
12/20/2017
1
VIRGINIA HOSPITALS AND SKILLED NURSING FACILITIES: PARTNERS IN PREVENTING READMISSIONS
Amy Boutwell MD MPPDecember 12, 13, 14, 2017
Leesburg, Mechanicsville, Lynchburg, VA
WELCOMEAbraham Segres, April Payne

12/20/2017
2
FORMAT, AGENDAAmy Boutwell, MD, MPP
AGENDAYour goalCurrent effortsData/root causesWhat works?What will work for you?Measures to drive resultsHarvest ideas, prioritizeAction plan, report out

12/20/2017
3
YOUR GOALWhat is your specific readmission reduction goal?
What – for whom – by how much – by when?
READMISSION REDUCTION GOAL
20% reduction from baseline is aggressive but feasible
Often is achievable within 1-2 years
Trend monthly# readmissions % readmission rate
12/20/2017
4
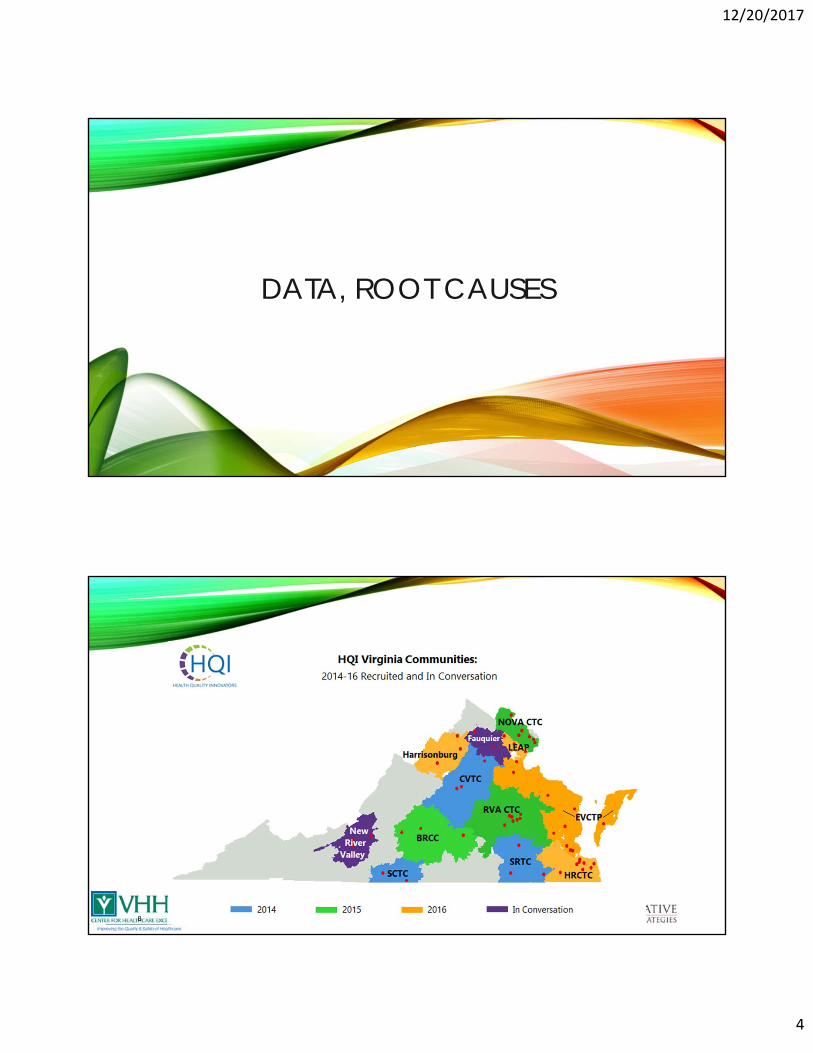
DATA, ROOT CAUSES
8
12/20/2017
5
CommunityTotal #
Hospital DCsTotal # of DCs Readmitted
Readmit Rate
Total # of Hospital DCs
to SNFs
Total # of Hospital DCs to SNFs Readmitted
SNF Readmit Rate
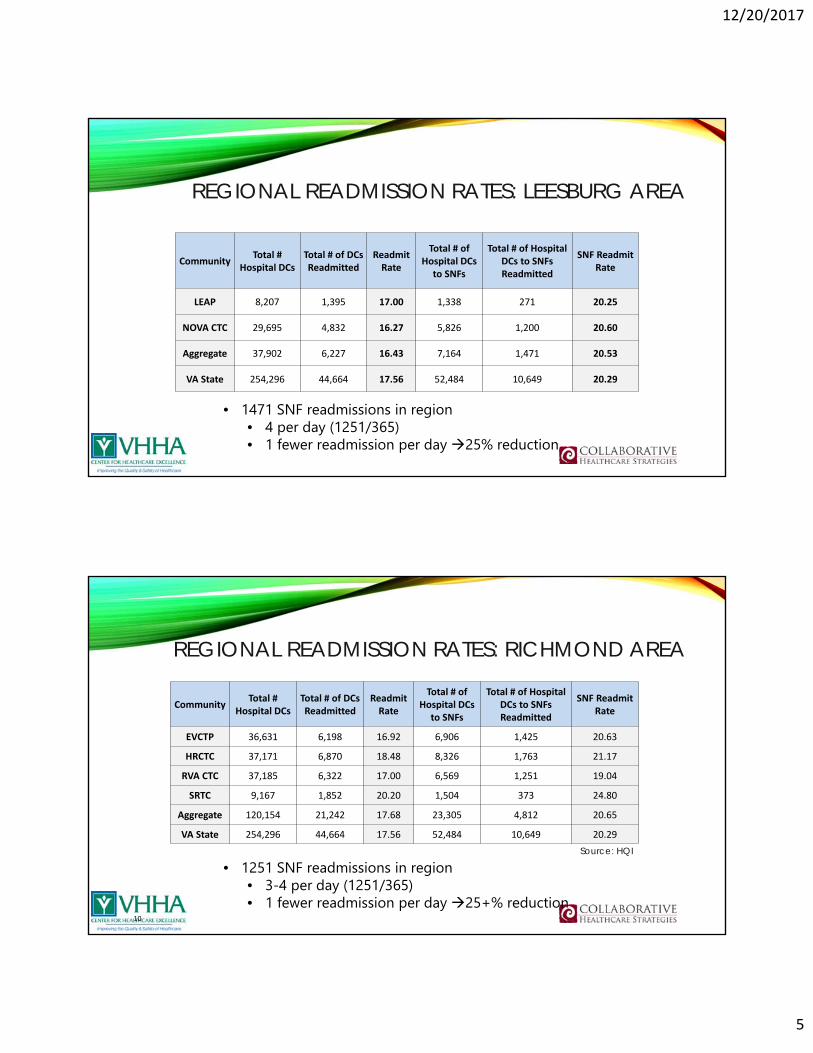
LEAP 8,207 1,395 17.00 1,338 271 20.25
NOVA CTC 29,695 4,832 16.27 5,826 1,200 20.60
Aggregate 37,902 6,227 16.43 7,164 1,471 20.53
VA State 254,296 44,664 17.56 52,484 10,649 20.29
REGIONAL READMISSION RATES: LEESBURG AREA
• 1471 SNF readmissions in region• 4 per day (1251/365)• 1 fewer readmission per day 25% reduction
REGIONAL READMISSION RATES: RICHMOND AREA
10
• 1251 SNF readmissions in region• 3‐4 per day (1251/365)• 1 fewer readmission per day 25+% reduction
Source: HQI
CommunityTotal #
Hospital DCsTotal # of DCs Readmitted
Readmit Rate
Total # of Hospital DCs
to SNFs
Total # of Hospital DCs to SNFs Readmitted
SNF Readmit Rate
EVCTP 36,631 6,198 16.92 6,906 1,425 20.63
HRCTC 37,171 6,870 18.48 8,326 1,763 21.17
RVA CTC 37,185 6,322 17.00 6,569 1,251 19.04
SRTC 9,167 1,852 20.20 1,504 373 24.80
Aggregate 120,154 21,242 17.68 23,305 4,812 20.65
VA State 254,296 44,664 17.56 52,484 10,649 20.29

12/20/2017
6
REGIONAL READMISSION RATES: LYNCHBURG AREA
11
• 1628 SNF readmissions in region• 4‐5 per day (1251/365)• 1 fewer readmission per day 20% reduction
Source: HQI
CommunityTotal #
Hospital DCsTotal # of DCs Readmitted
Readmit Rate
Total # of Hospital DCs
to SNFs
Total # of Hospital DCs to SNFs Readmitted
SNF Readmit Rate
BRCC 14,187 2,382 16.79 3,670 685 18.66
CVTC 11,477 1,908 16.62 2,280 446 19.56
SCTC 8,551 1,594 18.64 2,259 497 22.00
Aggregate 34,215 5,884 17.20 8,209 1,628 19.83
VA State 254,296 44,664 17.56 52,484 10,649 20.29
12
DAYS UNTIL READMISSION
Source: HQI
Consider the different causes of readmissions over 30 days:
• 0-5 days?
• 5-20 days?
• 20-30 days?
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Days Until Readmission from SNF Aggregate Communities (Jul2016‐Jun2017)

12/20/2017
7
13
DISCHARGE DXS LEADING TO READMISSION
What’s surprising? 246
68
64
56
55
52
50
40
34
34
0 50 100 150 200 250 300
Other sepsis
Cerebral infarction
Acute kidney failure
Hypertensive heart and chronic kidney disease
Heart failure
Fracture of femur
Other disorders of urinary system
Type 2 diabetes mellitus
Respiratory failure, not elsewhere classified
Osteoporosis with current pathological fracture
Top Principal Discharge Diagnoses Leading to a Readmission from SNFs in Aggregate Communities (Jul2016‐Jun2017)
14
TOP READMISSION DXS
What’s surprising? 364
90
75
57
43
39
36
36
33
32
0 50 100 150 200 250 300 350 400
Other sepsis
Hypertensive heart and chronic kidney disease
Acute kidney failure
Respiratory failure, not elsewhere classified
Heart failure
Cerebral infarction
Other diseases of digestive system
Other disorders of urinary system
Other chronic obstructive pulmonary disease
Hypertensive heart disease
Top Principal Readmission Diagnoses from SNFs in Aggregate Communities (Jul2016‐Jun2017)

12/20/2017
8
ROOT CAUSES OF READMISSIONS
• 78M hospitalized for UTI; readmitted 1 day for altered mental status
• 69F hospitalized for back pain; readmitted 3 days after family called 911 from SNF
• 84F hospitalized for weakness; sent to ED 1 week after discharge for “bad labs”
• 89F hospitalized for pneumonia; readmitted 22 days later from home
ADDRESS THE ROOT CAUSES
Incomplete information about clinical status
Incomplete information about functional status
Incomplete information about behavioral health or “sundowning”
Missing hard copies of controlled substance prescription
Missing documentation of placement of tubes or lines (eg picc lines)
Delays in obtaining (rare, expensive) medications
Change in clinical status but not emergency
Patient/family dissatisfaction with the facility
Readmissions following discharge from SNF to home
Others?

12/20/2017
9
WHAT WORKS?
“PORTFOLIO OF STRATEGIES”
Improve standard care processes for all patients
Collaborate with cross-setting partners; ensure linkage
Provide enhanced services
Use data, analytics, flags, workflow prompts, automation, dashboards to support continuous improvement, ensure reliability, drive to results

12/20/2017
10
WARM HANDOFFS WITH “CIRCLE BACK” CALL
SNF Circle Back Questions (Hospital calls back SNF 3‐24h after d/c): Did the patient arrive safely?
Did you find admission packet in order?
Were the medication orders correct?
Does the patient’s presentation reflect the information you received?
Is patient and/or family satisfied with the transition?
Have we provided you everything you need to provide excellent care to the patient?
Key Lessons:• Transitions are a process (forms are useful, but need intent)
• Best done iteratively with communicationSource: Emily Skinner, Carolinas Healthcare System
WARM HANDOFFS WITH “CIRCLE BACK” CALLIMPLEMENTATION TIPS
Richmond, VA hospital and several partnering SNFs
• 1 point person RN made the post transfer calls
• Each SNF knew the name, contact of that 1 RN at the hospital
• The asked the 6 questions and followed up on all issues
Key tips:
• Point person is key for fostering collaborative relationship
• RN provides “reminder” to floor RN, CM, MD about what was missing
• RN follows up with “issues here” and “issues there”

12/20/2017
11
CIRCLE BACK: “IDEAS THAT WORK”IMPLEMENTATION EXAMPLE
https://www.youtube.com/watch?v=SG28aJhs63s
“Anytime I discover an issue, I always follow up. When I started making the calls, I found issues 26% of the time; last month I only had issues 8% of the time”
‐ Hospital RN
“6 simple questions are making a difference in the Richmond community”
CO‐MANAGEMENT OVER TIME
• Dedicated Team: A Point Person
• ACO or Bundle clinical coordinator
• Co‐Management: Physical or Virtual Rounds in SNF
• RN / NP to see patient, discuss plan with SNF staff
• Respond to changes in clinical status to manage in setting
• Weekly telephonic rounds ACO/bundle coordinator and SNF
• LOS, progress toward discharge goals, transitional care planning
• Tele‐medicine consults in SNF to manage on‐site
• Direct admit back to SNF from home
Took a while to develop collaborative rapport v. hospital “in‐charge”
No substitute for verbal communication and problem solving
12/20/2017
12
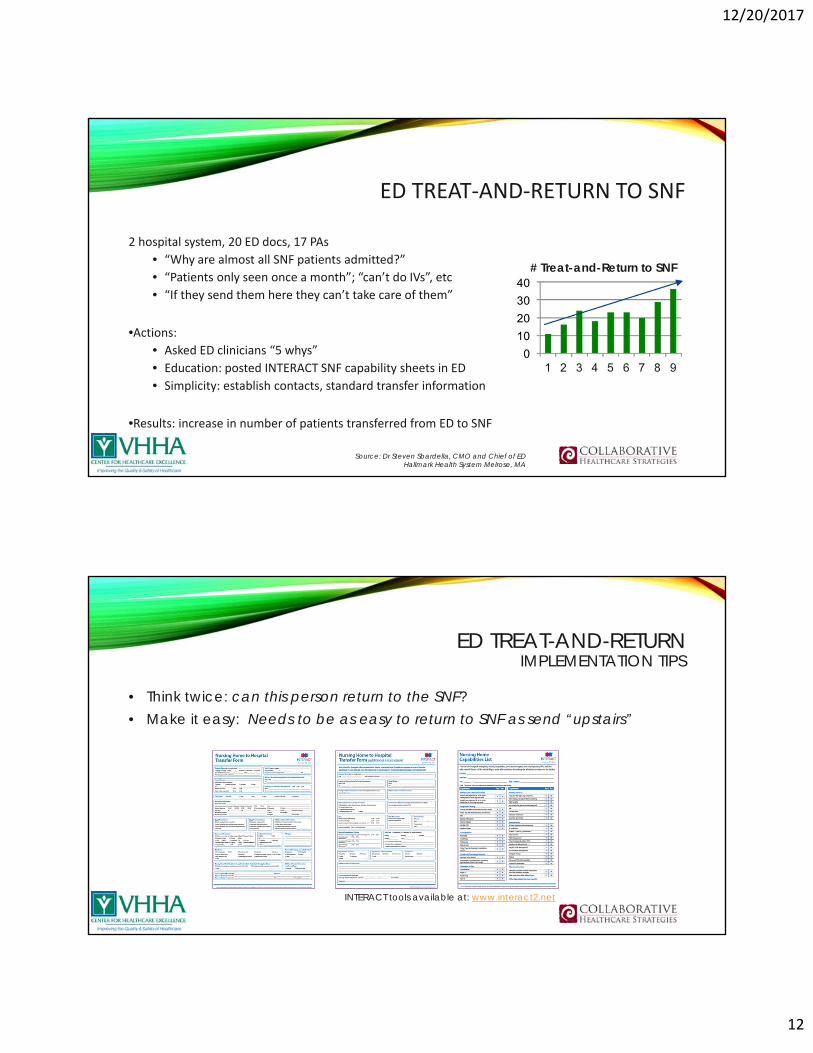
ED TREAT‐AND‐RETURN TO SNF
2 hospital system, 20 ED docs, 17 PAs
• “Why are almost all SNF patients admitted?”
• “Patients only seen once a month”; “can’t do IVs”, etc
• “If they send them here they can’t take care of them”
•Actions:• Asked ED clinicians “5 whys”
• Education: posted INTERACT SNF capability sheets in ED
• Simplicity: establish contacts, standard transfer information
•Results: increase in number of patients transferred from ED to SNF
Source: Dr Steven Sbardella, CMO and Chief of EDHallmark Health System Melrose, MA
# Treat-and-Return to SNF
ED TREAT-AND-RETURNIMPLEMENTATION TIPS
• Think twice: can this person return to the SNF?• Make it easy: Needs to be as easy to return to SNF as send “upstairs”
INTERACT tools available at: www.interact2.net

12/20/2017
13
BEST PRACTICES OF CROSS SETTING COLLABORATION
• Shared understanding of (best‐available) data
• Shared understanding of patients and caregivers’ perspective
• Shared understanding of “receivers” perspective
• Clearly identified specific, feasible improvement ideas
• Improvements are “hardwired” into new standard processes
• Regular meetings, joint problem‐solving
WHAT WILL WORK FOR YOU?

12/20/2017
14
MEASURES TO DRIVE RESULTSTrack implementation, not just outcomes – you will need to drive and
modify and innovate to get highly reliable implementation outcomes
PERCENT OF TARGET POPULATION SERVED
0
50
100
150
200
250
300
350
400
450
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr
Target Population
Target Population “Served” vs. Total Target Population
For hospitals: • # patients d/c to SNF• # “served”
For SNFs:• # patients admitted from hospital• # “served”
Close the gap! That takes focus, effort

12/20/2017
15
TIMELY CONTACT
For hospitals: • # patients d/c to SNF• # ”circle back” contact <48h• # contact <48h of d/c SNF to home
For SNFs:• # patients d/c to home• # contact <48h
Drive to goal >80% completed contact
PATIENT-FACING CONTACTS PER PATIENT
For hospitals: • # ”contacts” while in SNF• # contacts once d/c home
For SNFs:• # contacts once d/c home
Innovate: prioritize patient support, with same staff– that’s what helps

12/20/2017
16
HARVEST, PRIORITIZE
BRAINSTORM
• Do you have a clearly articulated readmission reduction goal? • Do you know you readmission data? • Have you analyzed the root causes of readmissions? • Do you review every readmission for root causes, opportunities for improvement? • Do you have a post-person relationship across settings? • Do you engage in warm handoffs or circle back?• Do you have a “portfolio of strategies” in place? • Do you have an operational dashboard to guide improvement work?

12/20/2017
17
Hard to Do --------Easy to Do
Low
Ben
efit
--
----
High
Ben
efit
ACTION PLAN
12/20/2017
18
ACTION PLAN
• Name of Plan• Action Steps
• What needs to happen, who will do it, by when?• ”Stakeholders”
• Who could stop progress, and how will you engage that person• Expected benefit
• What will be the benefit of completing this plan?• Measurement
• How will you measure what you did?
REPORT OUT

12/20/2017
19
THANK YOU FOR YOUR COMMITMENT TO REDUCING READMISSIONS
Amy E. Boutwell, MD, MPPAdvisor, VHHA Center for Healthcare Excellence
Physician Advisor, Cynosure Health for AHA/HRET [email protected]







