when does enhanced monitoring for atrial fibrillation add · pdf filewhen does enhanced...
TRANSCRIPT

When does enhanced monitoring for atrial fibrillation add value?
Jonathan P. Piccini, MD, MHS, FHRS
Associate Professor of Medicine
Duke Clinical Research Institute
Duke University Medical Center

DisclosuresResearch Grants
• AHRQ
• ARCA biopharma
• Boston Scientific
• German AFNet
• Gilead
• Johnson & Johnson
• ResMed
• St Jude Medical
Consulting
• BMS/Pfizer
• GSK
• Johnson & Johnson
• Laguna Pharmaceuticals
• Medtronic
• Spectranetics
Full disclosures available at
https://www.dcri.org
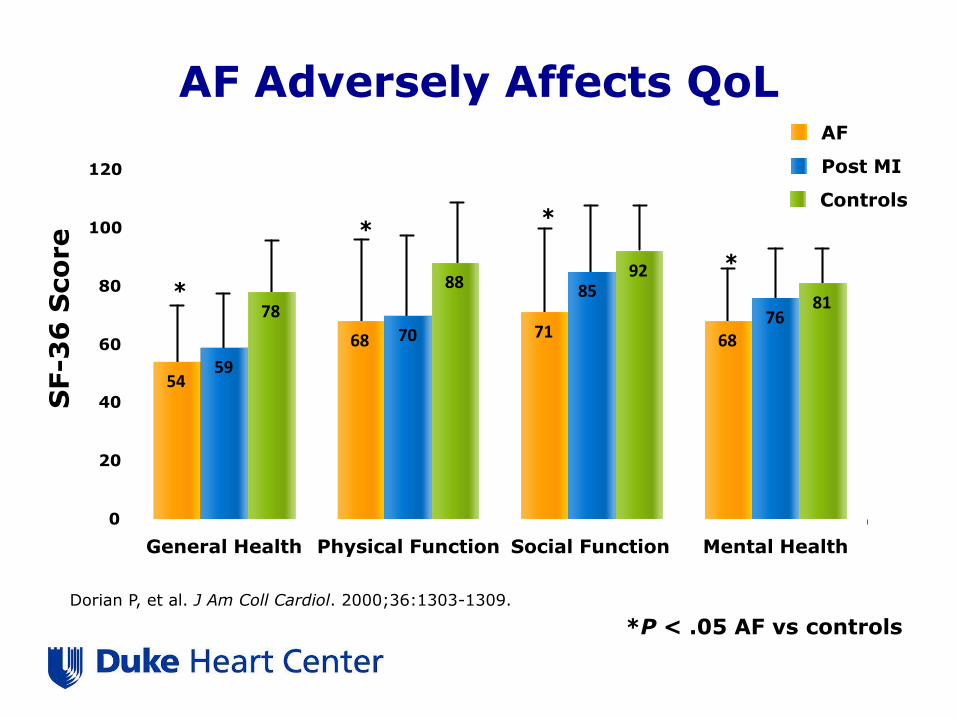
Controls
Post MI
AF
AF Adversely Affects QoL
*
**
*
54
68 71 68
59
70
85
7678
8892
81
0
20
40
60
80
100
120
General Health Physical Function Social Function Mental Health
SF-3
6 S
co
re
Dorian P, et al. J Am Coll Cardiol. 2000;36:1303-1309.
*P < .05 AF vs controls


Stroke
CV Hospitalization
Heart Failure
TIA
Death
Natural History of Atrial Fibrillation

Piccini J P et al. Eur Heart J 2014;35:250-256
The importance of outcomes beyond stroke
Death
Heart Failure

No. at Risk
Persistent 11485 11255 10962 8113 4975 2134
Paroxysmal 2490 2451 2404 1830 1216 498
Adjusted HRparoxysmal =
0.79 (0.67 – 0.94)
p=0.0061
Persistent AF is associated with worse survival
Steinberg, BS. Eur Heart J. 2014; In press.
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0 6 12 18 24 30
Ra
te o
f a
ll-c
au
se
mo
rta
lity
Months since randomization
Persistent AF
Paroxysmal AF

AFB is associated increased risk of hospitalization in pacemaker patients:
BRADYCARE
Mittal S, et al. HRS Scientific Sessions. 2015

• Pts <67 years HR 1.81 (95% CI 1.11-2.94)– Independent of clinical
stroke.
• Strongly associated with duration of exposure to AF
de Bruijn RF. JAMA Neurol. 2015;72:1288-94Alznet.org

Effectiveness Endpoints in Trials of Surgical Interventions for AF
Primary Endpoints
• Electrocardiographically documented AT/AF ≧30 seconds
• Antiarrhythmic therapy
• Cardioversion
• Repeat surgical/catheter ablation
Secondary Endpoints
• AF burden
• Symptom scores
• Quality of life
• Exercise tolerance
• LVEF
• Atrial transport function
• Left atrial size
CDRH. Clinical Study Designs for Surgical Ablation Devices for Treatment of Atrial Fibrillation.
February 15, 2013

Effectiveness Endpoints in Trials of Surgical Interventions for AF
Primary Endpoints
• Electrocardiographically documented AT/AF ≧30 seconds
• Antiarrhythmic therapy
• Cardioversion
• Repeat surgical/catheter ablation
Secondary Endpoints
• AF burden
• Symptom scores
• Quality of life
• Exercise tolerance
• LVEF
• Atrial transport function
• Left atrial size
CDRH. Clinical Study Designs for Surgical Ablation Devices for Treatment of Atrial Fibrillation.
February 15, 2013

Marina Urena et al. Circulation. 2015;131:469-477
24-Hour Continuous ECG Monitoring before TAVR

Marina Urena et al. Circulation. 2015;131:469-477
Cerebrovascular events within 30-days after TAVR

Scirica BM, et al. Europace 2015;17:32-37
Effect of ranolazine on AF in NSTEMI (MERLIN TIMI 36):
continuous ECG during the first 7 days

Scirica BM, et al. Europace 2015;17:32-37
Clinical AF events in patients treated with ranolazine or placebo

PASCAL: Importance of AF burden in clinical trials
Placebo 200 mg bid 400 mg bid 600 mg bid
-80
-70
-60
-50
-40
-30
-20
-10
0
10
20M
ed
ian
Perc
en
t C
han
ge f
rom
Baselin
e
11.2
-12.6
-54.4
-74.2
p=0.07 p=0.013 p=0.0013
ITT Population, % Change in AFB from Baseline
Dose Response: p=<0.0001
Jonckheer-Terpstra test
N=18
N=20
N=18
N=15
Wilcoxon rank sum test vs Placebo
Ezekowitz M et al; Abstract

DADs
EAD
↑[Ca2+]i NCX
↑[Na+]i
Enhanced Late INa Causes and/or contributes to
EP Mechanisms of Arrhythmias
↑QTc
VT
Triggers
Substrate
Abnormal
automaticity
Endo
Epi
∆APD
Dispersion
Spatial Temporal
Late INa
4
GS-6615 (eleclazine)
GS967
EP Phenotype
Belardinelli et al, Heart Rhythm 12: 440-448, 2015 Belardinelli et al, Heart Rhythm 12: 440-448, 2015
Enhanced Late Ina and Arrhythmogenesis

Changes in AF Burden Over 12 Weeks
≥70% Reduction in AFB Overall Changes in AFB
Reiffel JA. Circ Arrhythm Electrophysiol. 2015;8:1048-56.

CAT HF: Arrhythmia Substudy DesignOverall CAT-HF
Population
MV-triggered ASV Control Arm
~50 dual-chamber devices
~50 dual-chamber devices
1 and 2 Events at 0, 3, 6 months
Arrhythmia Core Lab Adjudication
R

Genotype-Directed Therapy of AF in HF: Bucindolol
b1389 Arg/Arg (n = 441; 36 events)
Hazard Ratio = 0.26 (0.12 – 0.57)P-value = 0.0003
Risk reduction 74%
0.70
0.75
0.80
0.85
0.90
0.95
1.00
0 6 12 18 24 30 36 42 48
Prob
abili
ty o
f Ev
ent-
Free
Sur
viva
l
Months After Randomization
Placebo
Bucindolol
Hazard Ratio = 1.01 (0.56 – 1.84)P-value = 0.969
b1389 Gly carriers (n = 484; 44 events)
No risk reduction
Interaction p = 0.008
0.70
0.75
0.80
0.85
0.90
0.95
1.00
0 6 12 18 24 30 36 42 48
Prob
abili
ty o
f Ev
ent-
Free
Sur
viva
l
Months After Randomization
Placebo
Bucindolol
Aleong R. JACC Heart Fail. 2013;1:338-34

LVEF <0.50, Class II-III HF w/in 90 days No contra-indications to b-blockers
b1389 Arg/Arg genotype
Recent onset Sx
AF, 1 wk – 1 yr;Class I-III HF
Bucindolol Toprol-XL
ECV @ 3 wks if still in AF
1° Endpoint = Recurrent AF or ACM at 24 weeksCo-Primary for Phase 2b = AF Burden
n = 100
(310)
n = 100
(310)
Time 0 (chemical conversion to SR or ECV)
AF free/event: from 24 hrs after ECV
Genetically Targeted Therapy for the Prevention of Symptomatic AF in Patients With Heart Failure (GENETIC-AF)
ClinicalTrials.gov Identifier:NCT01970501

Overaccessorize much?

Patch-Based Holter Monitoring
Smart Phone-Based Event Monitoring

Chung EH. J Electrocardiol. 2015;48:8-9
Monitoring DofetilideAntiarrhythmic Drug Therapy
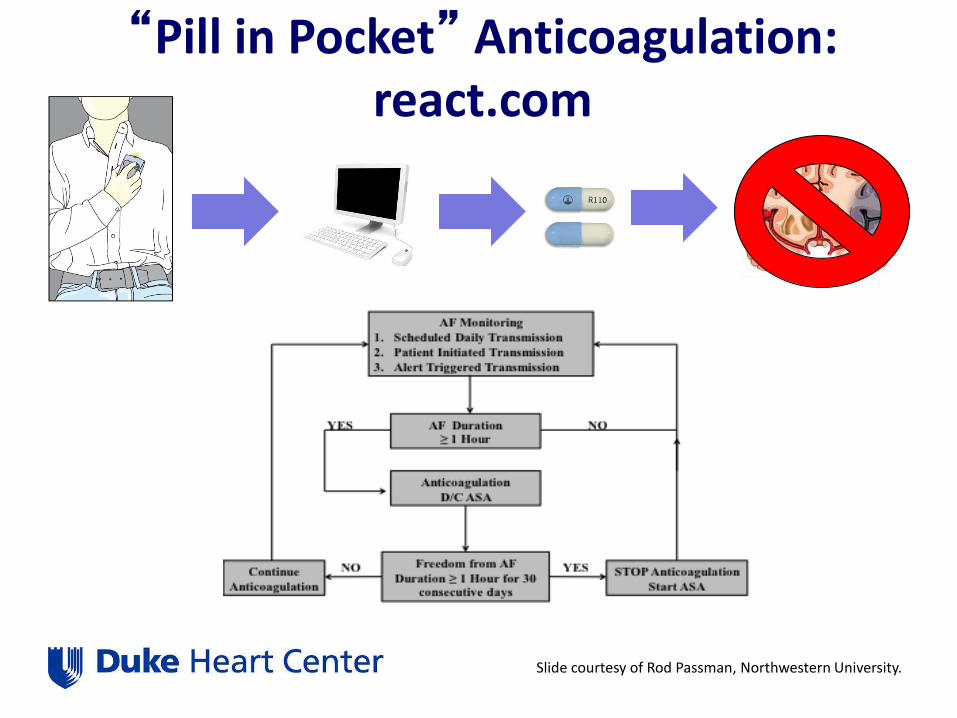
“Pill in Pocket” Anticoagulation: react.com
Slide courtesy of Rod Passman, Northwestern University.
Conclusions
• AF symptoms are the tip of the iceberg
• AF burden is an important biosignature– Associated with a variety of important outcomes
including stroke, hospitalization, and all-cause mortality
• AF burden can assist in trials, particularly in early clinical development

Summary• Safety first.
• Be aggressive with your ACT targets
• Bridging therapy is associated with a higher risk of bleeding complications– Emerging theme >> Anticoagulation transitions carry more risk than
continued anticoagulation
• Once a diagnosis of AF is made, stroke prophylaxis should be guided by risk stratification alone (and not rhythm)
Duke Center for Atrial Fibrillation