does patient blood glucose monitoring improve diabetes
TRANSCRIPT

Patient Blood Glucose Monitoring
991
McAndrew et al
Does Patient Blood GlucoseMonitoring ImproveDiabetes Control?A Systematic Review of the Literature
Objective
The purpose of this systematic review was 2-fold: first, toperform a comprehensive review of relevant studies onthe impact of self-monitoring of blood glucose (SMBG)on HbA1c levels for patients with type 2 diabetes melli-tus and, second, to explore mediators and moderatorswithin a self-regulation framework.
Data Sources
Five databases—Medline, PsychInfo, Cochrane Databaseof Systematic Reviews, Cochrane Central Register ofControlled Trials, and Cumulative Index to Nursing &Allied Health Literature (CINAHL)— were searched.
Study Selection
Cross-sectional, longitudinal, and randomized controltrials from 1990 to 2006, which included patients withtype 2 diabetes not on insulin, were reviewed. In total,6769 studies were screened for inclusion, 89 were retrievedfor detailed analysis, and 29 met criteria for inclusion inthe review.
Data Extraction
Data on the impact of SMBG on HbA1c, potential medi-ators and moderators, study design and participants, andlimitations of each study were retrieved.
Lisa McAndrew, MS
Stephen H. Schneider, MD
Edith Burns, MD
Howard Leventhal, PhD
From Rutgers University, Department of Psychology,Institute for Health & Behavior, New Brunswick,New Jersey (Ms McAndrew, Dr Leventhal); RobertWood Johnson Medical School, Division ofEndocrinology, Diabetes, Metabolism, New Brunswick,New Jersey (Dr Schneider); and Department ofMedicine, Medical College of Wisconsin, Milwaukee(Dr Burns). This article was funded through funds fromthe National Institute of Health, grant R24 AG023958,Center for the Study of Health Beliefs and Behaviors.
Correspondence to Howard Leventhal, PhD, RutgersUniversity, Department of Psychology, Institute forHealth & Behavior, 30 College Ave, New Brunswick,NJ 08901; e-mail: [email protected].
DOI: 10.1177/0145721707309807
TDE309807.qxd 11/7/2007 11:17 AM Page 991

Data Synthesis
Twenty-nine studies were included in this review: 9cross-sectional studies, 9 longitudinal studies, and 11randomized controlled trials. Evidence from the cross-sectional and longitudinal studies was inconclusive.Evidence from randomized controlled trials suggests thatSMBG may lead to improvements in glucose control.Very few studies examined potential mediators or mod-erators of SMBG on HbA1c levels.
Conclusions
SMBG may be effective in controlling blood glucose forpatients with type 2 diabetes. There is a need for studiesthat implement all the components of the process forself-regulation of SMBG to assess whether patient use ofSMBG will improve HbA1c levels.
This review summarizes current studies on therelationship between patient self-monitoringof blood glucose (SMBG) and the control oftype 2 diabetes. Although there is some evi-dence to suggest that SMBG is effective in
improving blood glucose levels among patients with type2 diabetes not on insulin, the evidence is still unclear andcontested. In this article, assessment of these studiesfocuses on the overall efficacy of monitoring on glucosecontrol and, more important, examines what the studiesdo and do not tell us as to how, and for whom, SMBGmay be effectively incorporated into patients’ voluntary,self-regulatory behavior to achieve effective blood glu-cose control. The authors use the commonsense model ofself-regulation1,2 as the theoretical framework for apprais-ing whether the studies address the “for whom” and“how” questions. The use of the model is consistent withcalls to make theory more explicit in research on diabeteseducation3 and to state hypotheses a priori.4
The current debate is focused on whether SMBG isefficacious among patients with type 2 diabetes who arenot on insulin.5,6 The American Diabetes Association(ADA), in its Clinical Practice Recommendations 2007,has found sufficient evidence to recommend SMBG forpatients prescribed multiple daily insulin injections(ADA level of evidence = A); the recommendation for
the use of SMBG among patients not on insulin, in addi-tion to recommendations for when and how patientsshould use SMBG, is based on less sufficient evidence(ADA level of evidence = E).7 The ambiguity regardingthe use of SMBG for patients not on insulin arises asprior studies and reviews have focused on the overallimpact of SMBG on HbA1c and have not assessedwhether the implementation was sufficiently comprehen-sive to address each of the factors needed to create acomplete feedback system for effective, patient-centeredself-management.6,8-11 The central issue for both theoryand practice is to identify the conditions under whichself-monitoring, a patient-centered “executive controlprocess,” can control the biomarkers that are ordinarilyregulated by complex, automatic, involuntary processesin patients without diabetes. Teaching volitional manage-ment to patients with type 2 diabetes involves more thaninstructing them in the use of a meter. SMBG can only beeffective if patients recognize when a reading is high orlow; make changes in oral medication, diet, or exercise inresponse to the reading; and evaluate the efficacy of theseself-management behaviors with a subsequent reading.The patients also must learn that these objective readingsand not their subjective feelings (fatigue, dizziness, etc)are valid indicators of elevated blood glucose and thebasis for guiding self-management. Learning to useobjective readings rather than subjective feelings asthe target for self-regulation means that patients mustignore the commonsense knowledge of their personalhistories and culture that define symptoms and dysfunc-tion as valid signs of illness.12,13
The logic underlying this study’s view of patient-centered self-management (ie, the commonsense model ofself-regulation1-3) led to the expectation that the efficacyof SMBG would depend on whether the interventionscreated a patient-centered behavioral control system thatwould address the patient’s skills in (1) taking a bloodglucose reading; (2) interpreting the reading as a targetfor action; (3) perceiving linkages between specific behav-iors (diet, exercise) and the reading (ie, which behaviorslower an above-target reading and which raise a below-target reading); (4) implementing action plans (ie, behav-ioral and treatment adjustments) in response to SMBG;(5) giving less weight to subjective symptoms that are thebasis for commonsense decisions that one is sick or well,as these cues are invalid guides for the regulation of bloodglucose levels; (6) incorporating the behavioral systeminto the patient’s ongoing daily behavioral patterns to
The Diabetes EDUCATOR
992
Volume 33, Number 6, November/December 2007
TDE309807.qxd 11/7/2007 11:17 AM Page 992

eventually become automatic; and (7) viewing difficul-ties in achieving control as issues of adjusting the behav-ioral treatment, not deficits in personal motivation orcompetence for self-management. The goals of this sys-tematic review are (1) to report on the overall impact ofSMBG on HbA1c for patients with type 2 diabetes and(2) to examine whether existent studies have identifiedand assessed the mediators and moderators comprisingthe processes underlying the relationship of SMBG toHbA1c.
Method
Searching
Five databases were searched: Medline, PsychInfo,Cochrane Database of Systematic Reviews (first quarter2006), Cochrane Central Register of Controlled Trials(first quarter 2006), and Cumulative Index to Nursing &Allied Health Literature (CINAHL). Search terms includedwords for (1) diabetes mellitus/diabetes, (2) monitoring/self-monitoring, and (3) glucose/blood glucose/bloodglucose in each database.
Selection
All citations were entered into endnotes and dupli-cates removed. Reviewer LD screened the remainingentries’ titles and abstracts for articles that met the inclu-sion and exclusion criteria. The articles were thenretrieved and read for final inclusion.
The inclusion criteria were empirical studies pub-lished since 1990 that included patients with type 2 dia-betes who were not using insulin and that examined theeffect of SMBG on HbA1c levels, the primary outcomemeasure, and the currently accepted standard for moni-toring long-term glucose control.14-18 Because a majorobjective of this review is to identify conditions thatmediate the efficacy of SMBG, this study retained cross-sectional, longitudinal, and randomized control trials(RCTs), as well as studies that included both patientswho were on and not on insulin and studies with patientswith both type 2 and type 1 diabetes.
Studies that focused on special subsets of patients,such as adolescents with type 2 diabetes and patientswith gestational diabetes and patients dealing with blind-ness or renal failure, were excluded, as these patients arenot representative of the broader population of patients
with type 2 diabetes. It is unclear how findings in spe-cialized populations would illuminate the efficacy ofmonitoring in the larger population. Studies were alsoexcluded if monitoring was performed by someone otherthan the patient (eg, a health professional) or used fruc-tosamine monitoring. Although this discussion isinformed by findings from relevant qualitative studies, acomprehensive review of these studies was not con-ducted as they do not provide quantitative results of theeffect of SMBG on HbA1c. Studies in which SMBG wasembedded in complex interventions that used multiplefactors unrelated to SMBG monitoring were alsoexcluded. The decision to exclude studies publishedbefore 1990 was based on substantial improvements inease and accuracy of monitoring from that time to thepresent. As the efficacy of monitoring for patients oninsulin is accepted,7 studies assessing efficacy of moni-toring only for patients on insulin were excluded. Finally,only studies available in English were reviewed.
Validity Assessment
Studies were reviewed for the ADA evidence grad-ing criteria by LD, and questions regarding gradingwere referred to and resolved by the medical membersof the team (SHS, EB). Only studies that met ADA evi-dence grading criteria A, B, or C were included in thereview.
Data Abstraction
The data were collected and organized by LD, and atrained research assistant reviewed the data for accuracy.Both the results of the data abstraction and questionsabout the data were then reviewed and discussed in detailwith all authors.
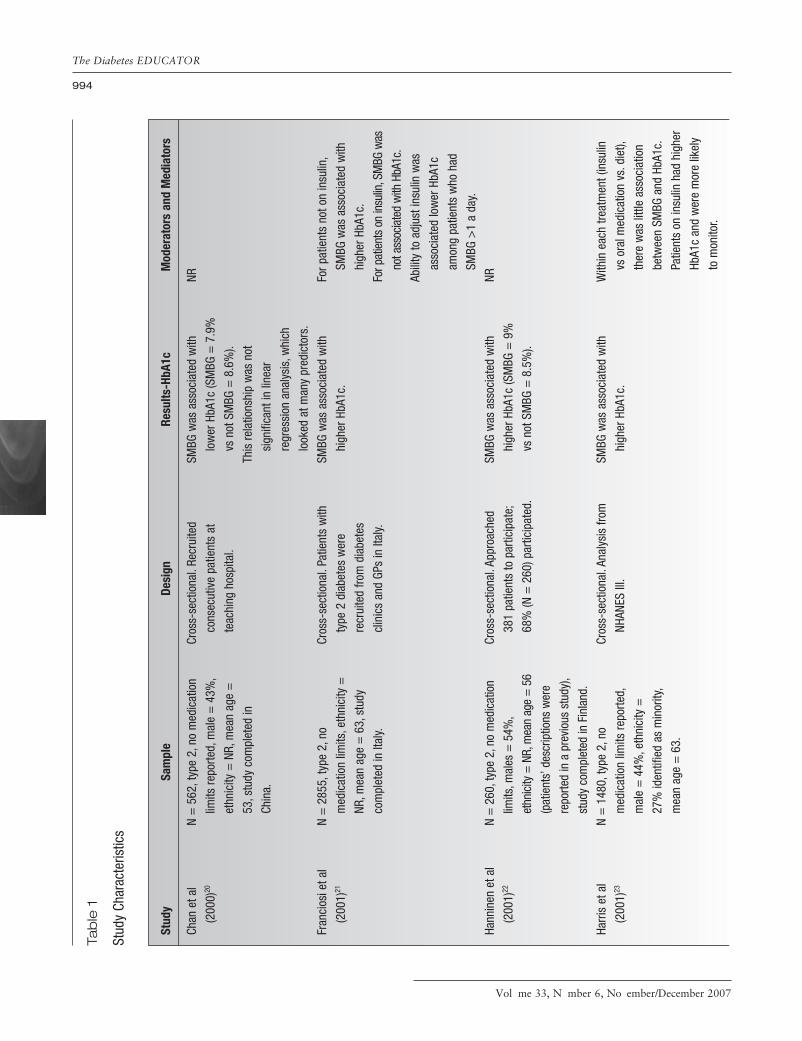
Study Characteristics
Data were collected on the primary outcome (HbA1c),study population (number of participants, gender, ethnic-ity, current medication used by patients, and type of dia-betes), study design, mediators and moderators, andlimitations.
Data Synthesis
Data are summarized in Table 1. Missing data weremarked “not reported” (NR) within the table.
Patient Blood Glucose Monitoring
993
McAndrew et al
(text continues on p. 1003)
TDE309807.qxd 11/7/2007 11:17 AM Page 993
The Diabetes EDUCATOR
994
Volume 33, Number 6, November/December 2007
Tab
le 1
Stud
y Ch
arac
teris
tics
Chan
et a
l
(200
0)20
Fran
cios
i et a
l
(200
1)21
Hann
inen
et a
l
(200
1)22
Harr
is e
t al
(200
1)23
N =
562
,typ
e 2,
no m
edic
atio
n
limits
repo
rted,
mal
e =
43%
,
ethn
icity
= N
R,m
ean
age
=
53,s
tudy
com
plet
ed in
Chin
a.
N =
285
5,ty
pe 2
,no
med
icat
ion
limits
,eth
nici
ty =
NR,m
ean
age
= 6
3,st
udy
com
plet
ed in
Ital
y.
N =
260
,typ
e 2,
no m
edic
atio
n
limits
,mal
es =
54%
,
ethn
icity
= N
R,m
ean
age
= 5
6
(pat
ient
s’ d
escr
iptio
ns w
ere
repo
rted
in a
pre
viou
s st
udy)
,
stud
y co
mpl
eted
in F
inla
nd.
N =
148
0,ty
pe 2
,no
med
icat
ion
limits
repo
rted,
mal
e =
44%
,eth
nici
ty =
27%
iden
tifie
d as
min
ority
,
mea
n ag
e =
63.
Cros
s-se
ctio
nal.
Recr
uite
d
cons
ecut
ive
patie
nts
at
teac
hing
hos
pita
l.
Cros
s-se
ctio
nal.
Patie
nts
with
type
2 d
iabe
tes
wer
e
recr
uite
d fro
m d
iabe
tes
clin
ics
and
GPs
in It
aly.
Cros
s-se
ctio
nal.
Appr
oach
ed
381
patie
nts
to p
artic
ipat
e;
68%
(N =
260
) par
ticip
ated
.
Cros
s-se
ctio
nal.
Anal
ysis
from
NHAN
ES II
I.
SMBG
was
ass
ocia
ted
with
low
er H
bA1c
(SM
BG =
7.9
%
vs n
ot S
MBG
= 8
.6%
).
This
rela
tions
hip
was
not
sign
ifica
nt in
line
ar
regr
essi
on a
naly
sis,
whi
ch
look
ed a
t man
y pr
edic
tors
.
SMBG
was
ass
ocia
ted
with
high
er H
bA1c
.
SMBG
was
ass
ocia
ted
with
high
er H
bA1c
(SM
BG =
9%
vs n
ot S
MBG
= 8
.5%
).
SMBG
was
ass
ocia
ted
with
high
er H
bA1c
.
NR For p
atie
nts
not o
n in
sulin
,
SMBG
was
ass
ocia
ted
with
high
er H
bA1c
.
For p
atie
nts
on in
sulin
,SM
BG w
as
not a
ssoc
iate
d w
ith H
bA1c
.
Abili
ty to
adj
ust i
nsul
in w
as
asso
ciat
ed lo
wer
HbA
1c
amon
g pa
tient
s w
ho h
ad
SMBG
>1
a da
y.
NR With
in e
ach
treat
men
t (in
sulin
vs o
ral m
edic
atio
n vs
.die
t),
ther
e w
as li
ttle
asso
ciat
ion
betw
een
SMBG
and
HbA
1c.
Patie
nts
on in
sulin
had
hig
her
HbA1
c an
d w
ere
mor
e lik
ely
to m
onito
r.
Stud
ySa
mpl
eDe
sign
Resu
lts-H
bA1c
Mod
erat
ors
and
Med
iato
rs
TDE309807.qxd 11/7/2007 11:17 AM Page 994

Patient Blood Glucose Monitoring
995
McAndrew et al
Jaw
orsk
a et
al
(200
4)26
Mitc
hell
et a
l
(200
4)25
Oki e
t al (
1997
)24
Patri
ck e
t al
(199
4)27
Rost
et a
l
(199
0)19
N =
218
,typ
e 2,
no m
edic
atio
n
limits
repo
rted,
mal
es =
31%
,eth
nici
ty =
NR,
mea
n
age
= 6
2%,s
tudy
com
plet
ed
in P
olan
d.
N =
434
,typ
e 2,
no in
sulin
,
mal
e =
52%
,eth
nici
ty =
NR,
mea
n ag
e =
64,
stud
y
com
plet
ed in
Can
ada.
N =
98,
type
2,n
o m
edic
atio
n
limits
,mal
e =
29%
,eth
nici
ty:
AA =
69%
,C=
27%
,H=
2%,
O =
2%
,mea
n ag
e =
56.
N =
200
,typ
e 2,
no in
sulin
,
mal
e =
52%
,eth
nici
ty =
NR,
mea
n ag
e =
65.
N =
84,
type
2,n
o m
edic
atio
n
limita
tions
,mea
n ag
e =
56,
32%
= m
ale,
ethn
icity
= N
R.
Cros
s-se
ctio
nal.
Recr
uite
d
patie
nts
who
pre
sent
ed fo
r
outp
atie
nt c
are.
Cros
s-se
ctio
nal.
This
stu
dy
repo
rted
base
line
data
from
a
rand
omiz
ed c
ontro
l tria
l.
Patie
nts
wer
e gi
ven
a
ques
tionn
aire
and
sen
t to
have
HbA
1c te
sted
.
Cros
s-se
ctio
nal.
A to
tal o
f 98
cons
ecut
ive
patie
nts
who
pres
ente
d fo
r rou
tine
care
.
Cros
s-se
ctio
nal.
Com
pare
d
patie
nts
who
mon
itore
d
(blo
od,u
rine,
or b
oth)
to
thos
e w
ho d
id n
ot m
onito
r.
Cros
s-se
ctio
nal.
Surv
eyed
patie
nts
with
type
2 d
iabe
tes
hosp
italiz
ed fo
r ele
ctiv
e
adm
issi
on.
SMBG
was
not
ass
ocia
ted
with
HbA1
c.
SMBG
was
not
ass
ocia
ted
with
HbA1
c.
SMBG
was
not
ass
ocia
ted
with
HbA1
c.
SMBG
was
not
ass
ocia
ted
with
HbA1
c.
SMBG
was
ass
ocia
ted
with
low
er H
bA1c
.
With
in e
ach
treat
men
t gro
up
(insu
lin v
s or
al m
edic
atio
n),
SMBG
was
not
rela
ted
to
HbA1
c.Am
ong
patie
nts
who
repo
rted
the
abili
ty to
cha
nge
insu
lin d
ose
base
d on
SM
BG,
SMBG
was
not
rela
ted
to
HbA1
c.
NR No d
iffer
ence
in H
bA1c
betw
een
patie
nts
who
had
SMBG
<7/
wk
and
patie
nts
who
had
SM
BG >
7/w
k.
SMBG
not
ass
ocia
ted
with
HbA1
c w
hen
anal
yzed
bas
ed
on tr
eatm
ent g
roup
(ins
ulin
vs d
iet/o
ral).
No d
iffer
ence
bet
wee
n pa
tient
s
who
repo
rted
that
they
wou
ld
act o
n m
onito
ring
resu
lts a
nd
thos
e w
ho re
porte
d th
at th
ey
wou
ld n
ot a
ct.
Not t
este
d di
rect
ly,bu
t the
rela
tions
hip
of S
MBG
to H
bA1c
was
inde
pend
ent
of o
ther
sel
f-ca
re
beha
vior
s.
(con
tinue
d)
TDE309807.qxd 11/7/2007 11:17 AM Page 995

The Diabetes EDUCATOR
996
Volume 33, Number 6, November/December 2007
Blon
de e
t al
(200
2)34
Karte
r et a
l
(200
1)33
Klei
n et
al
(199
3)35
Mei
er e
t al
(200
2)32
N =
228
,typ
e 2,
no m
edic
atio
n
limits
repo
rted,
mal
e =
NR,
ethn
icity
= N
R,m
ean
age
=
NR (a
ge ra
nge,
35-6
5).
N =
23
412,
type
s 1
& 2,
no
med
icat
ion
limits
,mal
e =
52%
,eth
nici
ty:C
= 6
0%,
AA =
11%
,H =
8%
,A/P
I =
12%
,NA
= 1
%,O
= <
1%,
M =
7%
,mea
n ag
e =
60.
N =
229
,typ
e 2,
no m
edic
atio
n
limits
,mal
e =
97%
,eth
nici
ty:
AA =
11%
,C =
68%
,H =
20%
,mea
n ag
e =
62,
recr
uite
d fro
m V
A.
N =
146
7,ty
pe 2
,no
insu
lin,
mal
e =
98%
,eth
nici
ty =
NR,
mea
n ag
e =
64,
patie
nts
recr
uite
d fro
m V
A.
Long
itudi
nal.
Char
t rev
iew
com
pare
d co
nsis
tent
repo
rting
of S
MBG
vs
inco
nsis
tent
repo
rting
of S
MBG
vs
no
repo
rting
of S
MBG
.
Long
itudi
nal.
Revi
ewed
HM
O
data
base
for a
dher
ence
to g
ener
al S
MBG
reco
mm
enda
tions
.
Long
itudi
nal.
Revi
ewed
cha
rts
at V
A m
edic
al c
ente
r for
patie
nts
with
type
2 d
iabe
tes
who
rece
ived
blo
od o
r urin
e
mon
itorin
g su
pplie
s.
Long
itudi
nal.
Char
t rev
iew
of
patie
nts
who
fille
d sc
ript f
or
mon
itorin
g st
rips.
Initi
ated
a
VA p
olic
y ch
ange
that
redu
ced
the
num
ber o
f
disp
ense
d st
rips
for p
atie
nts
with
type
2 d
iabe
tes
not o
n
insu
lin to
50
per 9
0 da
ys.
Seve
nty
perc
ent o
f pat
ient
s w
ith
cons
iste
nt re
porti
ng o
f SM
BG
had
95%
of r
epor
ted
HbA1
c
belo
w 8
% v
s 18
% o
f pat
ient
s
with
inco
nsis
tent
repo
rting
of
SMBG
vs
22%
of p
atie
nts
with
no
repo
rting
of S
MBG
.
Follo
win
g AD
A
reco
mm
enda
tions
for S
MBG
,
base
d on
pat
ient
dia
bete
s
type
and
med
icat
ion,
was
asso
ciat
ed w
ith lo
wer
HbA
1c.
Ther
e w
ere
no s
igni
fican
t
diffe
renc
es b
etw
een
SMBG
and
urin
e m
onito
ring.
SMBG
was
ass
ocia
ted
with
low
er H
bA1c
.Cha
nges
in
frequ
ency
of S
MBG
had
no
effe
ct o
n Hb
A1c.
NR Grea
ter f
requ
ency
of S
MBG
asso
ciat
ed w
ith lo
wer
HbA
1c.
HbA1
c di
d no
t diff
er b
ased
on
leng
th o
f tim
e m
onito
red
or
num
ber o
f stri
ps d
ispe
nsed
.
Seve
n pa
tient
s re
porte
d
mak
ing
insu
lin c
hang
es in
resp
onse
to m
onito
ring;
this
was
not
ass
ocia
ted
with
HbA1
c.
NR
Tab
le 1
(c
on
tinu
ed
)
Stud
ySa
mpl
eDe
sign
Resu
lts-H
bA1c
Mod
erat
ors
and
Med
iato
rs
TDE309807.qxd 11/7/2007 11:17 AM Page 996

Patient Blood Glucose Monitoring
997
McAndrew et al
New
man
et a
l
(199
0)31
Rind
one
et a
l
(199
7)28
Soum
erai
et a
l
(200
4)36
Wen
et a
l
(200
4)30
Wie
land
et a
l
(199
7)29
N =
38,
type
s 1
& 2,
no
med
icat
ion
limits
,mal
e =
NR,e
thni
city
= N
R,m
ean
age
= 6
0,re
crui
ted
from
VA.
N =
115
,typ
e 2,
on o
ral
med
icat
ions
onl
y,m
ale
= N
R,
ethn
icity
= N
R,m
ean
age
= 6
8,pa
tient
s re
crui
ted
from
VA.
N =
321
9,on
insu
lin o
r ora
l
diab
etes
med
icat
ion,
type
1
or 2
,mea
n ag
e =
54,
mal
e =
54%
,eth
nici
ty:C
=
46%
,AA
= 1
9%,O
= 3
%,
M =
32%
.
N =
976
,mal
e =
97%
,
pres
crib
ed o
ral m
edic
atio
n,
mea
n ag
e =
63,
ethn
icity
:
AA =
8%
,C =
38%
,H=
48%
,
O =
6%
,rec
ruite
d fro
m V
A.
N =
216
,typ
e 2,
pres
crib
ed
glyb
urid
e,m
ale
= 1
00%
,
ethn
icity
= N
R,m
ean
age
=
NR (a
ge ra
nge,
39-8
9),
recr
uite
d fro
m V
A.
Long
itudi
nal.
Rand
omly
revi
ewed
cha
rts fr
om p
atie
nts
who
mon
itore
d an
d pa
tient
s
who
did
not
(3 p
atie
nts
who
mon
itore
d ur
ine
wer
e
cons
ider
ed n
onm
onito
rs).
All p
atie
nts
had
2 Hb
A1c
reco
rded
a y
ear f
or 3
yea
rs.
Long
itudi
nal.
Com
pare
d pa
tient
s
who
wer
e pr
escr
ibed
mon
itorin
g st
rips
to p
atie
nts
who
wer
e no
t.Da
ta w
ere
colle
cted
ove
r 2 y
ears
.If
mul
tiple
dat
a po
ints
wer
e
reco
rded
,mea
ns w
ere
used
.
Long
itudi
nal.
Inte
rrup
ted
time-
serie
s an
alys
is o
f a d
atab
ase
of a
n HM
O th
at b
egan
offe
ring
free
SMBG
mon
itors
to p
atie
nts
with
dia
bete
s.
Prev
ious
yea
r’s d
ata
wer
e
cont
rolle
d fo
r.
Long
itudi
nal.
Revi
ewed
3 y
ears
of m
edic
al c
harts
for p
atie
nts
pres
crib
ed o
ral m
edic
atio
n fo
r
diab
etes
.Com
pare
d Hb
A1c
of
patie
nts
who
did
not
SM
BG v
s
SMBG
yea
r 3 v
s SM
BG y
ears
2-3
vs S
MBG
yea
rs 1
-3.
Long
itudi
nal.
SMBG
was
oper
atio
naliz
ed a
s re
fill o
f
SMBG
stri
ps.C
ompa
red
HbA1
c
of p
atie
nts
who
did
not
mon
itor,
SMBG
onc
e a
day,
and
SMBG
2 o
r mor
e tim
es a
day
.
SMBG
was
not
ass
ocia
ted
with
HbA1
c.
Rece
ivin
g a
scrip
t for
SM
BG
strip
s w
as n
ot a
ssoc
iate
d
with
HbA
1c.
Star
ting
SMBG
was
not
asso
ciat
ed w
ith im
prov
ed
HbA1
c fo
r pat
ient
s w
ith
“goo
d or
ade
quat
e co
ntro
l”
but w
as a
ssoc
iate
d w
ith
impr
oved
HbA
1c a
mon
g
thos
e w
ith p
oor c
ontro
l.
SMBG
was
not
ass
ocia
ted
with
HbA1
c.
Freq
uenc
y of
SM
BG w
as n
ot
asso
ciat
ed w
ith H
bA1c
.
NR Rece
ivin
g m
ore
bottl
es o
f SM
BG
strip
s w
as n
ot a
ssoc
iate
d
with
HbA
1c.
Effe
ct o
f SM
BG w
as m
oder
ated
by in
itial
HbA
1c a
nd
pote
ntia
lly m
edia
ted
by
med
icat
ion
adhe
renc
e.
NR NR
(con
tinue
d)
TDE309807.qxd 11/7/2007 11:17 AM Page 997

The Diabetes EDUCATOR
998
Volume 33, Number 6, November/December 2007
Alle
n et
al
(199
0)46
Davi
dson
et a
l
(200
5)43
Guer
ci e
t al
(200
3)37
N =
54,
type
2,n
o in
sulin
,
mal
e =
100
%,e
thni
city
:
C =
63%
,mea
n ag
e =
58,
recr
uite
d fro
m V
A.
N =
88,
type
2,n
o in
sulin
,
mea
n ag
e =
50,
ethn
icity
:AA
= 2
2%,H
= 7
5%,O
= 3
%.
N =
689
,typ
e 2,
oral
med
icat
ion
only,
mal
es =
55%
,eth
nici
ty =
NR,
mea
n
age
= 6
2,st
udy
com
plet
ed in
Fran
ce.
RCT.
Com
pare
d ur
ine
mon
itorin
g to
SM
BG.
SMBG
:SM
BG 3
6/m
onth
.
Urin
e:M
onito
red
urin
e
36/m
onth
.
Both
:Rec
eive
d di
et
coun
selin
g an
d m
onth
ly v
isits
with
trea
tmen
t tea
m,w
hich
used
trea
tmen
t alg
orith
m
(incl
udin
g m
edic
atio
n
chan
ges)
in re
spon
se to
mon
itorin
g.
RCT SM
BG =
inst
ruct
ed to
mon
itor B
G be
fore
and
1/2
hour
s af
ter m
eals
6 ti
mes
a
wee
k.
C =
not
inst
ruct
ed to
SM
BG.
Both
= m
eet w
ith d
ietit
ian
5
times
; nur
ses
blin
ded
to
treat
men
t use
d a
treat
men
t
algo
rithm
that
incl
uded
med
icat
ion
chan
ges.
RCT SM
BG =
SM
BG tr
aine
d by
GP; p
atie
nts
inst
ruct
ed to
mon
itor 6
/wee
k.
Both
= F
ollo
wed
eve
ry 6
wee
ks fo
r 24
wee
ks,g
iven
gene
ral d
ieta
ry a
nd d
iabe
tes
reco
mm
enda
tions
,HbA
1c
SMBG
:Bas
elin
e =
12.
4%,6
mon
ths
= 1
0.4%
(P <
.001
).
Urin
e:ba
selin
e =
11.
7%,6
mon
ths
= 9
.7%
(P <
.001
).
No s
igni
fican
t bet
wee
n-gr
oup
diffe
renc
es.
SMBG
= a
sig
nific
ant
redu
ctio
n of
0.8
% in
HbA
1c.
C =
a s
igni
fican
t red
uctio
n
of 0
.6%
.
No s
igni
fican
t bet
wee
n-gr
oup
diffe
renc
es.
SMBG
= a
sig
nific
ant
redu
ctio
n of
0.8
8% in
HbA
1c.
Cont
rol =
a s
igni
fican
t
redu
ctio
n of
0.6
0%.
SMBG
sho
wed
a s
tatis
tical
ly
sign
ifica
nt im
prov
emen
t as
com
pare
d to
con
trol.
Tren
d to
war
d yo
unge
r and
bette
r edu
cate
d im
prov
ing
mor
e.Ba
selin
e Hb
A1c,
base
line
wei
ght,
base
line
fast
ing
plas
ma
gluc
ose,
use
of o
ral m
edic
atio
ns,d
urat
ion
of d
iabe
tes,
and
race
did
not
pred
ict i
mpr
oved
glu
cose
cont
rol.
NR Patie
nts
who
did
SM
BG w
ere
mor
e lik
ely
to re
port
follo
win
g di
etar
y ad
vice
.
Pred
icto
rs o
f im
prov
emen
t
incl
uded
SM
BG g
roup
,hig
her
initi
al H
bA1c
,low
er d
urat
ion
of d
iabe
tes,
and
low
er b
ody
mas
s in
dex.
Tab
le 1
(c
on
tinu
ed
)
Stud
ySa
mpl
eDe
sign
Resu
lts-H
bA1c
Mod
erat
ors
and
Med
iato
rs
TDE309807.qxd 11/7/2007 11:17 AM Page 998

Patient Blood Glucose Monitoring
999
McAndrew et al
Kibr
iya
et a
l
(199
9)38
Kwon
et a
l
(200
4)39
N =
64,
type
2,o
n or
al
med
icat
ion
or in
sulin
,mal
e =
55%
,mea
n ag
e =
50,
ethn
icity
= N
R,st
udy
com
plet
ed in
Ban
glad
esh.
N =
110
,typ
e 2,
no m
edic
atio
n
limits
repo
rted,
mal
e =
61%
,
ethn
icity
= N
R,m
ean
age
=
54,s
tudy
com
plet
ed in
Kore
a.
take
n ev
ery
3 m
onth
s,an
d
GP a
llow
ed to
cha
nge
treat
men
t bas
ed o
n Hb
A1c
at
3-m
onth
vis
it.
RCT SM
BG =
2-d
ay c
lass
on
SMBG
,ins
truct
ed to
mon
itor
fast
ing
and
2 ho
urs
afte
r
brea
kfas
t and
/or 2
hou
rs
afte
r lun
ch a
nd to
adj
ust
med
icat
ions
.Tau
ght t
o m
ake
treat
men
t cha
nges
in
resp
onse
to S
MBG
.Vis
ited
doct
or e
very
3 m
onth
s.
Cont
rol =
Mon
thly
vis
its;
doct
or c
ould
mak
e m
ed
chan
ges.
Both
:Rec
eive
d ed
ucat
ion.
RCT In
tern
et S
MBG
= 1
2-w
eek
Inte
rnet
reco
rdin
g of
SM
BG;
patie
nt re
ceiv
ed
reco
mm
enda
tions
via
the
Inte
rnet
,inc
ludi
ng s
ome
med
icat
ion
chan
ges,
no
outp
atie
nt v
isit,
SMBG
pre
-
and
post
mea
ls.
Cont
rol =
regu
lar m
onth
ly
outp
atie
nt v
isits
.
Both
= re
com
men
ded
to
SMBG
3 o
r mor
e da
ys p
er
wee
k 1
to 3
tim
es a
day
,
incl
udin
g af
ter m
eals
.
SMBG
= H
bA1c
dec
reas
ed
1.37
% (P
= .0
22).
Cont
rol =
HbA
1c d
ecre
ased
0.38
% (P
= .2
9).
Did
not r
epor
t if t
here
was
a
stat
istic
ally
sig
nific
ant
diffe
renc
e be
twee
n th
e
2 gr
oups
.
Inte
rnet
SM
BG =
HbA
1c
redu
ced
0.54
% (P
< .0
01).
Cont
rol =
HbA
1c in
crea
sed
0.33
% (N
S).
Ther
e w
as a
sta
tistic
ally
sign
ifica
nt d
iffer
ence
in th
e
2 gr
oups
.
NR The
diffe
renc
es b
etw
een
the
2 gr
oups
wer
e m
ore
pron
ounc
ed a
mon
g pa
tient
s
with
an
initi
al H
bA1c
of 7
or
high
er.
(con
tinue
d)
TDE309807.qxd 11/7/2007 11:17 AM Page 999

The Diabetes EDUCATOR
1000
Volume 33, Number 6, November/December 2007
Mile
s et
al
(199
7)47
Mor
elan
d et
al
(200
6)45
Muc
hmor
e et
al
(199
4)44
N =
150
,typ
e 2,
no m
edic
atio
n
limits
repo
rted,
mal
e =
60%
,
mea
n ag
e =
65,
ethn
icity
=
NR,s
tudy
com
plet
ed in
Unite
d Ki
ngdo
m.
N =
199
,typ
es 1
& 2
,no
med
icat
ion
limits
,mal
e =
58%
,eth
nici
ty =
NR,
mea
n
age
= 4
9.
N =
23,
type
2,n
o in
sulin
,
mal
e =
39%
,eth
nici
ty =
NR,
mea
n ag
e =
59,
all p
atie
nts
over
wei
ght.
RCT.
Patie
nts
aske
d to
eith
er
SMBG
or u
rine
mon
itor.
Both
= P
atie
nts
aske
d to
mon
itor e
ither
bef
ore,
2 ho
urs
afte
r mea
ls,o
r bed
time
once
daily
and
to a
ttend
4
educ
atio
n se
ssio
ns.A
t 3
mon
ths,
patie
nts
switc
hed
to
an a
ltern
ativ
e m
onito
ring
met
hod.
At 6
mon
ths,
patie
nts
wer
e ab
le to
cho
ose
pref
erre
d
met
hod
for m
onito
ring.
RCT Co
ntro
l = d
iabe
tes
educ
atio
n.
“MT”
(atte
ntio
nal c
ontro
l) =
mon
itorin
g ed
ucat
ion
sess
ion,
supp
ort f
rom
edu
cato
r.
“BGT
”(in
terv
entio
n) =
blo
od
gluc
ose
mon
itorin
g bo
okle
t,
mon
itorin
g ed
ucat
ion
sess
ion,
supp
ort f
rom
edu
cato
r.
RCT SM
BG =
edu
catio
n on
car
b
coun
ting
and
SMBG
,give
n
mon
itor a
nd s
trips
to m
onito
r 6
times
a d
ay (b
efor
e an
d 2
hour
s af
ter m
eals)
for 4
wee
ks,
then
redu
ced
to tw
ice
a da
y fo
r
4 m
onth
s,re
sults
cha
rted.
HbA1
c si
gnifi
cant
ly d
eclin
ed in
both
gro
ups
at 1
2 m
onth
s
(10.
3% to
7.5
% in
bot
h
grou
ps).
Ther
e w
ere
no
betw
een-
grou
p di
ffere
nces
.
No s
igni
fican
ce,i
mpr
ovem
ent i
n
HbA1
c in
any
gro
up.W
hen
indi
vidu
als
who
impr
oved
wer
e co
mpa
red
to in
divi
dual
s
who
did
not
impr
ove,
a
grea
ter p
erce
ntag
e of
impr
over
s w
ere
in th
e “B
GT”
grou
p.
SMBG
= H
bA1c
redu
ced
1.54
% (P
< .0
5).
Cont
rol =
HbA
1c re
duce
d
0.84
% (P
> .3
).
No s
igni
fican
t diff
eren
ces
betw
een
grou
ps a
t stu
dy e
nd.
NR NR Dura
tion
of d
iabe
tes,
initi
al
HbA1
c,an
d nu
mbe
r of S
MBG
wer
e no
t rel
ated
to H
bA1c
.
Tab
le 1
(c
on
tinu
ed
)
Stud
ySa
mpl
eDe
sign
Resu
lts-H
bA1c
Mod
erat
ors
and
Med
iato
rs
TDE309807.qxd 11/7/2007 11:17 AM Page 1000

Patient Blood Glucose Monitoring
1001
McAndrew et al
Rutte
n et
al
(199
0)44
Schw
edes
et a
l
(200
2)41
N =
149
,typ
e 2,
no in
sulin
,
mal
e =
35%
,eth
nici
ty =
NR,
mea
n ag
e =
63.
N =
223
,typ
e 2,
no in
sulin
,
mal
e =
52%
,eth
nici
ty =
NR,
mea
n ag
e =
60.
Cont
rol =
gen
eral
dia
bete
s
educ
atio
n.
Both
= 2
8-w
eek
beha
vior
al
wei
ght c
ontro
l pro
gram
,
follo
wed
by
GP w
ho c
ould
mak
e m
edic
atio
n ch
ange
s.
RCT.
Eigh
t pra
ctic
es m
atch
ed
and
rand
omiz
ed.
Inte
rven
tion
= 3
3 pa
tient
s
rece
ived
2 to
5 e
duca
tion
sess
ions
on
SMBG
,and
patie
nts
cont
acte
d di
abet
es
nurs
e m
onth
ly to
repo
rt
fast
ing
bloo
d gl
ucos
e.If
BG
high
,mad
e ap
poin
tmen
t and
also
met
with
GP
afte
r 6
mon
ths.
Thirt
y-th
ree
patie
nts
did
not S
MBG
and
met
with
GP a
t lea
st 4
tim
es a
yea
r.Al
l
used
med
icat
ion
algo
rithm
to
treat
pat
ient
s.
Cont
rol =
pat
ient
s no
t
inst
ruct
ed in
SM
BG,d
id n
ot
use
fixed
app
oint
men
ts.
RCT SM
BG =
SM
BG b
efor
e an
d 1
hour
afte
r 3 m
eals
,tw
ice
a
wee
k,an
d re
cord
the
mon
itorin
g; p
atie
nts
wer
e
seen
eve
ry 4
wee
ks b
y a
nurs
e w
ho u
sed
a SM
BG
coun
selin
g al
gorit
hm.
Cont
rol =
non
stan
dard
ized
coun
selin
g ev
ery
4 w
eeks
.
Inte
rven
tion
= m
ean
grou
p
HbA1
c de
crea
sed
0.5%
(P <
.05)
.
Cont
rol =
mea
n gr
oup
HbA1
c
incr
ease
d in
0.5
% (P
< .0
01).
SMBG
= re
duct
ion
of 1
%.
Cont
rol =
redu
ctio
n of
0.5
4%.
Ther
e w
as a
sta
tistic
ally
sign
ifica
nt d
iffer
ence
bet
wee
n
the
grou
ps.
Patie
nts
with
initi
al H
bA1c
>10
in th
e in
terv
entio
n co
nditi
on
wer
e m
ore
likel
y to
impr
ove
than
thos
e w
ith in
itial
HbA
1c
>1
in th
e co
ntro
l con
ditio
n.
In th
e SM
BG g
roup
,not
mak
ing
beha
vior
al c
hang
es in
resp
onse
to S
MBG
led
to
failu
re.
Long
er d
iabe
tes
dura
tion
and
high
er b
asel
ine
HbA1
c
pred
icte
d a
dela
y in
resp
onse
.
(con
tinue
d)
TDE309807.qxd 11/7/2007 11:17 AM Page 1001

The Diabetes EDUCATOR
1002
Volume 33, Number 6, November/December 2007
Seat
on (1
996)
42N
= 1
0,ty
pe 2
,onl
y on
ora
l
med
icat
ions
,mea
n
age
= N
R,m
ale
= N
R,
ethn
icity
= N
R.
RCT.
Repo
rted
in a
bstra
ct.
Both
= s
tand
ardi
zed
treat
men
t alg
orith
m.
SMBG
= S
MBG
.
Cont
rol =
no
SMBG
.
SMBG
= s
tatis
tical
ly
sign
ifica
nt re
duct
ion
of 0
.8%
in H
bA1c
.
Cont
rol =
no
chan
ge.
Did
not r
epor
t if t
here
was
a
stat
istic
ally
signi
fican
t
diffe
renc
e be
twee
n th
e 2
grou
ps.
NR
Tab
le 1
(c
on
tinu
ed
)
Stud
ySa
mpl
eDe
sign
Resu
lts-H
bA1c
Mod
erat
ors
and
Med
iato
rs
RCT,
rand
omiz
ed c
ontro
l tria
l; SM
BG,s
elf-
mon
itorin
g of
blo
od g
luco
se; N
R,no
t rep
orte
d; G
P,ge
nera
l pra
ctiti
oner
; AA,
Afric
an A
mer
ican
; H,H
ispa
nic;
C,C
auca
sian
; O,o
ther
; A/P
I,As
ian/
Paci
fic Is
land
er; N
A,Na
tive
Amer
ican
; M,m
ixed
race
or e
thni
city
; ADA
,Am
eric
an D
iabe
tes
Asso
ciat
ion;
HM
O,he
alth
mai
nten
ance
org
aniz
atio
n; V
A,Ve
tera
ns A
dmin
istra
tion;
BG,
bloo
d gl
ucos
e; N
HANE
S III
,Thi
rd N
atio
nal H
ealth
and
Nut
ritio
nEx
amin
atio
n Su
rvey
.
TDE309807.qxd 11/7/2007 11:17 AM Page 1002

Results
Trial Flow and Study Characteristics
Twenty-nine studies met criteria for review: 9 cross-sectional studies, 9 longitudinal studies, and 11 RCTs(see Figure 1 for trial flow). Study details are shown inTable 1.
Data Synthesis
Data are presented by the 3 types of study design:cross-sectional, longitudinal, and RCT. Each section firstdescribes the results of SMBG on HbA1c, reports nexton study limitations, and then describes factors thatmediate or moderate the relationship between SMBGand HbA1c levels.
Cross-sectional studies. Results of the 9 cross-sectional studies were inconclusive. Two showed thatmonitoring of glucose was correlated with lower HbA1clevels,19,20 and 3 found that glucose monitoring correlatedwith higher HbA1c levels.21-23 Among the latter 3 studies,
that by Franciosi and colleagues21 found monitoringassociated with worse control only for patients not oninsulin; there was no association of SMBG with HbA1cfor patients on insulin. The remaining 4 studies reportedno significant association between self-monitoring andHbA1c24-27; 1 of the 4 compared “home glucose monitor-ing” of urine (74 patients) and blood glucose (19patients) to patients not monitoring (103) and found nosignificant differences in HbA1c among the groups.27
As monitoring and glucose control are assessed at thesame time point in cross-sectional studies, it is impossibleto tell whether monitoring affected glucose control or, con-versely, whether patients in poor control were motivated tomonitor. As it is unlikely that monitoring would worsencontrol, it seems likely that the 3 studies reporting a nega-tive relationship of monitoring to HbA1c reflect high levelsof self-monitoring among patients with elevated HbA1c.This interpretation is consistent with Harris’s23 finding thatpatients with higher levels of HbA1c were both more likelyto monitor and more likely to be on insulin.
With respect to mediators and moderators ofSMBG, only 3 cross-sectional studies assessed if and how
Patient Blood Glucose Monitoring
1003
McAndrew et al
Articles retrieved for detail appraisal (N=89)
Articles included within the review (N=29)
Articles excluded (N=60)Intervention too comprehensive (N=8). Did not examine the association of HbA1c and SMBG (N=26)
Only included pt on insulin
Articles screened for inclusion from databases and references of relevant
Articles eliminated because were not relevant to current review or duplicates
Figure 1. Trial flow diagram.
TDE309807.qxd 11/7/2007 11:17 AM Page 1003

monitoring affected patient behavior. For example,Franciosi and colleagues21 reported better control amongpatients prescribed insulin who self-administered inresponse to SMBG readings in comparison to patientswho did not use insulin in response to these readings.Self-management procedures were not assessed for non-insulin users. In a study by Patrick and colleagues,27 only38% (37 of 97) of patients with type 2 diabetes not treatedwith insulin reported they would change a treatment inresponse to self-monitoring feedback. Glucose control forthese patients was not significantly better than that of the62% of patients who did not report making changes; how-ever, it is unclear how often these patients actuallychanged their management practices in response to mon-itoring information. Finally, Jaworska and colleagues26
found that patients who reported being able to makeinsulin changes in response to readings did not have lowerHbA1c levels. In summary, the cross-sectional studies areinconclusive as to the result of the effect of SMBG on glu-cose control. Most important, the directionality of any ofthe reported effects is indeterminate.
Longitudinal studies. Nine studies examined the effectof SMBG on HbA1c using longitudinal data. Four28-31 ofthe 9 found no association of SMBG with HbA1c. Twoother studies found lower HbA1c levels among patientswho did SMBG in comparison to those who did not mon-itor32 and to those who did not monitor at a recommendedfrequency.33 A brief commentary in a seventh studystated that patients whose medical charts documentedthat they were doing SMBG were significantly morelikely to have HbA1c levels below 8%.34 An eighth studyby Klein and colleagues35 compared those who moni-tored urine to those who did SMBG. There was no con-trol group that did not monitor, and there was nodifference in HbA1c between the 2 groups that did.
The ninth study by Soumerai and colleagues36 exam-ined the effects of providing free monitors to patients ina New England health maintenance organization (onlymonitoring strips had been previously provided).Monitoring behavior, defined as test strip distribution,was examined for 19 months prior to the policy change,5 months during the transition, and 17 months after thepolicy change. An interrupted time-series analysis oftrend line for monitoring behavior, pre- and postintro-duction of free monitors, showed an increase in the initi-ation of SMBG and in the use of test strips amongpatients with type 2 diabetes on oral medication. Patients
who previously had been inconsistent in refilling theiroral medication and now increased their use of test stripsalso increased medication adherence, and patients whowere previously in poor control and began monitoringshowed a reduction in HbA1c levels. The analyses bySoumerai and colleagues36 suggest that the initial level ofHbA1c may moderate one’s ability to detect the efficacyof monitoring and that the effects of monitoring onHbA1c may be mediated by increases in medicationadherence.
The Methods sections of these studies point to limita-tions in the implementation and assessment of mediatorsand moderators similar to those found in the cross-sectional studies. It is unclear if patients were instructedto monitor because they were in poor control or if self-monitoring did not lead to control. It was also unclearwhether the intervention addressed the components ofself-regulation essential for mediating the benefits ofmonitoring. The specific instructions patients were givenabout the procedure and the validity of self-monitoring(ie, when to monitor and what to do in response to read-ings) were rarely described, and most studies did notassess these mediators. One study31 reported that whenclinicians became aware “that SMBG level may be unre-liable, these levels were rarely used alone as criteria forinsulin change or life-style adjustment suggestions.” Ifthis was explicitly or implicitly communicated topatients, it would likely undermine motivation to self-monitor and the use of SMBG to guide behavior.
Five of the 9 studies reported mixed results on the rela-tionship between frequency of monitoring and HbA1clevels. Karter and colleagues33 found that more frequentmonitoring was correlated with better control amongpatients with type 2 diabetes. Although Meier and col-leagues32 found that SMBG was associated with bettercontrol, they also found no change in glucose controlfrom a policy change that reduced the availability of teststrips and lowered the average frequency of monitoringfrom 1.37 to 0.74 times a day had. Finally, 3 of the 9 thatassessed frequency of monitoring28,29,35 found no evidenceof a relationship of frequency of SMBG to HbA1c, and 2reported no relationship between length of time monitor-ing and HbA1c levels.30,35 In summary, the evidence issuggestive at best that monitoring might help patients bet-ter manage blood glucose levels and lower HbA1c levels.
Randomized control trials. Eleven RCTs tested theeffects of monitoring on HbA1c levels. Six of the 11 trials
The Diabetes EDUCATOR
1004
Volume 33, Number 6, November/December 2007
TDE309807.qxd 11/7/2007 11:17 AM Page 1004

comparing monitoring to a control condition reportedimproved glucose control in the monitoring condition.37-42
One38 of the 6 reported a significant decrease of HbA1c(1.37%) in the intervention arm and a nonsignificantreduction (0.38%) in the control arm but did not, how-ever, report whether the magnitude of HbA1c reductionin the monitoring arm was statistically superior to that inthe control.
Two of the 5 remaining trials failed to detect an advan-tage of a monitoring intervention on glucose control.That by Davidson and colleagues43 reported a reductionof HbA1c in the monitoring condition (0.8%) not signif-icantly different from the control (0.6%), and Muchmoreand colleagues44 reported that the comparison betweenthe 12 patients in the monitoring group (HbA1c loweredby 1.54%) was not significantly greater than that for the11 patients in the control condition (HbA1c reduced0.84%); the study was likely underpowered. The third ofthe 5 studies by Moreland and colleagues45 used a 3-armdesign that compared an intervention, which combinedmonitoring with a booklet designed to help patients formmore reasonable “expectations and responses” to moni-toring, to monitoring alone and a control arm. Althoughthere were no significant differences in the magnitude ofthe change in HbA1c across the 3 conditions, Morelandand colleagues45 found that the number of patients whoshowed an improvement in HbA1c was significantlygreater in the monitoring intervention with a booklet.
The final 246,47 of the 5 nonsignificant RCTs are lessrelevant to the main objective of this review (ie, doespatient monitoring lead to improvements in HbA1c?) asthey compared SMBG to urine monitoring and did notuse a nonmonitoring control. Both studies46,47 reportedsignificant reductions in HbA1c in both trial arms and nodifferences in HbA1c between patients who monitoredurine levels and those monitoring blood glucose.
A number of methodological factors complicate theinterpretation of the results of these trials. In 3 tri-als,39,41,42 patients in the monitoring arm received addi-tional resources (ie, education, medication, or support)not given control patients. Additions that told patientshow to respond to high or low SMBG readings woulddefine a key mediator for the formation of a coherentself-regulatory system. Additions that facilitated reduc-tions in HbA1c but were unrelated to the behavioralmonitoring system (eg, additional social support) wouldbe defined as independent influences or trial confounds.Studies also combined data from patients with type 1 and
type 2 diabetes, as well as data from patients on insulin,with patients controlled by oral medication or dietalone.38,39 Perhaps less problematic, patients were ran-domized by group rather than by person, and newpatients were added to replace dropouts.38,44,46 Davidsonand colleagues43 conducted the only trial that blinded cli-nicians to the patients’ treatment group. Finally, the trialby Seaton42 should be given little weight as only 10patients were randomized, the author did not report if thebetween-group difference was statistically significant,and the results were reported only in an abstract.42
In examining potential moderators of response, 3studies37,39,40 found that patients in poor control weremore likely to benefit from SMBG. This supports theprior suggestion36 that the initial level of glucose controlwill moderate the effects of SMBG on HbA1c. Guerciand colleagues37 found that lower duration of diabetespredicted improved HbA1c, whereas Schwedes and col-leagues41 found that longer duration of diabetes may leadto a delayed response. Muchmore and colleagues44 andAllen and colleagues,46 however, did not find that eitherinitial HbA1c or duration of illness was related to theeffect of SMBG on HbA1c. Finally, Allen and colleaguesreported a trend for greater improvement in HbA1c fromSMBG among younger and more educated patients.
The RCTs differed on the instruction given to patientsconcerning monitoring. Supplemental findings from 2studies37,41 are consistent with the view that SMBG shouldbe viewed as a component of a larger behavioral system.Schwedes and colleagues41 instructed patients to monitor12 times a week before and after meals and to changetheir regulatory behaviors (diet, exercise, medication) inresponse to their SMBG readings; patients who changedbehaviors in response to SMBG readings had signifi-cantly lower HbA1c levels than those who did not.Although Guerci and colleagues37 did not give explicitinstruction to patients concerning changing behaviors inresponse to monitoring, they reported that patients whomonitored were more likely to follow dietary recommen-dations and had better controlled HbA1c.
Discussion
Effect of SMBG on HbA1c
Neither the cross-sectional nor longitudinal studiessupport the hypothesis that SMBG can be effective forimproving the control of blood glucose levels among
Patient Blood Glucose Monitoring
1005
McAndrew et al
TDE309807.qxd 11/7/2007 11:17 AM Page 1005

patients with type 2 diabetes not using insulin. Six stud-ies found that monitoring was related to lower levels ofHbA1c (2 cross-sectional19,20 and 4 longitudinal33-36), 8found no association between monitoring and HbA1c(4 cross-sectional24-27 and 4 longitudinal28-31), and 3 cross-sectional studies21-23 reported that SMBG was associatedwith worse control. Regardless of their findings, thecross-sectional studies are basically uninterpretable asone cannot conclude that SMBG preceded or was acci-dentally correlated with good control, or was initiated bypatients who were in poor control. The longitudinal stud-ies fail to clarify the picture as they are evenly dividedbetween positive effects and null effects.
A more favorable image of SMGB for controllingblood glucose levels emerges from the results of theRCTs and Soumerai and colleagues’36 well-designedinterrupted time-series analyses. Of the 9 RCTs37-45 thatcompared a monitoring intervention to a control, 637-42
reported lower levels of HbA1c for patients in the moni-toring condition. In no trial did the monitoring conditionlead to worsening of HbA1c, although for 343-45 of the 9,improvements in the monitoring condition were not sta-tistically greater than the control condition. Soumeraiand colleagues’36 time-series analysis finding of lowerHbA1c levels following the initiation of monitoring thanduring the nonmonitoring time period is consistent withthe results of the RCTs.
This study’s positive view of the benefit of SMBG incontrolling HbA1c for patients with type 2 diabetes isconsistent with previous reviews by Welschen and col-leagues in Diabetes Care6 and the Cochrane Database.10
Sarol and colleagues11 also concluded that SMBGimproved glucose control for patients with type 2 dia-betes. All 3 reviews examined only RCTs whose partici-pants were not on insulin. Less favorable judgments wereoffered by Coster and colleagues9 and Faas and col-leagues,8 both of whom stated that the evidence is insuf-ficient to support the hypothesis that self-monitoring iseffective in improving glycemic control, although bothcalled for further studies. Coster and colleagues9 andFaas and colleagues8 also included a study in which someparticipants were on insulin.
This study broadened the criteria for inclusion andreviewed cross-sectional studies, longitudinal studies,and RCTs using a variety of treatment strategies, includ-ing studies with some patients on insulin, to obtain asmuch evidence as possible respecting the effects ofSMBG on HbA1c and the moderators and mediators of
treatment outcomes.48-50 This study balanced the broaderinclusiveness in the type of studies reviewed by narrow-ing the focus to studies of patients with type 2 diabetes,some of whom were not on insulin and others who were.By excluding studies of patients with type 1 diabetes andstudies that only included patients on insulin, this studyavoided duplicating prior recommendations that have ledto acceptance of SMBG for patients using multipleinsulin injections a day (ADA level of evidence = A).7
This allowed the authors to conduct a thorough review ofstudies for which the ADA recommendations have theleast evidence (ADA level of evidence = E).7 It is impor-tant to note, however, that the favorable evidence forSMBG for patients using insulin is consistent with thisstudy’s theoretical model. Insulin is relatively fast acting,and SMBG provides a direct indication of its effects. Thecombination of insulin and SMBG provides patients withclear evidence of the utility of the combination for con-trolling blood sugar levels and facilitates the acquisitionof the volitional patient-centered feedback loop essentialfor effective self-management.
Mediators and Moderators
The optimistic message that monitoring can be aneffective tool in patient-centered care for patients withtype 2 diabetes (ie, for self-regulation of blood glucoseand lower levels of HbA1c over time) assumes thatSMBG is embedded in a multicomponent system foreffective, volitional control. This study suggests thatconscious or voluntary management requires the imple-mentation of a complete control system in which thepatient must (1) know how to take a reading; (2) under-stand when the reading is above (or below) target values;(3) see the connection between deviant readings andprior behavior (eating, exercise, and under- or overuse ofmedication); (4) have and implement an action plan tocontrol glucose levels; (5) rely more heavily on SMBGreadings and give less weight to subjective feelings ofwell-being and possibly false signs of hyperglycemicdistress (eg, feeling dizzy or shaky); (6) create simpleaction plans that will allow the patient to integrate theminto his or her ongoing life patterns, the use of SMBG,and the behaviors needed for effective blood glucosemanagement; and (7) evaluate glucose readings in anonjudgmental framework. Meeting blood glucose tar-gets needs to be viewed as an ongoing problem-solvingprocess and target misses as problems with the intensity
The Diabetes EDUCATOR
1006
Volume 33, Number 6, November/December 2007
TDE309807.qxd 11/7/2007 11:17 AM Page 1006

or timing of specific control behaviors and not as fail-ures of the self.
Of these 6 hypotheses, only 1 hypothesis was examinedby the studies reviewed. The RCT conducted by Schwedesand colleagues41 found that patients who changed self-management behaviors in response to SMBG showedimprovement in HbA1c, and this finding is consistent withthis study’s hypothesis that SMBG is effective when it isused by the patient to make treatment adjustments.Similarly, Guerci and colleagues37 found that patients whomonitored were more likely to follow dietary advice andhad better glucose control. Of the 3 cross-sectional stud-ies21,26,27 and 1 longitudinal study35 that examined theimpact of treatment adjustment in response to SMBG onHbA1c, only 1 found that patients who made treatmentchanges in response to SMBG were in better control.21 Thequality of these studies, however, prevents interpretation(all used self-report, 2 studies asked only about the abil-ity26 or if the patient “would ever”27 adjust therapy, and in1 study, only 7 patients reported making changes35).Although this study had no specific hypotheses regardingmoderators, evidence from the review of RCTs suggestedthat greater initial HbA1c37,39,40 and shorter duration ofdiabetes37,41 may be associated with improved responseand lower HbA1c. Other RCTs, however, found no asso-ciation of initial HbA1c44,46 or duration of diabetes44,46 withimproved response.
This study’s finding of an inadequate assessment ofmoderators and mediators by the studies reviewed mayreflect a particular bias in the way medical investigatorsview the RCTs. Randomized controlled trials testingSMBG and lifestyle changes are not experiments inwhich the independent variable is a single factor, as seenin classical behavioral studies of perception and learning.The RCT for glucose monitoring implements a multi-component system; SMBG is not equivalent to a medicalRCT comparing an active pill to a placebo (with biasessuch as differences in adherence, etc, removed).Interventions that introduce monitoring without creatingthe perceived linkages between specific behaviors andmeaningful and valid blood glucose readings do littlemore than provide the patient a number, which may bediffer from target but be of little utility for control. Thecall for the assessment of moderators and mediators isnot new: it has been advocated by clinical trial investiga-tors.51 Assessment of the specific components of an inter-vention allows statistical analyses to identify those thatare active.52
Implications
This systematic review suggests that SMBG may leadto improvements in HbA1c for patients with type 2 dia-betes not on insulin. Few studies, however, implementedand/or examined the components of the behavioral mon-itoring system that self-regulation and behavior theorywould suggest as critical for patients to manage diabeteson their own. Thus, this study found little data to supportor refute hypotheses regarding mediators. For example,the studies reviewed did not report on the specifics ofwhat patients were instructed to do in response to theirmonitoring results. Some instructed patients to use fixedtime monitoring schedules, which does little to helppatients see how self-management by medication, diet,and exercise relates to glucose levels. And in 1 instance,46
patients were instructed to monitor blood glucose levelsbefore meals. It is not clear that patients would learn howspecific meals affected blood glucose levels by premealand/or fasting blood glucose monitoring. When SMBG isembedded in a volitional control system, it providesfeedback as to how specific behaviors increase ordecrease blood glucose.
In addition to using monitoring within a system thatconnects behaviors to blood glucose levels, interventionsneed to ensure that the objective data provided by SMBGare used in place of the commonsense subjective cues thatare highly available and easy for patients to use to man-age diabetes. Patients and clinicians believe that fluctua-tions in blood glucose produce subjective changes.Seventy-seven percent of patients have answered yes tothe question “Can you tell, just by how you feel, whenyour glucose is too high?”53 The subjective cues that com-mon sense selects as indicators of blood glucose may beambiguous, confounded by affective experiences unre-lated to variation in blood glucose and therefore poorlycorrelated with actual blood glucose levels. Not surpris-ing, patients generally underestimate their blood glucoselevels.53 Moving patients from commonsense cues toobjective blood glucose monitoring may be an importantstep for improving monitoring interventions and is con-sistent with Peel and colleagues’54 conclusion from theirdetailed qualitative findings that SMBG helped patientsmake “their otherwise invisible and imperceptible illnessvisible.” None of the studies reviewed assessed or dis-cussed the transition from subjective cues and feelings toobjective monitoring as patients shaped their self-regulatorybehaviors to control blood glucose.
Patient Blood Glucose Monitoring
1007
McAndrew et al
TDE309807.qxd 11/7/2007 11:17 AM Page 1007

Finally, success in self-regulation requires thatpatients create and implement action plans that fit withintheir daily lives. Studies of patients with type 1 diabeteshave taught strategies and specific skills that allowpatients to adjust insulin in response to glucose levelsand diet and develop a high level of autonomy for effec-tive management that allows them the “life they wouldlive without diabetes.”55,56 There is no indication that theinterventions reviewed here considered the issuesinvolved in incorporating SMBG into the daily life ofpatients with type 2 diabetes. This is not a trivial issue astime for self-management has been reported to take anaverage of 2 hours a day.57 Measures of quality of lifeare a potential source of evidence for effective andautonomous self-management processes that fit within apatient’s life pattern; quality of life was assessed in only421,22,41,44 of the studies reviewed. Only 1 study foundthat SMBG was associated with higher depression,21
whereas the remaining 322,41,44 found that SMBG was notassociated with impaired quality of life. Of these, 1 RCTfound that SMBG led to improved quality of life forpatients in the monitoring arm. Both qualitative54 andquantitative58 research on quality of life and SMBG isconsistent with the assumption that quality of life will bepositively associated with SMBG when it is imple-mented effectively (ie, the patient views the informationnonjudgmentally and takes responsibility for his or hermanagement).
Given the scarcity of the empirical evidence, cautionis needed respecting the conclusions that have beendrawn about specific mediators and moderators of theeffectiveness of SMBG. Caution does not, however, pre-clude emphasizing the importance of a theoretical analy-sis of the behavioral processes that underlie a volitionalaction such as SMBG. Effective blood glucose controlthrough blood glucose monitoring, either in a RCT or inclinical practice, requires careful and thorough imple-mentation. Medication and lifestyle changes that areunused or used inappropriately will not improve thefunction of a complex, in vivo physiological system; thisis true for the control of blood glucose, blood pressure,and other biological markers for risk. Successful treat-ment, whether it be medication, diet, or exercise in com-bination with SMBG, requires that practitioners addressboth the physiological and the behavioral control sys-tems regulating blood glucose levels. Failure of bloodglucose control in personalized medicine represents afailure of the medical care system, not a failure ofthe patient.
References
1. Leventhal H, Brissette I, Leventhal EA. The common sense modelsof self-regulation of health & illness. In: Cameron LD, Leventhal H,eds. The Self-Regulation of Health and Illness Behavior. London:Routledge Taylor & Francis Group; 2003:42-61.
2. Leventhal H, Diefenbach M, Leventhal EA. Illness cognition:using common sense to understand treatment adherence andaffect cognition interactions. Cogn Ther Res. 1992;16:143-163.
3. Anderson R, Funnell M. Theory is the care, vision is the horse:reflections on research in diabetes patient education. DiabetesEduc. 1999;25:43-51.
4. Cook D, Sackett D, Spitzer W. Methodological guidelines for sys-tematic reviews of randomized control trials in health care fromthe Potsdam consultation on meta-analysis. J Clin Epidemiol.1995;48:167-171.
5. Davidson MB. Counterpoint: self-monitoring of blood glucose intype 2 diabetic patients not receiving insulin: a waste of money.Diabetes Care. 2005;28:1531-1533.
6. Welschen LM, Bloemendal E, Nijpels G, et al. Self-monitoring ofblood glucose in patients with type 2 diabetes who are not usinginsulin: a systematic review [see comment]. Diabetes Care. 2005;28:1510-1517.
7. American Diabetes Association. Standards of medical care in dia-betes [position statement]. Diabetes Care. 2007;30:S14-S41.
8. Faas A, Schellevis FG, Van Eijk JT. The efficacy of self-monitoringof blood glucose in NIDDM subjects: a criteria-based literaturereview. Diabetes Care. 1997;20:1482-1486.
9. Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.Monitoring blood glucose control in diabetes mellitus: a system-atic review. Health Technol Assess. 2000;4:1-93.
10. Welschen LMC, Bloemendal E, Nijpels G, et al. Self-monitoringof blood glucose in patients with type 2 diabetes mellitus who arenot using insulin. Cochrane Database Syst Rev. 2006;1:1.
11. Sarol JN Jr, Nicodemus NA Jr, Tan KM, Grava MB. Self-monitoring of blood glucose as part of a multi-component therapyamong non-insulin requiring type 2 diabetes patients: a meta-analysis (1966-2004). Curr Med Res Opin. 2005;21:173-184.
12. Meyer D, Leventhal H, Gutmann M. Common-sense models of ill-ness: the example of hypertension. Health Psychol. 1985;4:115-135.
13. Halm E, Mora P, Leventhal H. No symptoms, no asthma: the acuteepisodic disease belief is associated with poor self-managementamong inner city adults with persistent asthma. Chest. 2006;129:573-580.
14. American Diabetes Association. Standards of medical care in dia-betes [position statement]. Diabetes Care. 2004;27:S15-S35.
15. Vijan S, Hofer TP, Hayward RA. Estimated benefits of glycemiccontrol in microvascular complications in type 2 diabetes. AnnIntern Med. 1997;127:788-795.
16. UK Prospective Diabetes Study Group. Intensive blood-glucosecontrol with sulphonylureas or insulin compared with conven-tional treatment and risk of complications in patients with T2DM.Lancet. 1998;352:837-853.
17. Gray A, Raikou M, McGuire A, et al. Cost-effectiveness of an inten-sive blood glucose control policy in patients with type 2 diabetes:economic analysis alongside randomized controlled (UKPKS 41).Br Med J. 2000;320:1373-1378.
18. Carter JS, Pugh JA, Monterrosa A. Non-insulin-dependent dia-betes mellitus in minorities in the United States. Ann Intern Med.1996;125:221-232.
The Diabetes EDUCATOR
1008
Volume 33, Number 6, November/December 2007
TDE309807.qxd 11/7/2007 11:17 AM Page 1008

19. Rost KM, Flavin KS, Schmidt LE, McGill JB. Self-care predic-tors of metabolic control in NIDDM patients. Diabetes Care.1990;13:1111-1113.
20. Chan WB, Chan JC, Chow CC, et al. Glycaemic control in type 2diabetes: the impact of body weight, beta-cell function and patienteducation. QJM. 2000;93:183-190.
21. Franciosi M, Pellegrini F, De Berardis G, et al. The impact ofblood glucose self-monitoring on metabolic control and quality oflife in type 2 diabetic patients: an urgent need for better educa-tional strategies. Diabetes Care. 2001;24:1870-1877.
22. Hanninen J, Takala J, Keinanen-Kiukaanniemi S. Good continu-ity of care may improve quality of life in type 2 diabetes. DiabetesRes Clin Pract. 2001;51:21-27.
23. Harris MI. Frequency of blood glucose monitoring in relation toglycemic control in patients with type 2 diabetes [see comment].Diabetes Care. 2001;24:979-982.
24. Oki JC, Flora DL, Isley WL. Frequency and impact of SMBG onglycemic control in patients with NIDDM in an urban teachinghospital clinic. Diabetes Educator. 1997;23:419-424.
25. Mitchell CG, Bowker SL, Majumdar SR, Toth EL, Johnson JA.Lack of correlation between patient-reported outcomes andglycemic control in type 2 diabetes not managed by insulin. CanJ Diabetes. 2004;28:362-368.
26. Jaworska J, Dziemidok P, Kulik TB, Rudnicka-Drozak E.Frequency of self-monitoring and its effect on metabolic controlin patients with type 2 diabetes. Ann Univ Mariae CurieSklodowska [Med]. 2004;59:310-316.
27. Patrick AW, Gill GV, MacFarlane IA, Cullen A, Power E,Wallymahmed M. Home glucose monitoring in type 2 diabetes: isit a waste of time? Diabetes Med. 1994;11:62-65.
28. Rindone JP, Austin M, Luchesi J. Effect of home blood glucosemonitoring on the management of patients with non-insulindependent diabetes mellitus in the primary care setting. Am JManag Care. 1997;3:1335-1338.
29. Wieland LD, Vigil JM, Hoffman RM, Janis LW. Relationshipbetween home glucose testing and hemoglobin Alc in type II dia-betes patients. Am J Health Syst Pharm. 1997;54:1062-1065.
30. Wen L, Parchman ML, Linn WD, Lee S. Association betweenself-monitoring of blood glucose and glycemic control in patientswith type 2 diabetes mellitus. Am J Health Syst Pharm. 2004;61:2401-2405.
31. Newman WP, Laqua D, Engelbrecht D. Impact of glucose self-monitoring on glycohemoglobin values in a veteran population.Arch Intern Med. 1990;150:107-110.
32. Meier JL, Swislocki AL, Lopez JR, Noth RH, Bartlebaugh P,Siegel D. Reduction in self-monitoring of blood glucose in per-sons with type 2 diabetes results in cost savings and no change inglycemic control. Am J Manag Care. 2002;8:557-565.
33. Karter AJ, Ackerson LM, Darbinian JA, et al. Self-monitoring ofblood glucose levels and glycemic control: the NorthernCalifornia Kaiser Permanente Diabetes registry. Am J Med. 2001;111:1-9.
34. Blonde L, Ginsberg B, Horn S. Frequency of blood glucose mon-itoring in relation to glycemic control in patients with type 2 dia-betes. Diabetes Care. 2002;25:245-255.
35. Klein CE, Oboler SK, Prochazka A, et al. Home blood glucosemonitoring: effectiveness in a general population of patients whohave non-insulin-dependent diabetes mellitus. J Gen Intern Med.1993;8:597-601.
36. Soumerai S, Mah C, Zhang F, et al. Effects of health maintenanceorganization coverage of self-monitoring devices on diabetes self-care and glycemic control. Arch Intern Med. 2004;164:645-652.
37. Guerci B, Drouin P, Grange V, et al. Self-monitoring of blood glu-cose significantly improves metabolic control in patients withtype 2 diabetes mellitus: the Auto-Surveillance InterventionActive (ASIA) study. Diabetes Metab. 2003;29:587-594.
38. Kibriya MG, Ali L, Banik NG, Azad Khan AZ. Home monitoringof blood glucose (HMBG) in type-2 diabetes mellitus in a devel-oping country. Diabetes Res Clin Pract. 1999;46:253-257.
39. Kwon HS, Cho JH, Kim HS, et al. Establishment of blood glucosemonitoring system using the Internet. Diabetes Care. 2004;27:478-483.
40. Rutten G, van Eijk J, de Nobel E, Beek M, van der Velden H.Feasibility and effects of a diabetes type II protocol with bloodglucose self-monitoring in general practice. Fam Pract. 1990;7:273-278.
41. Schwedes U, Siebolds M, Mertes G, Group SS. Meal-relatedstructured self-monitoring of blood glucose: effect on diabetescontrol in non-insulin-treated type 2 diabetic patients. DiabetesCare. 2002;25:1928-1932.
42. Seaton TL. Benefit of self-monitoring of blood glucose in patientswith NIDDM receiving oral sulfonylureas [abstract]. Pharmaco-therapy. 1996;16:498.
43. Davidson MB, Castellanos M, Kain D, Duran P. The effect of selfmonitoring of blood glucose concentrations on glycated hemo-globin levels in diabetic patients not taking insulin: a blinded, ran-domized trial. Am J Med. 2005;118:422-425.
44. Muchmore DB, Springer J, Miller M. Self-monitoring of bloodglucose in overweight type 2 diabetic patients. Acta Diabetol.1994;31:215-219.
45. Moreland E, Volkening L, Lawlor M, Chalmers K, Anderson B,Laffel L. Use of a blood glucose monitoring manual to enhancemonitoring adherence in adults with diabetes. Arch Intern Med.2006;166:689-695.
46. Allen BT, DeLong ER, Feussner JR. Impact of glucose self-monitoring on non-insulin-treated patients with type II diabetesmellitus: randomized controlled trial comparing blood and urinetesting. Diabetes Care. 1990;13:1044-1050.
47. Miles P, Everett J, Murphy J, Kerr D. Comparison of blood orurine testing by patients with newly diagnosed non-insulindependent diabetes: patient survey after randomised crossovertrial. BMJ. 1997;315:348-349.
48. Cook D, Sackett D, Spitzer W. Methodological guidelines for sys-tematic reviews of randomized control trials in health care fromthe Potsdam consultation on meta-analysis. J Clin Epidemiol.1995;48:167-171.
49. Montori V, Swiontkowski M, Cook D. Methodological issues insystematic reviews and meta-analysis. Clin Orthop. 2002;412:43-54.
50. Higgins JPT, Green S, eds. Cochrane Handbook for SystematicReviews of Interventions 4.2.6 [updated September 2006]. In: TheCochrane Library, Issue 4. Chichester, UK: John Wiley; 2006.
51. Kraemer H, Wilson GT, Fairburn CG, Agras WS. Mediators andmoderators of treatment effects in randomized clinical trials. ArchGen Psychiatry. 2002;59:877-883.
52. Peyrot M, Rubin RR. Modeling the effect of diabetes educationon glycemic control. Diabetes Educator. 1994;20:143-148.
53. Diamond E, Massey K, Covey D. Symptom awareness and bloodglucose estimation in diabetic adults. Health Psychol. 1989;8:15-26.
Patient Blood Glucose Monitoring
1009
McAndrew et al
TDE309807.qxd 11/7/2007 11:17 AM Page 1009

54. Peel E, Parry O, Douglas M, Lawton J. Blood glucose self-monitoring in non-insulin treated type 2 diabetes: a qualitativestudy of patients’ perspectives. Br J Gen Pract. 2004;54:183-188.
55. Reichard P. To be a teacher, a tutor and a friend: the physician’srole according to the Stockholm Diabetes Intervention Study(SDIS). Patient Educ Couns. 1996;29:231-235.
56. DAFNE Study Group. Training in flexible, intensive insulin man-agement to enable dietary freedom in people with type 1 diabetes:Dose Adjustment for Normal Eating (DAFNE) randomized con-trolled trial. BMJ. 2002;325:746-751.
57. Russell L, Suh D, Safford M. Time requirements for diabetes self-management: too much for too many? J Fam Pract. 2005;54:1.
58. Hanninen J, Takala J, Keinanen-Kiukaanniemi S. Quality of lifein NIDDM patients assessed with the SF-20 questionnaire.Diabetes Res Clin Pract. 1998;42:17-27.
Addendum
Since the completion of this systematic review of self-monitoring of blood glucose (SMBG) for patients withtype 2 diabetes, one of the largest randomized control tri-als of SMBG was published in the British MedicalJournal.1 This study provides an important contribution tothe literature in that it is a well-designed trial thataddresses many of the limitations of previous SMBGinterventions, including sufficient power to detect clini-cally meaningful differences in HbA1c levels. In addition,it examined not only SMBG but also SMBG within abehavioral framework using psychological theory. Farmerand colleagues1 randomized 453 patients to 1 of 3 arms: acontrol where patients and their doctors received HbA1creadings prior to an appointment; an SMBG interventionthat asked patients to monitor blood glucose 3 times a day,twice a week and talk to their doctor for interpretation;and an intense SMBG intervention that asked patients tomonitor their glucose levels at the same rate and taughtthem skills for personal interpretation. All patientsreceived a behavioral goal-setting intervention based onLeventhal’s commonsense model of self-regulation.Although the intense self-monitoring group showed a0.17% reduction in HbA1c, the between-group differencefor HbA1c did not reach statistical significance.
Although Farmer and colleagues1 should be com-mended for their well-thought-out and timely study, ofconcern is the discrepancy between HbA1c improvementfound in this trial and the HbA1c improvement found inother trials. Of the 11 randomized control trials (RCTs)examined in this systematic review, only 1 found lessimprovement in HbA1c levels for the SMBG arm,2 withthe majority showing at least 3 times the level of improve-ment. The results presented here suggest that patients
who are in poor control are the ones who may benefit themost from SMBG. The mean baseline HbA1c level of7.5% of the patients recruited by Farmer and colleagues1
may have limited the ability to detect improvement frommonitoring. Consistent with this possibility, Farmer andcolleagues’ reporting of subgroups suggests that patientsin their study who were in poorer control benefited themost from the SMBG intervention, as patients on oralmedication had a greater reduction in HbA1c levels thanthose treated with diet alone (this effect was not statisti-cally tested).
Further analysis of mediating and moderating vari-ables may provide clues as to why intensive interventionpatients did not show significant improvements inHbA1c levels. Specifically, patients need to substituteobjective readings (SMBG) for subjective cues to assessblood sugar levels. Participants in Farmer and col-leagues’ intensive intervention, however, were reportingsignificantly more subjective symptoms used to identifyhypoglycemia episodes.1 As patients concerned abouthypoglycemia have elevated glucose, intensive partici-pants may have experienced conflict between subjectivecues and objective indicators, accepted higher readings,and had the greatest difficulty with self-managementbased on objective readings. This is consistent with theirless frequent use of meters. In addition, patients appearmore likely to succeed in using SMBG to regulate dietand exercise if they monitor both before and 2 hours aftera meal.3 In the paper by Farmer and colleagues, patientswere described as monitoring either before or after ameal.4 It is unclear how patients could develop a behav-ioral regulatory system without specific feedback abouttheir diet and exercise activities.
Although the conclusion that SMBG may be effectivein controlling HbA1c for patients with type 2 diabetesnot treated with insulin is maintained here, the well-designed and adequately powered study by Farmer andcolleagues1 highlights the difficulties both for conductingtrials and for clinical practice. Attention to how (pre-and postaction), when (initially diagnosed), and forwhom (poorly controlled) can maximize the possibilitythat SMBG can help the patients achieve effective bloodsugar control. As patients develop a steady state of gooddiabetes control, they may use SMBG only as an occa-sional check. But as the patient’s physiology changes,causing a deterioration of control, the individual shoulduse SMBG to readjust his or her self-regulation.Recommendations to not use self-monitoring may have
The Diabetes EDUCATOR
1010
Volume 33, Number 6, November/December 2007
TDE309807.qxd 11/7/2007 11:17 AM Page 1010

small ramifications in the short term, but as patients con-tinue in maladaptive regulatory behaviors, the effectsmay be magnified. As such, trials should continue toexamine the effect of SMBG on patients with type 2 dia-betes not on insulin.
References
1. Farmer A, Wade A, Goyder E, et al. Impact of self monitoring ofblood glucose in the management of patients with non-insulintreated diabetes: open parallel group randomised trial. BMJ.2007;335:132.
2. Moreland E, Volkening L, Lawlor M, Chalmers K, Anderson B,Laffel L. Use of a blood glucose monitoring manual to enhancemonitoring adherence in adults with diabetes. Arch Intern Med.2006;166:689-695.
3. Schwedes U, Siebolds M, Mertes G, Group SS. Meal-relatedstructured self-monitoring of blood glucose: effect on diabetescontrol in non-insulin-treated type 2 diabetic patients. DiabetesCare. 2002;25:1928-1932.
4. Farmer A, Wade A, French D, Goyder E, Kinmonth A, Neil A.The DIGEM trial protocol: a randomised controlled trial to deter-mine the effect on glycaemic control of different strategies ofblood glucose self-monitoring in people with type 2 diabetes.BMC Fam Pract. 2005;6:25.
Patient Blood Glucose Monitoring
1011
McAndrew et al
TDE309807.qxd 11/7/2007 11:17 AM Page 1011