
Identifying Risk to Improve Safety:
The Keys to Conducting a Successful
Failure Modes and Effects Analysis
(FMEA)
Alex Jenkins, PharmD, MS
Medication Safety Officer
Department of Pharmacy
WakeMed Heath & Hospitals
Raleigh, NC

Raleigh, North Carolina
WakeMed Health & Hospitals
WakeMed Health & Hospitals The Power to Heal. A Passion for Care.
Disclosures
Neither I nor any member of my immediate
family has a financial relationship or interest
with an proprietary entity producing health care
goods or services related to the content of this
CE presentation.

Objectives
• Describe the methodology and purpose for conducting
regular FMEA projects in a healthcare organization.
• Summarize the critical role of FMEA as a quality
improvement tool to improve patient safety.
• Demonstrate how the principles of FMEA can be
applied to prevent errors and adverse outcomes with
high alert medications.
Brief History
• Developed for use by the U.S. military
• Adopted by the Joint Commission in 2001
• HFMEA – a risk assessment variation for
healthcare developed by the VA’s National
Center for Patient Safety
Understanding the Terminology F
ME
A Failure – poor, intermittent, or unintended
performance
Mode - the manner in which the failure occurs
Effects – one or more consequences of each anticipated failure
Where is FMEA in the Quality
Spectrum?
Prospective Hazard Analysis
Concurrent Monitoring
(Inspection)
Retrospective Analysis

Where is FMEA in the Quality
Spectrum?
Prospective Hazard Analysis
Concurrent Monitoring
(Inspection)
Retrospective Analysis

Prospective Risk Analysis
• Hazard and Operability Studies (HAZOP)
• The Structured What-if Technique (SWIFT)
• Human Error Assessment and Reduction Technique(HEART)
• Failure Mode and Effects Analysis (FMEA)
• Barrier Analysis
• Influence Diagrams
• Fault Tree Analysis (FTA)
• Event Tree Analysis (ETA)
• Absolute Probability Judgment (APJ)
• Risk Matrices

Types of FMEA
FMEA
System
Design
Process
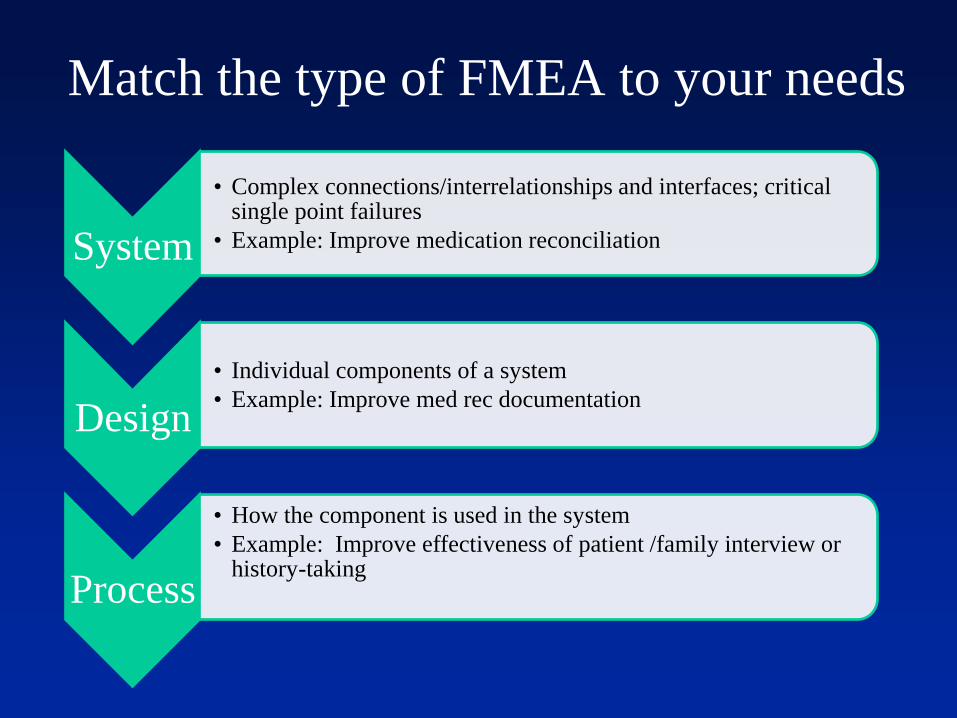
Match the type of FMEA to your needs
System
• Complex connections/interrelationships and interfaces; critical single point failures
• Example: Improve medication reconciliation
Design
• Individual components of a system
• Example: Improve med rec documentation
Process
• How the component is used in the system
• Example: Improve effectiveness of patient /family interview or history-taking
Why do we conduct FMEA?
“Look for
intelligence and
judgment and,
most critically, a
capacity to
anticipate, to see
around corners.”
-Colin Powell

Expected Outcomes
• Design or re-design safer processes or systems
• Reduce risk of sentinel events and medical
errors
• Prioritize highest risk areas
• Make decisions to reduce some risks
• Assign responsibility

FMEA in 8 Steps
Define the Topic
Assemble the Team
Review the Process
Brainstorm Modes, Causes, Effects
Evaluate the Risk of Failure
Calculate the Total RPN Score
Create an Action Plan
Determine Effectiveness of Actions

Benefits
• Full understanding of a process
• Measurable improvements
– Track over time (IHI FMEA Tool)
• Clarifies key risk points
• Improve staff satisfaction
• Regulatory compliance

Top 5 Barriers to Success

Top 5 Barriers to Success
1) Focus on compliance
rather than quality
improvement

Top 5 Barriers to Success
1) Focus on
compliance rather
than quality
improvement
2) Weak/Limited
sponsorship

Top 5 Barriers to Success
1) Focus on compliance
rather than quality
improvement
2) Weak/Limited
sponsorship
3) Scope is too broad

Top 5 Barriers to Success
1) Focus on compliance
rather than quality
improvement
2) Weak/Limited
sponsorship
3) Scope is too broad
4) Focus on fixing rather
than prevention

Top 5 Barriers to Success
1) Focus on compliance
rather than quality
improvement
2) Weak/Limited
sponsorship
3) Scope is too broad
4) Focus on fixing rather
than prevention
5) No value proposition

Key Points
• FMEAs are process and design driven
• Need input from multiple sources
• Healthy blend of knowledge base
– High degree of complexity in medication use
process
– Details can make the difference to the patient
• Communication is key

Application of FMEA
High Risk Medications

High Risk Meds: Opiates
Sentinel Event 49: Safe use of opiates in hospitals
• Pain Committee to develop policies and procedures
• Standards of care for assessing and monitoring pain, sedation, and
respiration
• Pain management specialist
• Process for tracking opiate-related incidents
• Establish red flags and dose limits in e-prescribing systems
• Utilize PCAs and smart pumps whenever possible
• Start with non-opiate pain medications first
• Counsel patients on how to assess pain and provide contact
information

High Risk Meds: Long-Acting Opiates

Duragesic (fentanyl) Patches: Drug Safety Communication -
Packaging Changes to Minimize Risk of Accidental Exposure
ISSUE: FDA is requiring color changes to the writing on Duragesic
(fentanyl) pain patches so they can be seen more easily. FDA continues to
learn of deaths from accidental exposure to fentanyl patches.
Patients and health care professionals are reminded that fentanyl patches
are dangerous even after they’ve been used because they still contain high
amounts of strong narcotic pain medicine. Accidental exposure to these
patches can cause serious harm and death in children, pets, and others.
High Risk Meds: Fentanyl Patch

High Risk Meds: Fentanyl Patch
National Alert Network Alert; April 2012:1-2
Example Case #1
Improving the use of Heparin
Across a Community Health-
System

Improving the Use of Heparin Order set/flowsheet changes
•Physician order updates – Adult Heparin Order Set
and related order sets with heparin embedded
•Heparin flowsheets – separated by indication,
updated and barcoded
Smart Pump changes
•Create ability to program using pweight
•Revise guardrails, remove soft stops for heparin in
appropriate libraries
Pharmacy/MAK changes
•Change out concentration of heparin drips in Pyxis
•Remove heparin drip from Pyxis override list
•Add Pyxis alerts for max doses on heparin boluses
Lab Changes
•Educate lab staff on new aPTT therapeutic ranges
and critical result
Staff Education
•General staff education
•Physician education – in person
•Physician education – poster for
lounges/dictation areas
•Nursing/pharmacy education – mandatory
Learning Link module
•Nursing/pharmacy education – poster
Go-Live
•Instructions for switching out heparin at 10AM
•Identify task force members to help with
heparin switches
•Sweep of nursing units for old flowsheets

Example Case #2
Implementation of Unit-Dose
Syringes in the Pediatric
Population
Step 1: Define the FMEA Topic
• Reduce the Risk of Harm when Preparing and
Administering Weight-Based Unit-Dose, Oral
Pediatric Meds at WakeMed-Raleigh Campus
– Selected to prevent dosing errors in pediatric patients
and to prevent med administration via the incorrect
route for oral medications.
– Steps in the Medication Use Process evaluated:
• Dispensing
• Administering
Step 2: Assemble the Team
• Performance Improvement Director
– Leadership/Executive Sponor
• Physician Advisor
• Nursing
– Pediatrics Nurse Manager
– 3 pediatrics staff nurses
• Pharmacy
– Pharmacy Director
– Pharmacy Supervisor
– Pediatrics Clinical Pharmacist
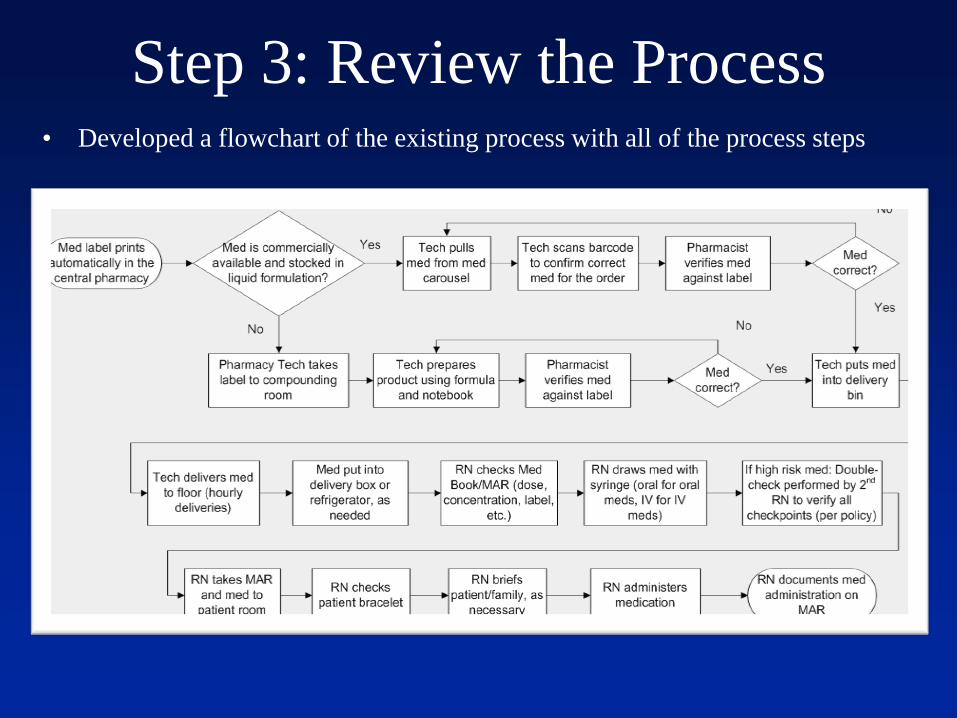
Step 3: Review the Process • Developed a flowchart of the existing process with all of the process steps

Step 4: Brainstorm Potential Failure Modes
• Failure Modes
– What could go wrong or fail at each process step
• Causes
– Why the failure may occur
• Effects
– The result or harm of the failure
• The number of identified failure modes: 28
– Number of identified failure modes scoring above
100: 16

Selected Process Failure Modes
• Incorrect pharmacist verification against label
• Drug delivered to wrong location
• Drug not refrigerated when needed
• Med check not performed on Peds unit
• Physician order incorrect
• Physician order illegible
• RN draws wrong med/dose
• RN administers med to wrong patient d/t not checking
patient bracelet

Failure Points in the Existing Process

Step 5: Evaluate the Risk of Failure • Risk Priority Number (RPN) = Severity x Occurrence Prob x
Detectability
• Severity of an Event
• Probability of the
Failure Mode
• Detectability before
Harm Occurs
• Score each from 1-10
– 10 is least desirable
Failure Mode:
Sev
Prob
Det
RPN
Physician order illegible 10 8 3 240
RN draws wrong med/dose 10 3 5 150
Med check not performed on Peds unit 10 3 5 150
Physician order incorrect 10 5 3 150
RN administers med to wrong patient
d/t not checking patient bracelet 10 2 5 100
Incorrect pharmacist verification
against label 10 2 5 100
Drug delivered to wrong location 3 5 5 75
Drug not refrigerated when needed 5 3 5 75

Step 6: Calculate the Total RPN Score
• Sum of
RPN Scores = 2,554
• Failure Modes – Ordering = 2
– Dispensing = 4
– Administering = 2
Distribution of Scores
RPN Quantity
211-240 1
181-210 0
151-180 0
121-150 5
91-120 10
61-90 4
31-60 3
0-30 5

Step 7: Create an Action Plan
• Identify the failure modes that have an RPN Score of
100 or higher
• Develop and implement actions to address each of
these high-hazard score failure modes
19 items were identified in the Action Plan to
address the previously-identified Failure Modes
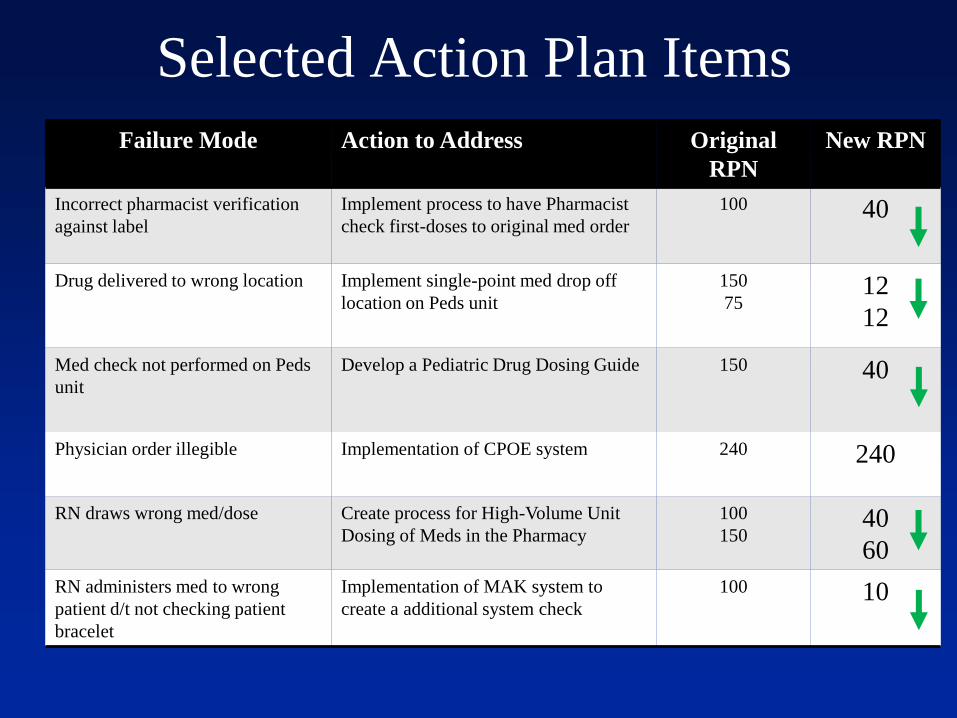
Selected Action Plan Items
Failure Mode Action to Address Original
RPN
New RPN
Incorrect pharmacist verification
against label
Implement process to have Pharmacist
check first-doses to original med order
100 40
Drug delivered to wrong location Implement single-point med drop off
location on Peds unit
150
75 12
12
Med check not performed on Peds
unit
Develop a Pediatric Drug Dosing Guide 150 40
Physician order illegible Implementation of CPOE system 240 240
RN draws wrong med/dose Create process for High-Volume Unit
Dosing of Meds in the Pharmacy
100
150 40
60
RN administers med to wrong
patient d/t not checking patient
bracelet
Implementation of MAK system to
create a additional system check
100 10
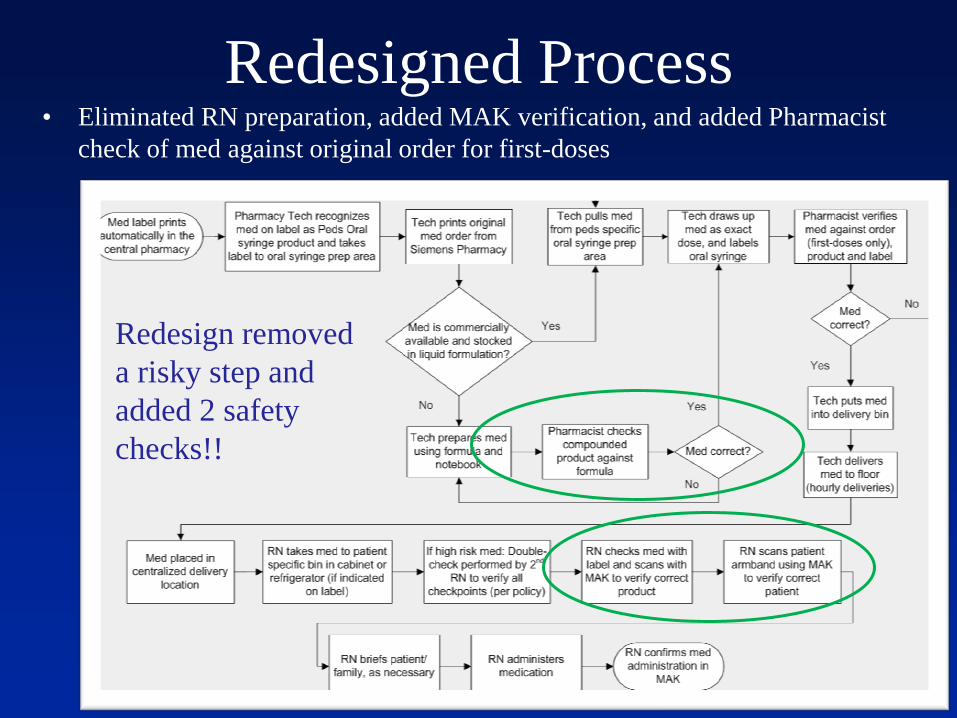
Redesigned Process • Eliminated RN preparation, added MAK verification, and added Pharmacist
check of med against original order for first-doses
Redesign removed
a risky step and
added 2 safety
checks!!
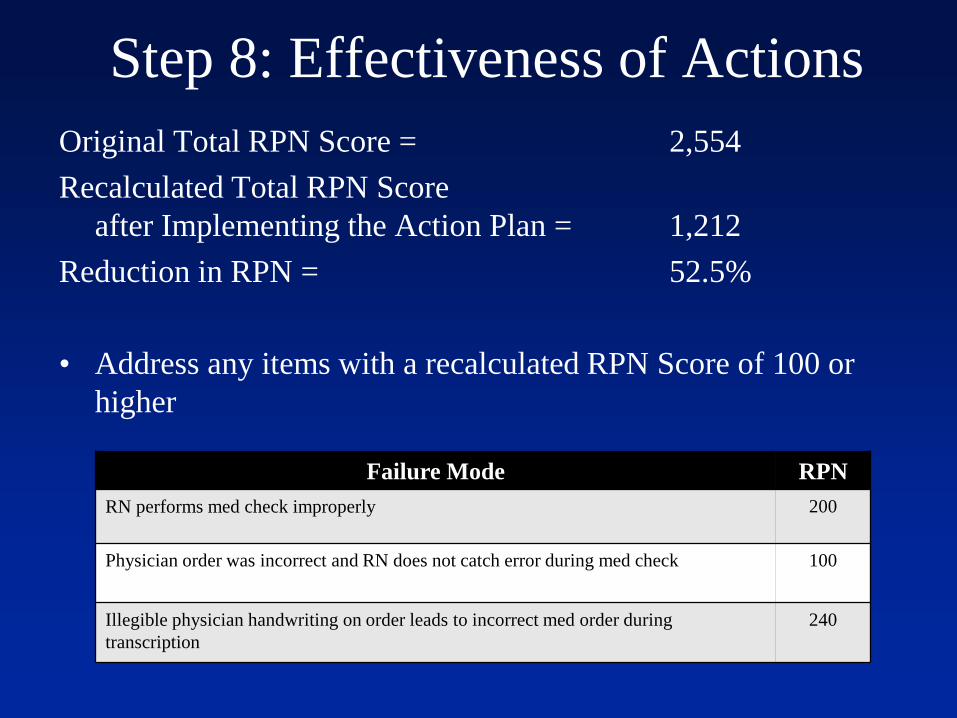
Step 8: Effectiveness of Actions
Original Total RPN Score = 2,554
Recalculated Total RPN Score
after Implementing the Action Plan = 1,212
Reduction in RPN = 52.5%
• Address any items with a recalculated RPN Score of 100 or
higher
Failure Mode RPN
RN performs med check improperly 200
Physician order was incorrect and RN does not catch error during med check 100
Illegible physician handwriting on order leads to incorrect med order during
transcription
240

Actions for Remaining RPNs >= 100
Failure Mode Proposed Risk
Reducing
Action
RN performs med check improperly
- Increased RPN due to implementation of MAK. Increase
results
from reliance on MAK to catch errors and reduced critical
thinking
Physician order was incorrect and RN does not catch error
during
med check
Implement CPOE
Illegible physician handwriting on order leads to incorrect med
order during transcription
Implement CPOE

Practice Case Scenario
Evaluation of Patient-Controlled
Analgesia

Case Description
A 600-bed community hospital has tasked the
Medication Safety Committee with pulling together
a multidisciplinary group to perform an FMEA on
PCA use. Several significant adverse drug events
have been reported that have indicated multiple
failure points exist in the PCA use process.

FMEA Exercise: Opiate Safety
1) Define the Topic
2) Assemble the Team
3) Review the Process
4) Brainstorm Modes, Causes, Effects
5) Evaluate the Risk of Failure
6) Calculate the Total RPN Score
7) Create an Action Plan
8) Determine Effectiveness of Actions
Conclusion • FMEA is a valuable tool that can be used to proactively
identify risk in healthcare organizations as a means of
initiating quality improvement.
• Incorporating FMEA into an organizational
quality/safety plan can help to implement effective
quality improvement changes.
• FMEA methodology can be applied to reduce risk,
prevent errors, and improve the overall safety of high
risk medication use.
Questions?






