
Trent J. Herda, Ph.D.Assistant ProfessorDocking Faculty ScholarNeuromechanics Laboratory – DirectorHawk Fitness Academy ‐ DirectorDept. of Health, Sport and Exercise SciencesUniversity of Kansas
Application of Electromyography in Strength and Conditioning Research
Electromyography in JSCR
• Journal of Strength and Conditioning Research
– Pubmed.com
– Searchable terms (2001 – current):
• electromyography = 371 papers
• EMG = 389 papers– 20 to 30 papers per year

Overview
• EMG hardware
• Motor units
• The EMG signal
• Study Design
• Interpretation
Technical sources:1. Farina et al. 2014 The extraction of neural strategies from the surface EMG: an update. J Appl Physiol 117:1215‐1230.
2. Merletti et al. 2009 Technology and instrumentation for detection and conditioning of the surface electromyographic signal: state of the art. Clin Biomech 24:122‐134.
3. Enoka . 2015. Neuromechanics of Human Movement. 5th Edition. Human Kinetics. Champaign, IL.
4. De Luca. 1993. The use of surface electromyography in biomechanics. Delsys, Inc. Boston, MA.
EMG Acquisition Systems
• BIOPAC Systems
• Delsys
• iWorx
• National Instruments
EMG Electrodes

Motor Units• Motor unit consists of a motor neuron in the ventral horn of the spinal cord or brain stem, its axon, and the muscle fibers it innervates.
1.
Motor Unit Behavior• The force exerted by a muscle during a contraction depends on the following:
– The number of motor neurons that are activated.
– The rates at which they discharge action potentials.
– The force twitches of muscle fibers.
Motor Unit Behavior
• Cyclic dynamic contractions.
2.

EMG Signal
• Represents the electrical activity generated in muscle fibers in response to the activation provided by motor neurons.
– Bipolar (two electrodes) surface EMG contains information from overlapping action potentials from many MUs.
• Source of information: the neural drive to the muscle provided by motor neurons and the electrical properties of the muscle fiber membranes.
– Does not differentiate between MU recruitment and firing rate.
EMG Signal
Surface Bipolar EMG
EMG Decomposition
EMG Signal
2.

EMG Signal• EMG recordings reflect extracellular field potentials.
• Action potential is generated for each muscle fiber of a MU.
3.
EMG Signal
• Bipolar EMG provides information about the timing and intensity of muscle activation.
– EMG decomposition techniques can provide information about the firing characteristics of single MUs.
• Currently, EMG decomposition provides information from only isometric muscle actions.
EMG Signal• Limitations (nonphysiological)
– Amplitude cancellation
4.

• Limitations (nonphysiological)
– Amplitude cancellation• Amplitude cancellation tends to reduce the contribution of individual or groups of MUs.
– Despite a significant reduction in firing rates of lower‐threshold MUs, EMG amplitude remained constant.
EMG Signal
5.
EMG Signal
• Limitations (nonphysiological)
– Subcutaneous fat• Low‐pass filter
6.
7.
3.
EMG Signal
• Limitations (nonphysiological)
– Unwanted signal content
• Bandpass filter is typically applied to the signals.– Sampling frequency should be twice as high as the low‐pass band frequency (500 Hz) to avoid aliasing.
• Notch or band‐stop filter can minimize a specific frequency (60 Hz).
– Cross‐talk
• Influence of neighboring muscle on the EMG signal.
• Double‐differential signal can reduce cross‐talk.

EMG Signal• Limitations (physiological)
– Distribution of conduction velocities.
– Shape of intracellular action potentials.
– Number and discharge rates of MUs.
– Synchronization.
Synchronization
8. 9.
EMG Signal• Amplitude
– Depends on the number of muscle fibers activated.• Not the number of MUs that were recruited.
– Typically reported as a root mean square (RMS).
• There are numerous ways to report amplitude of the EMG signal.
– Need to rectify.
10.
EMG Signal• Amplitude
– Isometric contractions• Linear or a curvilinear relation between the rectified EMG and force.
– Minimal changes in muscle length and when force is held constant.
11.
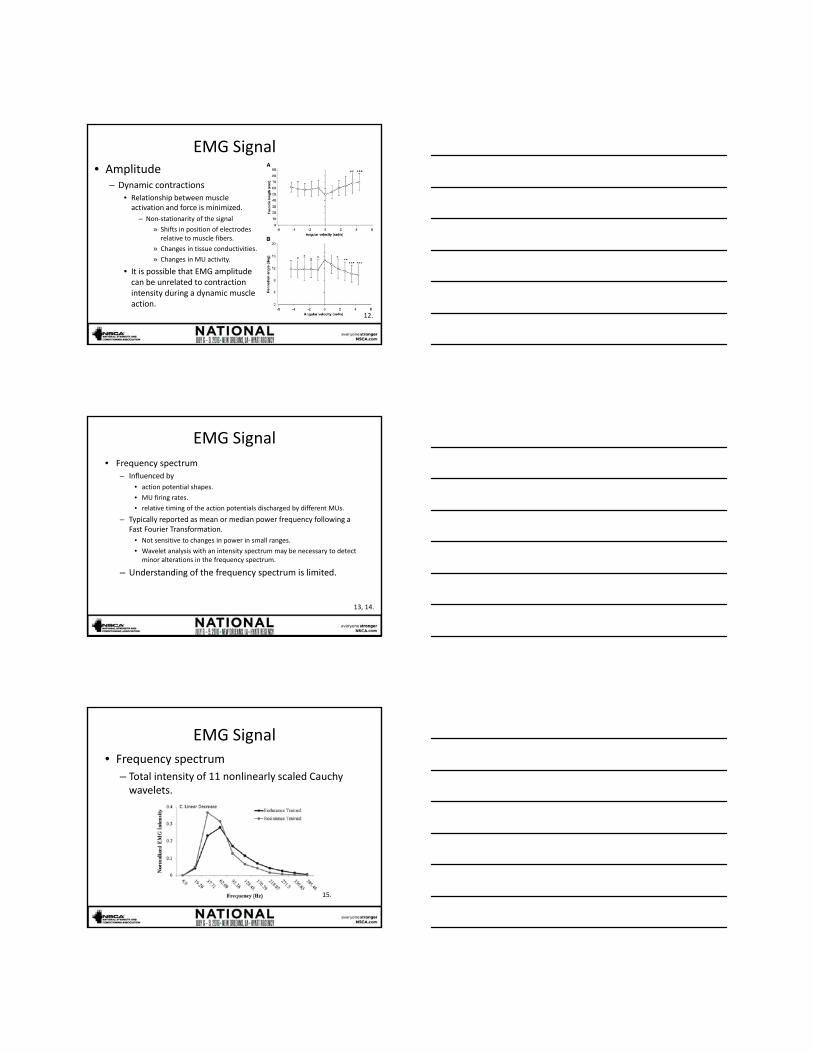
EMG Signal• Amplitude
– Dynamic contractions• Relationship between muscle activation and force is minimized.
– Non‐stationarity of the signal
» Shifts in position of electrodes relative to muscle fibers.
» Changes in tissue conductivities.
» Changes in MU activity.
• It is possible that EMG amplitude can be unrelated to contraction intensity during a dynamic muscle action.
12.
EMG Signal
• Frequency spectrum– Influenced by
• action potential shapes.
• MU firing rates.
• relative timing of the action potentials discharged by different MUs.
– Typically reported as mean or median power frequency following a Fast Fourier Transformation.
• Not sensitive to changes in power in small ranges.
• Wavelet analysis with an intensity spectrum may be necessary to detect minor alterations in the frequency spectrum.
– Understanding of the frequency spectrum is limited.
13, 14.
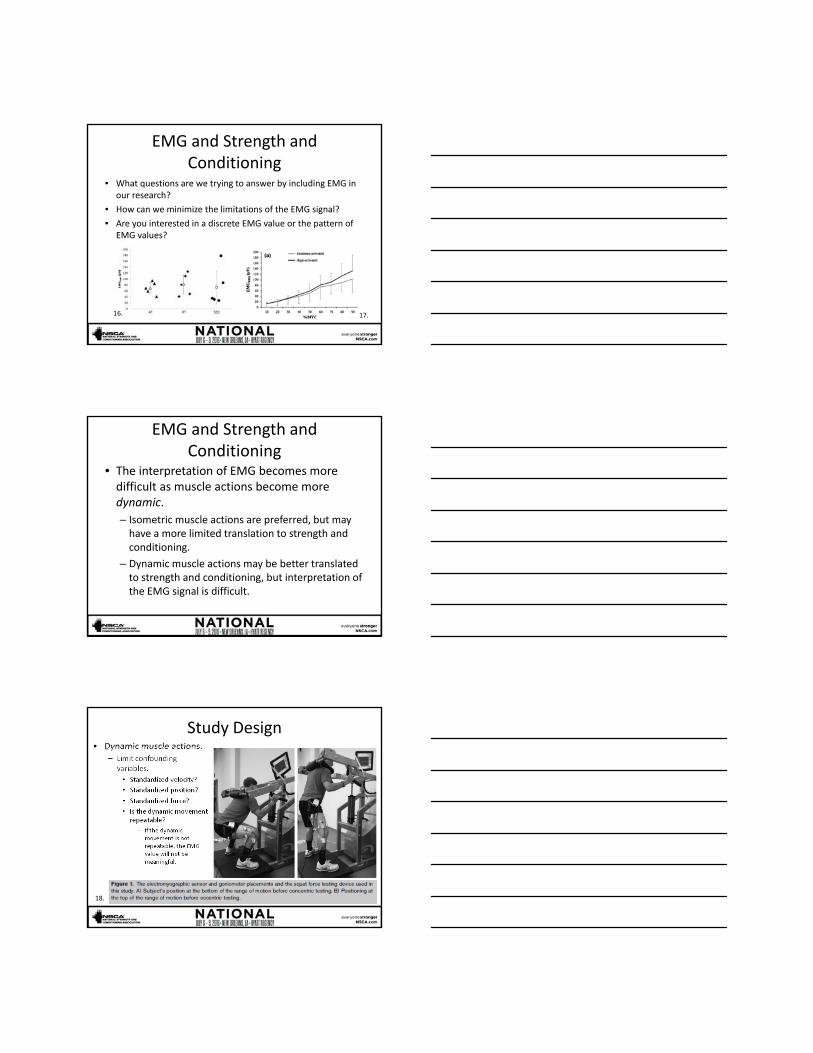
EMG Signal• Frequency spectrum
– Total intensity of 11 nonlinearly scaled Cauchy wavelets.
15.
EMG and Strength and Conditioning
• What questions are we trying to answer by including EMG in our research?
• How can we minimize the limitations of the EMG signal?
• Are you interested in a discrete EMG value or the pattern of EMG values?
16. 17.
EMG and Strength and Conditioning
• The interpretation of EMG becomes more difficult as muscle actions become more dynamic.
– Isometric muscle actions are preferred, but may have a more limited translation to strength and conditioning.
– Dynamic muscle actions may be better translated to strength and conditioning, but interpretation of the EMG signal is difficult.
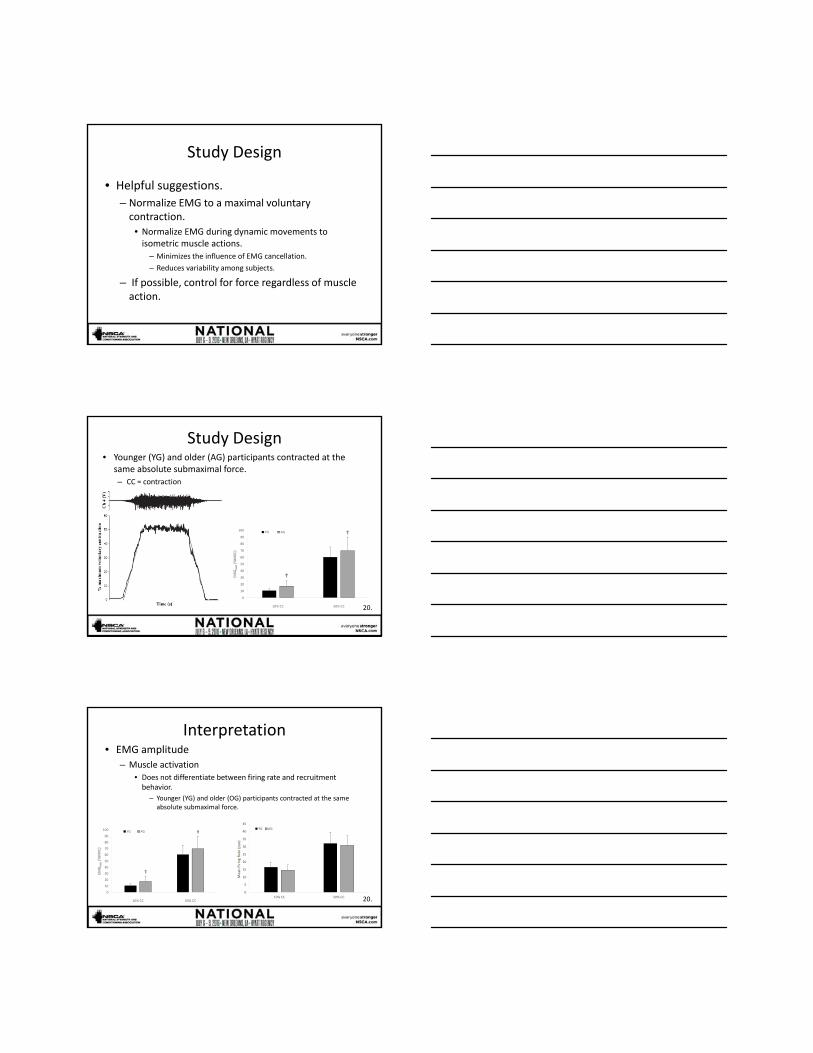
Study Design• Dynamic muscle actions.
– Limit confounding variables.
• Standardized velocity?
• Standardized position?
• Standardized force?
• Is the dynamic movement repeatable?
– If the dynamic movement is not repeatable, the EMG value will not be meaningful.
18.

Study Design
• Dynamic muscle actions.– Limit confounding variables.
• Standardized velocity?
• Standardized position?
• Standardized force?
19.
Study Design
• Regardless of muscle action, cross‐over design is preferred to test interventions.
– Comparing EMG between groups is difficult because of potential differences in
• subcutaneous fat.
• MU distribution.
• fiber pennation angle.
– Subcutaneous fat at the site of the sensor should always be measured and reported.
Study Design• Training interventions.
– Did EMG change as a function of subcutaneous fat?
• Muscle‐related differences.– Is EMG different because subcutaneous fat overlying the muscle is
different?
– MU distribution different?
Vastus Lateralis Rectus Femoris
17.
Study Design
• Helpful suggestions.
– Normalize EMG to a maximal voluntary contraction.
• Normalize EMG during dynamic movements to isometric muscle actions.
– Minimizes the influence of EMG cancellation.
– Reduces variability among subjects.
– If possible, control for force regardless of muscle action.
Study Design
0
10
20
30
40
50
60
70
80
90
100
10% CC 50% CC
EMGRMS(%MVC)
YG AG
• Younger (YG) and older (AG) participants contracted at the same absolute submaximal force.– CC = contraction
20.
Interpretation• EMG amplitude
– Muscle activation• Does not differentiate between firing rate and recruitment behavior.
– Younger (YG) and older (OG) participants contracted at the same absolute submaximal force.
0
5
10
15
20
25
30
35
40
45
10% CC 50% CC
Mean Firing Rate (pps)
YG AG
0
10
20
30
40
50
60
70
80
90
100
10% CC 50% CC
EMGRMS(%MVC)
YG AG
20.

Interpretation
• EMG amplitude– Muscle activation
• Can estimate timing and amplitude of muscle action.
• EMG amplitude is strongly correlated with force.
16.
Interpretation• EMG frequency
– Power spectrum has been reported to increase, not change, or decrease with an increase in muscle force.
21.
Interpretation• EMG frequency
• May provide valuable information regarding muscle fatigue.– Decreases in action potential conduction
velocity.
– Changes in action potential shape.
– Reduced relaxation rates of muscle.
– Increased inorganic phosphate concentrations.
– Decreased intramuscular pH.
– Altered sarcolemmal ion gradients.
19.

Interpretation
• EMG frequency
• Traditional measures of EMG center frequency cannot distinguish– decreases in low‐frequency power.
– increases in high‐frequency power.
» or a combination of both.
• Salutation ‐ Separate into– low‐frequencies.
– high‐frequencies.
13.
Interpretation
EMG Decomposition
22.
Questions?







