
Scaling up Prevention of Mother to Child Transmission of HIV (PMTCT):
What Will it Take to Eliminate MTCT?
Jessica RodriguesPresentation for UNICEF Written Test
04 May 2012
Photograph courtesy of EGPAF and NPR

Where We Are: Global Progress to Date
• More pregnant women counseled and tested for HIV
• Uptake of PMTCT services improving....
Follow up care for HIV exposed infants is poor
•35-42% pregnant women (PW) receive HIV testing and counseling•Significant increase in East and Southern Africa
•52-61% PW receive most effective regimens BUT ONLY•5 of 22 priority countries reached 80% coverage
•42% infants received antiretroviral (ARV) medicine for PMTCT•28% HIV exposed infants diagnosed early•23% children in need receive antiretroviral therapy (ART)

Smart Scale-Up
Source: Towards Universal Access, WHO, 2011
Focus on Countries With Highest MTCT Burden!
High PMTCT Coverage &
Low Rates of MTCT Country Adult HIV
Prevalence
HIV Prevalence in Pregnancy
PMTCT Coverage
ART Children Coverage
Nigeria 3% 2.4-4% 10% 12%
South Africa 18% 29% 73% 61%
US and UK 0.3-0.6% 0.06% >95% >95%
Source: Towards Universal Access, WHO, 2011 and Besser, 2011


Where We’re Going: Global Targets
MTCT accounts for 90%
of new infections
1,000 children infected
with HIV everyday
48% of pregnant women received ARV medicine for PMTCT
Reduce number of pediatric infections by 90%
Reduce number of AIDS related maternal deaths by 50%
Today 2015EffectivePMTCT
Source: Global Plan for the Elimination of Pediatric HIV and UNDP
Reduce HIV incidence
among women 15-49 yrs by 50%
Reduce unmet family
planning need to zero
MTCT to 5%
90% of eligible
pregnant women
ART
PrimaryInfection
Unintended Pregnancy
ARV prophylaxis
Care, Treatment & Support
Source: WHO, UNAIDS, UNICEF 2010
ANDMDGs 3-6
(Gender Equity, Infant Mortality, Maternal Health, Infectious Diseases)
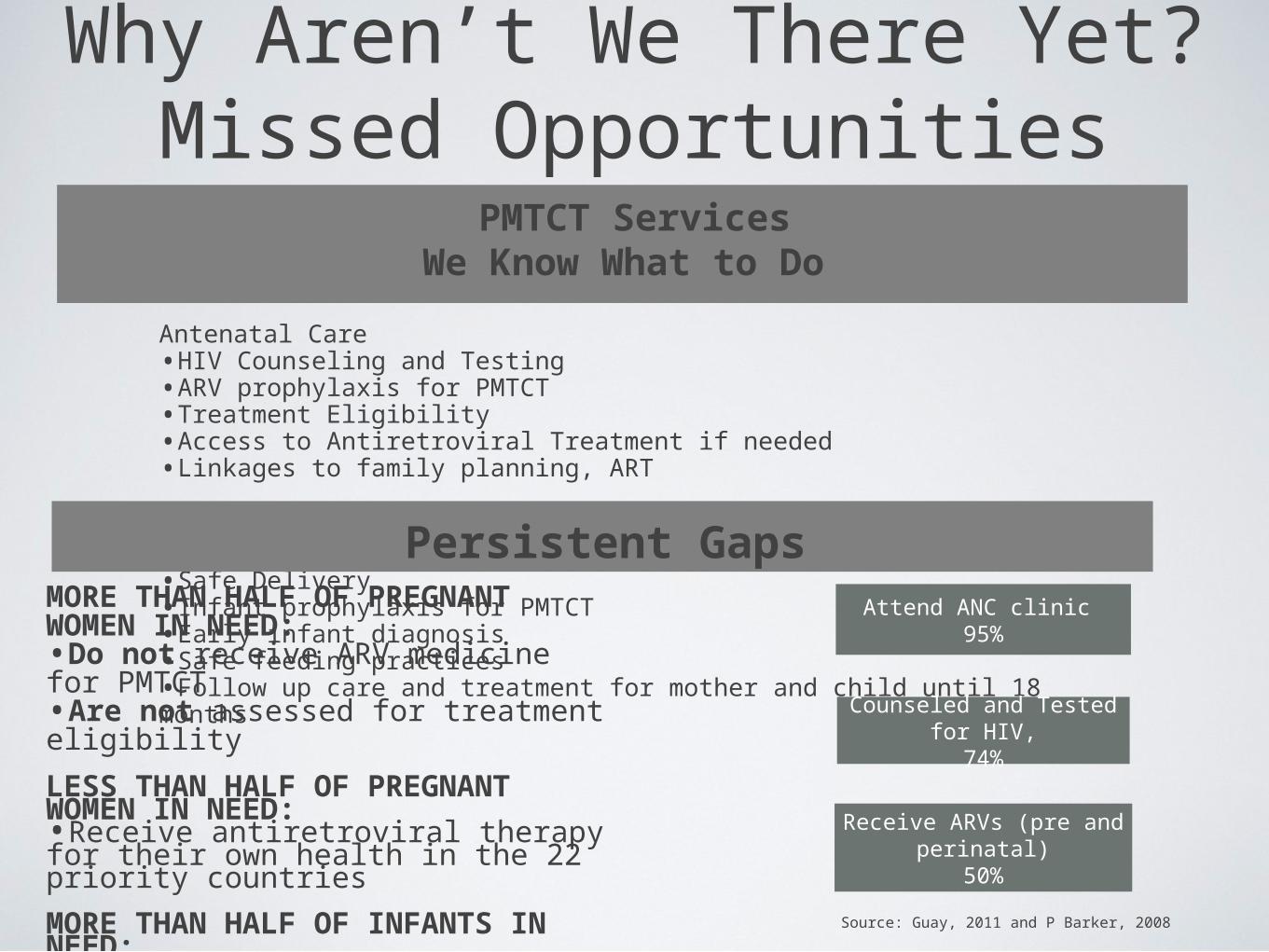
Antenatal Care•HIV Counseling and Testing •ARV prophylaxis for PMTCT•Treatment Eligibility•Access to Antiretroviral Treatment if needed•Linkages to family planning, ART
Labor and Delivery•Safe Delivery•Infant prophylaxis for PMTCT•Early infant diagnosis •Safe feeding practices•Follow up care and treatment for mother and child until 18 months
Why Aren’t We There Yet?Missed Opportunities
PMTCT ServicesWe Know What to Do
Persistent GapsMORE THAN HALF OF PREGNANT WOMEN IN NEED:•Do not receive ARV medicine for PMTCT•Are not assessed for treatment eligibility
LESS THAN HALF OF PREGNANT WOMEN IN NEED:•Receive antiretroviral therapy for their own health in the 22 priority countries
MORE THAN HALF OF INFANTS IN NEED:•Do not receive ARV medicine for PMTCT
Attend ANC clinic 95%
Counseled and Tested for HIV,
74%
Receive ARVs (pre and perinatal)
50%
Source: Guay, 2011 and P Barker, 2008

Challenges to Scaling Up PMTCT
• Quality
• Pre and post test, pre-ART, adherence counseling
• Limited diagnostic capacity
• Fragmented services
• Access
• Poverty (Long distances, transport, opportunity costs)
• Stigma and discrimination
• Low or late ANC attendance and home deliveries
• Health system bottlenecks
• Stock outs of tests, drugs and consumables
• Human resource shortages and high turnover
• Monitoring and evaluation tools and registers
HIGH ATTRITION
& POOR ADHERENCE
COMPROMISED RESPONSE
LATE IDENTIFICATIO
N

The Many Roads AheadHospital
Promote service integration (FP, MCH)
Increase uptake of more efficacious regimensImprove diagnostic
capacity with point of care technologyTask shifting for
counseling and testingExpand provider initiated
testing and counseling
Community Expand community
based testingStrengthening
community support, patient led support
groupsEncourage male
involvementIncrease patient
voice and feedback
Health SystemProduce, train and
retain health workers
Innovative financing
mechanismsStrengthen supply chain management
Improve data quality and use
CommitmentRamp up global
advocacy & resource
mobilizationCoordinated
technical assistancePromote
government accountability to
scale upIncrease private
sector involvement







