dubai, april 2018 esmo summit middle east … · urgences en cancérologie place des pncavt prise...
TRANSCRIPT

Dubai, April 2018ESMO Summit Middle EAST
Supportive Care
M. Dicato, M.D., FRCP(Edin).
Hematology- Oncology
Luxembourg Medical Center
L- 1210 Luxembourg

Supportive CareSupportive Care in Cancer is the prevention and management of the adverse effects of cancer and its treatment. This includes management of physical and psychological symptoms and side effects across the continuum of the cancer experience from diagnosis through anticancer treatment to post-treatment care. Enhancing rehabilitation, secondary cancer prevention, survivorship and end of life care are integral to Supportive Care.
MASCC homepage 2015
Supportive Care:- alleviates symptoms and complications of cancer- reduces or prevents toxicities of treatment- supports communication with patients about their disease and prognosis- allows patients to tolerate and benefit from active therapy more easily- eases emotional burden of patients and care givers- helps cancer survivors with psychological and social problems
MASCC homepage 2015

SUPPORTIVE AND PALLIATIVE CARE
Historical reasons have led to the development of specialist groups with expertise towards issues
• frequent at the end of life (often called palliative care)
• around treatment management, and post-treatment issues (supportive care)
Courtesy: M. Aapro 2015

PREDICTING SURVIVAL[ECC 2013, Abs 1745].
Predictive Factors Points
Metastatic Sites ≥ 3 1
PS 1 1
LDH 250 - 600 U/l 1
Hb < 6,2 mmol/l 1
Albuminemia < 35 g/l 2
LDH > 600 U/l 2
PS ≥ 2 3
Rotteveel K, et al. Abstract 1745 ESMO 2013.

FOUR GROUPS MEDIAN SURVIVAL (MS) AND MORTALITY (M)
AT 90 DAYS (D90)
• - Score ≥ 4: MS 2.6 ms D90 M 79%
• - Score = 3: MS 5.0 ms D90 M 43%
• - Score = 2: MS 7.1 ms D90 M 31%
• - Score = 1: MS 9.5 ms D90 M 28%
• - Score = 0: MS 15 ms D90 M 17%
Rotteveel K, et al. Abstract 1745 ESMO 2013.

LES RÉFÉRENTIELS EN SOINS DE SUPPORT AFSOS
Arrêt des traitements spécifiques
Abords et dispositifs veineux
Activité physique adaptée
Anémie
Antinauséeux/antiémétiques
Biphosphonates hypercalcémie
Confusion
Dépression
Douleur
Dyspnée
Epilepsie
Escarres
Fatigue
Fièvre
HTIC-céphalées-déficit neurologique
Reinsertion sociale et PEC de la précarité
Onco sexo: Gestion des complications
induites par CT
Réeducation fonctionnelle et cognitive en
neuro-oncologie
Lymphœdèmes
Mucites et candidoses
Nutrition
Prise en charge sociale
Sexualité et fertilité
Soins bucco-dentaires
Thrombose et cancer
Toxicités des thérapies ciblées
Urgences en cancérologie
Place des PNCAVT
Prise en charge dans les 1eres 20h d’un
patient pour syndrome confusionnel
Troubles de la fonction rénale et CT
Anxiété en cancérologie
Reconstruction mammaire
Toxicités des CT: Docetaxel
Neuropathies périphériques
80 référentiels existants à ce jour:
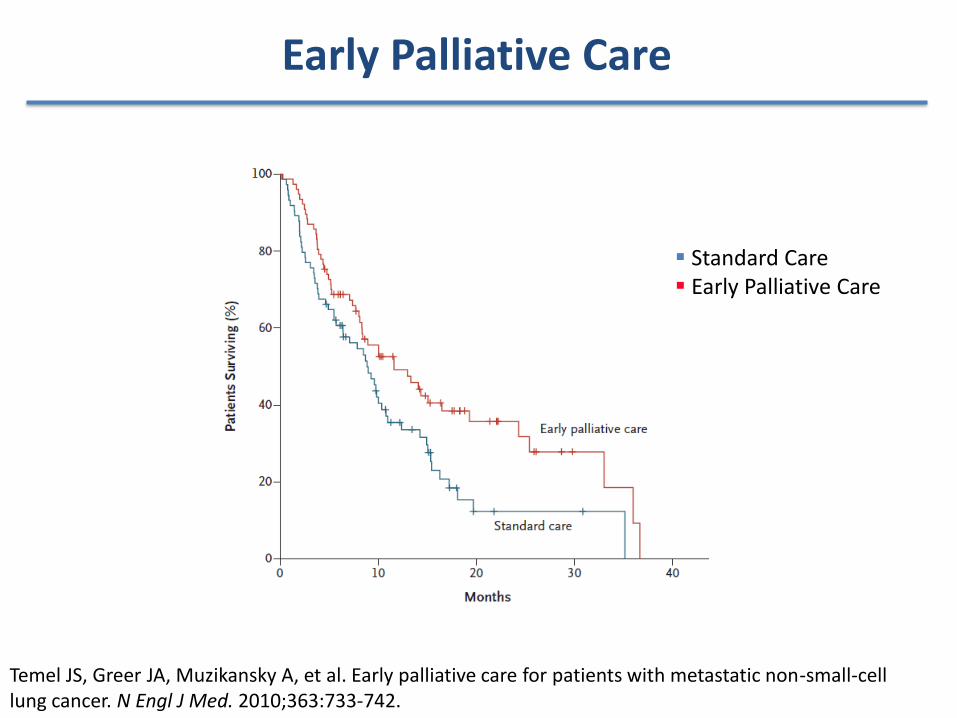
Survie Globale
Early Palliative Care
▪ Standard Care▪ Early Palliative Care
Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363:733-742.

Overall survival results of a randomized trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment (NCT00578006)
Presented By Ethan Basch at 2017 ASCO Annual Meeting LBA2

Study Design
Presented By Ethan Basch at 2017 ASCO Annual Meeting

Patient Self-Reporting Interface
Presented By Ethan Basch at 2017 ASCO Annual Meeting

Results
Presented By Ethan Basch at 2017 ASCO Annual Meeting

Slide 17
Presented By Ethan Basch at 2017 ASCO Annual Meeting

Slide 18
Presented By Ethan Basch at 2017 ASCO Annual Meeting

Potential Mechanisms of Action
Presented By Ethan Basch at 2017 ASCO Annual Meeting

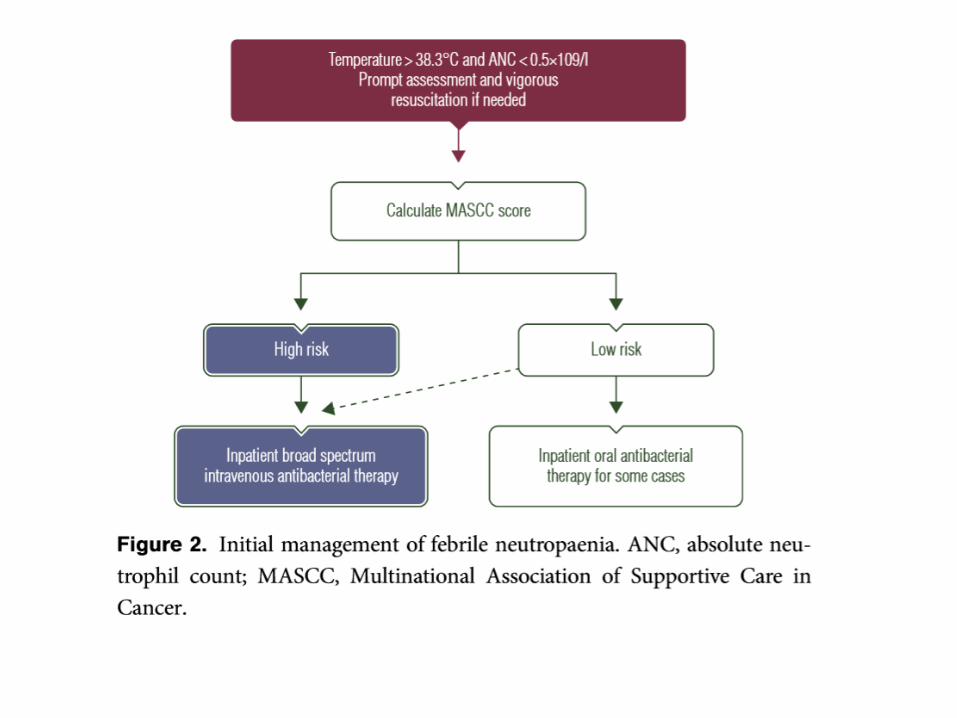
Febrile Neutropenia








Pegfilgrastim clearance is self-regulating, in contrast to that of filgrastim
Daily G-CSF: Filgrastim
Filgrastim is a recombinantgrowth factorthat regulatesthe number of
circulatingneutrophils
Neutrophil
Recepto
rFilgrastim
Filgrastim is cleared by both glomerular filtration and by neutrophils
Pegfilgrastim
Receptor
Neutrophil
Pegfilgrastim
Pegfilgrastim appears to have mainly neutrophil-mediated clearance
Pegfilgrastim is formed by
the addition of a
polyethylene glycol (PEG) group to the
N-terminus of filgrastim
Komrokji RS, et al. Expert Opin Biol Ther 2004;4:1897-910.

Theoretical Pegfilgrastim and Lipegfilgrastim Receptor Binding
Possibility of
steric interference
with the receptor
Low possibility of
steric interference
with the receptor
*Developed on the basis of crystallographic modelling of G-CSF/G-CSF-receptor binding.44
41. Pasut G, Veronese FM. J Control Release. 2012;161(2):461-472; 43. DeFrees S, et al. Glycobiology. 2006;16(9):833-843;
44. Tamada T, et al. Proc Natl Acad Sci U S A. 2006;103(9):3135-3140; 45. Zündorf I, Dingermann T. Pharmazie. 2014;69(5):323-
326.

Short-Acting vs Long-Acting G-CSF: Effect on Absolute Neutrophil Count (ANC)
• Study design: Randomised, multicentre study of patients with high-risk stage II-IV breast cancer (n = 310)
undergoing myelosuppressive chemotherapy with doxorubicin 60 mg/m²and docetaxel 75 mg/m²
• Filgrastim administered daily starting at day 2, continuing until a documented ANC ≥10 109/L after the
expected nadir or for up to 14 d, whichever occurred first
Holmes FA et al. J Clin Oncol. 2002;20:727-731.
ANC Profile of the Median ANC for All 4 Cycles

Lipegfilgrastim: Phase III Study in Breast Cancer (XM22-03): ANC During First Chemotherapy Cycle
Secondary Endpoint: Lipegfilgrastim vs Pegfilgrastim – Median Absolute Neutrophil Count (ANC) by Day in Chemotherapy Cycle 1 (per-protocol population)
ANC, absolute neutrophil count.
1.5-day difference in least
squares mean (p = 0.0026)
Adapted from Bondarenko et al 2013 (figure 3, page 9/12) to depict timepoint of
G-CSF administration on day 2 following chemotherapy treatment in cycle 1.
Day within chemotherapy cycle
55. Bondarenko I, et al. BMC Cancer. 2013;13:386.

Median Number of Daily G-CSF Injections:
Potential Impact on Outcomes
G-CSF Usage Daily G-CSF (n = 111) Pegfilgrastim (n = 75)
Primary prophylaxis, % 39.6 38.7
Median injections/cycle, n
(minimum, maximum)6 (1, 13) 1 (1, 3)
• Study design: LEARN was a multicentre, retrospective observational study in
Spain comparing patterns of use of daily G-CSF and pegfilgrastim and
CIN-related outcomes1,a
• Clinical studies suggest an average of 11 injections per chemotherapy cycle are required to achieve recovery of the ANC to within the normal range2
• Onset and duration of nadir are important to establish starting day and duration of G-CSF administration after chemotherapy3
• Long-acting G-CSF may provide benefits over filgrastim if current guidelines for daily administration cannot be realised4
a In adults with nonmyeloid malignancies receiving myelosuppressive chemotherapy.
CIN: chemotherapy-induced neutropenia.
1. Almenar D et al. Eur J Cancer Care (Engl). 2009;18:280-286. 2. Cooper KL et al (published online). BMC Cancer. 2011;11:404.
doi: 10.1186/1471-2407-11-404 3. Ria R et al. Hematology. 2013;18(3):131-7. 4. Aapro M et al. Eur J Cancer. 2011;47:8-32.

Anemia

Anaemia occurs most frequently in patients
receiving chemotherapy
Anaemia prevalence in patients receiving different cancer treatments
Ludwig H, 2004
Anaemia was defined as Hb<12g/dL
CT= Chemotherapy, RT= Radiotherapy

Anemia and Iron Deficiency
• Absolute Fe deficiency: Ferritin <100ng/ml
• Functional Fe deficiency: Ferritin >100 ng/ml + Tsat <20%

IL-6hepcidin Fe unavailability
Pathophysiology of Anemia of Cancer and of Chronic Disease*
a.
b.
*Modified from Nouwrousian1996 . M. DICATO, Curr. Opinion Oncol. 2010
GATA 1 & 2

F. Morceau, M. Dicato, M. Diederich: Mediators of inflammation, 2009
TNFa
TNFa inhibits induction of erythroid differentiation
inhibits expression of erythroid specific genes:
y-globin and EpoR
effects induced transcription factor GATA-1
Blocks binding of GATA-1 to its DNA sequence
Conclusion: TNFa acts at several levels of the regulation of
erythroid genes, in particular GATA- 1.
Inhibition of GATA-1 correlates to increased NF-kB activity
M.Dicato, et al.: Ann. Oncol. 2010

Tumour cells
Inhibition of EPO production and iron metabolism
causes anaemia of chronic disease (ACD)
1. Adamson JW, 2008; 2. Birgegard G, 2005; 3.Grotto HZW, 2008; 4 Weiss G, 2005; 5. Nowrousian MR, 2008; 6. Hedenus M, 2009
Inhibit
production
of EPO
Hypoproliferative
anaemia
Activated immune
system
Over-production of
cytokines
TNF-α, Interferon-γ, IL-1 Decreased Fe
absorption
Hepcidin
Inhibit
erythropoiesis
IL-6



Six published studies show higher haematologic
response with I.V. iron supplementation of ESAs
• Improved haematopoietic response although most patients were iron replete
at enrolment ESAs need mobilisable iron
1. Auerbach, JCO 2004;22:1301; 2. Hedenus; Leukemia 2007;21:627; 3. Henry, Oncologist 2007;12:231; 4. Bastit, JCO
2008;26:1611; 5. Pedrazzoli, JCO 2008;26:1619; 6. Auerbach, Am J Hematol 2010;85:655; 7. Steensma, JCO 2011;29:97.
ESA + I.V. iron
0
10
20
30
40
50
60
70
80
90
100
Resp
on
se r
ate
(%
)
73
86
Bastit
20084
25
68
Auerbach
20041
62
77
Pedrazzoli
20085
63
82
Auerbach
20106
6570
Steensma
20117
*
36
53
Henry
20073
*53
87
Hedenus
20072
* **
*
ESA alone* p<0.05

Tumour cells
Inhibition of EPO production and iron metabolism
causes anaemia of chronic disease (ACD)
1. Adamson JW, 2008; 2. Birgegard G, 2005; 3.Grotto HZW, 2008; 4 Weiss G, 2005; 5. Nowrousian MR, 2008; 6. Hedenus M, 2009
Inhibit
production
of EPO
Hypoproliferative
anaemia
Activated immune
system
Over-production of
cytokines
TNF-α, Interferon-γ, IL-1 Decreased Fe
absorption
Hepcidin
Inhibit
erythropoiesis
IL-6
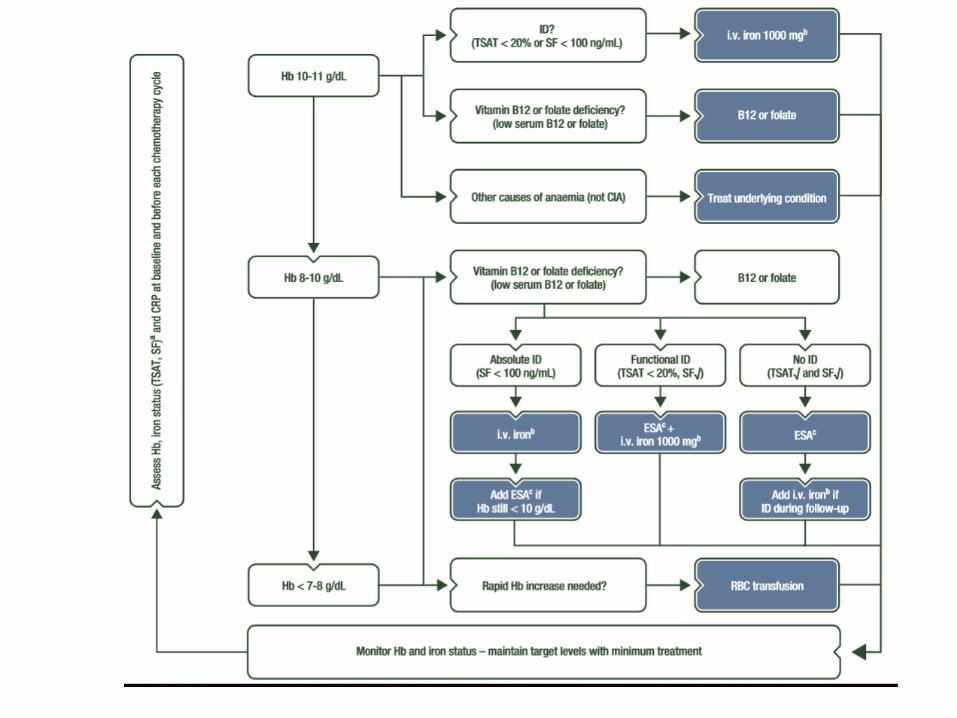

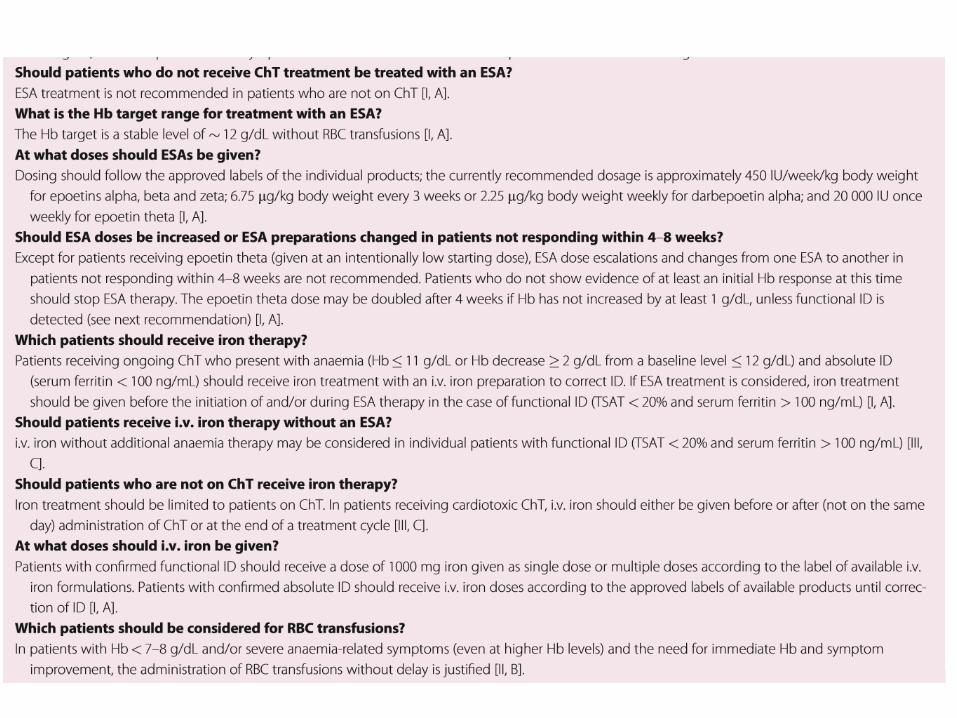
ESMO Clinical Practice Guidelines: Anemia 2018

IPSS

International Consensus Definition of “Cancer Cachexia”“Multifactorial syndrome defined by an ongoing loss of skeletal muscle mass (with or without fat mass) that
cannot be fully reversed by conventional nutritional support and leads to progressive functional impairment.”
Fearon K, et al. Lancet Oncol. 2011 May;12(5):489-95.

Nutrition- Cachexia- Sarcopenia
SARM: selective androgen receptor modulators:- Enobosarm
Anagrelin:- Anamorelin
Cannabis:- Dronabinol

Dobs et al. Lancet Oncol.

Dobs et al. Lancet Oncol. 2016
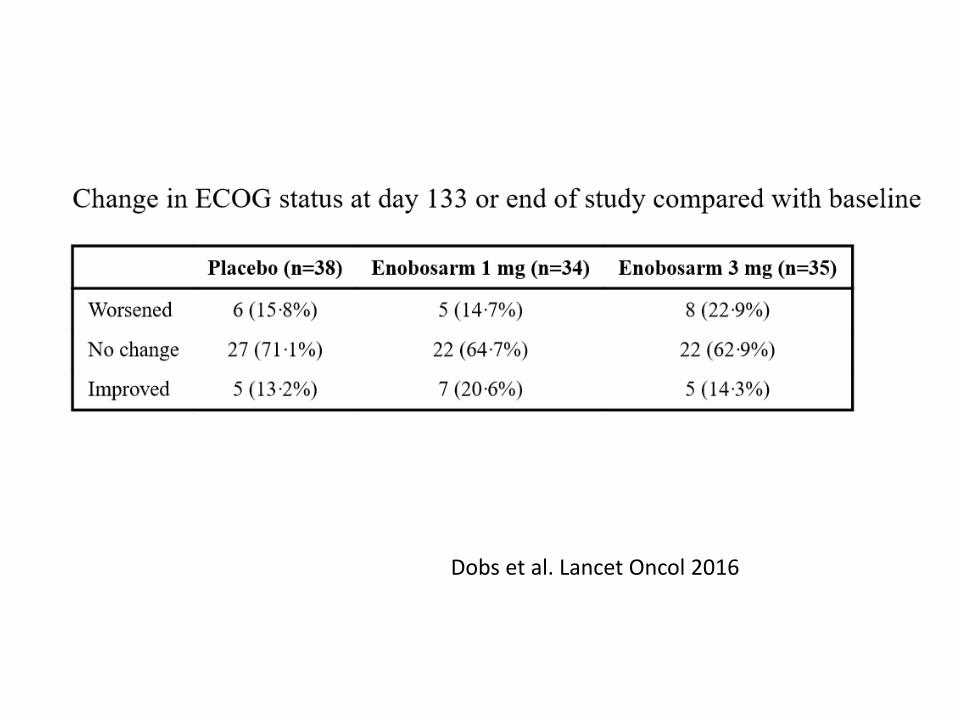
Dobs et al. Lancet Oncol 2016

Trial Design• ROMANA 1 (NCT01387269) is
one of two international,
double-blind, Phase 3 trials
• Patients with unresectable
stage III or IV NSCLC and
cachexia (≥5% weight loss
within prior 6 months or BMI
<20 kg/m2)
• Randomized (2:1) to receive
either 100 mg ANAM or
placebo, administered daily
orally for 12 weeks
• Assess ANAM efficacy and
safetyANAM, anamorelin HCl; BMI, body mass index; NSCLC, non-small cell lung cancer; QD, once a day.
Bonomi, et al. 2014 Chicago Multidisciplinary Symposium in Thoracic Oncology

EMA website. Last update 30.11.2017

Cannabis
• Dronabinol: 1985: FDA approval for anorexia in HIV and for N/V in cancer patients
As RP for anorexia in Cancer Patients:
- Older studies, non conclusive.
- 2006 Strasser study: n= 243 pts; no significance vs placebo
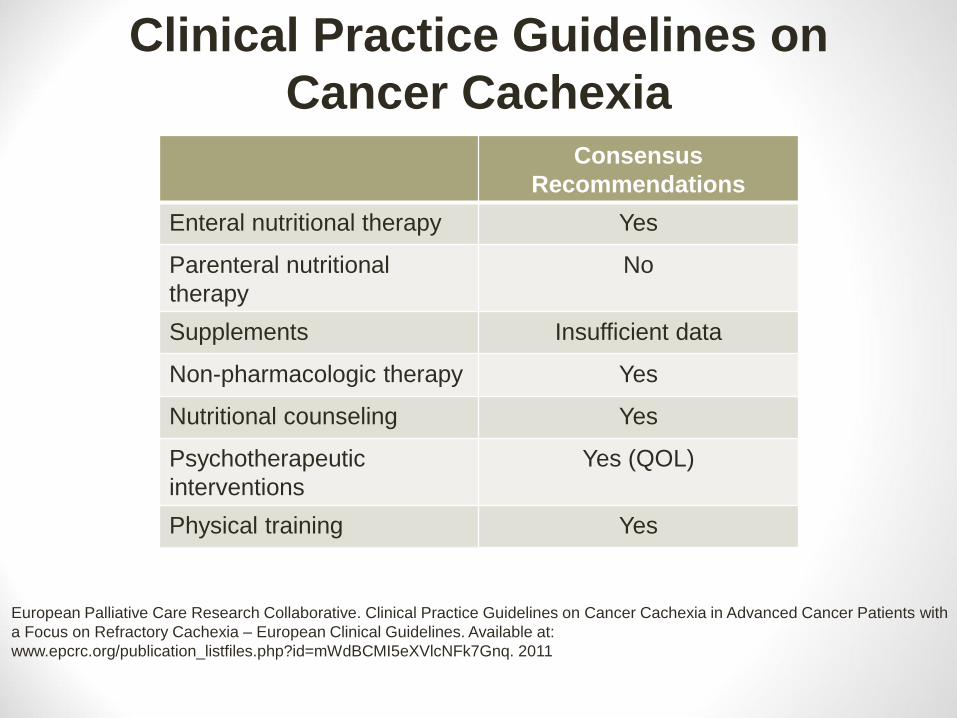
Clinical Practice Guidelines on
Cancer CachexiaConsensus
Recommendations
Enteral nutritional therapy Yes
Parenteral nutritional
therapy
No
Supplements Insufficient data
Non-pharmacologic therapy Yes
Nutritional counseling Yes
Psychotherapeutic
interventions
Yes (QOL)
Physical training Yes
European Palliative Care Research Collaborative. Clinical Practice Guidelines on Cancer Cachexia in Advanced Cancer Patients with
a Focus on Refractory Cachexia – European Clinical Guidelines. Available at:
www.epcrc.org/publication_listfiles.php?id=mWdBCMI5eXVlcNFk7Gnq. 2011

Pharmacologic TherapyConsensus
Recommendations
Thalidomide Insufficient data
Cannabinoids May increase appetite
Omega-3-fatty acids Insufficient data
Megestrol/progestins Stimulate appetite +
increase weight, but not
muscle
Steroids Yes (short term)
Anti-inflammatory agents Little benefit
Prokinetics Yes, for GI symptoms
Clinical Practice Guidelines on
Cancer Cachexia
European Palliative Care Research Collaborative. Clinical Practice Guidelines on Cancer Cachexia in Advanced
Cancer Patients with a Focus on Refractory Cachexia – European Clinical Guidelines. Available at:
www.epcrc.org/publication_listfiles.php?id=mWdBCMI5eXVlcNFk7Gnq. 2011

Emesis

ASCO 2014: 50 years
• MOPP
• BEP
• Ondansetron
• Imatinib
• HPV
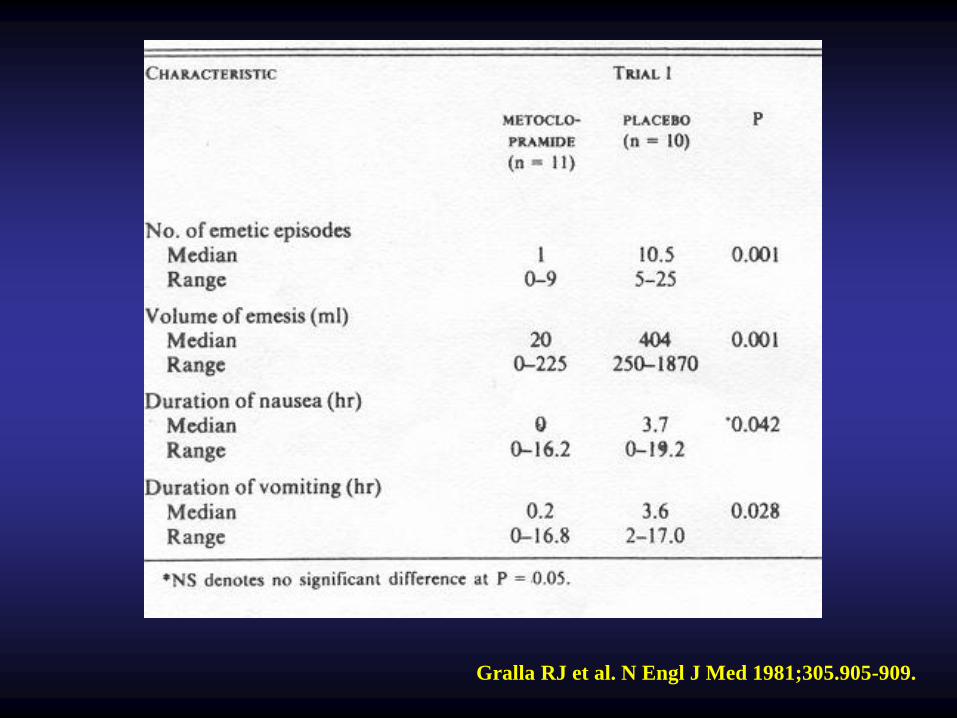
Gralla RJ et al. N Engl J Med 1981;305.905-909.

26-30 September 2014, Madrid, Spain esmo.org
Under-reporting

34
1724
15
35
13
52
28
0
20
40
60
80
100
Acute
Nausea
Acute
Vomiting
Delayed
Nausea
Delayed
Vomiting
Perc
en
t o
f P
ati
en
ts
MD/RN prediction
Patient experience
Physicians and nurses from 14 oncology practices in 6 countries
Patients: 75% women; 78% Mod emetic chemo; 50% breast cancer; 18% lung cancer
Perceptions and Reality- Underestimation of emesis with chemotherapy -
Grunberg et al. (2004). Cancer, 100, 261-268

Prevalence of guideline-consistent CINV prophylaxis (GCCP) for cycle 1 single-day
chemotherapy, by emetogenicity of chemotherapy and for the total study population.
Aapro M., Molassiotis A., Dicato M. et al.: Ann Oncol 2012;23:1986-1992
© The Author 2012. Published by Oxford University Press on behalf of the European Society for
Medical Oncology. All rights reserved. For permissions, please email:

26-30 September 2014, Madrid, Spain esmo.org
Anorexia Nausea Vomiting Constipation Diarrhea Hair loss
Toxicity reported by:
Patient: NO
Physician: NO51.4% 44.5% 76.7% 59.3% 73.1% 55.6%
Patient: NO
Physician: YES2.4% 10.1% 6.4% 3.2% 4.2% 1.7%
Patient: YES
Physician: NO37.0% 24.6% 9.7% 29.7% 13.9% 28.8%
Patient: YES
Physician: YES9.2% 20.8% 7.2% 7.8% 8.9% 13.9%
Cohen's ĸ* 0.162 0.280 0.377 0.183 0.396 0.323
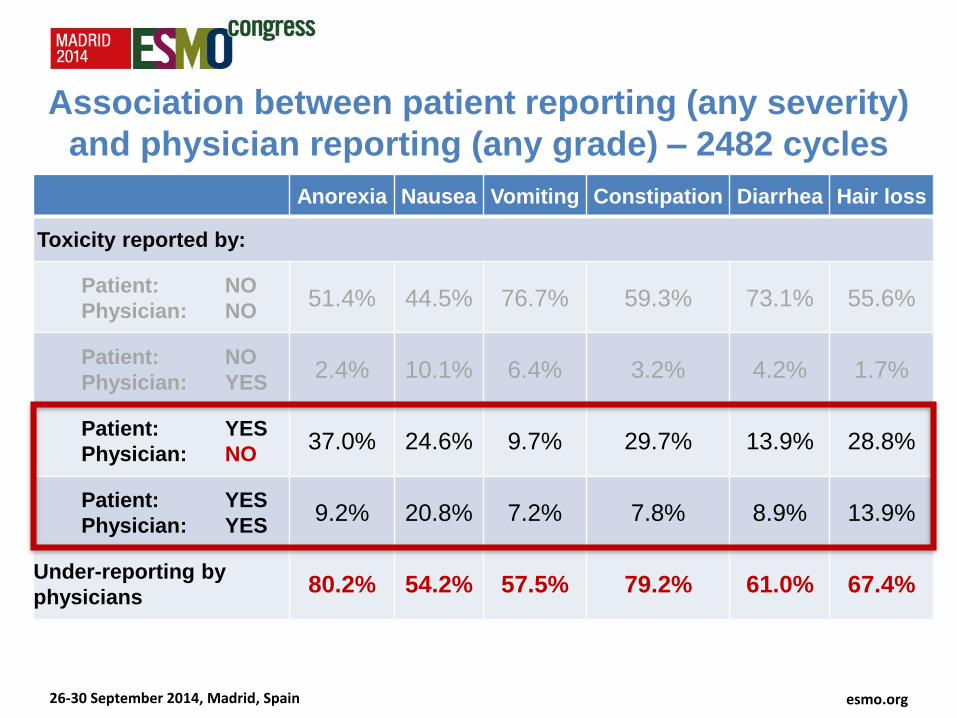
Association between patient reporting (any severity)
and physician reporting (any grade) – 2482 cycles
* ĸ>0.75: excellent agreement; ĸ=0.40-0.75: fair to good agreement; ĸ<0.40: poor agreement.(Fleiss JL . New York: John Wiley 1981)
26-30 September 2014, Madrid, Spain esmo.org
Anorexia Nausea Vomiting Constipation Diarrhea Hair loss
Toxicity reported by:
Patient: NO
Physician: NO51.4% 44.5% 76.7% 59.3% 73.1% 55.6%
Patient: NO
Physician: YES2.4% 10.1% 6.4% 3.2% 4.2% 1.7%
Patient: YES
Physician: NO37.0% 24.6% 9.7% 29.7% 13.9% 28.8%
Patient: YES
Physician: YES9.2% 20.8% 7.2% 7.8% 8.9% 13.9%
Under-reporting by
physicians80.2% 54.2% 57.5% 79.2% 61.0% 67.4%
Association between patient reporting (any severity)
and physician reporting (any grade) – 2482 cycles

Points of Relevance
• Separate i-v vs p.o. agents• Underestimation of acute and delayed N/V• Combination of drugs. Usually the most
emetogenic agent. Separate category AC.• Palonosetron: prolonged half life: delayed emesis• Olanzapine• NK1-RA: Netupitant. NEPA > Palo-dex in HEC and
AC, over multiple cycles• Rolapitant: half-life 180h, CYP3A4; (+ CYP2D6: P-
glycoprotein PG-170)• Genetics of N/V: CYP, MDR- PGP, SNPs ethnicity…

Take Home
• HEC: 3 drug combo: NK-RA, 5HT3-RA, Dexa, if no NK1-RA available, Palo preferred
• MEC: 5HT3-RA (Palo preferred) + Dexa
• Low: single: dexa or 5HT3-RA
• Refractory: different group, check dose, olanzapine in HEC
• Anticipatory: Balint, anxiolytics, cannabis…?



R. Navari: Oncology Journal March 15, 2018

Case Study
• 31 year old female patient presents withabdominal discomfort and back pain.
• CT-Scan: abdominal-retroperitoneal mass, 15 cm diameter, vascular structures in vicinity, level of ombilicus.
• Tumor board:
- Preoperative Radiotherapy: 50 Gy

N/V prevention?
• 1. No antiemetic
• 2. 5HT3-RA before each RT +5d dexamethasone
• 3. 5HT3-RA before, 5 d dex optional
• 4. 5HT3-RA optional, if necessary

• 2. 5HT3-RA + dex

• Tolerance excellent. Tumor mass regressed to 6cm on control CT. Surgery is performed. Clips left in place at resection borders.
• Histology: leiomyosarcoma, grade 3, no nodal involvement, some microscopic necrosis, no vascular invasion, no R0, involved margins.

• Tumor Board:
1. Additional Radiotherapy, e.g. 20-24 Gy
2. Chemotherapy: CYVADIC, Adria- Ifosfamide
3. Pazopanib, Regorafenib

Chemotherapy: CYVADIC
• 1. 5HT3-RA + dex
• 2. 5HT3-RA, NK1 +dex
• 3. 5HT3-RA

Chemotherapy: Adria- Ifos
• 1. 5HT3-RA + dex
• 2. 5HT3-RA, NK1 +dex
• 3. 5HT3-RA

Radiotherapy
• 1. 5HT3-RA + dex
• 2. 5HT3-RA
• 3. Metoclopramide + dex
• 4. Antiemetic if necessary
• 5. 1 + 3 are correct

Targeted Treatment
• 1. 5HT3-RA, NK1 + dex
• 2. 5HT3-RA +dex
• 3. 5HT3-RA
• 4. Dex
• 5. None
• 6. 1-4 are correct


Immuno-oncology
Pictures: courtesy of Dr. Mario Lacouture, MSKCC NY. NY.

ESMO guidelines



Weber et al. ASCO 2015
Nivolumab(n=474)

Minkis et al, JAAD 2013; Photo courtesy of Prof A Hauschild; Robert et al, NEJM 2015; Hamid et al, NEJM 2013; Margolin et al, Lancet Oncol 2012; Rosenberg et al, Lancet 2016
Maculopapular rash
• Incidence
• Ipilimumab:19%
• Nivolumab: 34%
• Ipi+nivo: 40%
• Pembrolizumab: 39%
• Atezolizumab: 10%
• Treatment
• Grade 1/2
• Oral Antihistamines
• Top Steroids
• Grade 3
• PO steroids
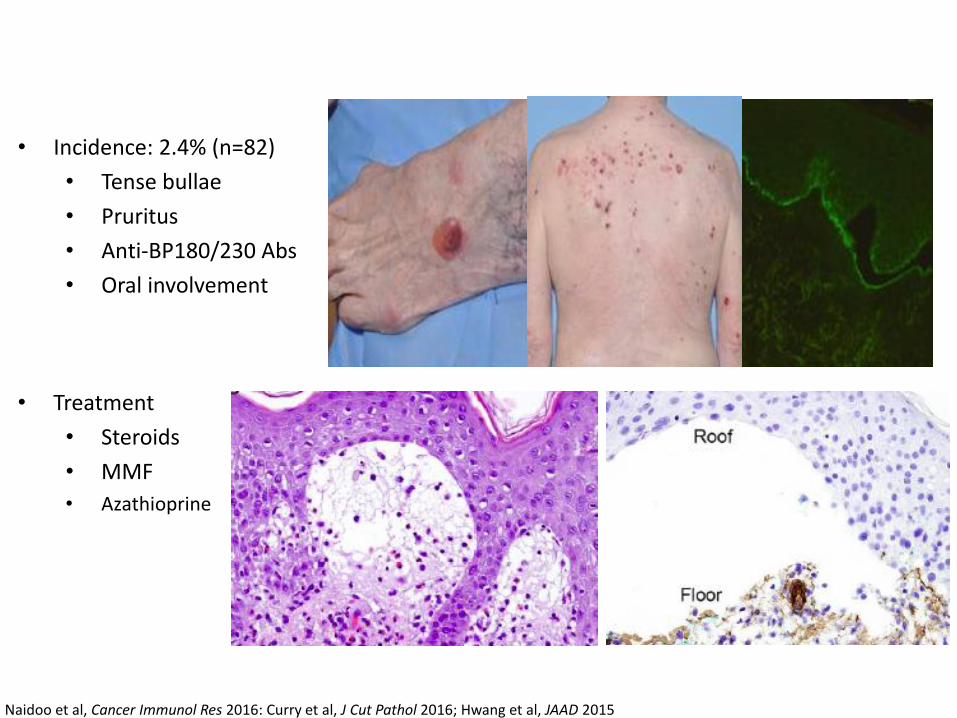
• Incidence: 2.4% (n=82)
• Tense bullae
• Pruritus
• Anti-BP180/230 Abs
• Oral involvement
Naidoo et al, Cancer Immunol Res 2016: Curry et al, J Cut Pathol 2016; Hwang et al, JAAD 2015
• Treatment
• Steroids
• MMF
• Azathioprine

Dermatomyositis (n=3) Psoriasis (n=21)
Lacouture , unpublished; Bonigen et al, 2016; Sibaud et al ,2016

Keratoacanthomas (n=4)
Lacouture , unpublished; Bonigen et al, 2016; Sibaud et al ,2016
Rosacea (n=3)
H&E
CD4
CD8

• Incidence
• Ipilimumab: 4%
• Nivolumab: 17%
• Ipi+Nivo: 33%
• Pembrolizumab: 21%
• Atezolizumab: 7%
Ensslin et al, JAAD 2014; Sanlorenzo et al, 2014Valentine et al, JAAD 2015; Santoni et al, 2015; Rosenberg et al, 2016
Excoriations

Santini et al, Lancet Oncol 2012
• First line therapy for pruritus:
• PO antiH1/steroids
• Topical steroids/anti pruritics (menthol, pramoxine)
• 93% of patients responded to aprepitant (>50% reduction in pruritus)
• Median duration of one cycle effect 30 days (range 7-90 days), >50% did not recur
Patient-reported Pruritus

Robert et al, NEJM 2015; Hamid et al, NEJM 2013; Margolin et al, Lancet Oncol 2012; Hua et al, JAMA Derm 2015
Pembrolizumabn=67
Vitiligo

1

2
VTE

Risk Factors for VTE
• Previous venous thromboembolism
• Increased age
• Surgery
• Trauma - major, local leg
• Immobilization - bedrest, stroke, paralysis
• Malignancy and its treatment (CTX, hormonal..)
• Heart or respiratory failure
• Estrogen use, pregnancy, postpartum, SERMs
• Central venous lines
• Thrombophilic abnormalities

Risk Factors for VTE
• Previous venous thromboembolism
• Increased age
• Surgery
• Trauma - major, local leg
• Immobilization - bedrest, stroke, paralysis
• Malignancy and its treatment (CTX, hormonal..)
• Heart or respiratory failure
• Estrogen use, pregnancy, postpartum, SERMs
• Central venous lines
• Thrombophilic abnormalities

Relative Risk of VTE in Cancer Patients
Stein, Am J Med, 2006





« Markers » of Duration of VTE treatment
• D-dimer
• Tissue Factor
• Residual Venous thrombosis on compression US


Ambulatory Prophylaxis of VTE in Cancer Patients
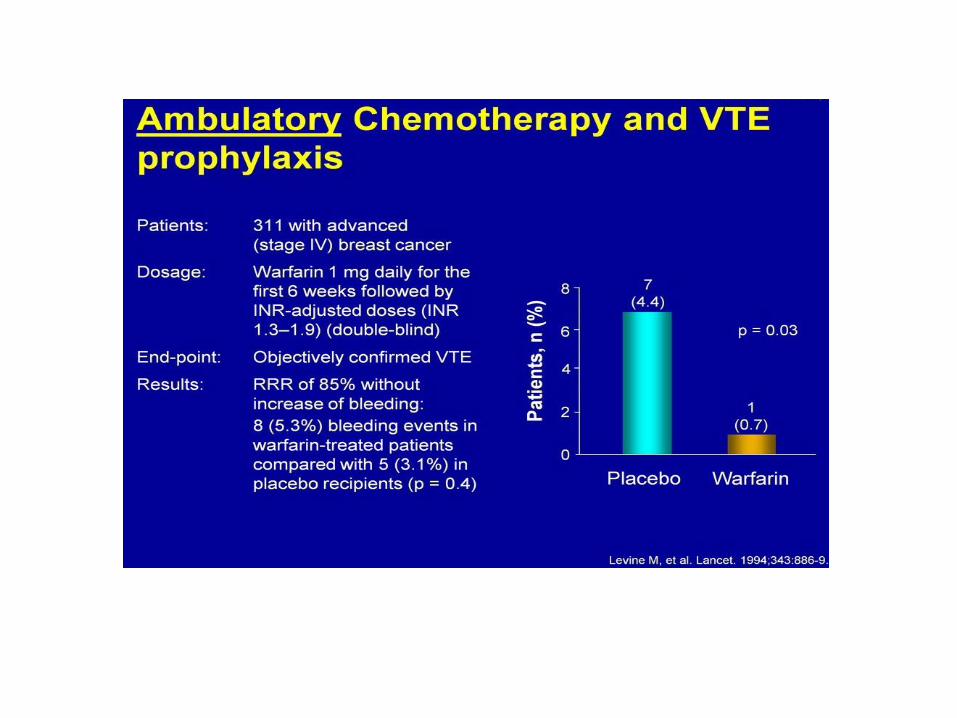

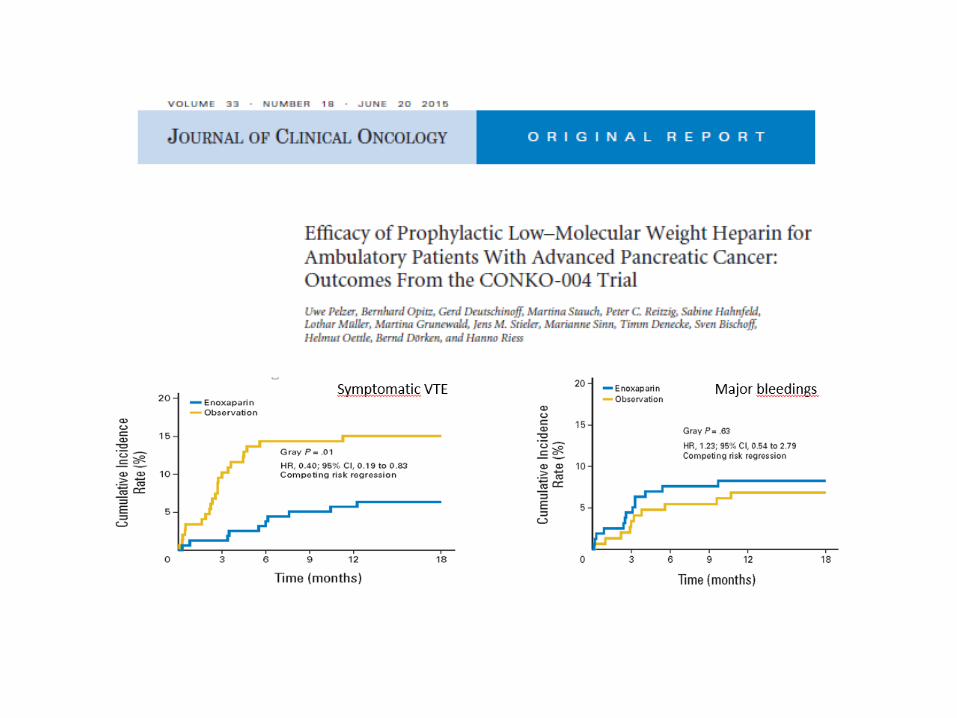

U. Pelzer et al :CONKO- 004 Trial , JCO 2015

• Open label unblinded randomized study
• No baseline screening at study entrance
• No stratification for chemo agent (cDDP -> VTE..)
• Pancreatic Ca: 43% of patients no other risk factor versus others with risk factors:
- VTE: 2.6% if no other risk factor vs 6.3% if one or 10.5% >1 risk factor.

Novel Anticoagulants
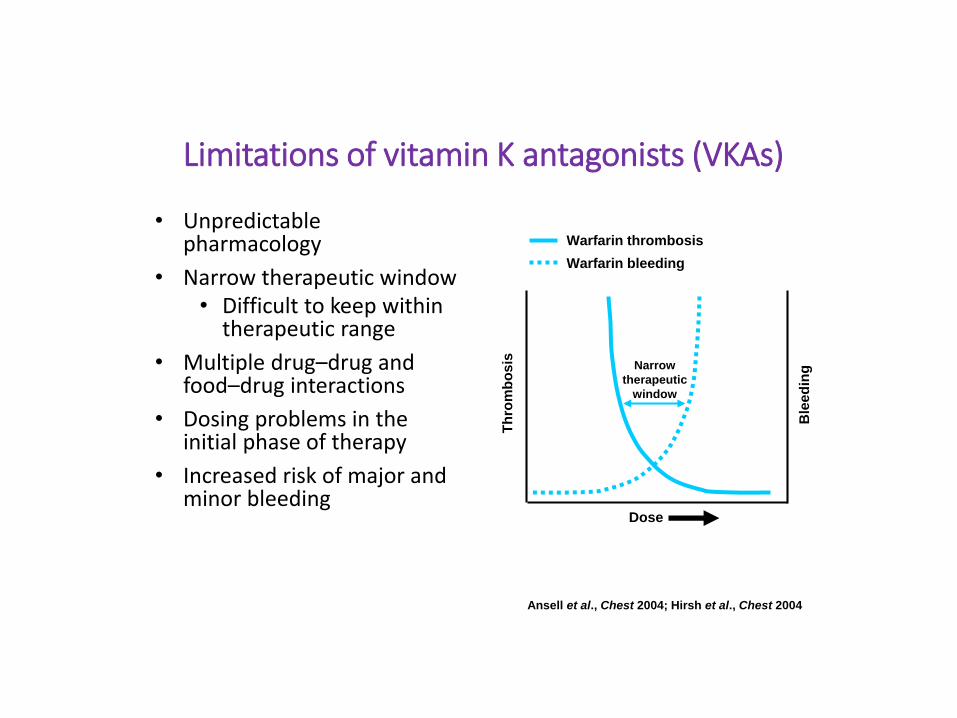
Limitations of vitamin K antagonists (VKAs)
• Unpredictable pharmacology
• Narrow therapeutic window• Difficult to keep within
therapeutic range
• Multiple drug–drug and food–drug interactions
• Dosing problems in the initial phase of therapy
• Increased risk of major and minor bleeding
Warfarin thrombosis
Warfarin bleeding
DoseT
hro
mb
osis
Ble
ed
ingNarrow
therapeutic
window
Ansell et al., Chest 2004; Hirsh et al., Chest 2004

Percentage of Patients in therapeutic range (INR 2-3) with Coumarins
•Warfarin ~ 45% at 4 weeks ( S.Kimmel NEJM 2013)
•Acenocoumarol & Phenprocoumon ~60% at 10 weeks (T Verhoef NEJM 2013)

Limitations of prolonged LMWH
• Daily injections
• Platelet monitoring
• HIT
• Cost: 8- 16 €
• Nurse (?)
• Bruising- hematomas
• Difficult to use over prolonged periods
• Recurrent VTE: 5% to 7% at 3 or 6 months
• Bleeding risk 5% to 7% not lower than VKA
New Anticoagulants
• FXI-ASO: FXI antisense oligonucleotide
• Semuloparin
• Oral: Dabigatran
Rivaroxaban
Apixaban
Edoxaban

FXI-ASO (ISIS Pharmaceuticals) 2e generation diminishes synthesis of FXI
N=300 pts. Knee replacement, Venography
FXI-ASO (200 vs 300mg) vs enoxaparine 40mg/j:
• Result similar for 200mg vs enoxaparine.
• For 300mg vs enoxaparine:
- VTE 3/71pts (4%) vs 21/69 (30%), p<0.001.
- Bleeding 3% vs 8%
➢ Antithrombotic with low risk of bleeding
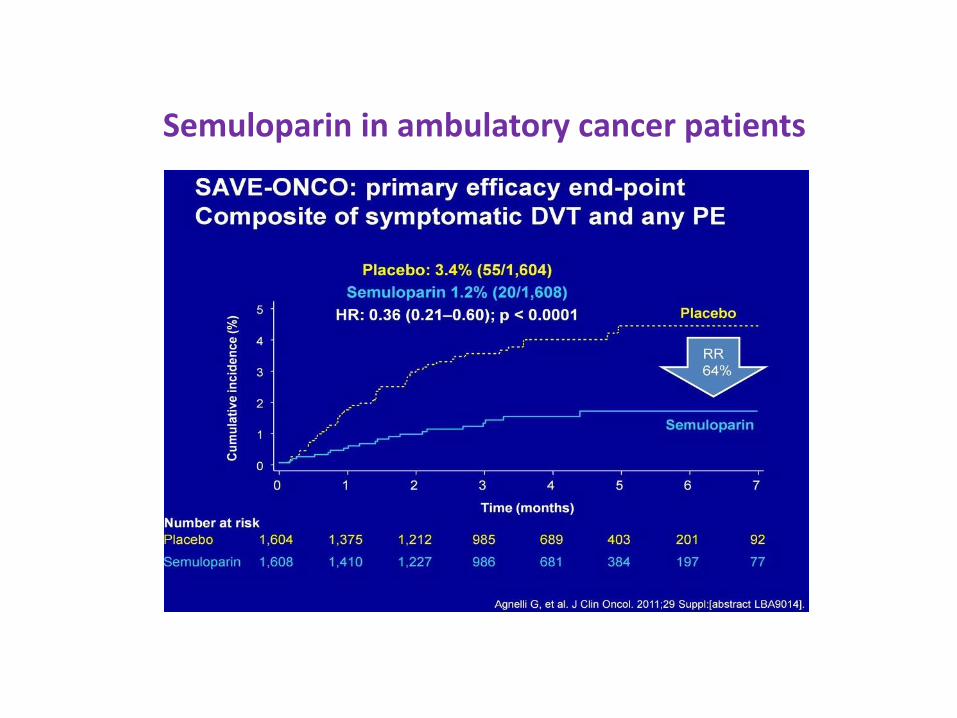
Semuloparin in ambulatory cancer patients

Slide 12
Presented By Stephan Moll at 2016 ASCO Annual Meeting

Novel oral anticoagulants
- Comparator non-inferiority studies on NOAC have been done with short initiation LMWH followed by AVK. No direct comparison with LMWH
- Treated cancer patients are small subgroups of patients within the general medical population treated.
- Specific Ca patient studies on-going NOAC vs LMWH

Slide 49
Presented By Stephan Moll at 2016 ASCO Annual Meeting

Abstract 625: Prospective randomised open label trial comparingDalteparin (D) to Rivaroxaban ®N= 406 patients
• Recurrent VTE: 11% vs 4%• Major bleeds: 6/6 vs 9/8 patients• Clinically relevant non major bleeds: 5/5 vs 28/27 patients

ASH 2017: Select-d trial: Rivaroxaban vs Dalteparin in
• N= 406 patients
• At 6 months: recurrence R vs D 4% vs 11%
major bleeding: R vs D 9 vs 6
clinically relevant non major bleeding: 28 vs 5
major + clin relev. R vs D: 37 vs 11 bleeds ( 35 vs 11 patients)

• Open label, non inferiority study comparing Edoxaban (E) to Dalteparin (D). N= 1046 pts.
• Primary event: E vs D: 62/522 (12,8%) vs 71/524(13,5%).
p= 0.006 for non-inferiority, 0.87 for superiority
• Recurrent VTE: E vs D: 41(7.9%) vs 59(11.3%)
• Major bleeding 36(6.9%) vs 21(4%)

Hemostasis: Case Study

• 62 y old Caucasian male with non-valvular atrial fibrillation is on rivaroxaban since 2010 and doing fine.
• 2012: Colorectal cancer with liver metastases is diagnosed. The patient is given chemotherapy (FOLFOX) and after 4 cycles is on partial remission but not resectable.
• Before his 5th cycle (to be switched to FOLFIRI), a diagnosis of left leg DVT is made.
• What to do?
Slide 1

1. Increase dosage of rivaroxaban?
2. Switch to AVK
3. Switch to LMWH followed by AVK?
4. Only LMWH?
Slide 2
• The patient was treated with LMWH only
• He continued his chemotherapy and while on LMWH for 2 months, he had again a DVT.
• What next?
Slide 3
1. Increase dose of LMWH?
2. LMWH 2x/day?
3. Inferior Vena Cava filter?
4. 1 & 3
Slide 4

• The patient had a retrievable IVC filter and LMWH once daily.
• 10 weeks after insertion of filter, the patient is doing fine with LMWH, on chemotherapy.
• Cancer regressed and the patient has become operable. After surgery the patient is still on LMWH.
• Complete remission from CRC.
• LMWH is given now for 6 months postoperatively. To be given for how long?
Slide 5

Slide 6
1. Indefinitely ?
2. If patient remains in complete remission, to be stopped after x more months and switched to rivaroxaban?

• It was decided, following also the patient’s request, to stop LMWH after 3 more months and go back to rivaroxaban. The IVC filter was retrieved. The patient is fine.
• The patient, always in complete remission, now February 2016, wants to visit his nephew in Canada.
• His wife had a DVT after hip replacement 2 years ago. Does she need anticoagulation for the journey?
Slide 7
« Economy Class Syndrome »
1. Does not exist?
2. It is a reality?
3. May exist sometime?
Slide 8
If it exists. What to do?
1. LMWH
2. Rivaroxaban
3. ASA
4. 1 & 3 are correct
5. 1, 2 & 3 are correct
6. If it does not exist, no therapy is necessary.
Slide 9

Economy Class Syndrome Traveler’s VTE
• If risk factor and long distance (>4h), consider Rp
• No ASA?
• (NEJM: T. Brighton 2012, Nov 4, 2012: Low dose aspirin to prevent recurrent Venous thromboembolism)
Slide 10


• We gave aspirin. The couple had an uneventful trip.
• March 2018: the patient is in complete remission
• This is a real patient’s history
• I thought at some point making up this patient’s wife as a femalepatient with breast cancer and bringing in a hormone story, but as you have stood through a whole program so far, we’ll leave it at thatand
Slide 11

Financial ToxicityESMO grades for drug benefit in PFS and/or OS
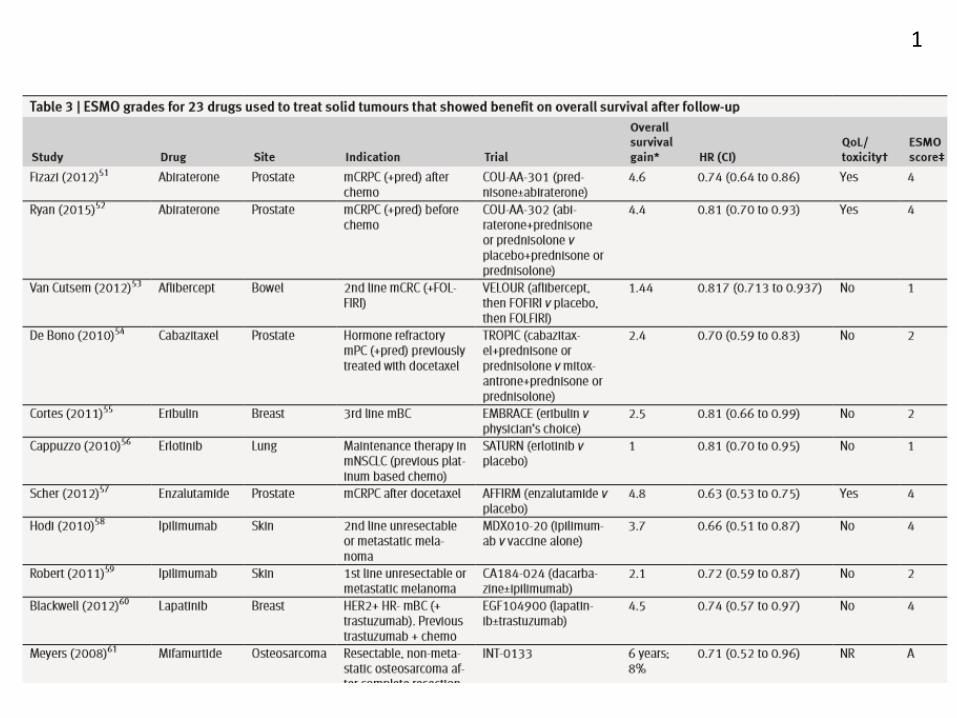
1

2

3


2nd Edition


Fertility in Cancer Patients

Berrington de Gonzalez A. et al.: BodyMass Index and mortality among 1,46 million white adults N. Engl. J. Med 2010

BMI HR
« Normal » 18.5-<25 1.00
0verweight 25-<30 0.94
Obesity grade 1 30-<35 0.95
Obesity grade 2+3 =>35 1.29
All cause mortality, corrected for smoking, no cause-specific mortality