e-poster13 rusza aimradial20170922 hybrid approach
Upload: international-chair-on-interventional-cardiology-and-transradial-approach
Post on 21-Jan-2018
310 views
TRANSCRIPT

Zoltán Ruzsa MD PhD

Speaker's name: Zoltan Ruzsa
I do not have any potential conflict of interest to report:
Potential conflicts of interest

Access site selection for lower limb interventions
0
50
100
150
200
250
300
350
1 2 3 4 5 6
Femoral
Radial
Brachial
Dual- Radial + Femoral
Dual- Radial + Transpedal
Dual- Femoral + Transpedal

Background
• Limited data exists in the literature about transradial femoral interventions 1,2.
• The purpose of this pilot study was to evaluate the acute success and complication rate of the transradial access for femoral artery intervention.
1. Lorenzoni R et al. J Endovasc Ther. 2014 Oct;21(5):635-40.
2. Lorenzioni R et al. EuroIntervention. 2011 Dec;7(8):924-9.
3. Hanna EB, Prout DL. J Endovasc Ther. 2016 Apr;23(2):321-9.

Routine access site selection-femoral
- Multilevel diseaseIliac + Femoral + BTK
- Distal stenosis- Non diseased
CFA- Popliteal lesion
Anterograde femoral
- SFA stenosis close to the CFA
- Diseased CFA
Cross overpossible
Brachial or radial access
No cross over-Scar-Bypass-Stents in the iliac ostium-Extreme angulation-Extreme tortuosity
Is there a place for primary radial
access for femoral artery intervention
???
Cross over
- Complex CTO(failed antegrade)
Popliteal or transpedal
yes
No
No No

Sheathless guidingCoronary SG 8.5 F 100 cmInternal D: 2.28 mm
External D: 2.8 mm
Peripheral SG 6F 120 cmInternal D: 2.29 mm
External D: 2.8 mm

Methods
The clinical and angiographic data of 141 consecutive patients with symptomatic femoral artery stenosis treated via transradial access using 6F sheathless guiding between 2014 and 2016.12 were evaluated in a pilot study.
Inclusion criteria:
•Significant, isolated femoral artery stenosis or occlusion
•Intermittent claudication (Fontaine IIa-b)
•Critical limb ischemia (crural ulcer, pedal gangrene, ischemic rest pain)
Exclusion criteria:
•Contraindication of the transradial access (negative Allen test, radial artery occlusion)
•Contraindication of the 6 F usage in the radial artery: very small radial artery (<2 mm) and severe calcification or stenosis
End points:
•Primary endpoint:
– major adverse events (MAE), – rate of major and minor access site complications.
•Secondary endpoints:
– angiographic outcome of the femoral artery intervention,
– consumption of the angioplasty equipment
– X Ray dose, procedural time, cross over rate to another puncture site and hospitalisation in days.

Methods: Angioplasty technique
• Medical therapy
- Transradial cocktail (NaHeparin5000 U and 2.5 mg Verapamil)
- Per os Aspirin and Clopidogrel
- Heparin up to 100 U/kg
• Patient positioning
– Right radial: Normal
– Left radial: Inverse
• Punction and cannulation
- Local anesthaesia and dedicated
5F TR sheath
• Diagnostic angiography
- 125 cm Pig tail catheter

Crossing the aortic arch
Easy aortic
arch
Difficult
aortic arch

Methods: Angioplasty technique
Cannulation of the iliac artery
- 6 F 120 cm Asahi sheathless guiding over a long Starter or
Extra-support 0.035 GW (Jindo, Amplatz)
- 6.5 F 90 cm Asahi sheathless coronary guiding catheter over a
long Starter or Extra-support 0.035 GW
- Telescoping technique with a MP 125 cm 5F catheter
Angioplasty
-„Road map imaging”
- Balloon angioplasty with long inflations (2-3 min)
- Focal stenting (Optimed stent with 180 cm long shaft)
- Long 300 cm 0.18 or 400 cm 0.18 GW (Roadrunner, Cook)
- Alternative access site is the popliteal or transpedal access for
stenting----For DEB or DES and Stent with high radial force
(Supera)
- Femoral access site only in bail out cases
- Final angio
Postop treatment
- Non occlusive pressure bandage
- Immediate mobilisation

Femoral arteryCTO

Demographic and clinical data n (%)
Demographic data Age (years)
Male
Hypertension
Current smokers
Diabetes mellitus
- IDDM
- NIDDM
Weight (kg)
Height (cm)
Chronic obstuctive pulmonary disease
Renal insuffitiency
67.6 ± 9.8
89 (63.1)
136 (96.5)
22 (15.6)
74 (52.5)
25 (17.7)
49 (34.8)
79.4 ± 16.6
168.0 ± 8.2
8 (5.7)
31 (22)
Cardiac and vascular history CAD
Previous PTA
Previous bypass
Previous major amputation
PAD
- IC
- CLI
- ALI
47 (33.3)
52 (36.9)
15 (10.6)
0 (0.0)
57 (40.4)
82 (58.2)
2 (1.4)
Fontaine classification I
IIa
IIb
III
IV
0 (0)
11 (7.8)
45 (31.9)
34 (24.1)
51 (36.2)

Results- Angiographic dataAngiographic and procedural data n (%)
Quantitative measurements
Common femoral artery
Diameter stenosis (%)
Lesion length (mm)
Reference diameter (mm)
Superficial femoral artery
Diameter stenosis (%)
Lesion length (mm)
Reference diameter (mm)
Popliteal artery
Diameter stenosis (%)
Lesion length (mm)
Reference diameter (mm)
12.3 (29.3)
6.2 (19.7)
5.8 (0.8)
79.4 (27.6)
82.2 (67.2)
5.5 (0.6)
14.2 (33.4)
9.2 (28.6)
4.6 (0.5)
Angiographic and procedural data n (%)
Lesion type
Chronic total occlusion (%)
TASC A
TASC B
TASC C
TASC D
66 (46.8)
74 (52.5)
32 (22.7)
14 (9.9)
21 (14.9)
Angiographic result of the intervention
Successful
-Good result
-Satisfactory result
Unsuccessful
128 (87.2%)
11 (7.8%)
7 (5%)

Results- Procedure
Primary Access:
- Radial n=138 (97.9%)
- Ulnar n= 3 (2.1%)
Side:
- Right side n= 114 (80.8%)
- Left side n= 27 (19.2%)
Secondary Retrograde Access (DUAL):
- Popliteal and AFS n= 4 (2.8%)
- Pedal n= 14 (9.9%)
Cross over to Anterograde Femoral
- to femoral n=4 (2.8%)

Results- technique and devices
• POBA: 107 (75.9%)• 5 pts retrograde IMPACT
• Stenting: 34 pts (24.1%)• Anterograde 22 pts (64.7%)
• Retrograde 12 pts (35.9%)• 10 Supera
• 2 Zilver PTX

Results – Impact of the side selection
Left hand access
(n= 27)
Right hand access
(n= 114)
Procedure time (min) 35.5 27.7-43.3 34.9 30.3-39.5
Fluroscopy time (sec) 806.7 554.8-1059 723.2 601.7-844.8
X Ray dose (Gy) 14.09 10.4-17.7 23.5 8.3-38.6 ★
Contrast consumption (ml) 107.6 84.5-130.6 114.3 101.2-127.4
Advantage of the left hand access:
- Easy access to the descendentic aorta
- Shorter delivery system is necessary

Long term follow up• MAEs at 12 months: 33 pt (23.4%)
•TLR at 12 months: 10 pts (7.1%)
•Another PTA at 12 months: 17 (12.1%)
MAE (MACCE+ TLR + Amp) n (%)
- Death- AMI- Stroke- Amputation- rePTA- MAE- ALL MAE
10 (7.1)1 (0.1)2 (1.4)10 (7.1)10 (7.1)37 (26.2)33 (23.4)
MAE (n=33) n (%)
- IC- ALI- CLI
10 (30.3)1 (3)21 (63.6)

POC n (%)
Procedural complications - Distal embolisation
- Edge dissection and additional stent
Renal failure
Summary
1 (0.7)
5 (3.5)
0 (0)
Access site complications
Minor
RAO
Compartment syndrome Spasm
Perforation
Major
Summary
3 (2.1) 0 (0)
0 (0)
0 (0)
0 (0)
3 (2.1)
Perioperative complications

Limitations of the study
- The main limitation of the study is the lack of femoral control group
- It is not a randomized study
• Technical limitation:
– We haven’t drug eluting balloons and stents with long shaft length, therefore for these cases the transpedal and transpoplitealaccess must be prepared
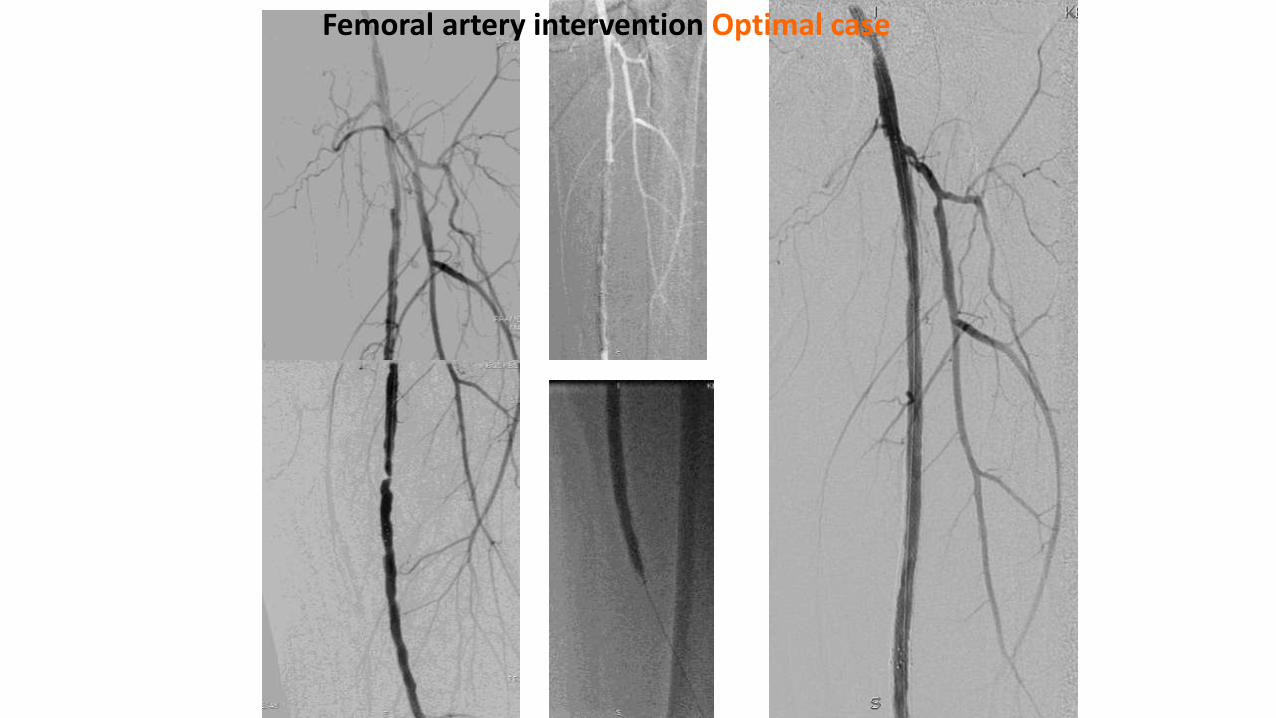
Femoral artery intervention Optimal case

Access ??- iliac stent- diseases CFA-Long SFA CTO-Popliteal CTO- ATA and ATP occl
TR access
-6F SG
-V18 GW 300
-Treasure12 300
-Invatec 5x150 180
-Invatec 6x150 180
-Optimed 6x80 180
Peroneal access
-Cook 4F
-Progress40 300
-Fox 4x80
Difficult case
-Multilevel
-Long CTOs

Patient with CCS 3 angina and rest pain


Right SFA recanalisationRight ulnar artery access
6F 120 cm SGStarter GWV18 GWPacific 180 cm 5x150 mm


Zilver PTX 6x120 mm

CASE – Pt with CLI and SFA occlusion






Conclusion• Femoral artery angioplasty can be safely and
effectively performed using radial access andsheathless guiding with acceptable morbidity and hightechnical success.
• Although complication rates of the present pilotregister are promising, larger studies are needed todetermine the long term success rate of transradialfemoral PTA.

Thank you for your attention !!!