doctors news nairobi hospital fraternity including admitting doctors, the hospitals senior...
TRANSCRIPT

KENYA UGANDA TANZANIA
Disease Pictorial
Ultrasound Guided Apical Pericardiocentesis
KENYA UGANDA TANZANIA
Doctors NewsDoctors News
Doctor Profile: Dr John KibosiaLeading from the front
OpinionWhy CME is important
BusinessLessons From A Medical Camp In Tigania West
BusinessLessons From A Medical Camp In Tigania West
OpinionWhy CME is important
Doctor Profile: Dr John Kibosia Leading from the front
Medical Doctors Professional, Business and Lifestyle News / Volume 16 2011Medical Doctors Professional, Business and Lifestyle News / Volume 16 2011 AfricaEast
AfricaEast
Disease Pictorial
Ultrasound Guided Apical Pericardiocentesis

– 2 – Doctors News, Volume 16 / 2011

Doctors News, Volume 16
From the Contents
W h a t’ s N e wAstraZeneca Launches products in Kenya
B u s i n e s s
Lessons From A Medical Camp In Tigania West
By Carole Kimutai
O p i n i o nWhy Continuing Medical Education? -
Time for Change
By Dr J Aluoch
Fe a t u r eLaparoscopic Ventral Hernia Repair
By Dr Bernard Ndung’u
D i s e a s e P i c t o r i a lUltrasound Guided Apical Pericardiocentesis
By Dr Robert Mathenge
D o c t o r P r o f i l eDr John Kibosia
By Patricia Muigai
22
11
12
14
20
26
Welcome to the 16th edition of Doctors News EA magazine.
In this issue, we have a feature on the health of inmates in Kenyan prisons and the person in charge of the department, Dr Kibosia. He is the director of Health services in the prisons Department.
In the Doctor Profile, he talks about his passion for managing health institutions and his efforts to reduce mortality in Kenyan prisons.
Dr Bernard Ndung’u writes an in-depth feature on laparoscopic hernia repair, while we feature Ultrasound Guided Apical Pericardiocentesis in the disease pictorial.
In our regular opinion and business columns, Dr J A Aluoch raises the the question of the importance of continuing medical education. Finally Carole Kimutai, has written an insightful article on lessons from a recent medical camp in TiganiaWest.
We would like to remind our readers and advertisers that Doctors News EA is a magazine for doctors only published by doctors. It is the only magazine of its kind and is distributed to registered physicians across East Africa.
As always, we invite you to share your wisdom, products and services with other
doctors through Doctors News EA.
Enjoy the magazine.
Dr Robert Mathenge
Doctors News East Africa
Medical Editor Dr Robert Mathenge [email protected]
Editorial Advisory Board Dr J A Alouch Dr P H Rees Dr J B O Okanga Prof Zipporah Ngumi Dr Stephen Muhudhia Prof John Atinga Dr Willy Mutunga Dr Githinji Gitahi Carole Kimutai Joe Muchekehu Sam Madoka
Editor/Design Patricia Muigai [email protected]
Contributors Carole Kimutai, Dr J A Aluoch, Dr Bernard M Ndung’u
Accounts: Carol King’ori [email protected]
Subscriptions and Distribution Kennedy Munyao [email protected]
Publisher Prof Nelson Awori Centre Ralph Bunche Road, P. O. Box. 2665-00200, Nairobi, Kenya. Tel: +254-20-271-2121 Cell: +254-722-698211
Disclaimer: Although every precaution has been taken to ensure accuracy of published materials Doctors News East Africa cannot be held responsible for opinions expressed or facts supplied by its authors. Printed in Kenya. Copyright, Sterling Media Limited. All rights reserved. Doctors News EA is published by doctors for doctors six times a year.
M e d i c a l E d i t o r N o t e


– 6 – Doctors News, Volume 16 / 2011
external audit by a SANAS Assessment Team on 19th and 20th October 2010 following one year of operations.
The Lancet Group has traditionally prescribed to ISO 17025. ISO 17025 is an International Standard (published by the International Organization for Standardization) that specifies the general requirements for the competence to carry out tests and/or calibrations. The requirements as stipulated in ISO 17025 and ISO 15189 are very similar with minor differences between the two related to the scope for each. ISO 17025 is intended for application to a wide range of medical and non-medical testing environments. Its broad based application is relevant to human and non-human samples such as test on animals, occupation and environmental health
Pathologists Lancet Kenya adheres to strict internal quality and system maintenance for equipment calibration and validation. They also undertake constant internal and external quality assurance programmes. Relevant documents demonstrating adherence to quality systems are well controlled and available for perusal as required.
I n d u s t r y N e w s
The South African National Accreditation System (SANAS) Approval Committee has granted Pathologists Lancet Kenya Laboratory the unique accreditation of
M0462 indicating as SANAS Accredited Medical Laboratory. Pathologists Lancet Kenya laboratory underwent successful
Lancet Kenya Now SANAS Accredited
CEO of Pathologists Lancet Kenya Dr Ahmed Khalebi addressing guests during the gala dinner the company hosted to celebrate its accreditation
Medical Waste Management gets a Boost
The Nairobi Women’s Hospital has commissioned a new incinerator in
an effort to enforce its waste management policy. During the recent official launch ceremony, the hospital’s CEO, Dr Sam Thenya said that the institution was commited to ensuring a safe environment, free from bio medical waste contamination.
Installed within the Adam’s Arcade branch of the hospital, the incinerator will benefit the Nairobi Women’s and other hospitals as well as the manufacturing industry.
“It is the largest in this region, with capacity of 200kg per run. We have already trained staff members on bio medical waste management. The mandate of the team is to ensure that no waste within the organization finds its way into our sewarage system,” Dr Thenya said.
He further urged institutions to ensure their waste management is properly coordinated and thanked the hospital’s partners, including
NEMA, GIZ, Plenser Limited and the hospital’s staff whose support has enabled the Nairobi Women’s Hospital make the project a reality.
(L-R) Nairobi Women’s Hospital CEO Dr Sam Thenya and NEMA Director General Dr Ayub Macharia lead other invited guests in cutting the ribbon
to officially launch the incinerator
Doctors News, Volume 16
– 8 – Doctors News, Volume 16 / 2011
I n d u s t r y N e w s
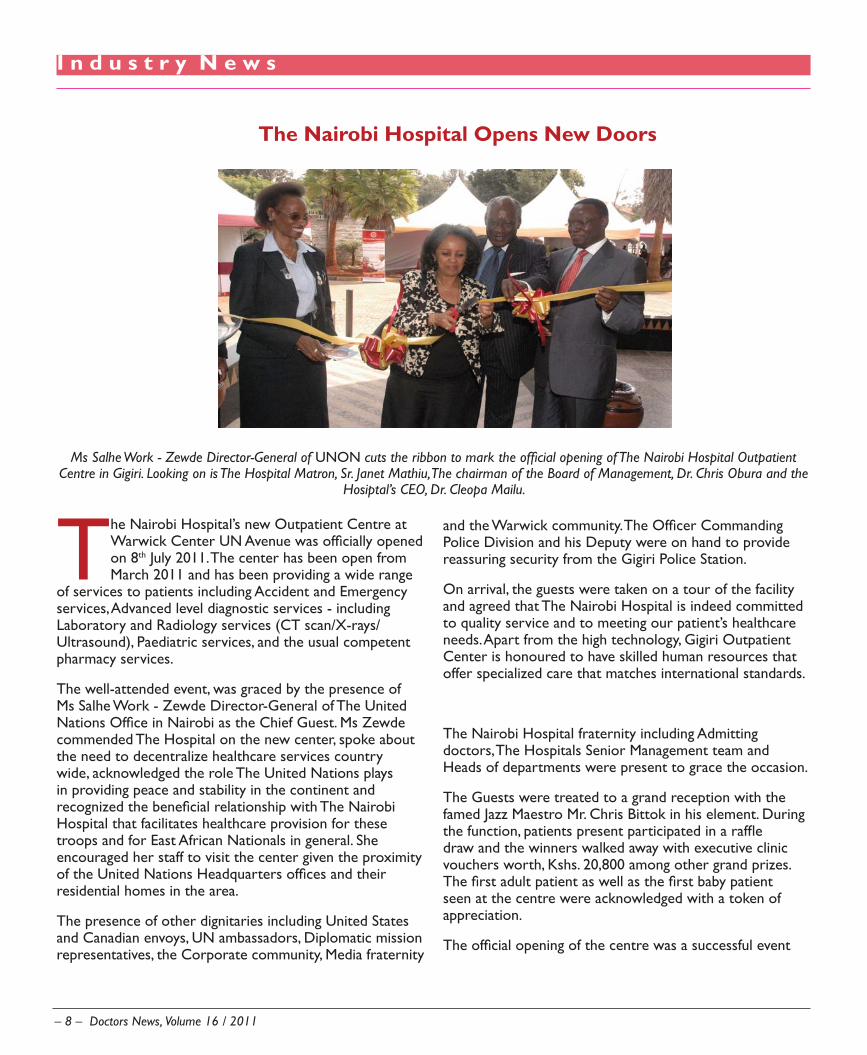
The Nairobi Hospital’s new Outpatient Centre at Warwick Center UN Avenue was officially opened on 8th July 2011. The center has been open from March 2011 and has been providing a wide range
of services to patients including Accident and Emergency services, Advanced level diagnostic services - including Laboratory and Radiology services (CT scan/X-rays/Ultrasound), Paediatric services, and the usual competent pharmacy services.
The well-attended event, was graced by the presence of Ms Salhe Work - Zewde Director-General of The United Nations Office in Nairobi as the Chief Guest. Ms Zewde commended The Hospital on the new center, spoke about the need to decentralize healthcare services country wide, acknowledged the role The United Nations plays in providing peace and stability in the continent and recognized the beneficial relationship with The Nairobi Hospital that facilitates healthcare provision for these troops and for East African Nationals in general. She encouraged her staff to visit the center given the proximity of the United Nations Headquarters offices and their residential homes in the area.
The presence of other dignitaries including United States and Canadian envoys, UN ambassadors, Diplomatic mission representatives, the Corporate community, Media fraternity
The Nairobi Hospital Opens New Doors
and the Warwick community. The Officer Commanding Police Division and his Deputy were on hand to provide reassuring security from the Gigiri Police Station.
On arrival, the guests were taken on a tour of the facility and agreed that The Nairobi Hospital is indeed committed to quality service and to meeting our patient’s healthcare needs. Apart from the high technology, Gigiri Outpatient Center is honoured to have skilled human resources that offer specialized care that matches international standards.
The Nairobi Hospital fraternity including Admitting doctors, The Hospitals Senior Management team and Heads of departments were present to grace the occasion.
The Guests were treated to a grand reception with the famed Jazz Maestro Mr. Chris Bittok in his element. During the function, patients present participated in a raffle draw and the winners walked away with executive clinic vouchers worth, Kshs. 20,800 among other grand prizes. The first adult patient as well as the first baby patient seen at the centre were acknowledged with a token of appreciation.
The official opening of the centre was a successful event
Ms Salhe Work - Zewde Director-General of UNON cuts the ribbon to mark the official opening of The Nairobi Hospital Outpatient Centre in Gigiri. Looking on is The Hospital Matron, Sr. Janet Mathiu, The chairman of the Board of Management, Dr. Chris Obura and the
Hosiptal’s CEO, Dr. Cleopa Mailu.

Doctors News, Volume 16
I n d u s t r y P i c t o r i a l
Attendees arrive at the Riruta Health Centre, Nairobi to mark the World Health Day.
©IOM 2011 (Photo: Mary-Sanyu Osire)
Dr Allan Waxman (2nd R) from the American Society for Colposcopy and Cervical Pathology with trainees during the cervical cancer prevention
workshop at Kenyatta National Hospital
The Nairobi Hospital’s staff donate foodstuffs to residents of Isiolo during a recent medical camp
(Left) Minister for Public Health and Sanitation, Hon Beth Mugo (seated,
centre) in a group photo during the Consultation on Africa Based Manufacturers of Pharmaceuticals and other Malaria Technologies held at Crowne Plaza Hotel in
Nairobi. The meeting sought to find potential solutions to challenges
facing local pharmaceutical manufacturers
Photo courtesy of
Lake Victoria South Water Services Board staff give a demonstration to members of the public on water treatment and quality testing during the Water and Sanitation Expo held on 17th May at the Kenyatta grounds,
Kisumu

– 10 – Doctors News, Volume 16 / 2011
I n d s t r y N e w s
The entrance to AKUH’s Heart and Cancer Centre. The facility is set to position the AKUH as a hub in an integrated Aga Khan Development
Network (AKDN) health
Aga Khan University Hospital’s Heart and Cancer Centre Now Open
The US$ 50 million facility brings international standards of patient care and cardiology and oncology treatment to Kenya, positioning the University Hospital as a hub in an integrated
AKDN health system in East Africa. It also represents a significant expansion for the Aga Khan University’s Faculty of Health Sciences in the region.
“We see our medical programmes here in Nairobi as nodes in a broad, regional health care network, reaching from Arusha to Kampala, from Nyeri to Mtwara and from Kigali to Malindi. Our goal is an integrated, best practice regional health system – providing a continuum of services from preventive and primary care to tertiary hospital-based care,” said His Highness the Aga Khan, speaking at the inauguration ceremony.
The Centre is part of the Aga Khan University’s long term development plans for its Faculty of Health Sciences, which includes the expansion of the Nairobi University Hospital to a 600-bed tertiary care facility and the establishment of an Undergraduate Medical Education Programme, an Undergraduate Nursing Programme and a School of Allied Health Professionals.
A Response to Emerging Trends in Health An equally ambitious agenda for health-related programmes envisions an integrated regional health system for East Africa. Drawing on best practices, the system will seek to address fast-growing health problems that are emerging due to lifestyle changes in the developing world.
According to the WHO, 70 percent of new cancers in the next 15 years will occur in developing countries, affecting younger working-age populations. Developing countries will therefore face a growing burden of non-communicable diseases such as cancer, diabetes and heart disease alongside existing infectious diseases.
“In Kenya alone, some 80,000 new cancer cases are diagnosed each year, with an unusually high number among young people,” noted the Aga Khan. “The new Centre will be ideally positioned to address such issues,” he said, noting that it would offer specialised training in cardiology and oncology.
H. E. President Mwai Kibaki inaugurated the Centre, in the presence of His Highness the Aga Khan, Chairman of the Aga Khan Development Network (AKDN). The ceremony was attended by the Deputy Prime Minister and Minister for Finance, Honourable Uhuru Kenyatta, the Minister for Medical Services, Honourable Professor Peter Anyang’ Nyong’o, the Chief Executive Officer of Agence Française de Développement. Mr Zerah and various other government dignitaries and the Board of Trustees of the Aga Khan University.

Doctors News, Volume 16
W h a t ’s N e w
Keynote speaker, Prof Mungai-Ngugi gave an excellent presentation on current updates in Prostate cancer management, with special
focus on advanced disease
Zoladex 10.8mg Launch in Kenya
Attendees keenly follow launch proceedings

– 12 – Doctors News, Volume 16 / 2011
B u s i n e s s
I am slightly over one year old in Rotary; a worldwide organisation of business and professional men and women who come together to provide humanitarian service and undertake projects in various fields to
benefit local communities; mainly in the areas of children, water, peace, and conflict resolution and health.
In May 2011, the Rotary Club of Nairobi East (where I am a member), partnered with The Village Trust (TVT), a non-profit organisation to hold a medical camp in Tigania West - Meru. TVT is a local NGO based in Meru which has been organizing annual free medical camps in Tigania West since 2008. The medical camps are aimed at complementing the government’s efforts to address the health concerns of the Tigania West region. Over the
years, the free medical camps have brought affordable healthcare, free health information to the community and enabled identification of the common health problems of the community. Months before the day of the medical camp, a lot of effort went into looking for medical supplies, doctors, and volunteers. The role of Rotary was basically to mobilise people and resources. Together with other members of the Rotary Club of Nairobi East, we raised funds, approached corporates for financial support, medical institutions for supplies and other non-profit organisations who would assist. It was a difficult task sending out proposals and not receiving any responses and scheduling meetings with managers in charge of corporate social responsibility (CSR).
Lessons From A Medical Camp In Tigania WestBy Carole Kimutai
Patients line up for registration at the medical camp Dr Kilemi Mwiria has his blood pressure checked by a volunteer doctor from the Nairobi Women’s Hospital

Doctors News, Volume 16
B u s i n e s s
The actual job was when we got to the venue. Having travelled to Meru a day before the medical camp date, we were at the venue early. However, we were not as early as the residents of Tigania West who had travelled long distances to access free treatment. It was my first time to participate in a medical camp and get my hands dirty – literally – under the scorching sun, we registered the patients who had come for treatment. I also stared straight at the face of poverty, disease and helplessness. The previous night, I had engaged the area Member of Parliament Dr.Kilemi Mwiria in a discussion about the role of government in ensuring all its citizen have access to good quality health care. This he said was a herculean task and it needed private sector and citizens help bridge the gap. While looking at the long queue of people who had turned up, it occurred to me that what Dr. Mwiria talked about was more than a gap.Kenya has a major challenge when it comes to adequate medical facilities. A majority of the population can barely afford to buy or even access a simple pain killer. Because of this, most ignore and live with medical problems that generate into terminal ailments. Amongst the volunteers at the camp was staff from the Nairobi Women’s Hospital who had come with a Mammography truck donated by Safaricom.
There are alarming cases of breast cancer and other types of cancers in Tigania West. In one particular case, a 21 year old mother of five year old twins had advanced breast cancer and the medical personnel recommended further tests and medical intervention in Nairobi. The
mother was more worried about raising bus fare to Nairobi than her health which was very sad.
After eight hours spent in the sun what did I learn?
They say the devil is always in the details. When •planning a medical camp, ensure details like patient registration and crowd control are dealt with adequately. The people who turned up were more than 10,000 and dealing with the massive numbers was a huge challengeThere is need to have more volunteer doctors. •With a crowd of 10,000 people, 20 doctors were a drop in the ocean. It was humbling to see the doctors work long hours without a break as the numbers kept swellingIronically most people can’t leave without getting •a prescription. The pharmacy faced a major challenge in dispensing drugs as the pharmacists available were overstretched by the massive numbersAll hospitals and medical centres should have a •CSR project that involves reaching out to the community as there are many medical needs that need to be addressedI finally appreciated what doctors go through. •Patients go to them seeking help and sometimes doctors have no answers
Carole Kimutai is the Editor of MANAGEMENT Magazine.Email: [email protected]: @CaroleKimutai
– 14 – Doctors News, Volume 16 / 2011
O p i n i o n
By Dr J A Aluoch FRCP, EBS
Two apparently conflicting pieces of evidence exist about physician’s continuing medical education (CME). Physicians report spending, on average (and among other activities)
many hours per year in CME activities, ostensibly geared toward improving their performance and/or optimizing the outcomes of their patients. In addition, producing and accrediting formal, planned CME events and activities are large enterprise intended to bring physicians up-to-date with rapidly expanding medical information. Patterned after undergraduate medical education consisting of lectures, audio visual presentations, and printed materials, CME activities appear underpinned by a belief that gains in knowledge lead physicians to improve how they practice and thus improve patient outcomes. Despite this belief and the level of participation in and resources for CME, many studies have demonstrated a lack of effect on physicians’
Why Continuing Medical Education? Time for Change
performance of current practice guidelines or sizable gaps between real performance. In addition, a relatively weak effect of formal, planned CME on physician performance has been demonstrated in some studies.
Despite seemingly endless round of conferences, symposia, round-table discussions, and panel debates over the years, continuing medical education now is not greatly different from what it was 40 years ago. There is simply a greater quantity of the same familiar things.
Why continuing medical education? Three generalizations keep re-curring in the literature. We say first that it is the personal responsibility of professional to engage in never-ending refinement of his professional competence; second, that the body of biomedical knowledge is changing so rapidly that each of us must struggle constantly simply to keep up with an increasingly narrow field since it is hopeless
“Physicians can be of the
greatest service to society
if they work at preventing
disease rather than treating
it”

Doctors News, Volume 16
O p i n i o n
to try to keep abreast of general medical knowledge; and third, that many deficiencies in health care not only exist but could be corrected by the appropriate continuing education of practitioners-particularly those practitioners who do not take part in programs of continuing education.
The diagnosis of deficiencies in the care of patients is surely an indispensable strategy, but far more difficult is the successful translation of even distasteful findings into sound educational practices that have some hope of alleviating the shortcomings which are identified. As a profession we seem more willing to consider or even to adopt new information or new technology than to change in any fundamental fashion the way we use ourselves. We are convinced, or so the literature of continuing education would make us seem, that it is our failure to apply new knowledge that represents the weakest link in the chain of assuring that the highest quality of medical care is delivered by the greatest number of physicians to the largest number of patients.
While this view may be correct, I am not familiar with any solid data to support it. In fact, the correction of the major health problems in our country, as in other parts of the world, does not appear to require any substantial body of new knowledge. Rather, it requires that physicians use the knowledge they already have in a different way or more fully exhibit the professional attitudes that have characterized the physician’s role as long as there have been physicians. As more eloquent speaker that recently said, “If I were asked to compose an epitaph on medical throughout the 20th Century, it would read: ‘Brilliant in its discoveries, superb in its technological breakthroughs, but woefully inept in its application to those most in need….’’’
Since I was a medical student 48 years ago, I have heard and I have read in medical literature covering a far longer period that physicians can be of the greatest service to society if they work at preventing disease rather than treating it. But which gets more academic attention and reward: the replacement of damaged arteries and heart valves or the prevention of smoking and obesity? We

– 16 – Doctors News, Volume 16 / 2011
have been told again and again that most of those who consult us are the anxious well rather than the curable sick. But which gets more attention in our educational programs-the pharmacologic action of drugs and their side effects or the skill of listening and providing reassurance?
I am afraid that most of us have been seduced by the notion that the professional responsibility to keep abreast of current information even if the information may have little use to many patients and even if it means diverting attention from other elements of professional competence that may be of far greater importance to those we serve. Having been convinced that “Keeping
up” is the goal, we are easily led to the conclusion that the need in continuing education is for more instruction:
Regrettably a recently completed survey by the World Health Organization of continuing education in member nations has shown that the lecture is still the most widely used instructional method by a large margin.
I have little hope that many of us will be changed significantly by what you read today, although some of us may be better informed before reading the article. But if change in behavior is the goal of continuing education,
whether it is offered to practitioners or to medical educators, then perhaps most of what we now do must be dismissed in much the same way as Oliver Wendell Holmes, the autocrat of the breakfast table and one-time dean of the Harvard Medical School, once dismissed another component of medicine when he said: “I firmly
believe that if the whole material medica as now used could be sunk to the bottom of the sea it would be all the better for mankind-and all the worse for the fishes.”
I suggest that it is time for us to start a new with continuing medical education.
The ultimate effect of formal CME interventions on the practice of physicians and the health of their patients ( as in the case of any intervention) must be understood in the context of the methods by which the CME is delivered, including but not limited to the nature of the enabling resources where available, the environment in which the translated competence is played out, and in the complex intrapersonal, interpersonal, and professional educational variables that affect the physician learner immediate goal of a CME activity, the exclusively didactic CME modality has little or no role to play. Knowledge is clearly necessary but not in and of itself sufficient to
O p i n i o n
“Knowledge is clearly necessary but not in and of itself sufficient to bring about change in physician
behavior and patient outcomes”

Doctors News, Volume 16
bring about change in physician behavior and patient outcomes. Didactic interventions should receive less credit than do more effective methods and perhaps no credit. In contrast, variables over which the CME provider has control and appear to have a positive effect are the degree of active learning opportunities, learning delivered in a longitudinal or sequenced manner, and the provision of enabling methods to facilitate implementation in the practice setting.
While numerous questions remain regarding formal CME, including group size, the role of the learning and practice environment, the clinical dimensions of care, the assessment of learner needs, and barriers to change, one large question remains. In the face of longstanding knowledge about adult, self-directed learning and the general disinclination to believe that didactic CME works, now coupled with the findings that’s it does not, why would the medical profession persist in delivering such a product and accrediting its consumption? The reasons for the persistence of didactic CME include ( but are definitely not limited) the ease of designing and providing such activities, the substantial pharmaceutical sponsorship that promotes the transfer of information about new medications, and the dependence on traditional
undergraduate models of education that are easy-to-mount and revenue generating.
Changing this delivery system carries serious implications for several groups of stakeholders that want to design and deliver effective CME. First medical licensing boards and others with a genuine interest
in assuring the public of physician competence must rethink the value of CME credit system. Second, medical schools, specialty associations and societies, and other providers of CME must reconsider the value of the credit they provide, as well as the type and duration of learning activities they produce.
Organizations intending to ensure the quality of CME
must evaluate the services they provide to a large, complex, and expensive CME enterprise that values the production of single-session, teacher-centered activities over learner achievement. Finally, physicians must reflect on what they perceive as the CME experience itself and weigh the costs and lost learning opportunities of attendance at ineffective didactic sessions against participating in interactive, challenging, and sequenced activities that have increase potential for positively affecting their performance and the health of the patients they serve- the most important outcome of all.
O p i n i o n
“medical licensing boards and others with a genuine
interest in assuring the public of physician
competence must rethink the value of CME credit
system”
– 18 – Doctors News, Volume 16 / 2011
F e a t u r e
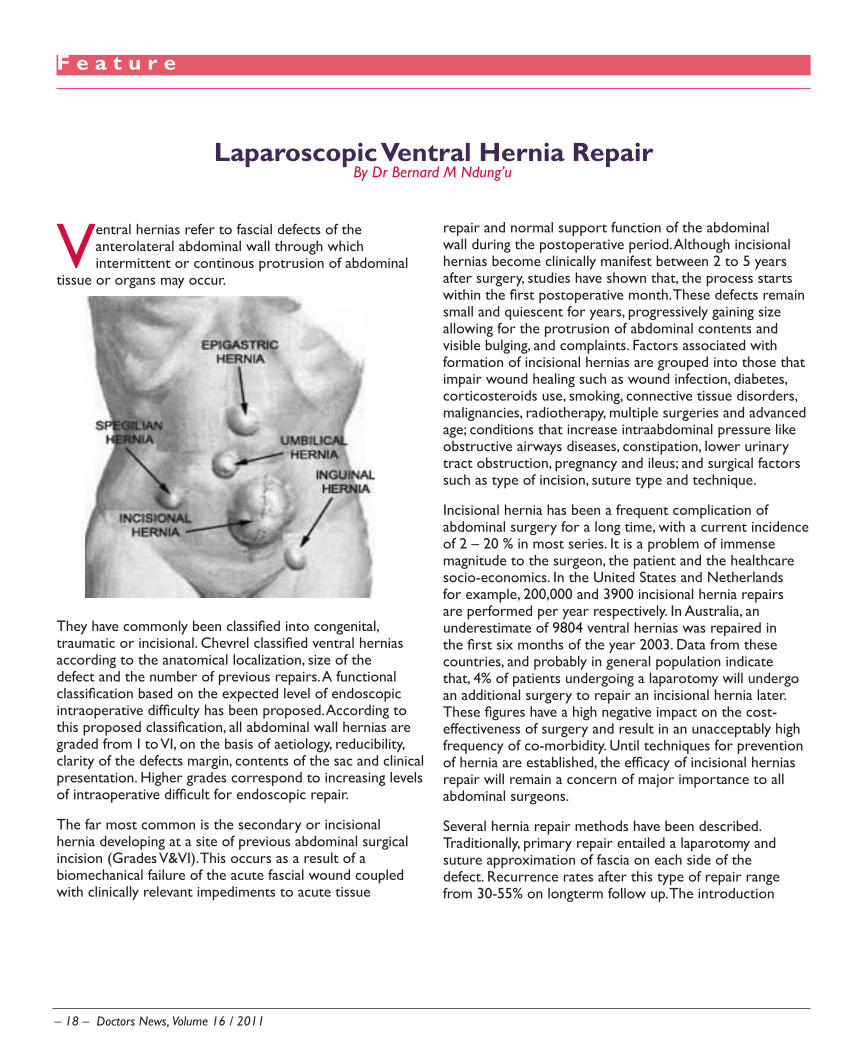
Ventral hernias refer to fascial defects of the anterolateral abdominal wall through which intermittent or continous protrusion of abdominal
tissue or organs may occur.
They have commonly been classified into congenital, traumatic or incisional. Chevrel classified ventral hernias according to the anatomical localization, size of the defect and the number of previous repairs. A functional classification based on the expected level of endoscopic intraoperative difficulty has been proposed. According to this proposed classification, all abdominal wall hernias are graded from I to VI, on the basis of aetiology, reducibility, clarity of the defects margin, contents of the sac and clinical presentation. Higher grades correspond to increasing levels of intraoperative difficult for endoscopic repair.
The far most common is the secondary or incisional hernia developing at a site of previous abdominal surgical incision (Grades V&VI). This occurs as a result of a biomechanical failure of the acute fascial wound coupled with clinically relevant impediments to acute tissue
repair and normal support function of the abdominal wall during the postoperative period. Although incisional hernias become clinically manifest between 2 to 5 years after surgery, studies have shown that, the process starts within the first postoperative month. These defects remain small and quiescent for years, progressively gaining size allowing for the protrusion of abdominal contents and visible bulging, and complaints. Factors associated with formation of incisional hernias are grouped into those that impair wound healing such as wound infection, diabetes, corticosteroids use, smoking, connective tissue disorders, malignancies, radiotherapy, multiple surgeries and advanced age; conditions that increase intraabdominal pressure like obstructive airways diseases, constipation, lower urinary tract obstruction, pregnancy and ileus; and surgical factors such as type of incision, suture type and technique.
Incisional hernia has been a frequent complication of abdominal surgery for a long time, with a current incidence of 2 – 20 % in most series. It is a problem of immense magnitude to the surgeon, the patient and the healthcare socio-economics. In the United States and Netherlands for example, 200,000 and 3900 incisional hernia repairs are performed per year respectively. In Australia, an underestimate of 9804 ventral hernias was repaired in the first six months of the year 2003. Data from these countries, and probably in general population indicate that, 4% of patients undergoing a laparotomy will undergo an additional surgery to repair an incisional hernia later. These figures have a high negative impact on the cost-effectiveness of surgery and result in an unacceptably high frequency of co-morbidity. Until techniques for prevention of hernia are established, the efficacy of incisional hernias repair will remain a concern of major importance to all abdominal surgeons.
Several hernia repair methods have been described. Traditionally, primary repair entailed a laparotomy and suture approximation of fascia on each side of the defect. Recurrence rates after this type of repair range from 30-55% on longterm follow up. The introduction
Laparoscopic Ventral Hernia RepairBy Dr Bernard M Ndung’u

Doctors News, Volume 16
F e a t u r e
of polypropylene mesh repair by User opened a new era of tension-free herniorrhaphy. The mesh, which was modified in 1962, gained popularity over 30 years and currently, popular polypylene meshes are commercially available. Polyester mesh was introduced in Europe in the 1950’s. Rives and Stoppa employed polyester mesh in their landmark article describing preperitoneal technique for abdominal wall hernia repair in 1989. This technique has become the standard by which all abdominal hernia repair methods are measured. The expanded polytetrafluoroetylene (ePTFE) initially used as a vascular graft was adapted for ventral hernia repair in 1983 by Goore et al and has been modified severally in the 1990’s. Unlike polypylene and polyester meshes, which were associated with severe intraabdominal adhesions leading to small bowel erosion, obstruction and fistulation, there are no reports of these complications with ePTFE. It is now well established that mesh repair significantly reduce the incidence of recurrence to 10-25% regardless of mesh type and operative technique. However, implantation of the mesh by open techniques requires wide dissection of soft tissue contributing to an increase in wound infection and wound – related complications in addition to the complications associated with the older mesh materials.
Since the first report of laparoscopic ventral hernia repair (LVHR) by Le Blanc and Booth in 1993, (photographs 1), the technique has been refined and has gained sufficient popularity within the surgical fraternity to be considered the standard procedure for ventral hernia repair.
Patient’s selectionIndications of laparoscopic ventral hernia repair a) include
Size of the defect: defects larger than (i) 3cm and smaller ones in obese patients, recurrent hernias and special types of hernias such as the spigelian hernia, are best treated laparoscopically (1). There are no objectively defined selection criteria
for the upper limit but some experts have suggested limiting LVHR to cases where transverse separation of the fascial edges is 10cm. However there are many reports in the literature of LVHR of far much larger hernias.Obese patients and recurrent hernias(ii) “Swiss-cheese” defects(iii)
Contra indicationsb) Extremely large hernias(i) End-stage cardiac, liver and pulmonary (ii) diseaseExtremely dense adhesions like in previous (iii) multiple laparotomies, peritonitis or end stage renal disease with peritoneal dialysis, as there may be obliteration of the peritoneal cavity for placement of cannulas and the attendant increased risk of enterotomy.Liver cirrhosis and portal hypertension(iv) General contraindications to laparoscopy (v) e.g. coagulopathy and ascites. Paediatic age group due to the potential of (vi) mesh migrationStrangulated hernias.(vii)
Lack of abdominal domain. This refers (viii) to patients with insufficient space in the abdomen to accommodate the contents of the hernia that are also at great risk for pneumoperitoneum.
Hernias in which the fascial edges extended (ix) lateral to the defect impossible. Defects in close proximity to the bony margins of the abdomen, especially those near the xiphoid, pose significant challenges for mesh fixation, though this is also true with open incisional herniorrhaphy

– 20 – Doctors News, Volume 16 / 2011
F e a t u r e
Preoperative preparationPatient should be counseled on expected outcome particularly on cosmesis and possible complication especially, the expectant management of seroma if it occurs.Bowel preparation is necessary to increase the size of the abdominal cavity and to prepare for bowel surgery should an enterotomy occur intraoperatively.Prophylaxis for DVT and respiratory dysfunction in high risk patients, and prophylactic antibiotics at the induction of general anesthesia.
Access and ports placement
Closed method with the veress needle or open (Hasson’s) technique depending on risk analysis is the most commonly used access methods. Optical trocar can also be used
Most preferred site is the Palmer’s point. Alternative sites include the right hypochondrium and the iliac fossae. Ultimately, the trochar position is determined by the location of the hernia.
Pneumoperitoneum is created and the defect localized during diagnostic laparoscopy. An angled (usually 30 degrees) scope is essential because dissection and repair are done on the undersurface of the anterior abdominal wall, which cannot be adequately visualized with a zero degree scope.
The baseball diamond concept is followed in port placement depending on location of the defect. Three trocars are usually adequate for small to moderate hernias with atleast one 10/12 mm for insertion of the mesh and tack applicator.
Complete adhesiolysis of the anterior abdominal wall is performed including release of the round ligament where necessary preferably with sharp and blunt dissection and avoiding energy sources as much as possible.
The content of the hernia sac(s) are reduced; the number of defect(s) confirmed and their extents mapped on the skin of the anterior abdominal wall.
Mesh placement and fixation
The prosthetic mesh is tailored to overlap the defect by 3-5 cm. In cases of incisional hernias the whole of the incision is covered by the prosthesis. More than one sheet of mesh may be needed depending on the locations of the defects and the size of the patient.

Doctors News, Volume 16
F e a t u r e
Dr Ndung’u is a Consultant General/Laparoscopic and Breast Surgeon based at Upper Hill Medical Centre. He is also a lecturer at the University of Nairobi’s School of Medicine.
Four sutures are placed extracorporeally at cardinal points of the mesh, marked on the skin and on the prosthesis. The side of the mesh to face the viscera is marked appropriately.
All necessary precautions are taken to avoid mesh contamination with skin pathogens.
The mesh is rolled, introduced into the abdomen through a 10/12 mm port and unrolled.
The sutures at the cardinal points are pulled transabdominally using a suture passer and knotted in a prefascial level. Additional transfascial sutures are placed around the prosthesis at 5 cm intervals. Further fixation is done with spiral tacks in a ‘double crown’ technique.
An intraabdominal drain has been used in cases of extensive adhesiolysis.
Final exploration for possible injuries is performed, all ports removed under direct vision. The pneumoperitoneum is released. The fascia at any trochar site 10mm in diameter or larger is closed. Careful closure of the site used for open insertion of the first trochar is mandatory to prevent trochar site hernia. The skin is then closed with subcuticular sutures and a compressive bandage applied for two to seven days depending on the size of hernia.
Postoperative care
The Foley catheter is removed at the end of the procedure. Unless adhesiolysis was minimal, patients are admitted to the hospital. Oral intake is begun immediately. Patients are discharged when oral intake is tolerated and pain is controlled with oral medication. Patients are informed that fluid may accumulate at the hernia site and are asked to report any fever or redness or severe pain. Finally, patients are instructed to resume all regular activities as soon as they feel capable.

– 22 – Doctors News, Volume 16 / 2011
D o c t o r P r o f i l e
Uasin Gishu, where Dr Kibosia hails from, is predominantly an agricultural area and most of the farmers’ children were not keen on going to school. “When Europeans exited the area, there were not many schools. There was actually one school in almost the whole division and pupils used to walk many miles to reach school. I was lucky the school was not very far from my home. I am probably the only one from those days who managed to go far in education.”
Coming from a polygamous family, Dr Kibosia says he enjoyed his childhood. “We were so many in our family that we rarely needed children from outside home to play with; it was lively,” he says. His father, who was a trader, was a hardworking man, and ensured his family was well taken care of. “I was born in Uasin Gishu District in 1957, went to school in Moiben Primary School and then we moved to Marakwet where my parents originally came from. I completed my primary school at Chebara Primary then joined Chebara Secondary School. From there I went to Nakuru High for form five and six, after which I went to the University of Nairobi medical school,” he fondly recalls.
Not one to give up easily when the going gets rough, Dr Kibosia remembers the one time he almost quit. “In 1984, I was posted to the Provincial Genaral Hospital, Machakos for internship. I remember my first day vividly; I was in the children’s ward and I did not sleep all night. There was a bad famine at that time that hit the area quite hard. The hospital was teeming with malnourished children who were very sick—and they kept coming in. The situation was so overwhelming that by the following day, I seriously doubted if I could do it. I almost quit.” However, seeing the weak children get well motivated him to hang on, and eventually he finished his internship in 1985.
“I was posted to Kitale District Hospital, and then in 1987 I went back to the University of Nairobi for my postgraduate in Surgery.” By 1991, after his postgraduate, Dr Kibosia had worked at various hospitals in Trans Nzoia, Eldoret District Hospital, Iten as well as Kenyatta National Hospital as Senior House officer, while doing a bit of private practice.
“In late 1991, I spearheaded a project that involved upgrading the Moi Teaching and Referral Hospital from a
For the better part of his career, Dr John Kibosia has never shied from taking head on, the daunting responsibility of transforming institutions for them to excel. His leadership capabilities were evident
from a tender age—when he finished high school in 1978, Kipsangui Secondary School in Marakwet appointed him head teacher. His recipe for success is simple. “Sometimes it is the surprisingly simple solutions that make the biggest difference, for example, being a surgeon I am meticulous with details and like cleanliness. A simple thing like maintaining high hygiene standards in hospitals can prevent many problems,” he explains. In addition, he says he is a good listener, prefers to involve people in decision-making and is quite passionate about his work.
This passion is what has driven him to actively mobilize resources that have made it possible for the Directorate of Health Services at the Prisons Department to set up health units in almost all correctional facilities in Kenya. “I was appointed Director of health services in the Prisons Department when death rate among inmates in Kenya was unacceptably high. Prior to that, there was no plan for inmates’ health at the Prisons Department; I had to start everything from scratch. I started with designing a work structure, incorporated it into the department, sought donors to fund our projects and then recruited staff. With time, the deaths have dropped by up to 80 percent and most of the inpatient wards we constructed are almost empty,” he says, as he displays images of numerous current projects in different parts of the country. The projects are mainly funded by donors.
Dr Kibosia’s desire to serve people stems from an experience he went through as a boy. “I was in form 5 and we were about to choose our courses then. Initially I was torn between studying agriculture and medicine, but my teachers were encouraging me to do medicine. At that time, I had an eye problem and could not see properly so I went to the provincial general hospital to seek treatment. I was not happy with the way people were treated. After being tossed around from one office to another, I eventually never was treated. I felt so bad that I made up my mind I was going to be a doctor, and a people’s doctor for that matter. I think health workers need to be more compassionate,” he adds.
Leading From the FrontBy Patricia Muigai

Doctors News, Volume 16
D o c t o r P r o f i l e
150 bed to a 500 bed facility. Moi University was gazetted in 1998 as a teaching hospital.” Within this period, Dr Kibosia was Medical Superintendent and consultant surgeon at MTRH, then Director.
He was then appointed Medical Superintendent of Provincial General Hospital, Nakuru, where he gave the hospital a facelift. “The Nakuru District hospital was in pretty bad shape when I moved there. By the time I was leaving in 2002, it was a completely different place,” says Dr Kibosia.
His next stop was the Kenya Medical Training College in Nairobi as director, then in 2005 as Chief Executive of Kenyatta National Hospital. At KNH, he implemented measures aimed at improving revenue collection, which resulted in more than 100 percent growth in revenue within just a year.
Of all his achievements however, Dr Kibosia’s most outstanding one, perhaps, is establishing prisons health services within the Prisons Department, which significantly reduced mortality rate in inmates. This was part of the prisons reforms that were established under the Office of the Vice President in 2002.
His professional training includes public health at Nordic
School of Public Health in Sweden, Palliative medicine at St Peter College in Oxford, UK, Health system Management at Galilee College (Israel), management of HIV in South Africa, and training in Corporate Governance. He is also a Fellow of the College of Surgeons, East, South and Central Africa.
Dr Kibosia believes in giving back, to society and is actively involved in activities aimed at improving the lives of communities at his rural home. He has assisted in putting up schools and churches, and is patron of the bursary fund for assisting needy students in Kapsowar, was key in establishing a medical training college at Kapsowar AIC. He is also is member of the board of Chebara Secondary and Prison Secondary Schools. In addition, he has served as chairman, Eldoret Rotary Club and Kenya Medical Association North Rift chain. About political leadership, Dr Kibosia says he is toying with the idea of getting into politics in future.
Despite his numerous responsibilities, Dr Kibosia does find the time to unwind. “There is always something to be fixed, which makes my schedule is full. Nevertheless, I enjoy a good read, golf and travelling when I am not working,” he says. He is married to Caroline; also, a doctor and they have three children who are all grown up— Kiplagat, Kigen and Kimosop.
Dr Kibosia (far right) and his family

– 24 – Doctors News, Volume 16 / 2011
F e a t u r e
The Prisons Department in Kenya has existed for the last one hundred years, having been started in 1911. After independence in 1963, the Prisons Service Department was established under an act
of parliament. Currently there are 106 prisons countrywide. The department falls under the Ministry of Home Affairs and is headed by a Commissioner. Working under the Commissioner of Prisons are eight directors, one of whom is the Director of Health Services, Dr John Kibosia. Being a member of the prisons senior management, he is involved in all aspects of prisons at the policy level.
For years, living conditions in prisons were far from good. However, the Government of Kenya introduced the Prison reform initiatives in 2002 aimed at restoring the dignity of inmates to acceptable levels. Part of these was provision of health care services.
Before the Directorate of Health services was established within the Prisons Department in 2006, all health matters were handled at individual prisons; sick inmates were taken to the nearest Ministry of Health facility, and sometimes the MoH would send health officers, to the prisons. The Kamiti Maximum Security Prison, being the largest maximum prison in Kenya and the only one where executions were carried out, was the only one that had a doctor from the Ministry of Health.
Dr Kibosia says, “In the Kenyan law, the right to freedom is the one that inmates don’t enjoy, but everyone has the right to adequate healthcare. When the reforms were started, there was an open door policy. It meant that people had access to prisoners. The civil society, particularly Kenya High Commission for Human Rights agitated for better health care for inmates,” he says.
Inmates were dying of preventable diseases such cholera, typhoid and TB by the numbers. “TB was particularly worrying because in 2004-2005, of the close to 1,000 people who died, 43 percent were because of TB. This was, made worse by HIV. Data was unavailable, but HIV prevalence among inmates was estimated to be between 10-12 percent,” says Dr Kibosia.
The first thing the Directorate of Health did was to put in place a health delivery system, as an emergency measure. “We did a quick scan to find out the causes of death and found that most of the causes were preventable and treatable.”
First, they made water provision and waste disposal top priority. “At that time, only 30 percent of prisons had adequate water. Then waste disposal was not acceptable. In 78 percent of prisons, they were using bucket toilets.”Now over 80 percent of prisons have clean water and most of the bucket toilets have been eliminated.
Next, they embarked on fighting vector-borne diseases. “We undertook regular spraying of prisons and as a result, malaria and diarrhea cases went down significantly. By 2010, the death rate was around 200 in a year. Before, it was about 1000. Our aim is to reduce this even further,” says the director.
One of the biggest challenges for prisons in Kenya is inadequate capacity. Every year, about 250,000-300,000 people pass through prison. While their capacity is 20,000 people, prisons have 50,000-54,000 people on average. “The other challenge is that there was no budget for our projects, but we have a small budget now. The government provides funds for drugs and medical equipment. Last year they gave us money that helped us put up four health facilities, and the other four we built with money from donors.”
After undertaking the initial measures to reduce mortality and morbidity in prisons, what followed was infrastructure development. Clinics have been constructed within the prisons facilities, and equipped. Some of the clinics have inpatient, X-ray and laboratory facilities. Now out of all the 106 prisons, 83 have health facilities, but even the rest have a place where inmates’ health needs are attended to.
“We have also now developed a policy for inmates and we have done an AIDS workplace policy.” This provides a framework to address HIV and AIDS effectively within the Prisons Service, and it applies to all management, staff, their families, prisoners and communities living around prisons. In addition, a scheme of service for health workers within prisons is now in place.
By Patricia Muigai
Reducing Disease and Death in Kenyan Prisons

Doctors News, Volume 16
F e a t u r e
“Within the last two years, we have recruited staff; doctors, nurses, clinical officers, radiographers etc, and this is going to be a continuous process. We are also dealing with other public health issues, and one of our recommendations to the government is provision of detergent, sanitary towels and bins for women and girls, and proper clothing, which also includes blankets and mattresses. We have also bought several ambulances.”
Furthermore, the department educates people on better living through health promotions, and almost every prisons officer has some health training in areas like VCT counseling and peer education, among others.
Previously, the Directorate did not have any data, and this made planning difficult. Students from University of Nairobi, Moi University, Kenyatta University and the Kenya Medical Training College who do their research in the Prisons Department have helped in providing useful data. “We now have enough information to enable us to do our strategic plan, which we’ve already started. The Strategic plan is going to guide us for future planning,” Dr Kibosia says.
Immediate plans include constructing a hospital for the staff, a psychiatric hospital at the Kamiti Prison and a drug and substance rehabilitation centre in Malindi. In addition, plans are underway to put up a maternity hospital at the Lang’ata Women’s prison.
Shimo la Tewa Prison Health Centre Laboratory at Shimo la Tewa Prison
Kodiaga Prison hospital’s X-Ray Inpatient ward at the Kodiaga Prison hospital
– 26 – Doctors News, Volume 16 / 2011
D i s e a s e P i c t o r i a l
Procedure in progress
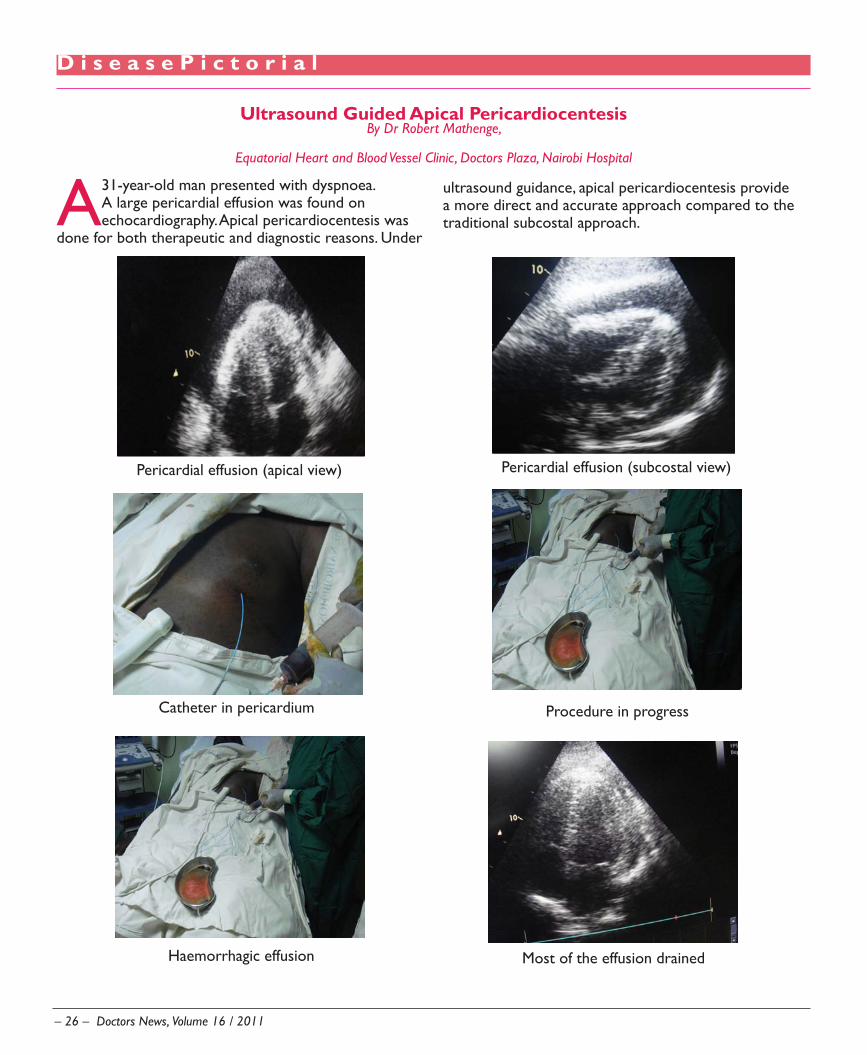
A 31-year-old man presented with dyspnoea. A large pericardial effusion was found on echocardiography. Apical pericardiocentesis was
done for both therapeutic and diagnostic reasons. Under
Ultrasound Guided Apical PericardiocentesisBy Dr Robert Mathenge,
Equatorial Heart and Blood Vessel Clinic, Doctors Plaza, Nairobi Hospital
Pericardial effusion (apical view)
Haemorrhagic effusion Most of the effusion drained
Pericardial effusion (subcostal view)
Catheter in pericardium
ultrasound guidance, apical pericardiocentesis provide a more direct and accurate approach compared to the traditional subcostal approach.
Doctors News, Volume 16
H o s p i t a l P r o f i l e
The Centre of Hope
The Coptic Orthodox Mission came to Kenya in 1976 with the desire to spread the Gospel of Christ and a spirit of service. With time, the Coptic Ministry grew tremendously, and today
Kenya has 40 churches and numerous projects, including the Coptic Hospital and Hope Centre in Nairobi, an orphan’s project, a street children’s project and many more. The Coptic Hospital’s Medical Director, Dr Sakr
attributes the hospital’s growth mainly to the dedicated staff and support from the Coptic community. “Many people were dedicated and worked hard to get the hospital where it is today. As a mission hospital, we know we are doing this for the glory of God. We are fulfilling our duty to help those in need and we instill the same spirit in our entire staff.”
Coptic Hospital’s Medical Director, Dr Rafie Sakr

– 28 – Doctors News, Volume 16 / 2011
H o s p i t a l P r o f i l e
Dr Sakr, who is a general surgeon, studied in Cairo, Egypt and came to Kenya in 1998. “When I finished my residency, Bishop Paul who is head of the mission of the Coptic Church and who is also my spiritual father, talked to me about coming to serve in the mission hospitals. I went to the Coptic Hospital in Lusaka, Zambia. It is one of the best in Lusaka and I was there for a year. In 1998, the bishop told me that there was more need in Nairobi and I moved here.”
The Coptic Hospital in Nairobi was started in 1994 as a small outpatient clinic on Ngong Road. At first, it was an arrangement between the Coptic Church and UNHCR to treat and accommodate refugees from war-torn countries. “The refugees had many needs besides medical needs. Some came here without any family or friends and many of their medical problems actually stemmed from psychological trauma. They needed hope. We were well placed to give them professional and spiritual counseling alongside medical care,” Dr
Sakr says. The church also noted that a major problem facing the people it served was lack of access to proper medical care. Most could not afford it. They decided to do something about it by setting up a medical facility offering good quality but affordable medical care.
The hospital was then upgraded to a nursing home and started admitting patients in 1996. In 2000 it became a fully fledged hospital. “The hospital has grown rapidly since then. I remember we had five nurses and two doctors at the beginning. Now we have more than 90 nurses and about 25 resident doctors in addition to clinical officers in different specialities of medicine. We also have many visiting and admitting doctors,” says Dr Sakr. He adds that this growth has put pressure on the facilities at the hospital. “Bishop Paul is a medical doctor by training. He knows what the hospital needs in terms of infrastructure. He has been very helpful in sourcing donations from the Coptic community in other countries.”

Doctors News, Volume 16
H o s p i t a l P r o f i l e
With time, Dr Sakr noticed a trend in which more and more patients were presenting with HIV. “At first we were in a dilemma because then we lacked the medical knowledge and experience for treating the disease and so we felt the need to improve on this area. Fortunately, I met a doctor from University of Washington in Seattle, USA who was doing HIV research at Kenyatta. He had heard about the Hope Clinic, which was the result of a renowned low-cost ARV program, which Coptic had pioneered in the country in 2002. That marked the beginning of a big project that we are still running now.”
The Coptic Hope Centre for Infectious Diseases is a comprehensive HAART treatment facility jointly established by the Coptic Orthodox Mission and the University of Washington (UW) in Nairobi, Kenya and is funded by the U.S. Government PEPFAR Initiative. Since it was launched, the Centre has initiated fully comprehensive and free HIV/AIDS management to nearly 5,000 patients. Half of these are on HAART.
Coptic Hospital prides itself in offering quality services that include outpatient and round the clock emergency services, specialized clinics, a comprehensive dental unit, inpatient, two well-equipped theatres, HDU, maternity, 10 most advanced dialysis machines and a diagnostic centre. There are also laboratory services, a well-stocked pharmacy, physiotherapy and occupational therapy unit and around the clock ambulance services. “In the last two years we have established a kidney dialysis unit, an ICU and improved our theatre. We hope to start a cancer centre in the near future, mammogram, CT scans and MRI. We shall also expand the dialysis unit. To this end, construction is underway for a much bigger facility with a bed capacity of 250 beds and six theatres. “We
– 30 – Doctors News, Volume 16 / 2011
H o s p i t a l P r o f i l e
aim to have all our services housed under one roof and hope that the construction will be complete in a year,” adds Dr Sakr.
In 2005, the Coptic Hospital opened the Coptic Medical Centre, an outpatient clinic in the heart of the Industrial Area, Nairobi. Thousands of the labourers from the surrounding slums get outpatient services at subsidized rates.
The Coptic Church also opened the Coptic Nursing Home in Maseno in January of 2004. Besides offering medical and spiritual care in this area, the church is fighting poverty and medical illiteracy through the clinic.
So how does Coptic Hospital sustaining itself? “We are a non-profitable organization offering services to those who can hardly afford. It is more like charity. Even so, we need to keep the hospital running and therefore, we strive to make our services affordable while offering quality. As long as we can keep the hospital running, we are happy.”
Dr Sakr says that it is because of team work that the hospital has managed to achieve its goals. “We are greatful to God and to all those who have contributed to our growth. We could not do it without their support,” he concludes.
An impression of the New facility under construction