high risk patients. Patients receiving 5 Fr PD stents have a reduced risk of post-ERCP pancreatitis compared to those receiving no active treatment (odds ratio0.13, 95% probability interval 0.02-0.37). 5Fr PD stents ranked as most efficaciousintervention for the prevention of PEP with a 97.6% probability of rankingamong the top 3 and 78% probability of ranking as the best form of prophylaxis.5 Fr PD stents were followed by 3 Fr PD stents (83.7% probability of rankingamong the top 3 interventions) and NSAIDs (49.6% probability of ranking amongthe top 3 interventions). Conclusion: 5 Fr PD stents are more efficacious than 3Fr PD stents and all pharmacologic agents in preventing PEP among high-riskpatients. Further studies will be needed to determine if a combination of PDstents and NSAIDs can synergistically reduce the incidence of PEP.
Sa1524A Meta-Analysis on the Role of Rectal Diclofenac andIndomethacin in the Prevention of Post-ERCP PancreatitisSaurabh Sethi*1, Nidhi Sethi2, Alphonso Brown1
1Division of Gastroenterology, Beth Israel Deaconess Medical Centerand Harvard Medical School, Boston, MA; 2Division of Hepatology,Beth Israel Deaconess Medical Center and Harvard Medical School,Boston, MABackground: Clinical trials evaluating the protective effect of non-steroidal anti-inflammatory drugs (NSAIDs) for the prevention of post-endoscopic retrogradecholangiopancreatography (ERCP) pancreatitis have yielded inconclusive results.Two meta-analyses looking at the role of NSAIDs in preventing post-ERCPpancreatitis were published in 2008 and 2009. Both the studies looked at andanalyzed the data from the clinical trials of Diclofenac and Indomethacintogether. We propose that pooling all available studies on these two NSAIDs
separately and systematically may provide a better understanding of anydifference in performance between these two medications. Also, since the lastmeta-analysis on this issue, 2 more randomized controlled studies have beenpublished including the recent large randomized controlled trial published byElmunzer et al. in NEJM, 2012. Objectives: To perform a meta-analysis of studiesevaluating the effect of prophylactic rectal NSAIDs i.e. Diclofenac andIndomethacin on post- ERCP pancreatitis. Methods: Searches were conducted inthe databases PubMed, EMBASE and the Cochrane Library. Two independentreviewers systematically identified prospective randomized controlled trials(RCTs) examining the effect of rectally administered prophylactic NSAIDs on theincidence of post-ERCP pancreatitis. A meta-analysis of these clinical trials wasperformed. Statistical analysis was performed using Review Manager (RevManversion 5.0). Meta-analysis was performed using fixed effect or random-effectmethods, depending on the absence or presence of significant heterogeneity. Weused the �2 test to assess heterogeneity between trials and the I2 statistic toassess the extent of inconsistency. P � 0.10 was defined as significantheterogeneity. Results were expressed as RR with 95% CI. P � 0.05 wasconsidered statistically significant. Results: Seven RCTs, enrolling a total of 2236patients, have been published. Three of these looked at Indomethacin and 4 atDiclofenac. The Mantel-Haenszel pooled relative risk (RR) for PEP afterprophylactic administration of NSAIDs was 0.51 (95% CI 0.40 to 0.65, P�0.01).The risk of pancreatitis was lower in the Diclofenac group than in the placebogroup (RR: 0.49, 95% CI: 0.26to 0.91, P�0.03). The same was true forIndomethacin group compared from placebo (RR: 0.51, 95% CI 0.37 to 0.70,P�0.01). No deaths or NSAID-related complications were reported in any of theclinical trials. Conclusions: In this meta-analysis, prophylactic NSAIDs wereeffective in preventing post-ERCP pancreatitis as a combined group and alsoseparately for Diclofenac and Indomethacin. Either of these agents can be usedprophylactically to reduce the incidence of post-ERCP pancreatitis, resulting inmajor clinical and economic benefit.
Network of randomized controlled trials (RCT) comparing different in-terventions for their efficacy in post-ERCP pancreatitis prophylaxis. Eachcircle represents an intervention used in the analysis and the numbers onlines connecting interventions indicate the number of RCTs and the oddsratios (95% probability intervals). Odds ratios are between the activeintervention and no active treatment, * between somatostatin and gabex-ate, # between 3 Fr PD stent and 5 Fr PD stent respectively. (IL -Interleukin, Fr - French, PD- pancreatic duct)
Rankograms comparing all the interventions used in analysis to compareefficacy in preventing post-ERCP pancreatitis. The vertical axis lists theintervention evaluated and horizontal axis lists the probability of achiev-ing the best, second best, or the third best rank. The intervention havingthe longest bar indicates the best performing intervention. (IL - Interleu-kin, Fr - French, PD- pancreatic duct)
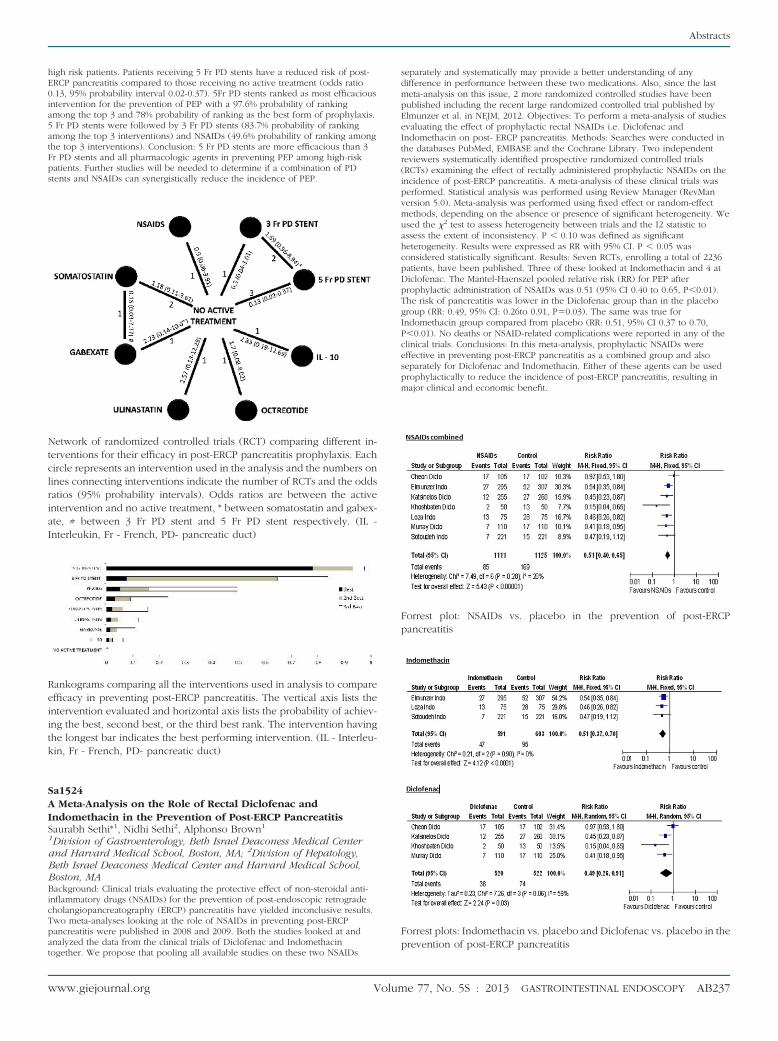
Forrest plot: NSAIDs vs. placebo in the prevention of post-ERCPpancreatitis
Forrest plots: Indomethacin vs. placebo and Diclofenac vs. placebo in theprevention of post-ERCP pancreatitis
Abstracts
www.giejournal.org Volume 77, No. 5S : 2013 GASTROINTESTINAL ENDOSCOPY AB237







