Download - Disclosures - PA NSQIP CONSORTIUM (PANC)

Disclosures
A Tafur
•I have the following financial relationships to disclose:
Consultant for: VTE TAP (Joint Commission),
ACCP Perioperative Anticoagulation Guidelines
Speaker’s Bureau for: None
Grant/Research support from: Janssen, BMS, Daiichi Sankyo, BioTab
Stockholder in: NA
Honoraria from: NA
Employee of: NSUHS

Disclosures
D Najman
•I have the following financial relationships to disclose:
Consultant for: None
Speaker’s Bureau for: None
Grant/Research support from: None
Stockholder in: None
Honoraria from: None
Employee of: NSUHS



Periprocedural anticoagulation
To bridge, or a bridge to nowhere.
Alfonso J Tafur MD MS RPVI FSVM
Vascular Medicine
Northshore University Health System
University of Chicago
David M Najman MD FACC
Cardiology
Northshore University Health System
University of Chicago
• Scope of the problem
• Why and What
Available resources
Cases
• Propositions to improve patient care
Scope of the problem
Why and What
Available resources
Cases
Propositions to improve patient care
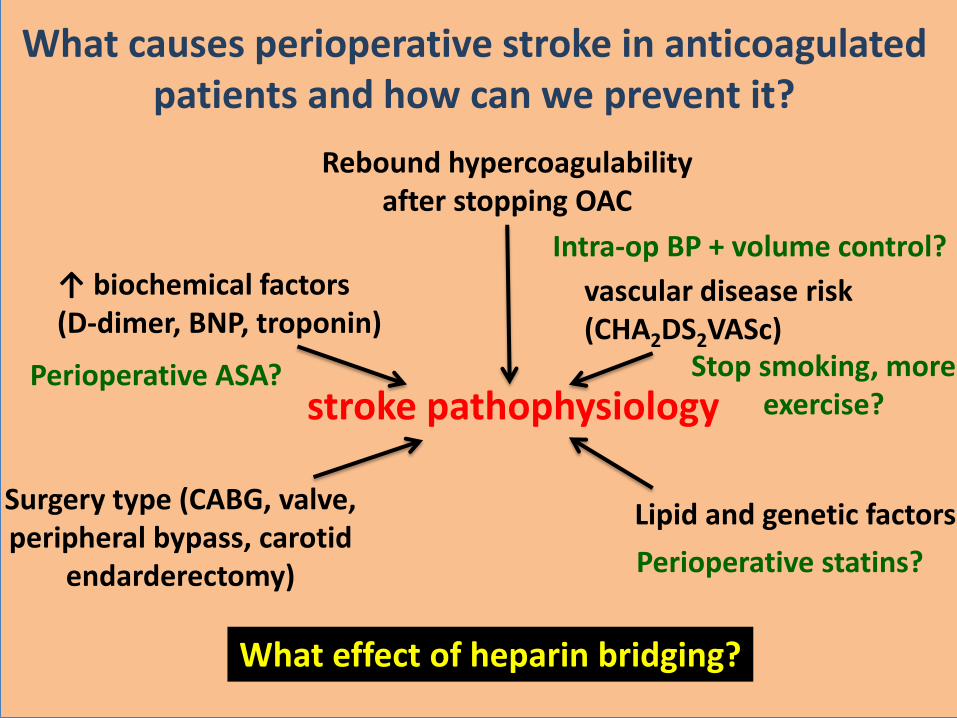
stroke pathophysiology
vascular disease risk (CHA2DS2VASc)
↑ biochemical factors (D-dimer, BNP, troponin)
Surgery type (CABG, valve, peripheral bypass, carotid
endarderectomy)
Lipid and genetic factors
Intra-op BP + volume control?
Perioperative statins?
Stop smoking, more exercise?
What effect of heparin bridging?
What causes perioperative stroke in anticoagulated patients and how can we prevent it?
Perioperative ASA?
Rebound hypercoagulability after stopping OAC

SCOPE OF THE PROBLEM SHOULD I STOP?
Outcomes Registry for Better Informed Treatment
of Atrial Fibrillation (ORBIT-AF) registry.
National community-based of 7,372 patients
treated with oral anticoagulation
2,803 interruptions.
More than 20% were avoidable: dental, cardiac
device, catheter ablation procedures
Steinberg BA, et al . Circulation. 2015;131(5):488-94.

Scope of the problem
Why and What
Available resources
Cases
Propositions to improve patient care

A B
C D
High Bleed risk?
Hig
h T
hro
mbotic r
isk?
The Golden Circle
“First Why and then Trust” Simon Sinek
WHY
HOW
WHAT
“ There are only two ways to influence human behavior: you can manipulate it or you can inspire it”

Why? • The bridging process risk and expense.
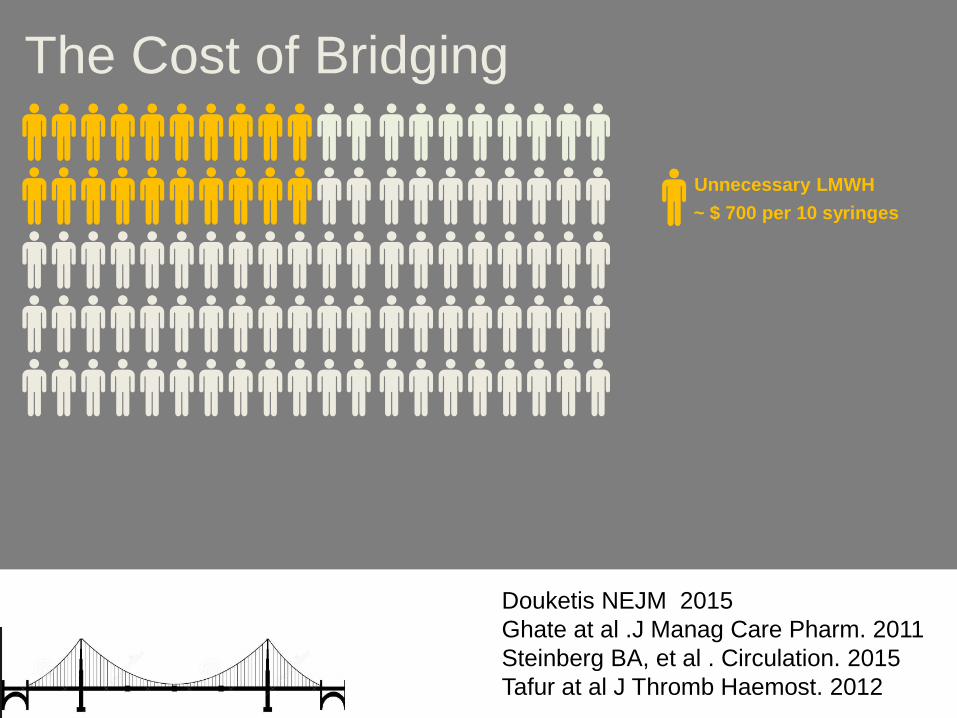
Unnecessary LMWH
~ $ 700 per 10 syringes
The Cost of Bridging
Douketis NEJM 2015
Ghate at al .J Manag Care Pharm. 2011
Steinberg BA, et al . Circulation. 2015
Tafur at al J Thromb Haemost. 2012
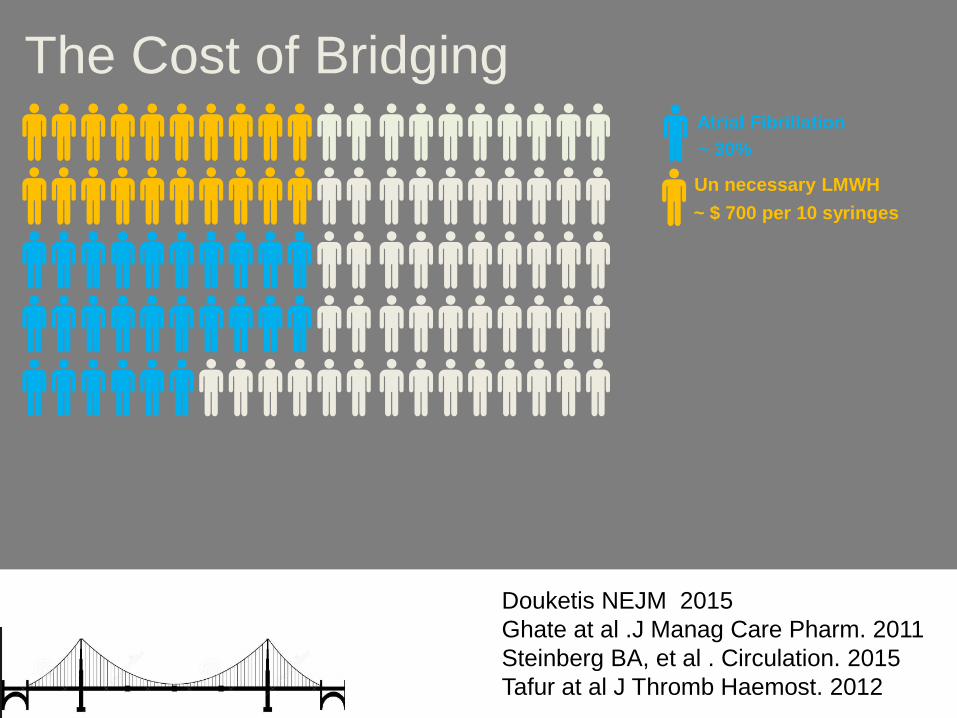
Un necessary LMWH
Atrial Fibrillation
~ $ 700 per 10 syringes
~ 30%
The Cost of Bridging
Douketis NEJM 2015
Ghate at al .J Manag Care Pharm. 2011
Steinberg BA, et al . Circulation. 2015
Tafur at al J Thromb Haemost. 2012

Excess Bleed
Un necessary LMWH
Atrial Fibrillation
~ $ 40,000 per Claim
~ $ 700 per 10 syringes
~ 30%
The Cost of Bridging
Douketis NEJM 2015
Ghate at al .J Manag Care Pharm. 2011
Steinberg BA, et al . Circulation. 2015
Tafur at al J Thromb Haemost. 2012
> $ 100,000 excess cost per 100 patients
Why? • The bridging process risk and expense.
How? • Ask first SHOULD I STOP ?
What? • Uninterrupted anticoagulation for minor
procedures
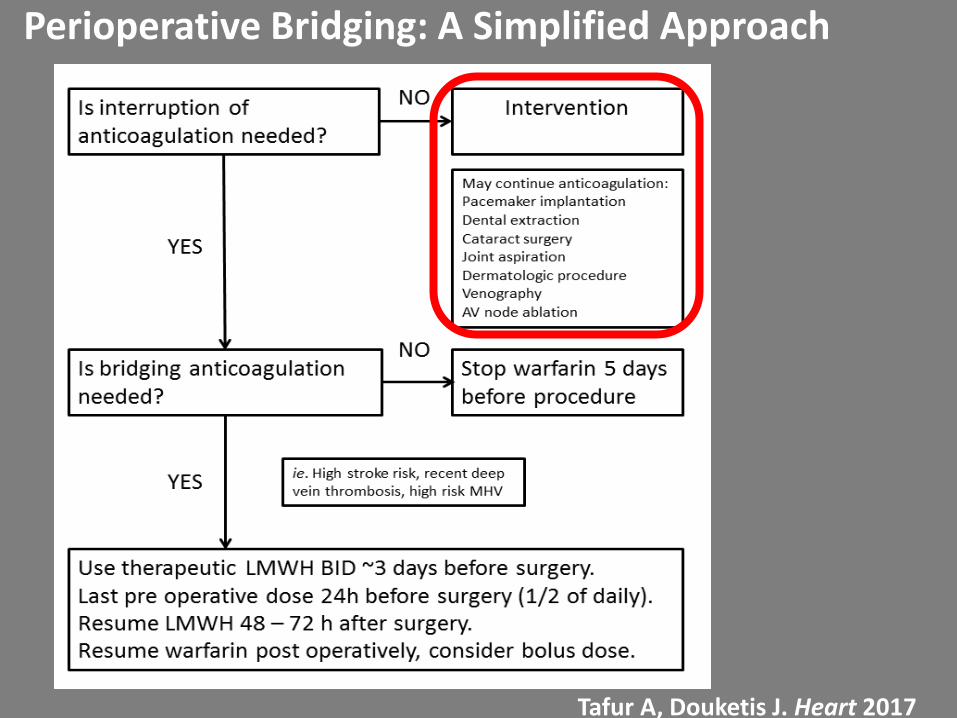
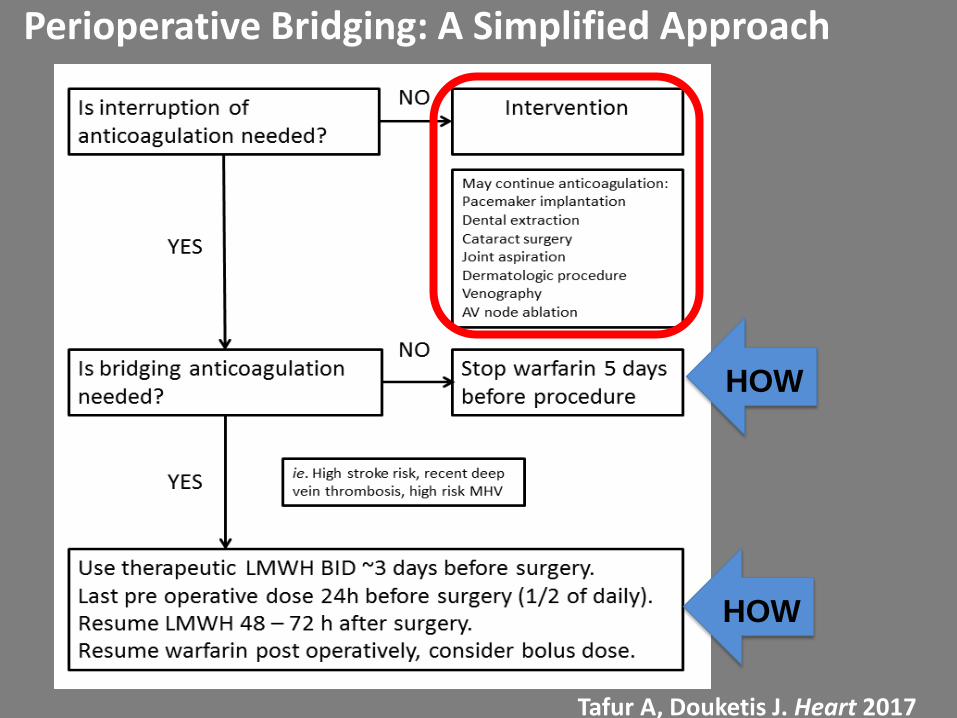
Perioperative Bridging: A Simplified Approach
Tafur A, Douketis J. Heart 2017
Case 1
• 65 YOM with Hernia, scheduled for elective LAPAROSCOPIC left INGUINAL HERNIA REPAIR WITH MESH.
• 72 Kg (BMI 22), creatinine 0.9
• V Leiden Hx and Warfarin anticoagulation noted during encounter
• Held Warfarin 4 d pre op. Enoxaparin 80 pre op.

• LMWH 40 mg BID and Coumadin bridge after PCP to manage INR
• POD 2 Patient confused about Augmentin
• POD 5 return to ED: ecchymosis over mid abdomen, penis and Scrotum. INR 1.1
• Discharge “Hgb was monitored and blood thinners held. Pt Hgb
remained stable and pt was discharged home with instruction to have Hgb drawn on Wed 10/25/17 and to cont to hold blood thinners until after CBC on 10/25/17”
Why? • The risk of perioperative thrombosis is NOT
predicted by thrombophilia alone.
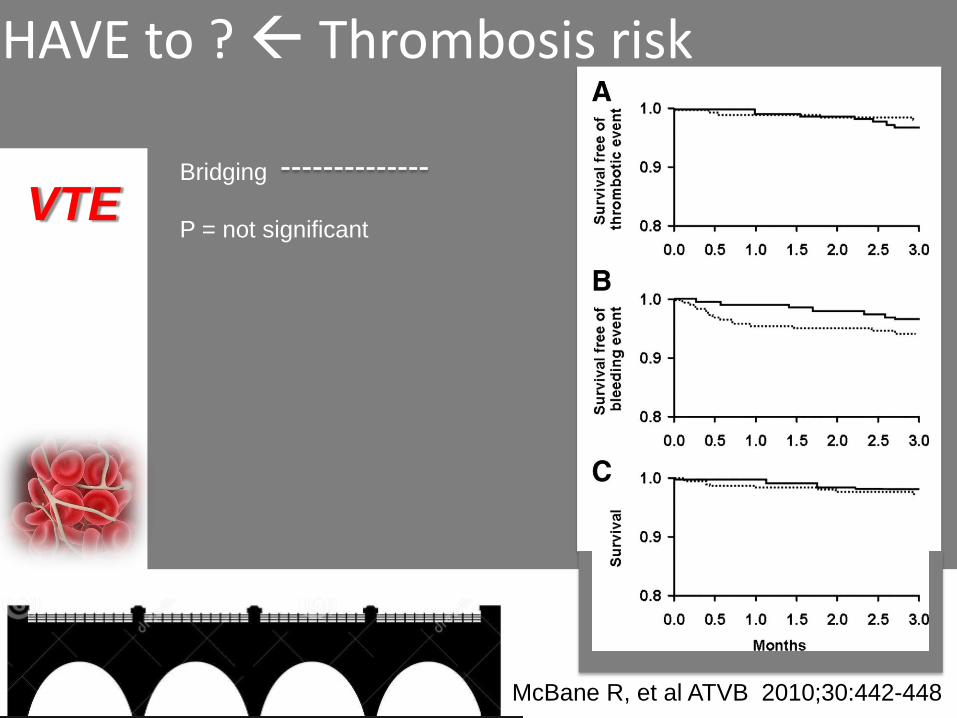
HAVE to ? Thrombosis risk
VTE Bridging
P = not significant
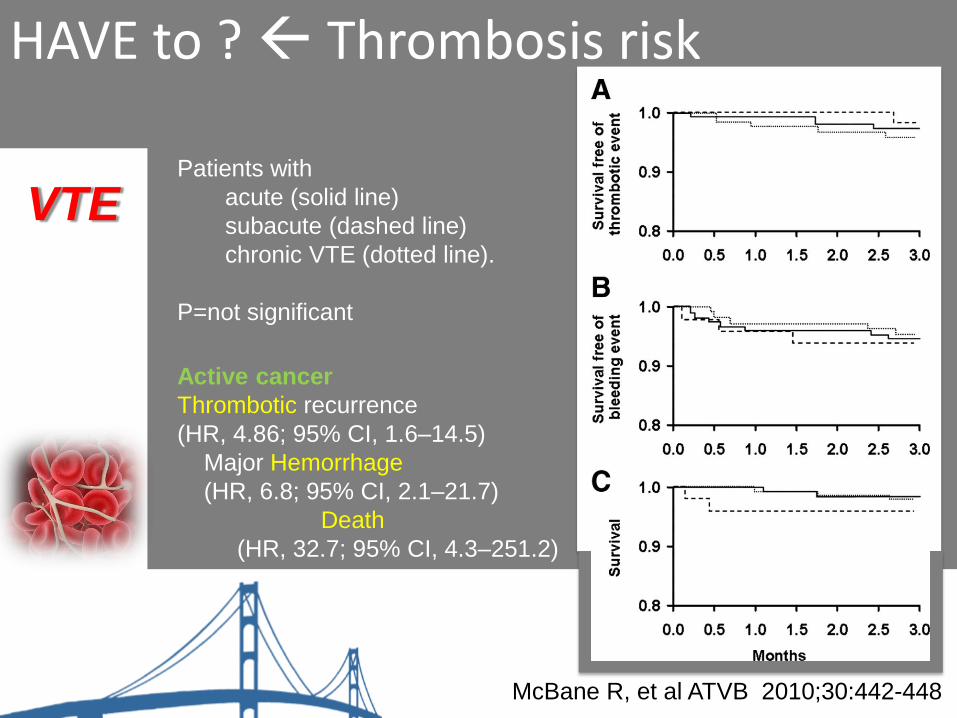
McBane R, et al ATVB 2010;30:442-448
HAVE to ? Thrombosis risk
VTE
McBane R, et al ATVB 2010;30:442-448
Patients with
acute (solid line)
subacute (dashed line)
chronic VTE (dotted line).
P=not significant
Active cancer
Thrombotic recurrence
(HR, 4.86; 95% CI, 1.6–14.5)
Major Hemorrhage
(HR, 6.8; 95% CI, 2.1–21.7)
Death
(HR, 32.7; 95% CI, 4.3–251.2)

HAVE to ? Thrombosis risk
CA
Tafur A, et al Ann Oncol (2012) 23 (8): 1998-2005.

HAVE to ? Thrombosis risk
CA
Tafur A, et al Ann Oncol (2012) 23 (8): 1998-2005.
More
VTE
(1.2 % vs 0.2 %)
Major bleeding
(3.4 % vs 1.7 %)
Death
(95 % OS vs
99 %).
HAVE to ? Thrombosis risk
VTE
Wysokinska E, et al Am J Med 2016; 129 (9):986
Prospective Cohort All pts followed 3 mo post op 362 patients with complete thrombophilia testing 165 (46%) had a defined thrombophilia Bridging was not randomized but equally distributed During follow-up, there were no thromboembolic events

Why? • The risk of perioperative thrombosis is NOT
predicted by thrombophilia alone.
How? • Inquire detailed anticoagulation indication Hx.
– Time since VTE, Cancer related?
What? • Avoid high dose bridging in non Cancer patients
Why? • The t ½ of Enoxaparin is 4.5 h
Study: Consecutive patients who had bridging
Enoxaparin, 1 mg/kg of body weight, twice daily.
The last dose was administered the evening before surgery.
Blood anti–factor Xa heparin levels measured shortly before surgery.
Average pre op anti-Xa heparin level was 0.6 U/mL.
Highest levels if:
Shorter interval since the last dose (P < 0.01)
Higher body mass index (P < 0.01)
O’Donnell M. et al. Ann Inter Med 2007

Why? • The t ½ of Enoxaparin is 4.5 h
How? • Written calendar format instructions to pt.
What? • Last dose of enoxaparin MORNING of day pre op
Why? • The t ½ of Enoxaparin is 4.5 h
How? • Written calendar format instructions to pt.
What? • Last dose of enoxaparin MORNING of day pre op
Perioperative Bridging: A Simplified Approach
Tafur A, Douketis J. Heart 2017
HOW
HOW
Atrial fibrillation, benign neck mass
• 74 YOM with Atrial fibrillation and anticoagulation with warfarin + ASA.
• AICD 2009, Hx of endocarditis, HTN.
• NO Hx of stroke, DM, PAD.
/CHADS2 2/
Case 2

• PCP Coumadin per Cardiology
• Cardiology: – 10/25 last dose coumadin
– 10/26, 27, 28, 29-one shot 2x/day
– 10/30-procedure-no lovenox
(optional pm dose, per neck surgeon)
– 10/31, 11/1-lovenox-one shot- 2x/day
– Restart coumadin 10/31-normal dose
– INR 11/2
• Procedure:
Excision 5cm soft tissue mass of the superior neck (superficial), excision, 3 cm soft tissue mass of the inferior neck (deep)
• POD 7 complains about chest bruise.
Why? • Bridging does not reduce cardioembolic stroke
risk in AF patients

HAVE to Bridge? Thrombosis risk
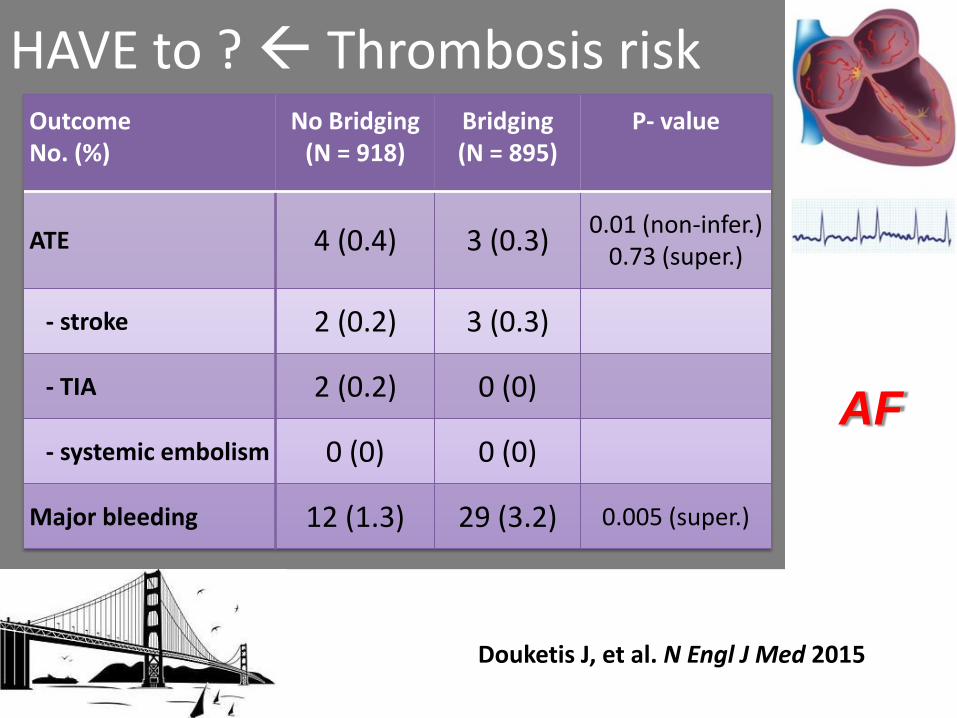
• 1 RCT of no bridging vs. bridging (BRIDGE trial)
– non-inferior for outcome of ATE: 0.4% vs. 0.3%
– superior for outcome of major bleeding: 1.3% vs. 3.2%
(17% with prior stroke/TIA, <5% with CHADS2 5-6)
• >10 non-randomized observational studies
– similar finding of low rates of ATE (<0.5%)
– higher rates of major bleeding with bridging (4-7%)
Douketis J, et al. Arch Intern Med 2004 Dunn AS, et al. J Thromb Haemost 2006 Kovacs MJ, et al. Circulation 2004 Douketis J, et al. Thromb Haemost 2004 Spyropoulos A, et al. J Thromb Haemost 2006 Schulman S, et al. J Thromb Haemost 2014 Douketis J, et al. N Engl J Med 2015
AF
HAVE to ? Thrombosis risk
Douketis J, et al. N Engl J Med 2015
Outcome No. (%)
No Bridging (N = 918)
Bridging (N = 895)
P- value
ATE 4 (0.4) 3 (0.3) 0.01 (non-infer.)
0.73 (super.)
- stroke 2 (0.2) 3 (0.3)
- TIA 2 (0.2) 0 (0)
- systemic embolism 0 (0) 0 (0)
Major bleeding 12 (1.3) 29 (3.2) 0.005 (super.)
AF

Why? • Bridging does not reduce cardioembolic stroke
risk in AF patients
How? • Consider CHADS2 / Dual indication
– stratification
What? • Restricted bridging for Atrial Fibrillation patients

Passaglia LG, et al . JTH. 2015;13(9):1557-67.
HAVE to ? Thrombosis risk • No definitive Answer.
• Waiting for PERIOP 1
– No bridging in AVR Bileaflet
– Meta-analysis specific to 23 studies (n 9,534)
Thromboembolic event rate > if no bridging
(2.1% vs 1.1%, p=0.035)
BUT
Early (<48h) versus late (>48h)
Not statistically different.
MHV
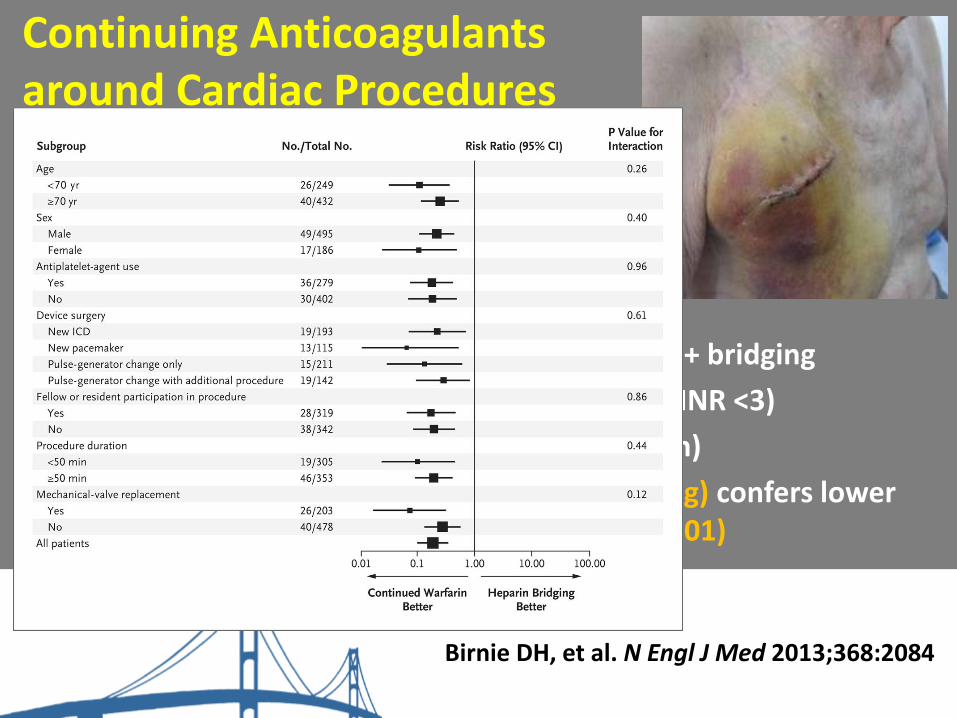
Continuing Anticoagulants around Cardiac Procedures
• Cardiac procedures
– pacemaker/ICD implantation
– AV node ablation
• RCTs: continuing VKA or DOAC vs. interruption + bridging
– BRUISECONTROL-1 (VKA continuation with INR <3)
– BRUISECONTROL-2 (dabigatran continuation)
– VKA continuation (vs. interruption + bridging) confers lower risk for pocket hematoma (3.5 vs. 16%; P<0.01)
Birnie DH, et al. N Engl J Med 2013;368:2084
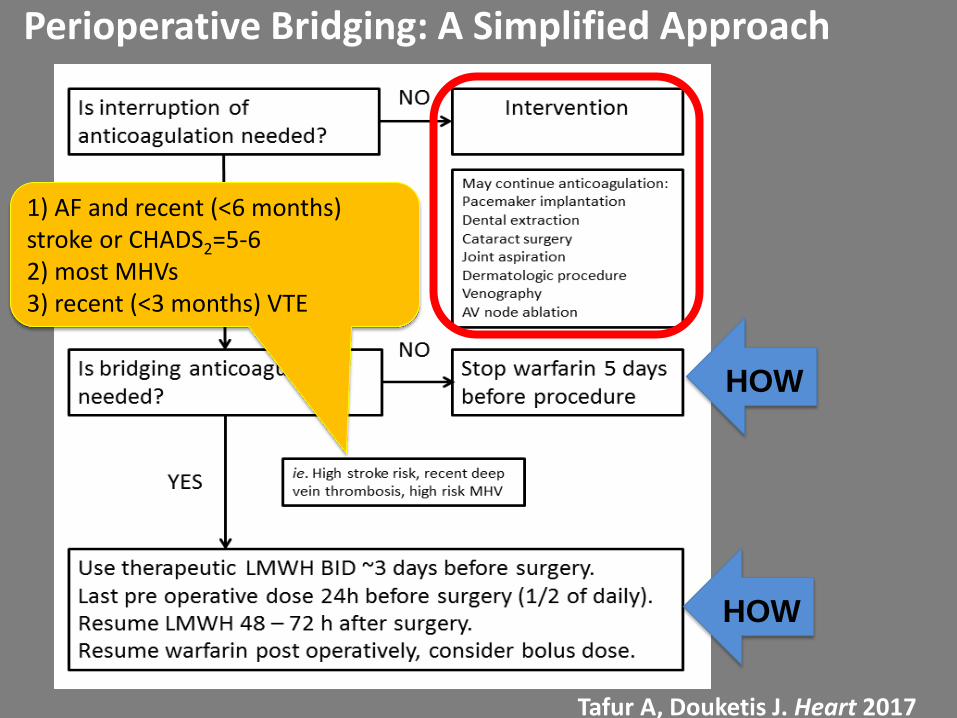
Perioperative Bridging: A Simplified Approach
Tafur A, Douketis J. Heart 2017
1) AF and recent (<6 months) stroke or CHADS2=5-6 2) most MHVs 3) recent (<3 months) VTE
HOW
HOW
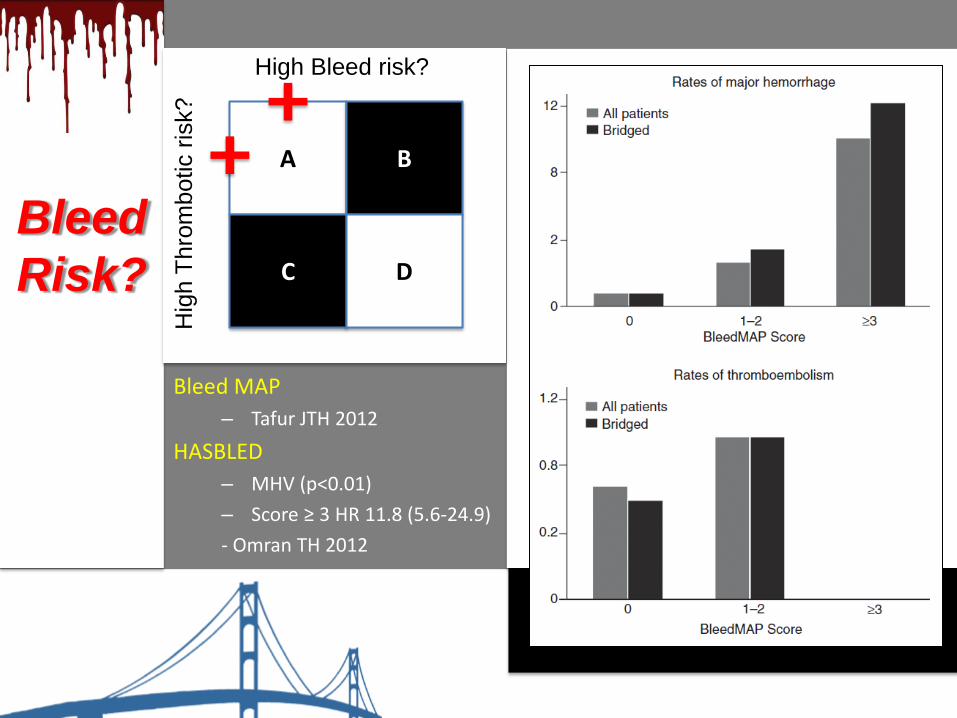
Bleed MAP
– Tafur JTH 2012
HASBLED
– MHV (p<0.01)
– Score ≥ 3 HR 11.8 (5.6-24.9)
- Omran TH 2012
Bleed
Risk?
A B
C D
High Bleed risk?
Hig
h T
hro
mbotic r
isk?

• 75-year, 65-kg old female with AF on apixaban, 5
mg BID
– hypertension, diabetes, TIA 10 years ago
(CHADS2 = 5)
– CrCl = 50 mL/min
• Scheduled for elective colon resection Monday 9AM, for incidentally found colon cancer…
Case 3

• “We recommend a 5 half-life interval between discontinuation of a NOAC and a medium- to high-risk procedure.”
• “If the risk of VTE is high, we recommend LMWH bridging during the stoppage of the NOAC with the LMWH discontinued 24 hours before the procedure.”
• “We could not provide strength and grading of recommendations as there are not enough well-designed studies concerning interventional pain procedures to support such grading.”
Narouze S, et al. Reg Anesth Pain Med 2015
2015 ASRA/ESRA Guidelines on Periprocedure DOAC Management
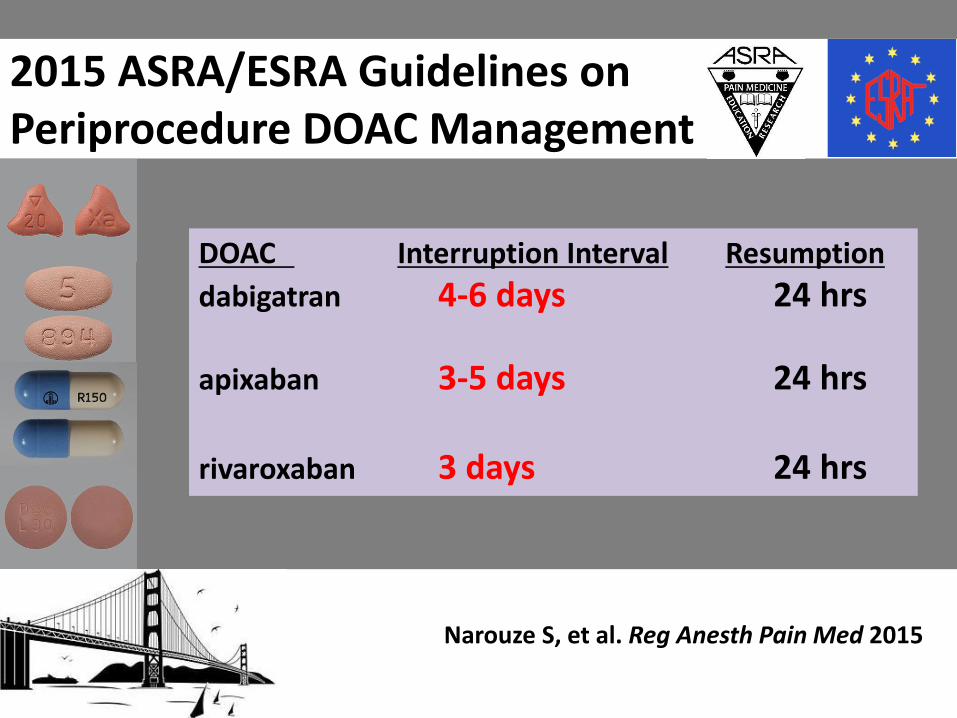
DOAC Interruption Interval Resumption
dabigatran 4-6 days 24 hrs
apixaban 3-5 days 24 hrs rivaroxaban 3 days 24 hrs
Narouze S, et al. Reg Anesth Pain Med 2015
2015 ASRA/ESRA Guidelines on Periprocedure DOAC Management

Why? • The t ½ of DOACs is short but renally modified

Is bridging needed during DOAC interruption?
• No RCTs of bridging vs. no bridging
• Sub-studies of AF RCTs (dabigatran, rivaroxaban, apixaban) looked at patients who had treatment interruption for procedures, but…
– bridging or no bridging NOT randomly allocated
– bridging regimen NOT standardized
– blinding to anticoagulant (warfarin or DOAC)
Douketis J, et al. Thromb Haemost 2014 Garcia D, et al. Blood 2014 Sherwood M, et al. Circulation 2015 Douketis J, et al. JACC 2015 (asbtract)
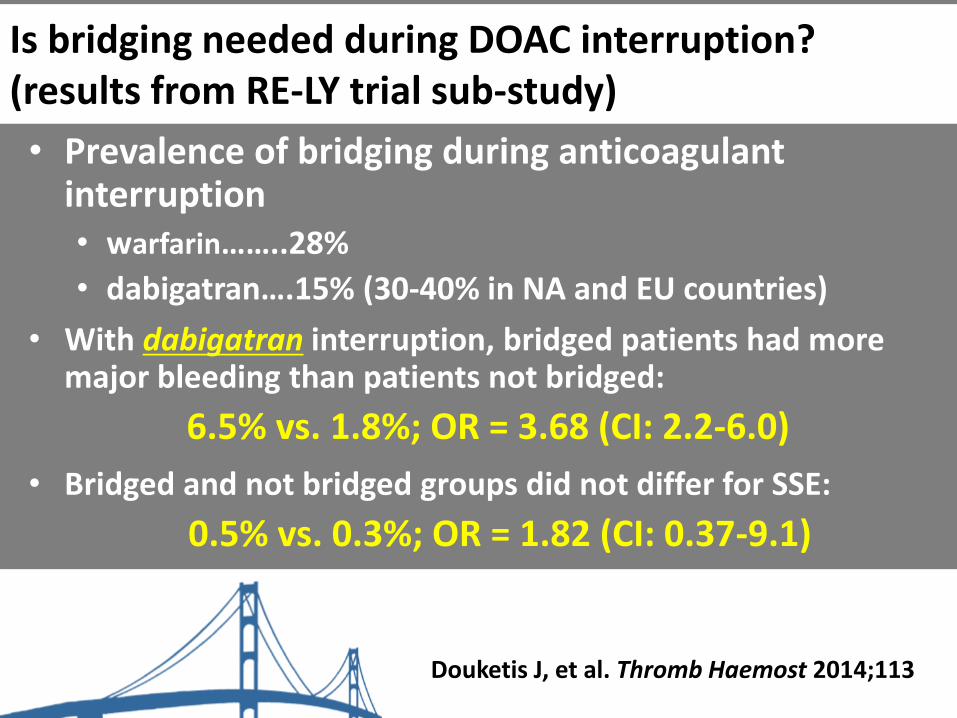
Is bridging needed during DOAC interruption? (results from RE-LY trial sub-study)
• Prevalence of bridging during anticoagulant interruption • warfarin……..28%
• dabigatran….15% (30-40% in NA and EU countries)
• With dabigatran interruption, bridged patients had more major bleeding than patients not bridged:
6.5% vs. 1.8%; OR = 3.68 (CI: 2.2-6.0)
• Bridged and not bridged groups did not differ for SSE:
0.5% vs. 0.3%; OR = 1.82 (CI: 0.37-9.1)
Douketis J, et al. Thromb Haemost 2014;113

Tafur A, Douketis J.
Heart 2017
Douketis J, et al
Thromb Haemost 2017

High-bleed risk surgery/procedure
When to interrupt apixaban?
TIME Thursday Friday Saturday Sunday Monday 9 AM
8 AM
Ø
6 PM
Ø Ø
Ø
Low-bleed risk surgery/procedure
24h 48h 62h
apixaban half-life = 9-12 hrs, 25% renal clearance
Why? • The t ½ of DOACs is short but renally modified
How? • Update pre op CrCl
What? • No bridging. 5 t ½ interruption

PAUSE Study (NCT02228798)
Aim: To establish a safe, standardized protocol for the perioperative management of patients with AF who are taking a DOAC and need an elective surgery/procedure.
Design: Multi-centre prospective cohort study
Patients: 3,300 patients with AF (1,100 per DOAC)
DOAC interruption interval: 4-5 half-lives (3-6% residual anticoagulant effect)

…a word of caution if NOT stopping DOAC
• 1-3 hrs
Frost C, etal. Clin Pharmacol 2014;6:179
Avoid peak
during
procedure
Delay dose until
2-4 hrs post-
procedure

• 70 y/o Indian Male
• 06/16 presenting STEMI, DES x2 to RCA, LAD disease with planned stenting in 2 weeks
• 06/23 Found to have renal mass
• 06/27 LAD stented
Case 4

• 06/30 ASA and Plavix stopped as advised by surgical scheduler
• 07/02 Developed chest pain, anterolateral ST elevation, ER asystole

Primary endpoint, by Kaplan-Meier method
No. at Risk
E-ZES +3-month
DAPT 1059 1049 1037 1027 45
Standard therapy 1058 1046 1032 1024 920
* Primary end-point; A composite of death from CV cause, MI, stent thrombosis, TVR or bleeding at 1 year
Primary endpoint
Months after the index procedure
Cu
mu
lative
in
cid
en
ce
(%
)
0 6 12
0.0
00.0
10
.02
0.0
30
.04
0.0
50
.06
0.0
70
.08
0
2
8
6
4
Cu
mu
lati
ve
eve
nt
rate
(%
)
0 6 12
Standard therapy
E-ZES + 3-month DAPT
4.7%
p-value for non-inferiority < 0.01
Months
Difference = 0.0%
95% CI, -2.5 to 2.5; p = 0.84
4.7%

Primary Endpoint: NACCE at 1 Year (All-Cause Death, MI, Stroke, Major Bleeding)
Month 0 1 3 6 12
No. at risk 1563 1520 1504 1468 1384
No. events 18 25 11 18 21
No. at risk 1556 1514 1497 1466 1381
No. events 16 25 11 16 22
Log-Rank P = 0.84
HR 1.03 (0.77 – 1.38)
Cu
mu
lati
ve
In
cid
en
ce
of
NA
CC
E (
%)
Time After Initial Procedure (Months)
0 12
0
10
15
5
3 6 9
6.0 5.8
12M DAPT
3M DAPT
Non-inferiority
P-value = 0.002

From: Lack of association between dual antiplatelet therapy use and stent thrombosis between 1 and 12
months following resolute zotarolimus-eluting stent implantation Eur Heart J. 2014;35(29):1949-1956. doi:10.1093/eurheartj/ehu026
Eur Heart J | Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2014. For permissions
please email: [email protected]

From: Lack of association between dual antiplatelet therapy use and stent thrombosis between 1 and 12
months following resolute zotarolimus-eluting stent implantation Eur Heart J. 2014;35(29):1949-1956. doi:10.1093/eurheartj/ehu026
Eur Heart J | Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2014. For permissions
please email: [email protected]

Scope of the problem
Why and What
Available resources
Cases
Propositions to improve patient care

• Mandatory discussion with cardiology if stent within 12 months.
• Consideration of discussion for all cardiac stents if on any antiplatelets.

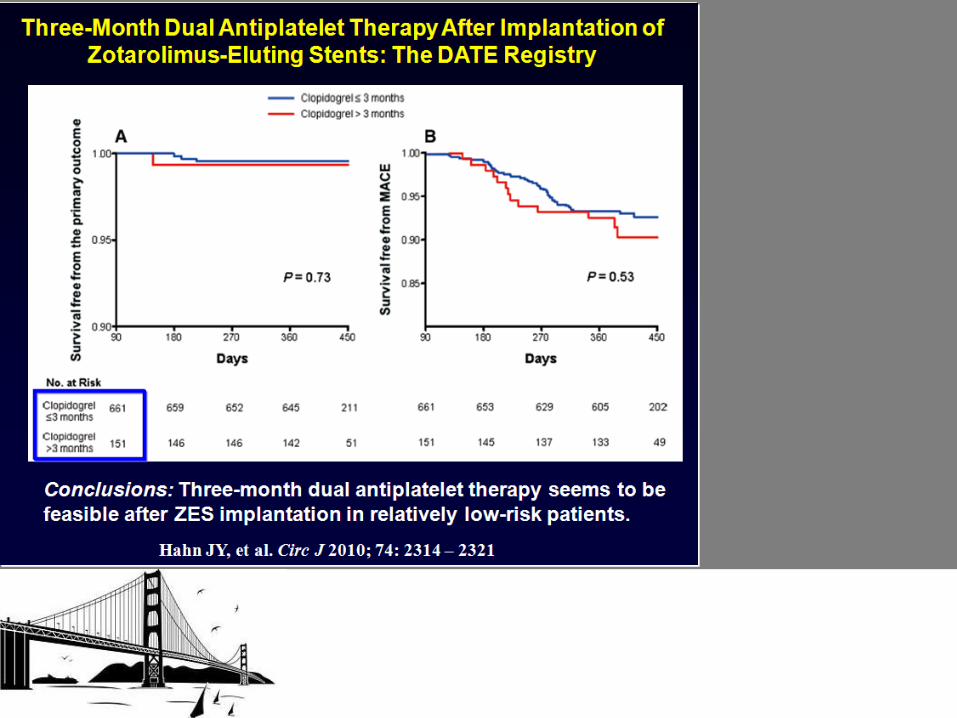
• One-year outcome of a prospective trial stopping dual antiplatelet therapy at 3 months after everolimus-eluting cobalt-chromium stent implantation:
ShortT and OPtimal duration of Dual AntiPlatelet Therapy after everolimus-eluting cobalt-chromium stent (STOPDAPT) trial.

• At the time an order is placed for a procedure, Epic will flag a patient who is on any anticoagulant or antiplatelet agent other than aspirin
– This needs to be done when a procedure is ordered, NOT when they show up in holding day of surgery.
– This needs to be pervasive.
• OR
• GI lab
• Cath lab
• Other sites and these need to be included in the policy we create.
– These include for anticoagulants warfarin, apixaban, rivaroxaban, dabigatran, edoxaban, and betrixaban.

For antiplatelets clopidogrel, ticagrelor, and prasugrel.
I question if EPIC should bear the responsibility or if it should be the
patient
At least 1/3 of patients seen in the outpatient setting do not have a
correct medication profile.
Patients with non-EPIC providers rarely ever have a correct
medication profile. For both of these patients EPIC as the responsible
notifier will fail.
If we put this responsibility on the patient they need to be provided a
list of the above agents, and I would recommend a written response
from the patient prior to procedure either stating that they are or are
not on it. A verbal no will lead to errors as well with no proper
documentation of this.
Perhaps using both EPIC and patient responses will yield the most
accurate response.

• This should be expanded to all higher risk surgical
patients.
– It may be best to start with anticoagulants and antiplatelets, assess
its success and then role out to others.
– We would need to know the most common reasons for late
cancellation of surgery.
• Failure of being NPO
• Markedly elevated glucose
• Markedly abnormal labs
– CBC
– BMG
– There will likely be a large overlap amongst these patients
• There needs to be a consistent responsible party in each area to decide how to
handle these patients.
– Primary care physician – I do not think there is an adequate consistent fund of
knowledge and also to consider would be delays in communication
– Anesthesia – This would be possible but would be a good amount of added
work by them
– Surgery – Once again possible but also a lot of added work.
– Surgery scheduling – I think this would be the best option
• Not all sites that schedule procedures have the same personnel
– Some utilize an APN or RN, others use a PSA
– There needs to be adequate knowledge by these people to be able to
identify the correct people to speak to, ie:
» Cardiologist for antiplatelets after stent or valve
» Neurologist if on anticoagulant for stroke, or cardiologist for valve
» Vascular or hematology for anticoagulant use due to pulmonary
embolus or DVT.
• This contact point must be where the already approved guidelines are known
and discussed with the ordering physician
– Less than half of the ordering physicians are aware of the various time
period of holding for various types of procedures.
– They need to be asked if it would be safe or in the patient’s best interest to
hold xxx drug for xxx days for xxx procedure.
– If there is a conflict there needs to be communication between the 2
physicians or physician representative.

• Also to be considered is these drugs are often held inappropriately. Current
recommendations for many procedures do not support holding these agents.
– That is a very patient specific decision
• The primary operator should have the first decision as to whether or not
holding it is necessary, if not there is no need to go down the flowsheet.
• The physician responsible for ordering the drug needs to have an
opinion as to whether or not it is safe to hold
– Anticoagulant within 6 weeks of large pulmonary embolus.
– Antiplatelet within 1, 6, or 12 months of stenting.
• These guidelines have been developed with a multidisciplinary team at Northshore, pharmacy will assist in ensuring the proper guidelines are updated on a routine manner and distributed to the appropriate personnel.

Anticoagulation per Cards
or Vascular or Curbside
phone call
TIME
Generic Pre op instructions
SECURITY
PCP Pre op 1stS
Stop
2nd Stop
2018
3rd Stop
2020
Lorem ipsum dolor sit amet, consectetuer adipiscing elit. Aenean commodo ligula eget
Lorem ipsum dolor sit amet, consectetuer
adipiscing elit. Aenean commodo ligula eget
Elective Surgery
What Happens now
Surgery

TIME
Pre op Clinic 1stS
Stop
2018 Lorem ipsum dolor sit
amet, consectetuer adipiscing elit. Aenean
commodo ligula eget
Elective Surgery
Mayo Clinic, Cleveland Clinic Model
Surgery
Thrombophilia Clinic.
Written instructions provided
2nd Stop

Potential Alternative
Unify Internal consensus
Elective
Surgery
Telemedicine Pre Op
Thrombophilia Clinic.
Written instructions provided

Potential Alternative
Unify Internal consensus
Elective
Surgery
Telemedicine Pre Op
Thrombophilia Clinic.
Written instructions provided
Cards Pre Op
Anesthesia
Research

What next ?







