
0970711
INFECTIONS IN ORTHOPAEDICS 1865: Lister open fracture with
carbolic acid World War II: Prophylactic antibiotics,
leaving wounds open Approach infections benign tumor
rarely is fatal, but recur if not adequately treated
the chemotherapy is antibiotics tumor surgery principles
millions of bacteria populate skin and body cavities
Microorganisms biofilm slime layer colonizing surfaces: resistant to antagonists
Colonization of surfaces: not always synonymous with infection

TABLE 18-1 Bacteria Commonly Found on the Surfaces of the Human Body
Bacterium SkinConjunctiva Nose
Pharynx Mouth
Staphylococcus epidermidis (1)
++ + ++ ++ ++
Staphylococcus aureus* (2) + +/- + + +Streptococcus mitis + ++Streptococcus salivarius ++ ++Streptococcus mutans* (3) + ++Enterococcus faecalis* (4) +/- +Streptococcus pneumoniae* (5)
+/- +/- + +
Streptococcus pyogenes* (6) +/- +/- + +Neisseria sp. (7) + + ++ +Neisseria meningitidis* (8) + ++ +Veillonellae sp. +Enterobacteriaceae* (Escherichia coli) (9)
+/- +/- +/- +
Proteus sp. +/- + + +Pseudomonas aeruginosa* (10)
+/- +/-
Haemophilus influenzae* (11) +/- + + +Bacteroides sp.*Bifidobacterium bifidum (12)Lactobacillus sp. (13) + ++Clostridium sp.* (14) +/-Clostridium tetani (15)++ = nearly 100 percent, + = common, +/- = rare, * = potential pathogen.
Pathogenesis
Planktonic state: bacteria / small clusters that are not colonized metabolically active susceptible to the body's host defense
systems / antibiotics Bacterial colonization: bacteria adhere
to a surface resists host and extrinsic efforts at eradication
Inert surface: glycoproteinaceous film
early stages of colonization: bacteria can be killed or contained by host defenses
bacteria can remain the inoculum is larger than threshold levels host defense mechanisms are impaired the tissue on which the bacteria colonize is
traumatized (or necrotic), a foreign body is present, the surface (or tissue) is acellular or inanimate
(e.g., dead bone, cartilage, and biomaterials) Colonization alone is not enough for
infection, but rather a necessary antecedent

Bacteria bone surface or biomaterial surface: direct contamination contiguous spreading hematogenous seeding
van der Waals forces bacteria to develop “irreversible” cross-links with the surface (adhesin receptor interaction)
Adhesion: time-dependent specific protein adhesion-receptor
interactions carbohydrate polymer synthesis charge and physical forces: surface is anionic and
initially repels bacteria (which are also anionic) anchorage to the surface polysaccharide slime
layer, “biofilm-enclosed” colony of bacteria forms
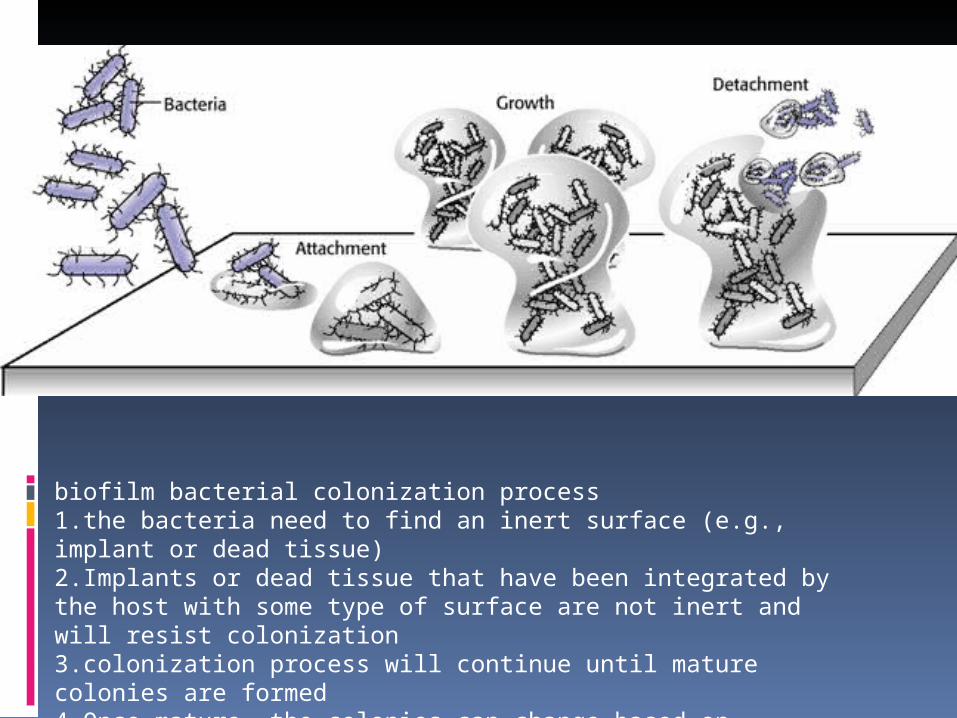
biofilm bacterial colonization process1.the bacteria need to find an inert surface (e.g., implant or dead tissue)2.Implants or dead tissue that have been integrated by the host with some type of surface are not inert and will resist colonization3.colonization process will continue until mature colonies are formed4.Once mature, the colonies can change based on environmental signals or signals between colonies

Biofilm: a community of sessile bacteria, surrounded by a glycocalyx of extracellular matrix only form on inert or nonviable surfaces antibiotics penetrate this film
Biofilm (or slime): extracapsular exopolysaccharides bind to surfaces / cell-to-cell aggregation
Inert surface (dead tissue, implants, or debris): area for bacteria to colonize and form biofilm escape the host defense, antibiotic treatments

Body control the bacterial colonization abscess or involucrum is formed
sinus: method to dispel the detritus and bacteria
equilibrium chronic infection history of intermittent symptoms and
drainage that responds to an antibiotic Bacteria numbers / weakening of the systemic
host: infection develop, spread, and persist Small electric fields, low pH, as well as acidic
and negatively charged surfaces: resistant to biofilms adjunctive treatments
Adherence to Bone and Biomaterials Damaged bone: bacterial
colonization Bone relatively acellular No normal periosteum presents a
collagen matrix bacteria can bind bone sialoprotein: a ligand for
bacterial binding to bone

Biomaterials / foreign bodies: bacterial colonization
outer surface atomic layer glycoproteins prokaryotic and eukaryotic cells Stainless steel and cobalt-chromium
and titanium resistant to corrosion Elemental composition, crystalline
homogeneity, and the surface oxide passivates
Antibiotic Resistance
resistance ~~ depend on the type of surface hydrocarbon polymers: extremely resistant to
antibiotics Metals: resist antibiotic therapy ↓
bacteria within biofilms decreased metabolic rate and undergo phenotypic changes resistance and virulence
bacteria adherent to surfaces: more resistant to antibiotics
within the biofilm: antibiotic concentrations of greater than 1,500 times normal
most antimicrobials work via interference with cell wall synthesis or reproduction and require metabolically active bacteria biofilm appear dormant resistant
Acute Posttraumatic Osteomyelitis Traumatized soft tissue and bone
exposes Traumatized tissue compromised
blood supply, tissue and bone necrosis infection
Fixation devices hypotension, inadequate debridement
of the fracture site, malnutrition, alcoholism, and smoking

Tissue injury or bacteria:A. activation of the complement cascade
local vasodilationB. tissue edemaC. migration of polymorphonuclear leukocytesD. enhanced ability of phagocytes to ingest
bacteria Trauma
A. delay the inflammatory response to bacteriaB. depress cell-mediated immunityC. impair function of polymorphonuclear
leukocytes (chemotaxis, superoxide production, and microbial killing)

Chronic Osteomyelitis
degree of bone necrosis, nutrition, infecting organism, age, comorbidity, and drug abuse
acute osteomyelitis Staphylococcus aureus
after a fracture polymicrobial (although in most cases, it is S. aureus)
IV drug users Pseudomonas / S. aureus infections
Gram-negative organisms: 50% of all cases of chronic osteomyelitis

fractures or surgical procedures: enter the bone directly
A surgical or traumatic insult: no longer perfused adequately
collagen protein matrix and acellular crystal regions
devascularization of bone necrotic material seclusion from systemic antibiotic therapy
Sequestrum wall off with a reactive and inflammatory (involucrum)
Involucrum: highly vascular and potentially viable and structural
Classification
acute or chronic based on the etiology of the
osteomyelitis type I (hematogenous) type II (osteomyelitis with fracture
union) type III (osteomyelitis without fracture
union) type IV (postoperative or posttraumatic
osteomyelitis without fracture)

1984, based on the nature of the bony involvement: Weiland et al: type I (open, exposed bone without soft tissue infection) type II (circumferential cortical and endosteal infection) type III (associated with a segmental defect).
1989, based on the nature of the bone after soft tissue and bony debridement: May et al: type I (intact tibia and fibula able to withstand functional loads
with no reconstruction needed) type II (intact tibia unable to withstand functional loads
requiring bone grafting; type III (<6 cm tibial defect with an intact fibula requiring
cancellous bone grant, tibiofibular synostosis, or distraction histogenesis)
type IV (<6 cm tibial defect and intact fibula requiring distraction histogenesis, tibiofibular synostosis, or a vascularized bone graft)
type V (>6 cm tibial defect without an intact fibula requiring a possible early amputation

Cierny and Mader
based on four factors: the degree of osseous involvement, the site of involvement, the degree of impairment caused by the disease, and the host's general condition
Type I: medullary osteomyelitis (examples of which include hematogenous osteomyelitis and infections of intramedullary rods).
Type II: superficial osteomyelitis confined to the bone surface.
Type III: localized osteomyelitis involving the full thickness of the cortex but without the loss of axial stability.
Type IV: diffuse osteomyelitis involving the circumference of the cortex and loss of axial stability.

Cierny and Mader's types of osteomyelitis.
Cierny-Mader Staging System for Osteomyelitis Anatomic Type
Stage 1: Medullary osteomyelitisStage 2: Superficial osteomyelitisStage 3: Localized osteomyelitisStage 4: Diffuse osteomyelitis
Physiologic ClassA host: HealthyB host: Bs: Systemic compromise Bl: Local compromise Bls: Local and systemic compromiseC host: Treatment worse than the disease
Factors Affecting Immune Surveillance, Metabolism, and Local VascularitySystemic factors (Bs): Malnutrition, renal or hepatic failure, diabetes mellitus, chronic hypoxia, immune disease, extremesof age, immunosuppression or immune deficiencyLocal factors (Bl): Chronic lymphedema, venous stasis, majorvessel compromise, arteritis, extensive scarring, radiation fibrosis, small-vessel disease, neuropathy, tobacco abuse Reprinted with permission from Cierny G, Mader JT, Pennick H. A clinical staging system of adult osteomyelitis. Contemp Orthop 1985;10:17–37.

Class A patients have normal systemic defenses, metabolic capabilities, and vascular supply to the limb.
Class B patients have a local (trauma, prior surgery, local inflammation) or systemic (immunosuppressed, on corticosteroids, peripheral vascular disease) deficiency
Class C patients are those in whom the treatment of the disease (the infection) is worse than the infection itself
success rates of 98% were achieved, even in type IV osteomyelitis
class B hosts: anatomic type, success ranged from 79% to 92%.







