Fetal Alcohol Spectrum Disorders
Your Name* Your Institution
Your Contact InformationDate
*in collaboration with the Southeastern Fetal Alcohol Syndrome Regional Training Center, supported by the U.S. Department of Health
and Human Services, Centers for Disease Control and Prevention

2
What non-prescription drug of abuse is most damaging to fetal brain development?
Of all the substances of abuse (including cocaine, heroin and marijuana), alcohol produces by far the most serious neurobehavioral effects in the fetus.
Institute of Medicine, Report on Fetal Alcohol Syndrome Diagnosis, Epidemiology, Prevention and Treatment, 1996.

3
Objectives
1. Need for a Clear Message about Alcohol Use in Pregnancy
2. Fetal Alcohol Spectrum Disorders (FASDs)
3. Fetal Alcohol Syndrome (FAS)
4. Intervention for Persons with FASDs
5. Prevention– Alcohol Screening – Brief Intervention
6. Resources

4
FASDs Current Health Context• 1973: FAS initially described in American
medical literature
• 1981: US Surgeon General issues an advisory about harmful effects of alcohol in PG
• FAS often undiagnosed
• Prevention opportunities frequently missed
• 2002: Congress directed CDC to develop advice to prevent, diagnose and refer for FAS

5
What Every Woman Should Know About Alcohol and Pregnancy
hen a pregnant woman drinks alcohol, so does her unborn baby. Read the 5 things every woman should know about drinking alcohol during
pregnancy.
When a pregnant woman drinks alcohol, so does her unborn baby. Read the 5 things every woman should know about drinking alcohol during pregnancy.
www.cdc.gov/Features/AlcoholFreePregnancy
6
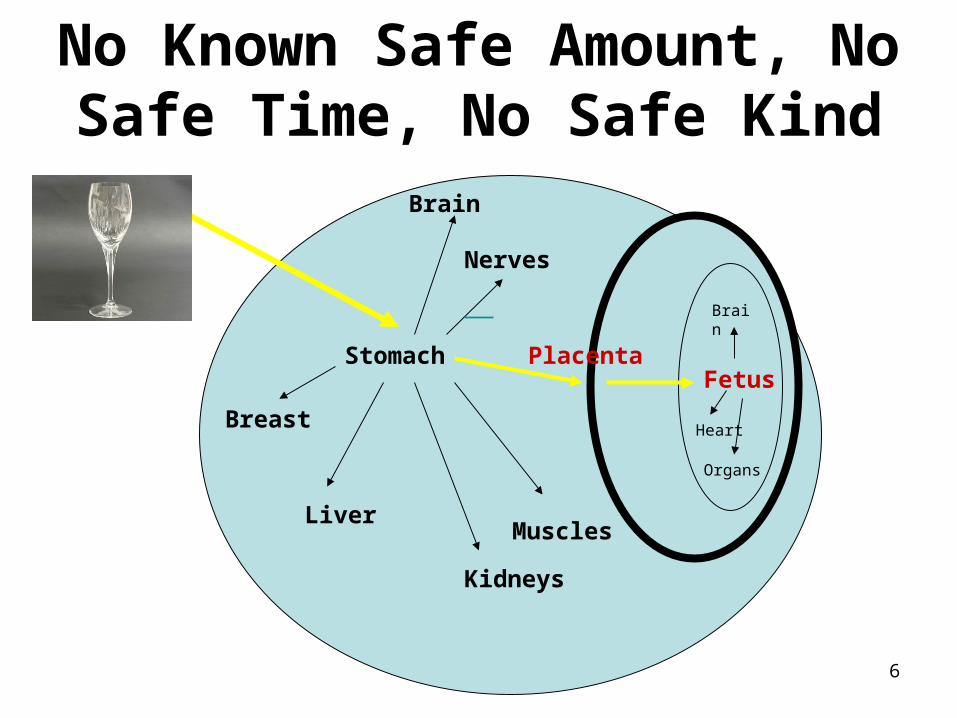
Stomach
Brain
Liver
Kidneys
Fetus
Muscles
Nerves
Placenta
Brain
Heart
Organs
Breast
No Known Safe Amount, No Safe Time, No Safe Kind

7
What are Fetal Alcohol Spectrum Disorders?
• Range of effects that can occur in a person whose mother drank alcohol during pregnancy
• Physical• Mental, Learning Disabilities• Behavioral
• Includes both persons with diagnosable FAS, and persons with other identifiable effects due to fetal alcohol exposure
• FASD is not a DiagnosisBertrand J, Floyd RL, Weber MK. Guidelines for Identifying and Referring Persons with Fetal Alcohol Syndrome. Morbidity and Mortality Weekly Review. October 28, 2005 / 54;1-10.

9
Figure 2. Percentages of Past Month Alcohol Use among Women Aged 15 to 44, by Pregnancy Status: 2002 and 2003
Percentages of Past Month Alcohol Use among Women Aged 15 to 44, by Pregnancy
Status: 2002 and 2003
Binge drinking defined as 5 or more drinks on one or more occasions in the last 30 days. Heavy alcohol use defined as 5 or more drinks on 5 or more occasions in last 30 days.-National Survey on Drug Use and Health. The NSDUH Report.Substance Use During Pregnancy: 2002 and 2003 Update. June2, 2005 (SAMHSA).

10
344.1
2.9
24.7
9.1
18.618.7
26.1
23.2
35.1
0
5
10
15
20
25
30
35
40
Total White Black Hispanic AmericanIndian
Asian Morethan 1race
Perc
enta
ge
PregnantNot Pregnant
Females Aged 15-44 Years Reporting Past Month Binge Alcohol Use, by Race/Ethnicity and Pregnancy Status, 2002 and 2003 Combined
Binge = drinking 5 or more drinks on the same occasion on at least 1 day in the past 30 days. Substance Abuse and Mental Health Services Administration, National Survey on Drug Use and Health, 2005.
11
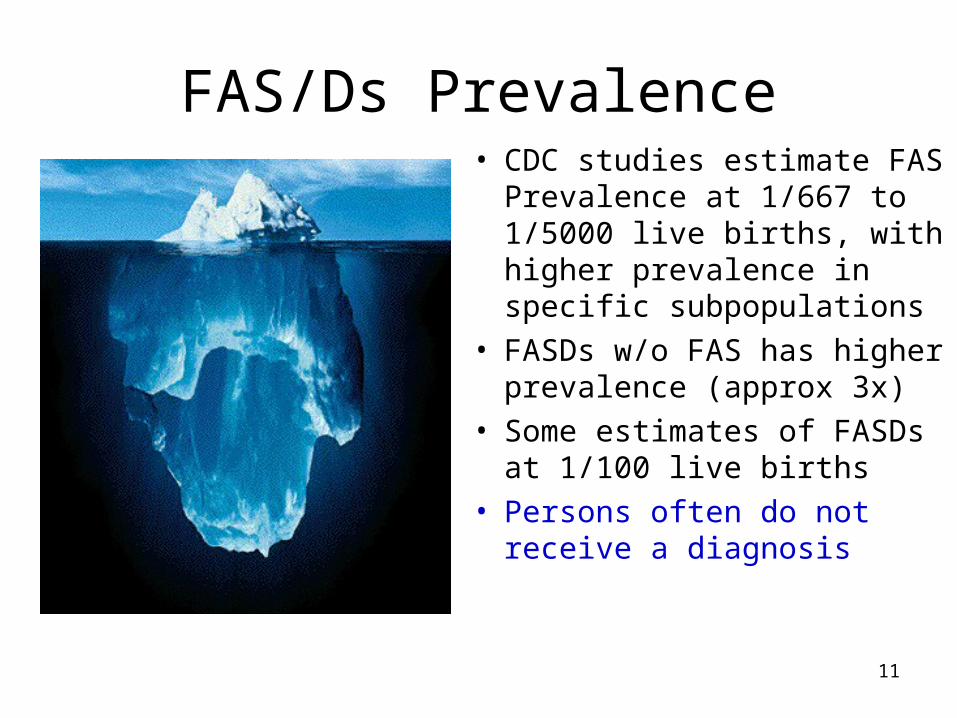
FAS/Ds Prevalence• CDC studies estimate FAS
Prevalence at 1/667 to 1/5000 live births, with higher prevalence in specific subpopulations
• FASDs w/o FAS has higher prevalence (approx 3x)
• Some estimates of FASDs at 1/100 live births
• Persons often do not receive a diagnosis

12
Diagnostic Criteria for Diagnostic Criteria for Fetal Alcohol SyndromeFetal Alcohol Syndrome
With or w/o confirmed maternal alcohol exposure
1. Documented facial abnormalities (all 3)1. Smooth philtrum
2. Thin vermillion
3. Small palpebral fissures
2. Documented Growth Deficits
3. Documented CNS abnormality (any of 3 types)

13
1.1. Facial Abnormalities Facial Abnormalities of FASof FAS
1. Smooth philtrum
2. Thin vermillion
3. Small palpebral fissures
Photo courtesy of Teresa Kellerman
Lip Philtrum GuidesUsed for Objective Measurements

14
2. 2. Growth Deficiency of FASGrowth Deficiency of FAS
Documented Height and/or Weight at ≤ 10%Documented Height and/or Weight at ≤ 10%• at any one point pre- or postnatally at any one point pre- or postnatally • adjusted for age, sex, gestational age, race, ethnicityadjusted for age, sex, gestational age, race, ethnicity

15
Growth DeficiencyGrowth Deficiency

16
3. CNS Abnormalities of FAS3. CNS Abnormalities of FASDocumentation of any of the following
1. Structural Abnormality1. Head circum ≤ 10%’ (adj for age, sex)
2. Clin significant brain abnormality via imaging
2. Neurological Damage1. i.e. seizure or motor control
3. Functional Deficits1. Young child: significant developmental delay
2. Global cognitive deficits (i.e., ↓IQ, below 3%’)
3. Below 16%’ in 3+ domains – cognitive; executive functioning; attention/hyperactivity; social skills, other

17
Brain Damage Resulting From Brain Damage Resulting From Prenatal AlcoholPrenatal Alcohol
photo: Clarren, 1986
Alcohol-Affected Brain vs Normal Brain

18
How are Children with FASDs Affected?• FAS: IQ avg 60, range
20-110• Poor Judgment• Problems with
– Behavior– Social Interactions– Motor Skills
• May have Physical Abnormalities
What future lies ahead?
19
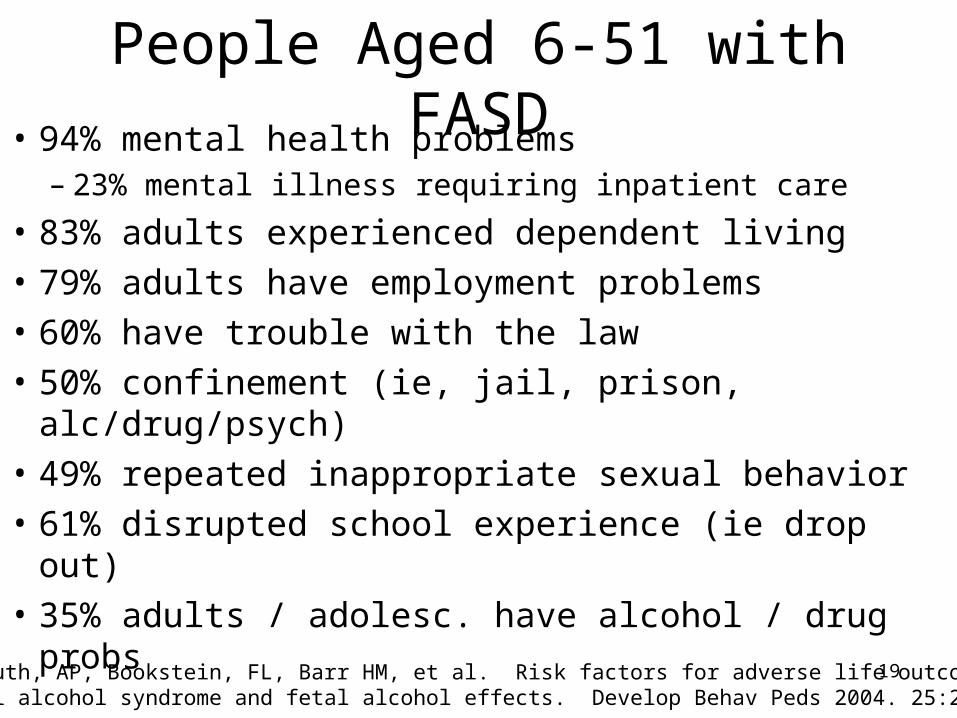
People Aged 6-51 with FASD• 94% mental health problems
– 23% mental illness requiring inpatient care
• 83% adults experienced dependent living
• 79% adults have employment problems
• 60% have trouble with the law
• 50% confinement (ie, jail, prison, alc/drug/psych)
• 49% repeated inappropriate sexual behavior
• 61% disrupted school experience (ie drop out)
• 35% adults / adolesc. have alcohol / drug probsStreissguth, AP, Bookstein, FL, Barr HM, et al. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. Develop Behav Peds 2004. 25:228-238.

20
Identifying FASDs Helps
• Early intervention is critical
• Protective factors include:– Stable and nurturing home environment– Early diagnosis (before age 6)– Absence of exposure to violence– Few changes in caretaking placements– Eligibility for social and educational services
Streissguth AP, Bookstein FL, Barr HM, Sampson PD, O'Malley K, Young JK. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J Dev Behav Pediatr. 2004 Aug;25(4):228-38.
21
Case Management across the Lifespan
• Medical and health care• Early intervention and education• Proactive mental health services• Increased supervision throughout adolescence
and early adulthood• Proactive preparation for adulthood• Juvenile justice and corrections assistance• Plan for supported living and employment
Alcohol Assessment and Intervention in 1ry Care
Ask, Assess, Advise and Assist

23
Alcohol Assessment: Know What a Standard Drink IsAn equivalent of 0.6 oz of absolute alcohol• 12 oz. of beer• 8 oz. malt liquor • 5 oz. of wine• 4 oz. sherry• 1 ½ oz. of liquor
Patients may minimize or underestimate their drinking levels; seek rapport and trust

24
Women’s Alcohol Risk
• Abstinence• Low Risk: ≤7 drinks/week and ≤3
drinks/occasion• At-Risk: 8-21 drinks/week or >3 drinks/
occasion, or in high-risk situations• Problem Drinker: >21 drinks/week, may
experience negative consequences• Alcohol-Dependent: Heavy drinking and
physical dependence, with neg. consequences

25
Recommended Alcohol Limit During Pregnancy and
Preconception
“I’m a mother to be,
NO DRINKS FOR ME!”

26
Alcohol Assessment: Frequency and Quantity
First ask: Do you drink alcohol of any kind, such as beer, wine or liquor?
• On average, how many days per week do you drink alcohol?
• On a typical day when you drink, how many drinks do you have?
• What’s the maximum number of drinks you had on a given occasion in the last month?

27
TWEAK Alcohol Assessment
• Developed originally to screen for at-risk drinking during pregnancy
• Five-item scale
• Shown effective in pregnant women and African-American women of low socio-economic status

28
“TWEAK”• T-Tolerance: "How many drinks does it take you to feel
the first effects of the alcohol?" • W-Worry: "Have close friends or relatives Worried or
complained about your drinking in the past year?" • E-Eye-openers: "Do you sometimes take a drink in the
morning when you first get up?" • A-Amnesia (blackouts); "Has a friend or family member
ever told you about things you said or did while you were drinking that you could not remember?"
• K(C)-Cut Down: "Do you sometimes feel the need to Cut Down on your drinking?"

29
Tweak Scoring• Tolerance: 3 or more drinks to feel effect = 2 points• Worry: Yes = 2 points• Eye Opener: Yes = 1 point• Amnesia: Yes = 1 point• Cut Down: Yes = 1 point
• A score of >0 indicates at-risk during pregnancy• For others, a score of 2 indicates likelihood of at-risk drinking; • A score of 3-4 or more indicates problem drinking or alcoholism
Chang G. Alcohol Screening Instruments for Pregant Women. Alcohol Research and Health. 2001;25(3):204-209.
30
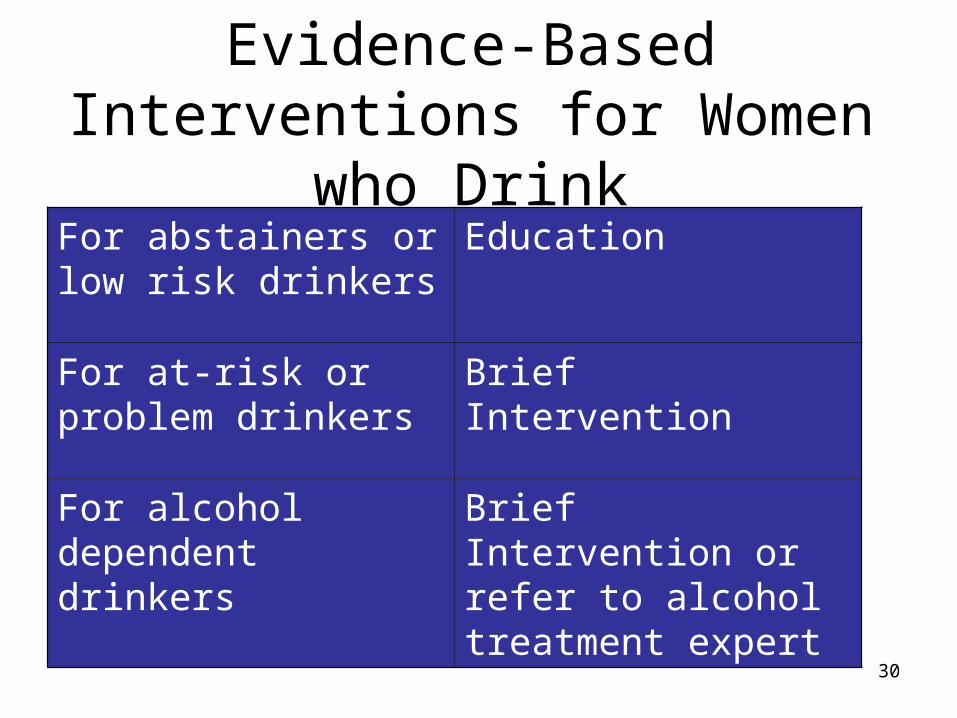
Evidence-Based Interventions for Women
who DrinkFor abstainers or low risk drinkers
Education
For at-risk or problem drinkers
Brief Intervention
For alcohol dependent drinkers
Brief Intervention or refer to alcohol treatment expert

31
Brief Intervention Counseling
• Found to be effective with women problem drinkers in primary-care clinics
• 5-10 minute counseling session has been found to reduce alcohol use in women by 20-30%
• … is not difficult
32
Brief Intervention: Ask and Assess Risk Level
1. Raise the subject: Alcohol Assessment Test“I like to ask all my patients about their drinking patterns”
2. Does the patient have alcohol-related problems? (Medical, behavioral, social, familial)
3. Provide feedback about alcohol risk level: Relate health concerns / pregnancy risks to alcohol use
“I am very concerned about how your drinking may affect your health”
“There is no known safe limit for drinking during pregnancy. It is important for you to stop drinking completely b/c when you drink, your baby drinks.”

33
Brief Intervention: Advise and Assist
4. Engage the patient in the process: Assess, enhance motivation and patient responsibility
“How do you feel about your drinking?”
5. For alcohol-risk, establish drinking goals: Advise and negotiate cut down “Are you ready to set a drinking goal? What do you think will work best for you?” (give brochure materials)
For alcohol dependence, advise abstinence and refer to specialized treatment.
6. Follow up: review progress, commend effort, reinforce positive change, reassess motivation
National Institute on Alcohol Abuse and Alcoholism and Office of Research on Minority Health, Identification of At-Risk Drinking and Intervention with Women of Childbearing Age. NIH Publication No. 99-4368 (Printed 1999).

34
Sending a Clear Message• Alcohol can hurt a fetus for
life• Women need education,
motivational counseling, some need treatment [Blame is counter-productive]
• Early ID and Dx for FASDs• FASDs are 100% preventable• “I’m a mother to be, NO
DRINKS FOR ME!”

35
Adopting Prevention and Intervention Practices
It may seem difficult
to talk with patients about FASDs,
but you can do it.

36
Information and Treatment Resources
• Southeastern Regional FASD Training Center
Tel: 615 327-5525 Web: http://www.fasdsoutheast.org
• University of Louisville Weisskopf Child Evaluation Center; Tel: 502 852-3020
• NOFAS (National Organization on FAS)
Tel: 202-785-4585 Web: www.nofas.org• Local Alcohol and Drug Treatment Resources:
Web: http://findtreatment.samhsa.gov• CDC FAS Home Page:
http://www.cdc.gov/ncbddd/fas







