
Does Tight Glycemic Control Improve CV Diabetic Complications?
Khalifa AbdallahProf. of Internal Medicine
Diabetes, Metabolism & Lipidology UnitAlexandria Faculty of Medicine
No

UKPDS: elevated blood glucose levels increase the risk of diabetic complications
Study population: White, Asian Indian and Afro-Caribbean UKPDS patients (n = 4,585) Adjusted for age, sex and ethnic groupError bars = 95% CI Adapted from Stratton IM, et al. BMJ 2000; 321:405–412.
20
40
60
80
Incidence per1,000 patient-years
5 6 7 8 9 10 11
Myocardialinfarction
Microvasculardisease
Updated mean HbA1c (%)
00
HbA1c
6.5%

Intensive vs. conventional management
Time from randomization (years)
Media
n A
1C (
%)
Conventional Treatment (n=1138)
Intensive Treatment (n=2729)
9
8
7
6
00 3 6 9 12 15
}0.9%
Adapted from UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837-853.
UKPDSUKPDS

NS = not significant; PVD = peripheral vascular disease.
*Per 1000 patient-years.
**Combined microvascular and macrovascular events.
Adapted from United Kingdom Prospective Diabetes Study Group (UKPDS) Lancet 1998;352:837-853.
Intensive Glucose Control Significantly Reduced Microvascular
Disease
Rate*Conventional Intensive
glucose glucosecontrol control % Risk
(n=2729) (n=1138) reduction p
Macrovascular events
• MI17.4 14.7 16 0.052
• Stroke 5.0 5.6 –11NS
• PVD 1.6 1.1 35NS
• Diabetes-related death 11.5 10.4 10NS
• All-cause mortality 18.9 17.9 6NS
Microvascular events 11.4 8.6 250.0099
All events** 46.0 40.9 120.029

57% risk reduction in non-fatal MI, stroke or CVD death*(P = 0.02; 95% CI: 12–79%)
Cu
mu
lati
ve i
nci
de
nce
o
f n
on
-fat
al M
I, s
tro
ke o
r d
eath
fro
m C
VD
Conventionaltreatment
Intensivetreatment
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21Years
0.06
0.04
0.02
0.00
Adapted from DCCT. N Engl J Med 1993; 329:977–986. DCCT/EDIC. JAMA 2002; 287:2563–2569.DCCT/EDIC. N Engl J Med 2005; 353:2643–2653.
DCCT/EDIC: glycaemic control reduces the risk of non-fatal MI, stroke or death from CVD in type 1 diabetes
0
7
1 6
Hb
A1
C (
%)
9
8
2 3 4 5 7 8 9
Conventional treatment
Intensive treatment
11 12 13 14 15 16 1710
*Intensive vs conventional treatment
DCCT (intervention period EDIC (observational follow-up)
DCCT (intervention period) EDIC (observational follow-up)
Years
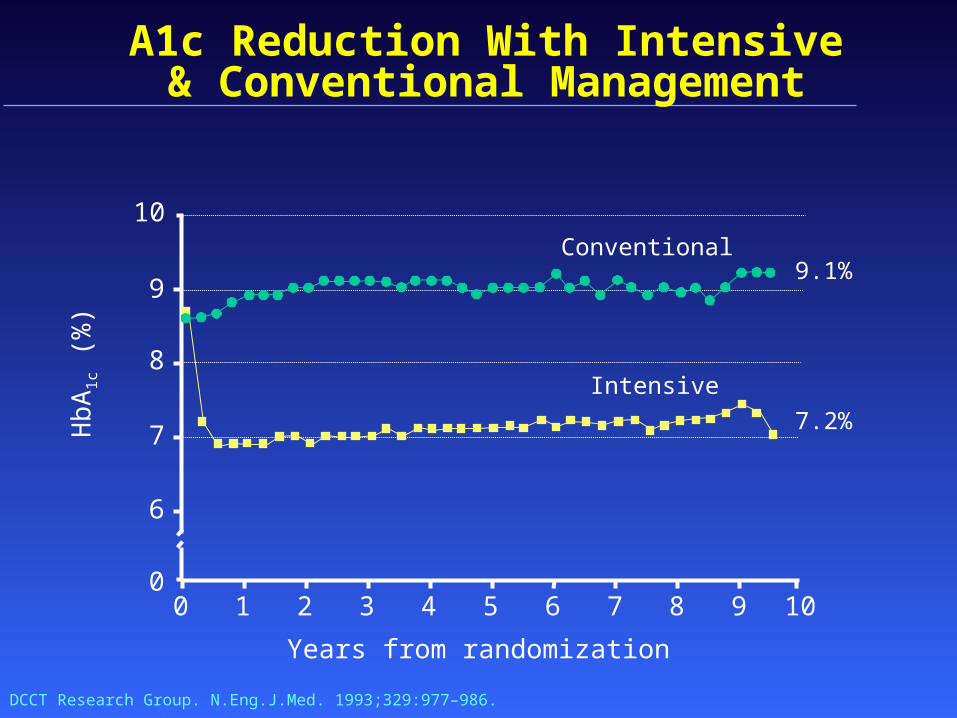
A1c Reduction With Intensive & Conventional Management
0 2 4 6 8 10
Years from randomization
5 731 9
8
9
10
7Hb
A1
c (%
)
6
0
Intensive
Conventional
DCCT Research Group. N.Eng.J.Med. 1993;329:977–986.
9.1%
7.2%

UKPDS: Post-Trial Changes in HbA1c
UKPDS resultspresented
Mean (95%CI)
UKPDS 80. N Eng J Med 2008; 359

After median 8.5 years post-trial follow-up
Aggregate Endpoint 1997 2007
Any diabetes related endpoint RRR: 12% 9% P: 0.029 0.040
Microvascular disease RRR: 25% 24% P: 0.0099 0.001
Myocardial infarction RRR: 16% 15% P: 0.052 0.014
All-cause mortality RRR: 6% 13% P: 0.44 0.007
RRR = Relative Risk Reduction, P = Log Rank
UKPDS: Legacy Effect of Earlier Glucose Control
N Eng J Med 2008

UKPDS: Post-Trial Monitoring: Patients
880 Conventional
2,118Sulfonylurea/Insulin
279 Metformin
1997# in survivor cohort
2002
Clinic
Clinic
Clinic
Questionnaire
Questionnaire
Questionnaire
2007# with final year data
379 Conventional
1,010Sulfonylurea/Insulin
136 Metformin
P
P
Mortality 44% (1,852)Lost-to-follow-up 3.5% (146)
Mean age62±8 years
N Eng J Med 2008

Intensive vs. conventional management
Time from randomization (years)
Media
n A
1C (
%)
Conventional Treatment (n=1138)
Intensive Treatment (n=2729)
9
8
7
6
00 3 6 9 12 15
}0.9%
Adapted from UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837-853.
UKPDSUKPDS
Median A1c Conventional : 7.9 %Intensive : 7%

Key insights from the latest randomised trials

ACCORD ADVANCE and VADT- No Significant ACCORD ADVANCE and VADT- No Significant Effect on Macro or Micro Vascular OutcomesEffect on Macro or Micro Vascular Outcomes
ACCORDACCORD ADVANCEADVANCE VADTVADT
No. of participants No. of participants 10,251 10,251 11,140 11,140 1791 1791
Participant age ,years Participant age ,years 62 62 66 66 60 60
Duration of diabetes at Duration of diabetes at study entry, years study entry, years
1010 88 11.511.5
HbA1C at Baseline, % HbA1C at Baseline, % 8.18.1 7.57.5 9.49.4
Participants with prior Participants with prior cardiovascular event, cardiovascular event, % %
3535 3232 4040
Duration of follow-up, Duration of follow-up, years years
3.43.4 5.05.0 66

Summary of ACCORD, ADVANCE and VADTSummary of ACCORD, ADVANCE and VADT
ACCORDACCORD ADVANCEADVANCE VADTVADTNo. of participants No. of participants 10,251 10,251 11,140 11,140 1791 1791
Participant Participant age ,years age ,years
62 62 66 66 60 60
HbA1C at Baseline, HbA1C at Baseline, % %
8.18.1 7.57.5 9.49.4
Significant Effect on Significant Effect on Macrovascular Macrovascular Outcomes?Outcomes?
NoNo NoNo NoNo
Significant Effect on Significant Effect on Microvascular Microvascular Outcomes?Outcomes?
NANA Significant for Significant for nephropathy, nephropathy,
not retinopathynot retinopathy
NoNo
Rosiglitazone use, Rosiglitazone use, (intensive vs. (intensive vs. standard)standard)
90% vs. 58%90% vs. 58% 17% vs. 11%17% vs. 11% 85% vs. 85% vs. 78%78%
Duration of follow-Duration of follow-up, years up, years
3.43.4 5.05.0 66

Summary of ACCORD, ADVANCE and VADTSummary of ACCORD, ADVANCE and VADT
ACCORDACCORD ADVANCEADVANCE VADTVADTNo. of participants No. of participants 10,251 10,251 11,140 11,140 1791 1791
Participant Participant age ,years age ,years
62 62 66 66 60 60
HbA1C at Baseline, HbA1C at Baseline, % %
8.18.1 7.57.5 9.49.4
Significant Effect on Significant Effect on Microvascular Microvascular Outcomes?Outcomes?
NANA Significant for Significant for nephropathy, nephropathy,
not retinopathynot retinopathy
NoNo
Rosiglitazone use, Rosiglitazone use, (intensive vs. (intensive vs. standard)standard)
90% vs. 58%90% vs. 58% 17% vs. 11%17% vs. 11% 85% vs. 85% vs. 78%78%
Duration of follow-Duration of follow-up, years up, years
3.43.4 5.05.0 66Significant Effect on Significant Effect on Macrovascular Macrovascular OutcomesOutcomes??
No No No

Summary of ACCORD, ADVANCE and VADTSummary of ACCORD, ADVANCE and VADTIncidence of Severe Hypoglycemia (%)Incidence of Severe Hypoglycemia (%)
ACCORDACCORD ADVANCEADVANCE VADTVADT
Intensive armIntensive arm 16.216.2 2.72.7 21.221.2
Standard armStandard arm 5.15.1 1.5 1.5 9.99.9

A1cA1c && HypoglycemiaHypoglycemiaIncrease incidence of HypoglycemiaIncrease incidence of Hypoglycemia
HbA1c (%)
5.5 6.0 6.5 7.0 7.5 8.0 8.5 9.0 9.5 10.0
ComplicationsHypoglycaemia
10.5
DCCT Research Group. N.Eng.J.Med. 1993;329:977–986.

Asymptomatic Episodes of Hypoglycemia May Go Unreported
• In a cohort of patients with diabetes, more than 50% had asymptomatic (unrecognized) hypoglycemia, as identified by continuous glucose monitoring1
• Other researchers have reported similar findings2,3
1. Copyright © 2003 American Diabetes Association. Chico A et al. Diabetes Care. 2003;26(4):1153–1157. Reprinted with permission from the American Diabetes Association.
2. Weber KK et al. Exp Clin Endocrinol Diabetes. 2007;115(8):491–494. 3. Zick R et al. Diab Technol Ther. 2007;9(6):483–492.
0
25
50
75
100
All patients with diabetes
Type 1 diabetes
Patie
nts,
%
Type 2diabetes
55.762.5
46.6
Patients With ≥1 Unrecognized Hypoglycemic Event, %
n=70 n=40 n=30

Severe Hypoglycemia Causes QTc Prolongation
P=NS
P=0.0003
Landstedt-Hallin L et al. J Intern Med. 1999;246:299–307.
Euglycemic clamp(n=8)
Hypoglycemic clamp2 weeks afterglibenclamide withdrawal(n=13)
0
360
370
380
390
400
410
420
430
440
450
Mea
n Q
T in
terv
al,
ms
Baseline (t=0)
End of clamp (t=150 min)ACCORD?
Significant QTc prolongation
during
hypoglycemia





Conclusions
• Although observational trials demonstrated that the relationship between glycemic control and CV diabetic complications was log-linear and extended down to the normal A1c with no threshold, yet randomized clinical trials failed to confirm this hypothesis
• There is no solid evidence that tight glycemic control ( A1c <6.5 %) has clear benefit on reducing CV outcome in type 2 diabetic individuals but there is definite evidence that tight glycemic control increases the risk of severe hypoglycemia

•Older patients with long standing diabetes and existing co-morbidities do not benefit from intensive glycemic control
•Controlling nonglycemic risk factors (hypertension, dyslipidemia, obesity, …) with standard glycemic control (A1c < 7%) is still the recommended strategy to prevent CV diabetic complications)
Conclusions-Cont.

Thank youThank you







