drugs for gout
TRANSCRIPT

Sofian Al Shboul ©
Drugs for Gout
Pharmacology and Toxicology
Musculoskeletal System
Third Year Medical Students
Faculty of Medicine
The Hashemite University
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved1

Sofian Al Shboul ©
Gout
• Gout: “the most common crystal-inducedarthropathy”
- Characterized by hyperuricemia andcrystals deposition.
- Inflammatory arthritis.
- Hyperuricemia does not always lead togout, but gout is always preceded byhyperuricemia; study of 990 vs 4200
- Primary or secondary
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved2

Sofian Al Shboul ©
Gout
- Recurrent attacks of a red, tender, hot,and swollen joint.
- Rapid progression in <12h.
- Lifestyle
- Genetics: SLC2A9, SLC22A12
- usually >30 yo
- "the disease of kings" or "rich man'sdisease“.
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved3
Sofian Al Shboul ©
Gout: Pathophysiology
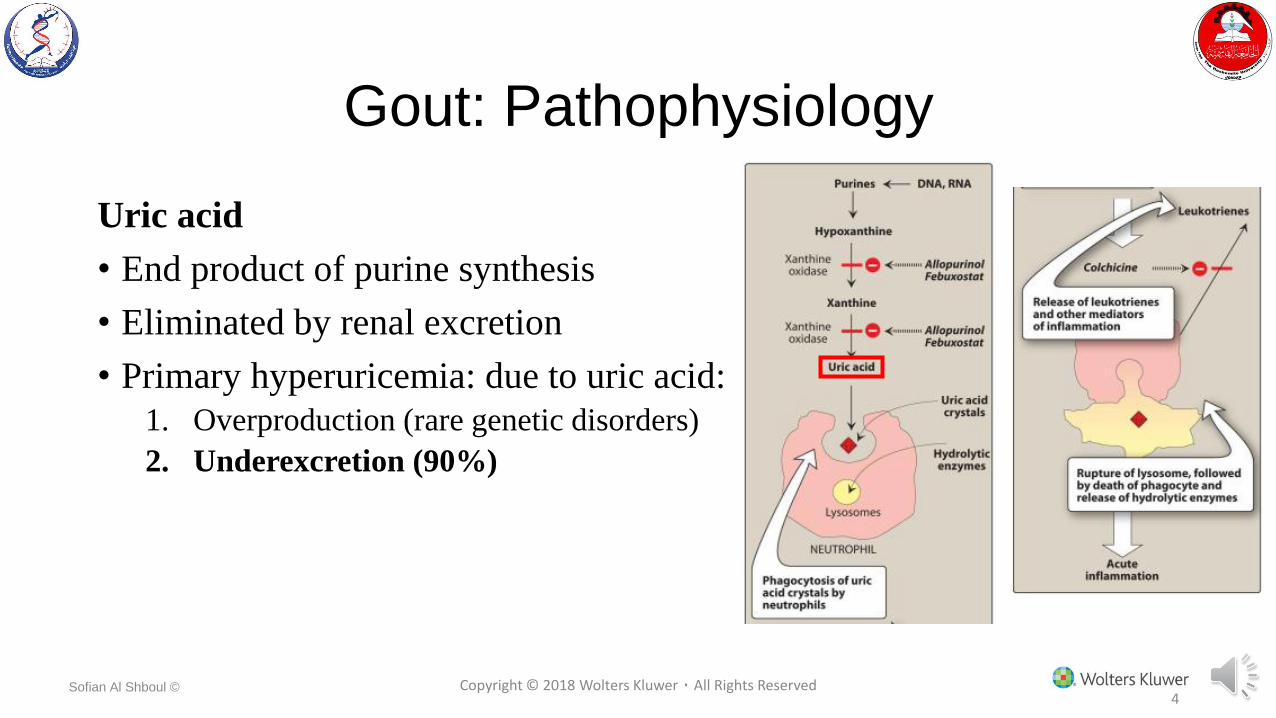
Uric acid
• End product of purine synthesis
• Eliminated by renal excretion
• Primary hyperuricemia: due to uric acid:
1. Overproduction (rare genetic disorders)
2. Underexcretion (90%)
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved4

Sofian Al Shboul ©
Gout: Pathophysiology
• Hyperuricemiaprecipitation of urate salts(needle-like crystals)
• Urate crystal depositionin tissues triggersinflammatory response:
infiltration ofgranulocytes
Needles of urate crystals
Neutrophils attacking the
urate crystals
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved5
Sofian Al Shboul ©
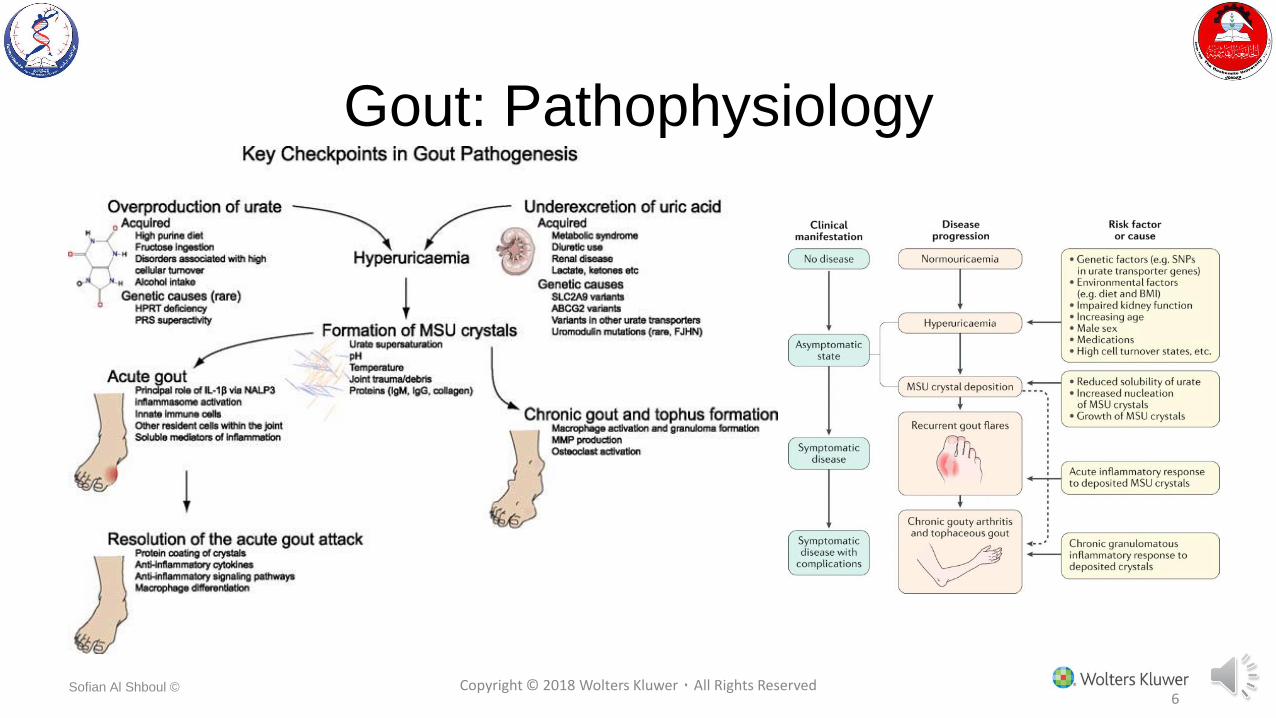
Gout: Pathophysiology
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved6

Sofian Al Shboul ©
Gout: Causes of Secondary Gout
Excessive alcohol consumption
Diet rich in purines
Nephropathy
Starvation or dehydration
Certain drugs
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved7

Sofian Al Shboul ©
What Are The Approach Considerations?
Principles of gout management are :
• Treatment of gout flares (4)
• Urate-lowering therapy
• Anti-inflammatory prophylaxis when starting urate-lowering therapy
• Screening and management of comorbidities associated with gout (Type 2 DM, cardiovasculardisease, hypertension, hyperlipidaemia, etc.)
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved8

Sofian Al Shboul ©
Treatment of Acute Gout
•NSAIDs: e.g., indomethacin•full dosage for 2-5 days•Stop 2 days after symptoms subside
•Intra-articular/systemic corticosteroids•Colchicine•Anakinra or Canakinumab (interleukin-1receptor antagonist)
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved9
Sofian Al Shboul ©
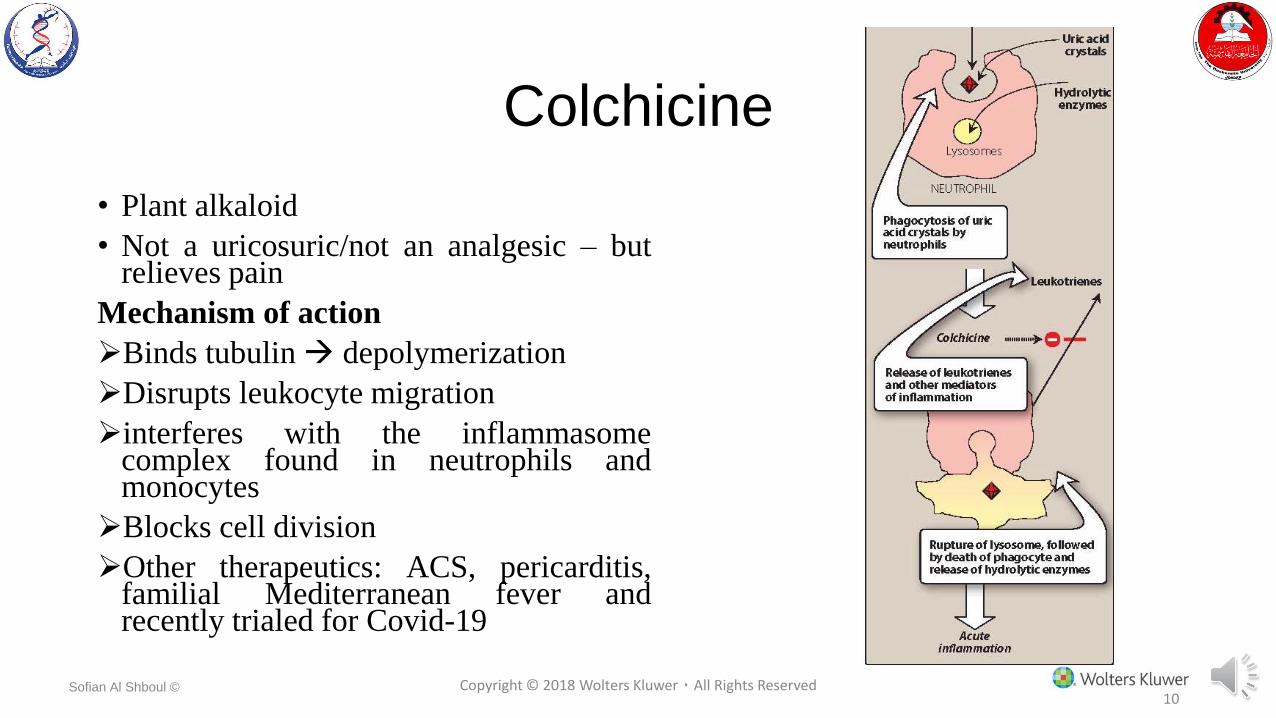
Colchicine
• Plant alkaloid
• Not a uricosuric/not an analgesic – butrelieves pain
Mechanism of action
Binds tubulin depolymerization
Disrupts leukocyte migration
interferes with the inflammasomecomplex found in neutrophils andmonocytes
Blocks cell division
Other therapeutics: ACS, pericarditis,familial Mediterranean fever andrecently trialed for Covid-19
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved10
Sofian Al Shboul ©
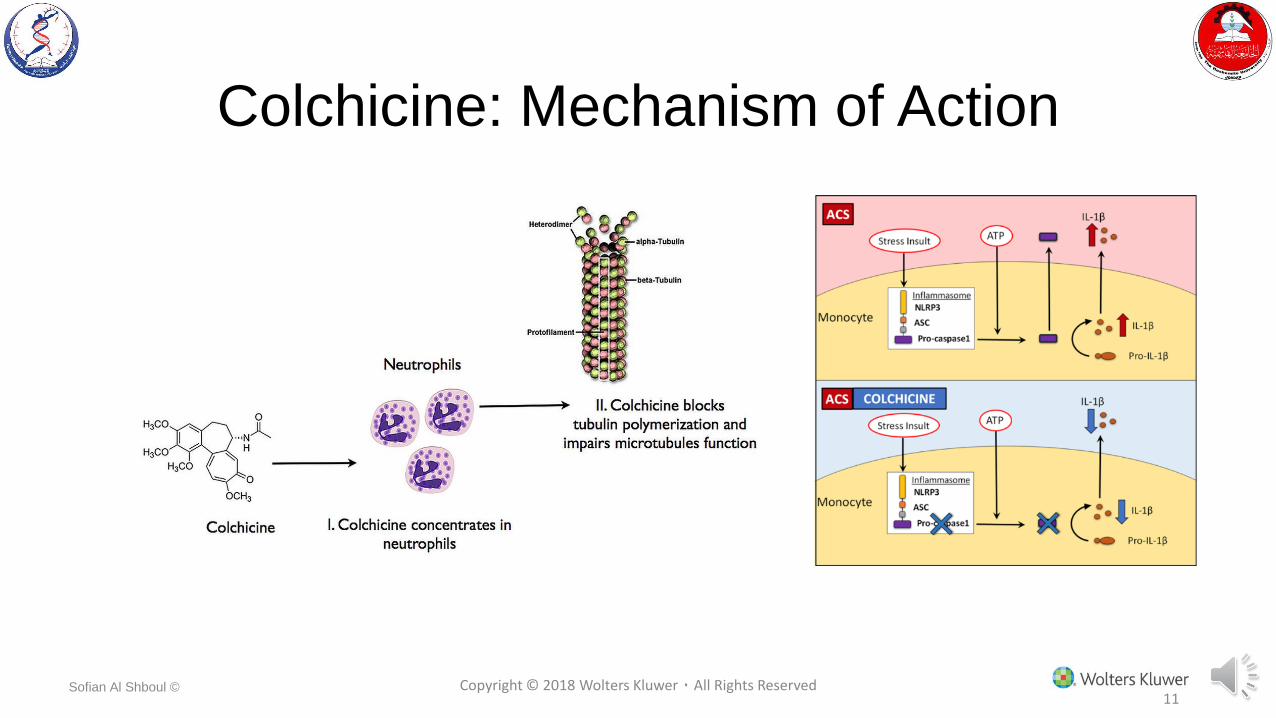
Colchicine: Mechanism of Action
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved11

Sofian Al Shboul ©
Colchicine
Therapeutic uses
1. Relieves acute gout pain within 12 h (given 36 h after onset)
2. Prophylactic agent against gout attacks in patients initiating urate lowering therapy.
Narrow therapeutic window
Pharmacokinetics
• Oral, rapidly absorbed
• Recycles in bile
• Excreted unchanged in feces and urine
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved12

Sofian Al Shboul ©
ColchicineAdverse effects
N/V/D and abdominal pain
Myopathy
Neutropenia, aplastic anemia
Alopecia
Should NOT be used in pregnancy!(FDA;C, AU:D)
Used with caution in patients with hepatic, renal disease
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved13

Sofian Al Shboul ©
Treatment of Chronic Gout
• Aims to reduce thefrequency of attacks andcomplications of gout
• Options:
Xanthine oxidaseinhibitors (allopurinol,febuxostat) – first-line
Uricosuric agents(probenecid)
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved14

Sofian Al Shboul ©
Indications for Uric Acid Lowering Therapy
ACR and EULAR guidelines:
Established diagnosis of gout with one ofthe following:
• Tophus or tophi identified on clinicalexamination or imaging study
• Frequent (≥2/yr) of acute gouty arthritis
• Chronic kidney disease (CKD) stage ≥2
• Previous urolithiasis
Gouty tophus
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved15

Sofian Al Shboul ©
Allopurinol
Mechanism of action
• Purine analog
• Xanthine oxidase inhibitor
• Interferes with the last two stepsin uric acid biosynthesis
• Reduces uric acid production
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved16

Sofian Al Shboul ©
Allopurinol
Pharmacokinetics
• Oral, completely absorbed
• Primary metabolite: alloxanthine (oxypurinol) (also active inhibitor)
• Half-life 15-18 hours
• Excreted in feces and urine
Adverse effects
• Hypersensitivity
• Administered concurrently with NSAIDs, steroids or colchicine. Why?
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved17

Sofian Al Shboul ©
Febuxostat
• Xanthine oxidase inhibitor
• Structurally unrelated toallopurinol (non-purine)
• Similar indication toallopurinol
• Elimination.. Liver > kidney
• Risk of hypersensitivity isless
• Reports of increased CVSevents lead to limited use
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved18

Sofian Al Shboul ©
Probenecid
• Uricosuric agent
• Weak organic acid
• Promotes renal clearance ofuric [inhibits urate-anionexchanger]
• Blocks tubular reabsorptionof uric acid
• How does it interact withaspirin/salicylates?
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved19

Sofian Al Shboul ©
Pegloticase
• Recombinant urate oxidase
• Converts uric acid to allantoin
• Allantoin is a nontoxicmetabolite excreted renally
• Indicated for patients who failstandard therapy
• Given IV every 2 weeks
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved20

Sofian Al Shboul ©
Dietary Restriction
Foods very high in purines:
• Organ meats such assweetbreads (eg, pancreas andthymus)
• Sardines
• Mussels
Foods moderately high in purines
• Trout
• Anchovies
• Haddock
• Scallops
• Mutton
• Veal
• Live
• Salmon
• Kidneys
• Turkey
Copyright © 2018 Wolters Kluwer ٠ All Rights Reserved21
Weight gain is a significant riskfactor for gout (M), whereasweight loss reduces the risk
Avoid Alcohol and encouragevegetables