documentation of tricuspid regurgitation by radionuclide ... · radionucide angiocardiography is a...
TRANSCRIPT
British HeartJournal, 1974, 36, IOI9-I022.
Documentation of tricuspid regurgitationby radionuclide angiocardiography
Fred S. Mishkin and Marvin E. MishkinFrom the Division of Nuclear Medicine, Department of Radiology, Martin Luther King, Jr. General Hospital,Los Angeles, California, U.S.A.
Review of the radionuclide cardiac angiograms of 82 patients studied during the past year showed reflux ofactivity down the inferior vena cava in 7, all ofwhom had clinical evidencefor or clinical conditions associatedwith tricuspid regurgitation. Analysis of theflow of the radioactive bolus through the cardiac chambers demon-strates that the inferior vena cava fills only after activity enters the right ventricle and that filling is mostpronounced during ventricular systole. In one case of right-sided endocarditis in which the characteristicmurmur of tricuspid regurgitation was heard, thisfinding could not be demonstrated. These results suggest thatradionuclide angiocardiography can provide a sensitive noninvasive means for documenting the presence oftricuspid regurgitation.
Although its incidence is uncertain, tricuspidregurgitation in the presence of mitral or aorticvalve disease may signify serious haemodynaniicabnormalities. Coexisting valvar disease responsiblefor functional tricuspid regurgitation or associatedwith an organic tricuspid lesion may make the clini-cal diagnosis difficult. Some have suggested that thefailure to replace surgically the tricuspid valve whenindicated at the time of repair of the left heartvalves may result in circulatory embarrassment sosevere that it precludes separation of the patientfrom cardiopulmonary support (Starr, Herr, andWood, I967). For these reasons an objective meansfor demonstrating the presence of tricuspid re-gurgitation would be welcome.
Contrast angiography uniquely provides preciseanatomical detail, but catheter position through thevalve and the high pressure system necessary todeliver the contrast medium may result in spuriousreflux. Haemodynamic data show that with tricus-pid regurgitation right atrial mean pressure exceedssuperior vena caval pressure (Bloomfield et al.,I946), so that during ventricular systole thereshould be reversal of flow from the right atrium tothe vena cava (Muller and Shillingford, i954).Radionucide angiocardiography is a noninvasiveprocedure permitting ready repetition on an out-patient basis and produces no direct haemodyn-amic changes (Kriss et al., I971). Our experiencesuggests that this technique provides a sensitive,Received I8 March I974.
objective means for documenting the flow reversalwhich occurs in tricuspid regurgitation.
MethodsThe records and radionuclide angiocardiograms of all 82patients referred for the procedure during the past yearwere reviewed. Radionuclide angiocardiography wasperformed with a few modifications according to stan-dard technique (Kriss et al., I97I). A scintillationcamera positioned over the cardiac area recorded thetransit of an intravenously injected radioactive bolus. Acollimeter with many parallel holes projects the gammarays onto a sensitive crystal surface coupled to anarray of photomultiplier tubes which almost instant-aneously detects the radioactive emissions occurring ina 28 cm diameter field. This is done using X and Y axiselectronic positioning circuits. These detected events areelectronically transcribed to an oscilloscope from whichthey may be recorded using sequential time exposures.Alternatively, the events which are analogue in naturemay be converted to digital signals and stored on videotape or other digital storage devices.
Usually, parallel hole collimators with holes verticallyoriented to the camera surface are used, but in order toobtain a more informative oblique view, the camera wasequipped with a collimator having the parallel holesangled 200 from vertical. Bringing the collimator flushagainst the chest with the holes angled towards thepatient's right produces a 200 left anterior oblique view,without the loss of photon yield which results when astraight parallel hole collimator is drawn away from thechest to place it at a 200 oblique position to the patient.The radionuclide, usually 20 mCi of D9mTc as pertechne-
on May 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.36.10.1019 on 1 October 1974. D
ownloaded from

x020 Mishkin and Mishkin
tate or labelled serum albumin, is placed in a venotubereservoir, and then flushed as a bolus through a scalpvein needle into the external jugular system, preferredbecause of its lack of valves, or into a medial antecubitalvein leading to the basilic vein.The passage of the bolus is recorded along with the
electrocardiogram on videotape. A complete account ofthis method for obtaining and storing the data is availablein the work of Ashburn et al. (I973). These data arelater played back and photographed onto 4 x 5 x-rayfilm during o 5 or i-o sec time intervals depending uponthe circulation time. Data are also played back using agating system coupled with the electrocardiographicsignal so that recording may be made only during dia-stole using the 50 millisecond portion of the data asso-
A
C
ciated with the QRS complex, or only during systoleusing the 50 millisecond interval associated with theinitial portion of the T wave. Such data recording allowsanalysis and separation of those events and motionsoccurring during systole from those occurring duringdiastole (Zaret et al., I97I). The data are also played intoan online computer for generation of time-activity histo-gram curves which may be selected from any region ofthe heart and lungs (Weber, dos Remedios, and Jasko,I972).
FindingsIn 7 cases, activity appeared in the inferior vena cavabefore circulation of the bolus through the lungs
B
D
FIG. I Sequential one-second frames from the radionuclide angiocardiogram in a patientwith cardiomyopathy showing regurgitation down the inferior vena cava (arrow) during rightheart transit of the bolus. In A, the superior vena cava is filled; in B, the right atrium; in C,the right ventricle; and in D, the pulmonary outflow tract.
on May 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.36.10.1019 on 1 October 1974. D
ownloaded from

Tricuspid regurgitation 1021
TABLE Clinical data in patients with tricuspid regurgitation
Case Age (yr) Cardiovascular Rhythm Congestive PulsatileNo. and sex disease failure liver
I 74 F Hypertension; Sinus Yes Noaortic insufficiency
2 82 F Arteriosclerosis Atrial Yes and Yesfibrillation right-sided
failure3 8 dy F None Sinus No No
(pneumonitis) tachycardia4 67 F Cardiomyopathy Sinus Yes No5 60 M Rheumatic mitral Atrial Yes Yes
stenosis; fibrillationarteriosclerosis
6 9i M Arteriosclerosis Atrial Yes and Nofibrillation right-sided
failure7 50 F Cardiomyopathy Sinus Yes No
(Fig. i). Each patient either had clinically certainevidence of tricuspid regurgitation or a situationassociated with functional tricuspid regurgitationcaused by increased resistance to passage of the bolusacross the tricuspid valve (Table). In one casestudied, a drug addict with right-sided staphylo-coccal endocarditis, there was a systolic murmurprobably accentuated during inspiration, but noreflux was demonstrated. It is not certain the patienthad tricuspid regurgitation. That the activityactually represents regurgitation from the right
ventricle rather than from the atrium is demon-strated by two findings. First, the activity in thevena cava does not appear until there is activity inthe right ventricle. This is shown by comparing thepeaks of time-activity histograms generated fromthe right atrium, the outflow portion of the rightventricle, and the inferior vena cava (Fig. 2). Peakactivity in the vena cava occurs only after the peakin the right ventricular outflow tract. Secondly,gated images for the same period show much moreactivity in the inferior vena cava during ventricular
.0I
*W Sx
*0
E0
-
c
I 0
00
0000
Right atrium
0o'. ..I.IIII.............I
ETime in half-seconds*L
.
S.0 0
00 00
000 0
0 0
.._'
E U
*
iRight ventricle
l.
UTime in half-seconds
r Io xI,'
WVIIII
0
l
ll
.2!a
C L-o
C
.E0
I
*
0
*0
* 0
0
S ~~~00 0~~~
*** 0
0
Inferior vena cava
II
o'IIIIIIIIIII IIf illIIiI i
-e ---in----
2-Time in half-seconds
FIG. 2 Time-activity histograms generatedfrom the right atrium, right ventricle, and inferiorvena cava. Each point represents a half-second time interval. Peak activity can be seen to occur inthe right atrium at 2 seconds and in the right ventricle at 4-5 seconds. A double peak is seen in theinferior vena cava, thefirst at 4-5 seconds, and the second and higher peak at 6 seconds.
00
0
u
E
Fi
on May 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.36.10.1019 on 1 October 1974. D
ownloaded from
1022 Mishkin and Mishkin
Diastole Systole
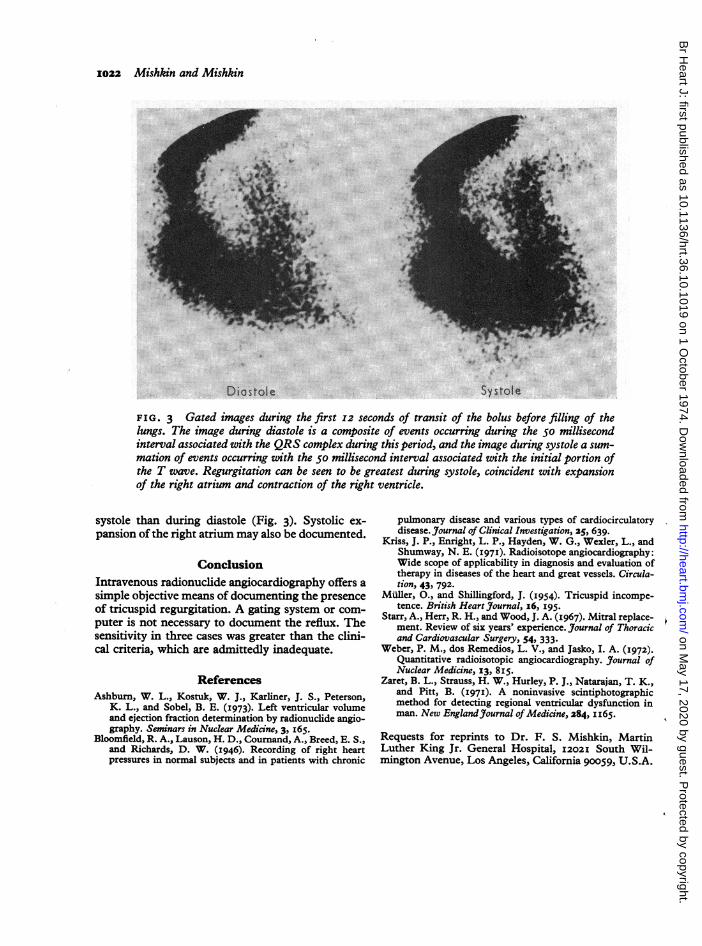
FIG. 3 Gated images during the first 12 seconds of transit of the bolus before filling of thelungs. The image during diastole is a composite of events occurring during the 50 millisecondinterval associated with the QRS complex during this period, and the image during systole a sum-mation of events occurring with the 50 millisecond interval associated with the initial portion ofthe T wave. Regurgitation can be seen to be greatest during systole, coincident with expansionof the right atrium and contraction of the right ventricle.
systole than during diastole (Fig. 3). Systolic ex-pansion of the right atrium may also be documented.
ConclusionIntravenous radionuclide angiocardiography offers asimple objective means of documenting the presenceof tricuspid regurgitation. A gating system or com-puter is not necessary to document the reflux. Thesensitivity in three cases was greater than the clini-cal criteria, which are admittedly inadequate.
ReferencesAshburn, W. L., Kostuk, W. J., Karliner, J. S., Peterson,
K. L., and Sobel, B. E. (1973). Left ventricular volumeand ejection fraction determination by radionuclide angio-graphy. Seminars in Nuclear Medicine, 3, I65.
Bloomfield, R. A., Lauson, H. D., Cournand, A., Breed, E. S.,and Richards, D. W. (1946). Recording of right heartpressures in normal subjects and in patients with chronic
pulmonary disease and various types of cardiocirculatorydisease. Journal of Clinical Investigation, 25, 639.
Kriss, J. P., Enright, L. P., Hayden, W. G., Wexler, L., andShumway, N. E. (I97I). Radioisotope angiocardiography:Wide scope of applicability in diagnosis and evaluation oftherapy in diseases of the heart and great vessels. Circula-tion, 43, 792-
Miiller, O., and Shillingford, J. (I954). Tricuspid incompe-tence. British Heart Journal, I6, I95.
Starr, A., Herr, R. H., and Wood, J. A. (I967). Mitral replace-ment. Review of six years' experience. Journal of Thoracicand Cardiovascular Surgery, 54, 333.
Weber, P. M., dos Remedios, L. V., and Jasko, I. A. (1972).Quantitative radioisotopic angiocardiography. Journal ofNuclear Medicine, I3, 8i5.
Zaret, B. L., Strauss, H. W., Hurley, P. J., Natarajan, T. K.,and Pitt, B. (197I). A noninvasive scintiphotographicmethod for detecting regional ventricular dysfunction inman. New England3Journal of Medicine, 284, iI65.
Requests for reprints to Dr. F. S. Mishkin, MartinLuther King Jr. General Hospital, I202I South Wil-mington Avenue, Los Angeles, California 90059, U.S.A.
:- 9 ik
V
0
#1
. -lw X%- w
.4,::,: .: :,,. ::i,.. t
"' "'
ilV1.
on May 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.36.10.1019 on 1 October 1974. D
ownloaded from