
When does enhanced monitoring for atrial fibrillation add value?
Jonathan P. Piccini, MD, MHS, FHRS
Associate Professor of Medicine
Duke Clinical Research Institute
Duke University Medical Center

DisclosuresResearch Grants
• AHRQ
• ARCA biopharma
• Boston Scientific
• German AFNet
• Gilead
• Johnson & Johnson
• ResMed
• St Jude Medical
Consulting
• BMS/Pfizer
• GSK
• Johnson & Johnson
• Laguna Pharmaceuticals
• Medtronic
• Spectranetics
Full disclosures available at
https://www.dcri.org
Controls
Post MI
AF
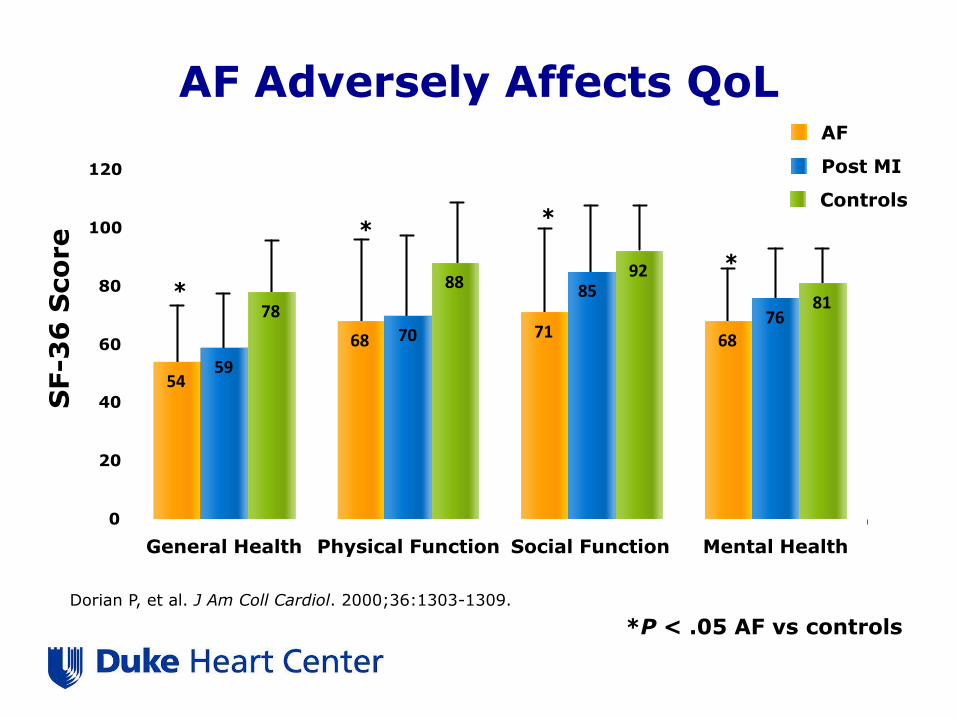
AF Adversely Affects QoL
*
**
*
54
68 71 68
59
70
85
7678
8892
81
0
20
40
60
80
100
120
General Health Physical Function Social Function Mental Health
SF-3
6 S
co
re
Dorian P, et al. J Am Coll Cardiol. 2000;36:1303-1309.
*P < .05 AF vs controls


Stroke
CV Hospitalization
Heart Failure
TIA
Death
Natural History of Atrial Fibrillation

Piccini J P et al. Eur Heart J 2014;35:250-256
The importance of outcomes beyond stroke
Death
Heart Failure

No. at Risk
Persistent 11485 11255 10962 8113 4975 2134
Paroxysmal 2490 2451 2404 1830 1216 498
Adjusted HRparoxysmal =
0.79 (0.67 – 0.94)
p=0.0061
Persistent AF is associated with worse survival
Steinberg, BS. Eur Heart J. 2014; In press.
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0 6 12 18 24 30
Ra
te o
f a
ll-c
au
se
mo
rta
lity
Months since randomization
Persistent AF
Paroxysmal AF

AFB is associated increased risk of hospitalization in pacemaker patients:
BRADYCARE
Mittal S, et al. HRS Scientific Sessions. 2015

• Pts <67 years HR 1.81 (95% CI 1.11-2.94)– Independent of clinical
stroke.
• Strongly associated with duration of exposure to AF
de Bruijn RF. JAMA Neurol. 2015;72:1288-94Alznet.org

Effectiveness Endpoints in Trials of Surgical Interventions for AF
Primary Endpoints
• Electrocardiographically documented AT/AF ≧30 seconds
• Antiarrhythmic therapy
• Cardioversion
• Repeat surgical/catheter ablation
Secondary Endpoints
• AF burden
• Symptom scores
• Quality of life
• Exercise tolerance
• LVEF
• Atrial transport function
• Left atrial size
CDRH. Clinical Study Designs for Surgical Ablation Devices for Treatment of Atrial Fibrillation.
February 15, 2013

Effectiveness Endpoints in Trials of Surgical Interventions for AF
Primary Endpoints
• Electrocardiographically documented AT/AF ≧30 seconds
• Antiarrhythmic therapy
• Cardioversion
• Repeat surgical/catheter ablation
Secondary Endpoints
• AF burden
• Symptom scores
• Quality of life
• Exercise tolerance
• LVEF
• Atrial transport function
• Left atrial size
CDRH. Clinical Study Designs for Surgical Ablation Devices for Treatment of Atrial Fibrillation.
February 15, 2013

Marina Urena et al. Circulation. 2015;131:469-477
24-Hour Continuous ECG Monitoring before TAVR

Marina Urena et al. Circulation. 2015;131:469-477
Cerebrovascular events within 30-days after TAVR

Scirica BM, et al. Europace 2015;17:32-37
Effect of ranolazine on AF in NSTEMI (MERLIN TIMI 36):
continuous ECG during the first 7 days

Scirica BM, et al. Europace 2015;17:32-37
Clinical AF events in patients treated with ranolazine or placebo

PASCAL: Importance of AF burden in clinical trials
Placebo 200 mg bid 400 mg bid 600 mg bid
-80
-70
-60
-50
-40
-30
-20
-10
0
10
20M
ed
ian
Perc
en
t C
han
ge f
rom
Baselin
e
11.2
-12.6
-54.4
-74.2
p=0.07 p=0.013 p=0.0013
ITT Population, % Change in AFB from Baseline
Dose Response: p=<0.0001
Jonckheer-Terpstra test
N=18
N=20
N=18
N=15
Wilcoxon rank sum test vs Placebo
Ezekowitz M et al; Abstract

DADs
EAD
↑[Ca2+]i NCX
↑[Na+]i
Enhanced Late INa Causes and/or contributes to
EP Mechanisms of Arrhythmias
↑QTc
VT
Triggers
Substrate
Abnormal
automaticity
Endo
Epi
∆APD
Dispersion
Spatial Temporal
Late INa
4
GS-6615 (eleclazine)
GS967
EP Phenotype
Belardinelli et al, Heart Rhythm 12: 440-448, 2015 Belardinelli et al, Heart Rhythm 12: 440-448, 2015
Enhanced Late Ina and Arrhythmogenesis

Changes in AF Burden Over 12 Weeks
≥70% Reduction in AFB Overall Changes in AFB
Reiffel JA. Circ Arrhythm Electrophysiol. 2015;8:1048-56.

CAT HF: Arrhythmia Substudy DesignOverall CAT-HF
Population
MV-triggered ASV Control Arm
~50 dual-chamber devices
~50 dual-chamber devices
1 and 2 Events at 0, 3, 6 months
Arrhythmia Core Lab Adjudication
R

Genotype-Directed Therapy of AF in HF: Bucindolol
b1389 Arg/Arg (n = 441; 36 events)
Hazard Ratio = 0.26 (0.12 – 0.57)P-value = 0.0003
Risk reduction 74%
0.70
0.75
0.80
0.85
0.90
0.95
1.00
0 6 12 18 24 30 36 42 48
Prob
abili
ty o
f Ev
ent-
Free
Sur
viva
l
Months After Randomization
Placebo
Bucindolol
Hazard Ratio = 1.01 (0.56 – 1.84)P-value = 0.969
b1389 Gly carriers (n = 484; 44 events)
No risk reduction
Interaction p = 0.008
0.70
0.75
0.80
0.85
0.90
0.95
1.00
0 6 12 18 24 30 36 42 48
Prob
abili
ty o
f Ev
ent-
Free
Sur
viva
l
Months After Randomization
Placebo
Bucindolol
Aleong R. JACC Heart Fail. 2013;1:338-34

LVEF <0.50, Class II-III HF w/in 90 days No contra-indications to b-blockers
b1389 Arg/Arg genotype
Recent onset Sx
AF, 1 wk – 1 yr;Class I-III HF
Bucindolol Toprol-XL
ECV @ 3 wks if still in AF
1° Endpoint = Recurrent AF or ACM at 24 weeksCo-Primary for Phase 2b = AF Burden
n = 100
(310)
n = 100
(310)
Time 0 (chemical conversion to SR or ECV)
AF free/event: from 24 hrs after ECV
Genetically Targeted Therapy for the Prevention of Symptomatic AF in Patients With Heart Failure (GENETIC-AF)
ClinicalTrials.gov Identifier:NCT01970501

Overaccessorize much?

Patch-Based Holter Monitoring
Smart Phone-Based Event Monitoring

Chung EH. J Electrocardiol. 2015;48:8-9
Monitoring DofetilideAntiarrhythmic Drug Therapy
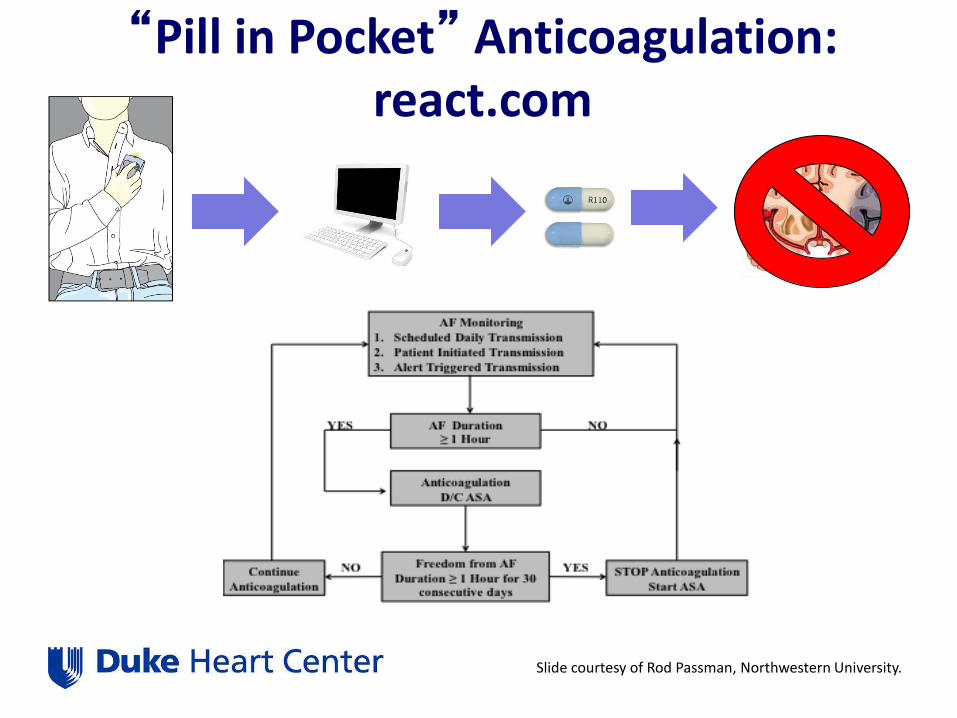
“Pill in Pocket” Anticoagulation: react.com
Slide courtesy of Rod Passman, Northwestern University.
Conclusions
• AF symptoms are the tip of the iceberg
• AF burden is an important biosignature– Associated with a variety of important outcomes
including stroke, hospitalization, and all-cause mortality
• AF burden can assist in trials, particularly in early clinical development

Summary• Safety first.
• Be aggressive with your ACT targets
• Bridging therapy is associated with a higher risk of bleeding complications– Emerging theme >> Anticoagulation transitions carry more risk than
continued anticoagulation
• Once a diagnosis of AF is made, stroke prophylaxis should be guided by risk stratification alone (and not rhythm)
Duke Center for Atrial Fibrillation







