in applying for this bursary
can approach the schools directly on the bursary
application. For further enquiries, please contact SMACF
July 2015 sma News • 35
introductionEnd-of-life decisions can
prove to be especially challenging
to doctors because protecting
our patients’ health is a central
tenet of the profession. However,
respecting life includes supporting
quality of life right to its very end
and there is no absolute obligation
to prolong life indefinitely without
regard for consequences such
as burden of care.1 To tread this
delicate balance, the ethical principle
of respect (both for patients and for
human life) provides the foundation
on which doctor-patient trust is built.
There should be no doubt that care
provided at the end of life is of the same
standard as the treatment provided to
any other patient. This trust provides
dying patients and their loved ones
with the confidence that they will
always receive the best care possible
and that their choices and values will be
honoured.
All medical treatment imposes
burdens on patients. The trade-off
with benefits diminishes with frailty,
co-morbidities, progressive disease and
incurable conditions. Burdens include
treatment-related side-effects, cognitive
impairment, loss of independence and costs
both in terms of time and finances. There may be
a misconception that palliative care should be reserved
until the last days of life. On the contrary, the control of
physical and psychological symptoms should always be
a priority and palliation can be initiated at any stage of
illness. Inappropriate treatment also results in a misuse of
limited healthcare resources that may be directed away
from other patients who may benefit from them.
Ambiguity arises because there is no universally
By Dr Anantham Devanand
accepted definition of a patient who is approaching the
end of life. The General Medical Council in the UK has
proposed to include all patients who are likely to die
within the next 12 months and not limit to those who are
imminently dying. This broad definition would encompass
patients with terminal disease, those with existing
conditions with a risk of dying from an acute crisis and the
physiologically frail who have multiple co-morbidities.1
This informs us of the range of patients to whom end-of-
life decision making may be applicable.
making an end-of-life decisionThe process begins with a comprehensive evaluation
of the patient to clarify concerns, diagnoses, prognoses
and available treatment options. Patients who retain
decision-making capacity should be respected and
allowed to make their own decisions including the option
to refuse life-saving treatment. This process should not
be reduced to doing whatever the patient wants.2 Instead,
doctors have an obligation to help patients come to terms
with their illness, understand what can be meaningfully
achieved and make decisions that are consistent with
personal values.
The Mental Capacity Act (MCA) clarifies that every
adult is assumed to have decision-making capacity until
it is proven otherwise.3 Mental incapacity is assessed
using a two-stage test: (1) Is the person suffering from an
impairment of mental function and; (2) Does the impairment
prevent the person from making the required decision.
Anyone is deemed incapable of making a specific decision
when he/she cannot understand information related to
the decision, remember the provided information, weigh
up information or communicate any decision that has
been made. Doctors are obligated to maximise capacity
by either improving one’s understanding and aiding
communication or delaying decisions until acute medical
conditions that cause temporary incapacity are treated.
Anticipatory decisions help extend the autonomy of
those who have lost decision-making capacity. An advance
directive and the appointment of a lasting power of
attorney are examples of such decisions. It is imperative
Guide to End-of-life Decision Making
36 • sma News July 2015
PROFESSIONALISM

Dr Anantham Devanand is a senior consultant in Department of Respiratory and Critical Care Medicine, Singapore General Hospital, an assistant professor at Duke-NUS Graduate Medical School and the deputy director of SMA Centre for Medical Ethics and Professionalism.
to ensure the validity and applicability of any available
anticipatory decisions.1 Valid decisions are informed and
made when mental capacity was intact without undue
external pressure. The Advance Medical Directive Act
allows adults who are terminally ill to reject life-sustaining
treatment when they become mentally incapacitated.4
If patients meet such criteria, a search for an advance
directive should be made with the Registry of Advance
Medical Directives at the Ministry of Health.
A Lasting Power of Attorney (LPA) registered at the
Office of Public Guardian is a legal proxy authorised
to make decisions on behalf of the patient (“doner”).3
However, the proxy’s scope of decision-making must
also be checked because he or she can be authorised to
make decisions on the donor’s personal welfare, property/
affairs, or both. In medical decisions, the proxy’s role
is further restricted by the statute to exclude refusal of
life-sustaining treatment and any other treatment that
the doctor believes to be necessary to prevent significant
deterioration in the patient’s condition.
If a patient without decision-making capacity has not
made any anticipatory decision, then doctors have the
responsibility to make decisions based on the patient’s
best interests. This is defined by the MCA to consider not
only the medical best interests, but also the patient’s past
wishes, values and beliefs.3 The decision should be least
restrictive of the patient’s future choices and cannot be
motivated by a desire to bring about death. Although
responsibility ultimately rests with the doctor, the law
requires that relevant legal proxies, caregivers and family
members should be consulted and not just be told what
has been decided.
When consulting with families, they must not be given
the impression that they are being asked to make any
decision.1 Instead, it must be made clear that they are
advising the healthcare team on the patient’s values and
likely preferences. Phrases such as “doing everything”
should be avoided because of the mistaken inference that
“everything” equates to better care.2 Ideally, an identified
doctor should take responsibility for the communication
with the family. Multiple doctors across different shifts
and subspecialties will struggle to build the necessary
trust to guide family members through the patient’s
critical illness.
advance care planningRegardless of the safeguards, making a best interests
decision in a medical crisis remains a less than ideal
solution. Advance care planning is a voluntary discussion
between patients, care providers and family to clarify
care preferences (including location of care).5 It extends
beyond end-of-life decisions to long-term care needs
as well. Although advance care plans are not as legally
binding as an advance medical directive or designating a
LPA, they create a record of patient’s wishes and decisions
to facilitate the future delivery of treatment. The advance
care planning process itself assists patients to understand
their medical condition and treatment options, motivates
them to reflect on values and beliefs, and facilitates a
discussion with caregivers and family on choices at the end
of life. Instead of being a box-ticking exercise, it should be
an information sharing and reflective experience that can
be re-visited.5
End-of-life decision making should not be reduced to a
single “life-or-death” decision.2 It comprises a process by
which patients understand their own medical condition,
come to terms with the prognosis, clarify personal goals
and communicate with those closest to them. This journey
is often fraught with grief, denial, ambivalence and hope.
Helping them navigate this journey with minimal distress,
as well as a genuine respect for life and human dignity is
the doctor’s contribution.
References1. General Medical Council. Treatment and care towards the
end of life: good practice in decision making. Available at http://www.gmc-uk.org/Treatment_and_care_towards_the_end_of_life___English_0515.pdf_48902105.pdf. Accessed 27 June 2015.
2. Berlinger N, Jennings B, Wolf SM. The Hastings Center Guidelines for Decisions on Life-Sustaining Treatment and Care Near the End of Life. Oxford University Press, 2013.
3. Singapore Statues Online. Mental Capacity Act. Available at:http://statutes.agc.gov.sg/aol/search/display/view.w3p;query=DocId%3A7f933c47-8a34-47d1-8d0a-0 a 4 5 7 d 6 f a 1 c 2 % 2 0 % 2 0 S t a t u s % 3 A i n f o r c e % 2 0Depth%3A0;rec=0;whole=yes.
4. Singapore Statues Online. Advance Medical Directive Act. Available at: http://statutes.agc.gov.sg/aol/search/display/view.w3p;query=DocId%3Ac3137d32-215d-4bd1-a935-fc4770fc5850%20%20Status%3Ainforce%20Depth%3A0;rec=0.
5. Singapore National Medical Ethics Committee. Guide for healthcare professionals on the ethical handling of communication in advance care planning. Available at:https://www.moh.gov.sg/content/dam/moh_web/Publications/Guidel ines/National%20Medical%20Ethics%20Committee%20Guidelines/2010/NMEC%20Guide%20for%20Comms%20in%20ACP.pdf. Accessed 24 June 2015.
July 2015 sma News • 37

INDuLGE
iN most of my travels, I try to fit in one or
two good meals to round up the trip. Sights,
attractions, museums and history – they
are like the staple, the expected and bland
experience that is highly recommended on
TripAdvisor but would be neither spectacular
nor mind-blowing. Worse, it may just lead
you to busloads of tourists and a handful of
pickpockets on weekends.
Food is different. Food gives you a glimpse
into the complex dynamics that shape a society,
on a plate, which you can taste. It tells you a
story – its history, the disparity in social class,
the blend of different cultures, the influence
of colonisation and the fertility of the lands.
It may or may not be on TripAdvisor’s top 100
list of must-do, but it is always an experience that
you can reflect on, to which people can relate.
My travels this summer brought me to two very
contrasting places geographically, socially and politically.
Holland, a coastal province in Netherlands, was a colonial
superpower ruled by a King, while Czech Republic, previously
a colony and communist, is landlocked.
the dutch capitalWhen we think of Holland, Amsterdam comes to mind.
I had the privilege of spending two nights there, and the
experience was unexpected but enjoyable. I always imagined
Amsterdam to be a place of vice, where teenagers get high on
amphetamines and retirees smoke weed while playing chess
by the canal. I imagined it to be a place where couples spend
their honeymoons just so they can feel closer to the brink of
danger. But I couldn’t be more wrong.
I checked into a very quaint and charming hotel and was
given, what I believe, the best room available. Occupying
the entire attic, the room was clean, decently sized and
overlooked the canal. It prodded my imagination and gave
Text and photos by Bryan Koh
A Journey Through
&PRAGUE
AMSTERDAM
me a sense of how Anne Frank might have lived half a century
ago, even though that vision was rather farfetched. I wasted
no time and made my way to the Anne Frank House only to
Clockwise from topThe quaint room at Ambassade Hotel, AmsterdamMouth-watering dishes enjoyed in AmsterdamLong wait to visit the Anne Frank House
38 • sma News July 2015

find a queue snaking more than a hundred metres long. Not
wishing to waste time queuing, I booked myself on a river
cruise instead.
The river cruise turned out to be an extremely entertaining
experience that celebrated the magnificence and architectural
genius of the Dutch in their heyday. The organisation of the
canal ring area, the engineering of dunes, dikes and dams to
channel water away from the third of Holland that sat under
sea level, not to mention Golden Age artists like Rembrandt
and impressionists like Van Gogh – such orchestral brilliance
is often forgotten, but they ought to be remembered when we
think of Amsterdam.
Then the sun set and it was time for dinner. Dry-aged Dutch
ribeye steak, Dutch white asparagus with morel mushrooms
(seasonal), and cod from the Dutch coast paired with amazing
wine. The freshness of the produce, the intricate presentation,
the delicate taste and balance of flavours all reflect Holland as
a province – precise, passionate and dedicated to their art.
the journey continuesAfter Amsterdam, my next stop was Prague, the capital
city of Czech Republic, known for its baroque buildings,
Gothic churches and Astronomical Clock. I stayed at the Jalta
Boutique Hotel, which used to be a nuclear fallout shelter and
the military base of the Warsaw Pact countries during the
Cold War. It is right smack in the centre of Wenceslas Square,
next to the National Museum. The city of Prague is starkly
different from Amsterdam. The people are more wary, cold
and unwelcoming of tourists. This is understandable given
that the Velvet Revolution happened only recently in 1989.
The Bone Church in Kutna Hora, with skeletons of at
least 40,000 adults decorating its walls and halls, reminded
me of the Black Death and Hussite Wars. Even the
Astronomical Clock in the Old Town Square told the story
of a clockmaker, Master Hanus, who had his eyes gorged out
by the city councilmen just so he could not repeat his work.
Similar stories were told about Gothic churches and Jewish
synagogues. Living in this century in a place like Singapore,
I find it difficult to imagine the tumultuous life that people
have led in such a place for centuries. As I marvelled at the
beautiful architectural structures and the stories behind
them, I couldn’t help but pause for a moment to appreciate
the country that I grew up in.
As my journey through the two cities came to a close, I
sat with my mum, atop the Prague Castle Gardens, in Terasa
u Zlate Studne, the best restaurant in Czech Republic.
Taking in the scenic landscape, we talked about the history
of Czechoslovakia, the mechanics of the Astronomical Clock
and the poor quality of seafood in Czech Republic.
Bryan Koh is a final year medical Student at Yong Loo Lin School of Medicine. When not with his books or at the hospital, he spends time pursuing his interests in sport, food and horology. He had wished to be a rugby coach, chef or watchmaker but settled for his best option – being a doctor.
Clockwise from top leftCanal view of Amsterdam at nightAstronomical Clock in PragueHuman skeletons decorate the walls of the Bone Church, Kutna Hora, PragueThe fine cuisine savoured in PragueMum and I posing for the camera as we dinedThe crowd taking in the Nightwatch by Rembrandt
July 2015 sma News • 39

Contents• Topic 1: Overview of Mental Capacity Act (MCA)
• Topic 2: Code of practice
• Topic 3: Overview of incapacity
• Topic 4: How to assess mental capacity and when to
refer
• Topic 5: Writing a mental capacity assessment report for
purposes under the MCA
• Appendix
learning objectives• Understanding the principles and application of the
MCA in the assessment of mental capacity.
• Appreciating the importance in Lasting Power of
Attorney Certificate issuance.
• Understanding the requirements in preparing a mental
capacity report for the purposes specified in the MCA
MCA Online Training ModuleAssessment of Mental Capacity under the Mental Capacity Act
For enquiries, please contact the sma secretariat by phone at 6223 1264 or via email at [email protected].
Register online
• Visit SMA website
(www.sma.org.sg)
• Click on MCA
Online Training
Module
• Click on “Get this
course”
Account signup
• Sign up as a user
• Fill in the required
details
• Create an account
MCA online training
module
• An email will be
sent to you once
your account is
activated
• You are ready to
start
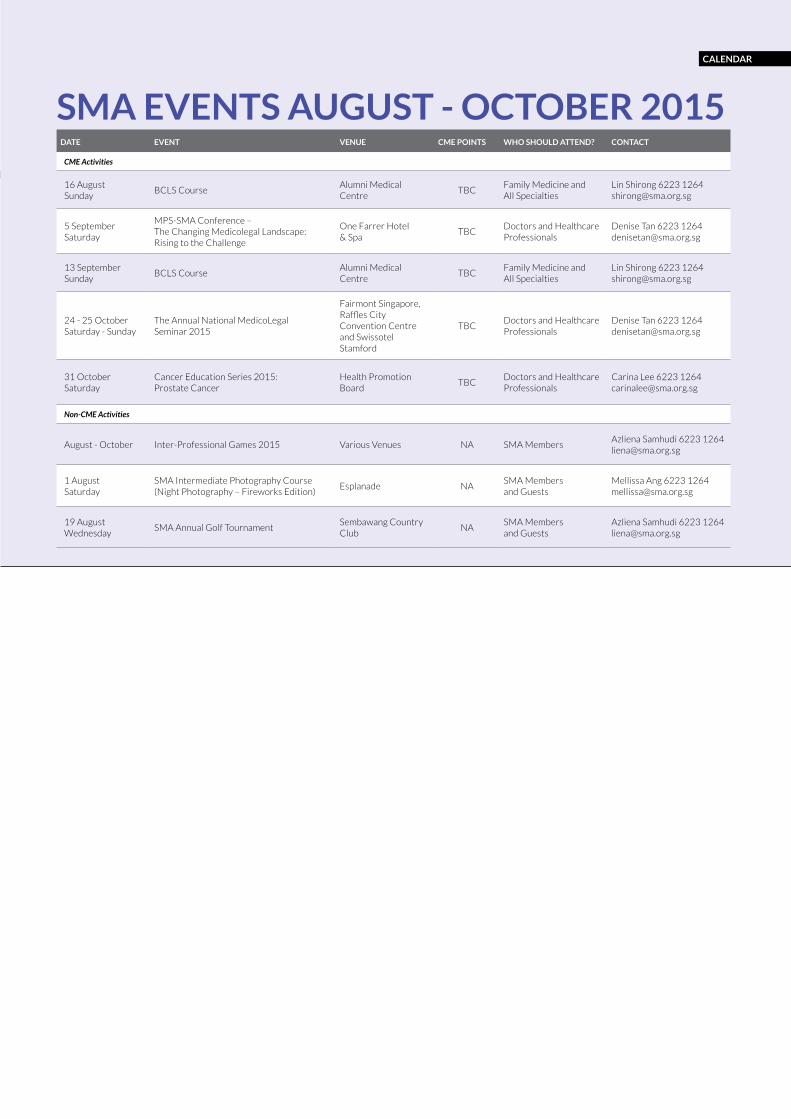
DATE EVENT VENUE CME POINTS WHO SHOULD ATTEND? CONTACT
CME Activities
16 AugustSunday
BCLS CourseAlumni Medical Centre
TBCFamily Medicine and All Specialties
Lin Shirong 6223 [email protected]
5 SeptemberSaturday
MPS-SMA Conference – The Changing Medicolegal Landscape: Rising to the Challenge
One Farrer Hotel & Spa
TBCDoctors and Healthcare Professionals
Denise Tan 6223 [email protected]
13 SeptemberSunday
BCLS CourseAlumni Medical Centre
TBCFamily Medicine and All Specialties
Lin Shirong 6223 [email protected]
24 - 25 OctoberSaturday - Sunday
The Annual National MedicoLegal Seminar 2015
Fairmont Singapore, Raffles City Convention Centre and Swissotel Stamford
TBCDoctors and Healthcare Professionals
Denise Tan 6223 [email protected]
31 OctoberSaturday
Cancer Education Series 2015: Prostate Cancer
Health Promotion Board
TBCDoctors and Healthcare Professionals
Carina Lee 6223 [email protected]
Non-CME Activities
August - October Inter-Professional Games 2015 Various Venues NA SMA MembersAzliena Samhudi 6223 [email protected]
1 AugustSaturday
SMA Intermediate Photography Course (Night Photography – Fireworks Edition)
Esplanade NASMA Members and Guests
Mellissa Ang 6223 [email protected]
19 AugustWednesday
SMA Annual Golf TournamentSembawang Country Club
NASMA Members and Guests
Azliena Samhudi 6223 [email protected]
SMA EVENTS AUGUST - OCTOBER 2015
CALENDAR

AIC SAYS
42 • sma News July 2015