early history of methylene blue
TRANSCRIPT

7/21/2019 Early History of Methylene Blue
http://slidepdf.com/reader/full/early-history-of-methylene-blue 1/6268
ReflectionsScience in the cultural context
In 1906, Alois Alzheimer, togetherwith Emil Kraepelin and two Italian
colleagues, studied the brain of a
deceased patient suffering from pro-found short-term memory loss anddementia. They observed the cerebralcortex was smaller than normal andidentified, in stained sections, fibrousaggregates of protein, more com-monly called amyloid plaques. Laterthat year, Alzheimer presented the firstevidence of observable brain pathology associated with mal-functioning cognition and dementia, yet it was Kraepelin whofirst referred to the pathophysiology as Alzheimer’s disease(AD) (1).
An estimated 26.6 million people worldwide have AD;this number may quadruple by 2050 (1); in the US alone,there are thought to be 4.5 million afflicted patients (2).
Establishing a therapy that would delay the onset of AD byonly one year would save $9 billion in the US alone (3).
Recently, results from a clinical trial, presented at the 2008International Conference on Alzheimer’s Disease (ICAD),showed that an investigational drug was capable of arrestingprogression in mild and moderate AD (4, 5). Enthusiasm mustbe tempered, as the study involved relatively few patientsand the results must be confirmed by more extensive trials.Nevertheless, this was the first intervention ever to arrest theinexorable progression of AD.
Alois Alzheimer
7/21/2019 Early History of Methylene Blue
http://slidepdf.com/reader/full/early-history-of-methylene-blue 2/6 2 December 2008
Volume 8, Issue 6
On reading this news, the first question to come to mind was:what is the identity of the investigational drug? The answercame as a stunning surprise. Not a bioengineered protein,
not a monoclonal antibody, not a new synthetic compoundspecially designed to fitsnugly into an enzyme’spocket, the drug can-didate is a dye knownsince 1876: methyl-thioninium chloride, ormethylene blue (MB).
Despite a long and varied history, MB has fallen into obscu-rity. Its rebirth might come soon: if further clinical research
yields favorable results, MB may become a compound of sur-
passing interest to scientists and lay persons alike. It thereforeseems appropriate to review its 130-year medical history andexplore the rationale for its possible effectiveness against AD.
Early History of Methylene BlueMethylene blue is made by reacting N,N-Dimethyl-p -phenylenediamine in acidic medium with hydrogen sulfideand ferric chloride. The sulfur atom bridges two moleculesof the phenylenediamine, forming a phenothiazine, and isoxidized by the ferric ion to a positively charged thioniumion. For industrial use as a dye, MB is supplied as a doublechloride with zinc; for bacteriologic and medicinal uses thezinc-free form is employed.
First synthesized in 1876, concomitant with the beginningsof bacteriology, MB found immediate use in the staining ofmicroorganisms, and its effect on bacterial metabolic behav-iors was also studied. MB became an early research interestof Paul Ehrlich, who would later participate in developingdiphtheria antitoxin, concocting the first chemotherapy forsyphilis (salvarsan), and enunciating the receptor theory ofantibody action. Ehrlich made the important observation that
in some tissues, MB was reversiblyreduced to a colorless (leuco-) form.He also found that it possessed
a selective affinity for nerve cellsand nerve fiber endings, a find-ing which may have significancein today’s context. Reasoning thatit might therefore interfere withconduction of pain impulses by thenerves, Ehrlich obtained a supplyof purified MB and, together with
a physician named Lippmann, conducted a clinical trial inpatients with neuralgia and arthritis (6). MB produced ananalgesic effect but it tended to damage the kidneys if usedcontinuously (7).
MB as an Antimalarial
Noting that malaria-causing Plasmodia were stained by MBand that the dye seemed safe for short-term administration,
Ehrlich and Guttmann, in 1891, administered MB as a treat-ment for malaria, on two patients in a Berlin hospital. Theresults were positive, though not equal to those with quinine(6). Still, the desirability of another antimalarial, lacking qui-nine’s side effects and usable by patients unable to toleratequinine, led to further trials by other physicians. In 1904,Horatio C. Wood, Jr. performed what today would be calleda meta-analysis ofthe clinical resultspublished as of thatdate. Reviewing425 cases (including
Ehrlich’s two) gleanedfrom eleven publishedreports, he concludedthat 362 (85%) werefinal cures, whereasthirty-one sufferedrelapses (8).
Although the search for antimalarials focused on syntheticsubstitutes for quinine, physicians still turned to MB under cer-tain conditions. Thus, a report from World War II–era SovietUnion described the treatment of forty patients with a typeof malaria that had proved refractory to repeated courses
of quinine. Treatment consisted of five or six intravenous (iv)infusions of 15-20 mL of 1% MB in 25% glucose. In most ofthese patients, fever was terminated after the first or secondinfusion and attacks did not recur. In twenty of the thirty-fivepatients in whom plasmodia had been seen, the organ-isms disappeared from the peripheral blood. The authorconcluded that MB has a definite role when the patient isquinine-intolerant or does not respond to quinacrine and plas-moquine (9).
More recently, the antiplasmodial activity of MB was con-firmed in vitro by Vennerstrom et al. whereby several dyeswere tested against three different strains of
P. falciparum,
each having a different drugsusceptibility/resistance pro-file. Dyes of the xanthine,azine, oxazine, and thiazinecategories were tested. Thethiazine (phenothiazine) dyeswere found to be the mostactive antimalarials whileshowing low cytotoxicity––MBwas among the most potentof this group (10).
Paul Ehrlich
H3C
CH3
Cl–
Methylene blue
S+S+
NN
NNNN
CH3
CH3
C r e d i t : S m i t h s o n i a n I n s t i t u t i o n
Anopheles gambiae , bearer of malaria
Plasmodium falciparum
Something Old... Something Blue

7/21/2019 Early History of Methylene Blue
http://slidepdf.com/reader/full/early-history-of-methylene-blue 3/6270
Reflections
MB and Antimalarial Synthesis
MB’s main contribution to the cure of malaria lies not in itsdirect use in therapy, but in serving as a template for the
synthesis of substitutes for quinine. Sneader (11) relates thatEhrlich had suggested making derivatives of MB as possiblyimproved antimalarials. He was prevented from pursuing hisidea, first, because no animal model for malaria existed atthe time on which compounds could be tested, and second,because he became involved in research on diphtheria anti-toxin [see (12) for historical details of mushing the antitoxinto Nome].
Only in 1924 did a screening method, using canaries,become available. Werner Schuleman and colleagues at I. G.Farben then took up Ehrlich’s suggestion. By substituting a
diethylaminoethyl (DEAE) side chain for one of MB’s methylgroups, they obtained a promising compound, but as it wasdeeply colored, they felt it might be unacceptable to patients.Schuleman’s group substituted quinoline for the phenothiazinenucleus, retained the DEAE side chain, and added some fea-tures of the quinine structure. Of the hundreds of compoundsprepared, the first clinically tested and marketed compoundwas Plasmoquine (pamaquine). Thus, the first synthetic drugdesigned as an antimalarial derives partly from MB (11).
A Urinary Antiseptic PrescriptionBecause it possesses antibacterial activity and is secreted intothe urine, MB is a key ingredient in a combination product
for treating infections and painful disorders of the urinarytract. This product is remarkable for its longevity: it predatesthe New Drug Application requirement of the 1938 Food,Drug, and Cosmetic Act, and is still on the market today.
Originating in an era when physicians were accustomed towriting multi-ingredient prescriptions (termed polypharmacy),the product resembles such a prescription. In addition to 5.4mg of MB, each tablet contains atropine sulfate 0.03 mg,hyoscyamine 0.03 mg, methenamine 40.8 mg, benzoic acid5.4 mg, and phenyl salicylate 18.1 mg (13). The atropineand hyoscyamine, both parasympatholytic alkaloids, were
intended to relieve the pain of smooth muscle spasms in theurinary tract. Methenamine, a complex compound made bycondensing formaldehyde with ammonia, was at one timehighly regarded. In acid medium methenamine breaks downinto its components; thus, if the urine is acidified (e.g., bybenzoic acid) the antibacterial action of free formaldehydewould be released. In the 1930s, methenamine was rec-ommended for many conditions, including pyelitis, cystitis,prostatitis, urolithiasis, gonorrhea, meningitis, and polio(14)––truly a wonder drug, had it worked! The rationalefor adding phenyl salicylate (salol) resided in its antisepticaction, as it contains insufficient salicylate for any analgesic
effect. This formula is on the market as Urised and Uriseptic,and in generic form as Urinary Antiseptic #2 (13).
Treatment of MethemoglobinemiaMB is used therapeutically for a relatively uncommon condi-tion wherein high concentrations of methemoglobin are pres-ent in the blood. Methemoglobin, an oxidation product ofhemoglobin in which the iron atom is in the ferric (trivalent)state, gives the blood a brown color but does not combinewith oxygen, thus reducing the oxygen-carrying capacityof the blood. Methemoglobinemia may be congenital, ormay be acquired, for example, from well-water containingnitrites or from drugs such as benzocaine and sulfonamides.MB acts through the MB–leuco-MB redox system. Upon ivinjection MB reacts
with reductases inerythrocytes, forming itsdihydro derivative, col-orless leuco-MB, whichcan reduce methemo-globin back to normalhemoglobin (15).
This use of MB was discovered long ago, and was wellestablished by the 1940s. In 1947, Bodansky and Gutmanninduced varying degrees of methemoglobinemia severity indogs. By correlating their animal data with results publishedin the clinical literature they confirmed that an iv dose of
1-2 mg/kg of MB is rapidly effective against the symptomsof severe methemoglobinemia (16). In 1993, Eldadah andFitzgerald recommended that methemoglobinemia be treatedby iv administration of 1-2 mg/kg of MB as a 1% solution,infused over fifteen minutes. A second dose may be given,up to a maximum of 7 mg/kg/24 hrs (17). Methylene BlueInjection, a 1% sterile solution of MB, is officially recognizedin the United States Pharmacopeia (USP).
Drug Treatment of AD:
Present and Future
Currently Approved Drugs
The drugs currently used to treat AD patients act on brainneurotransmitters, although it is recognized that they do notaddress the cause. Some of the signs and symptoms of ADcan be attributed to a deficiency of cholinergic neurotrans-mission––part of the cholinergic system theory of AD. Thus,enhancing cholinergic function by inhibition of cholinesterasecould be helpful. Four AD drugs based on this mode ofaction have been developed. Cholinesterase inhibitors donot alter the course of the dementia but act to slow cognitivedemise. As AD progresses and fewer cholinergic neuronsremain functional, the effect of these drugs diminishes (18).
H3C
CH3
Cl–
SS
N+
N+
NN
NHNH
NN
CH3
Leucomethylene blue
(colorless, protonated form)
CH3
7/21/2019 Early History of Methylene Blue
http://slidepdf.com/reader/full/early-history-of-methylene-blue 4/6 2 December 2008
Volume 8, Issue 6
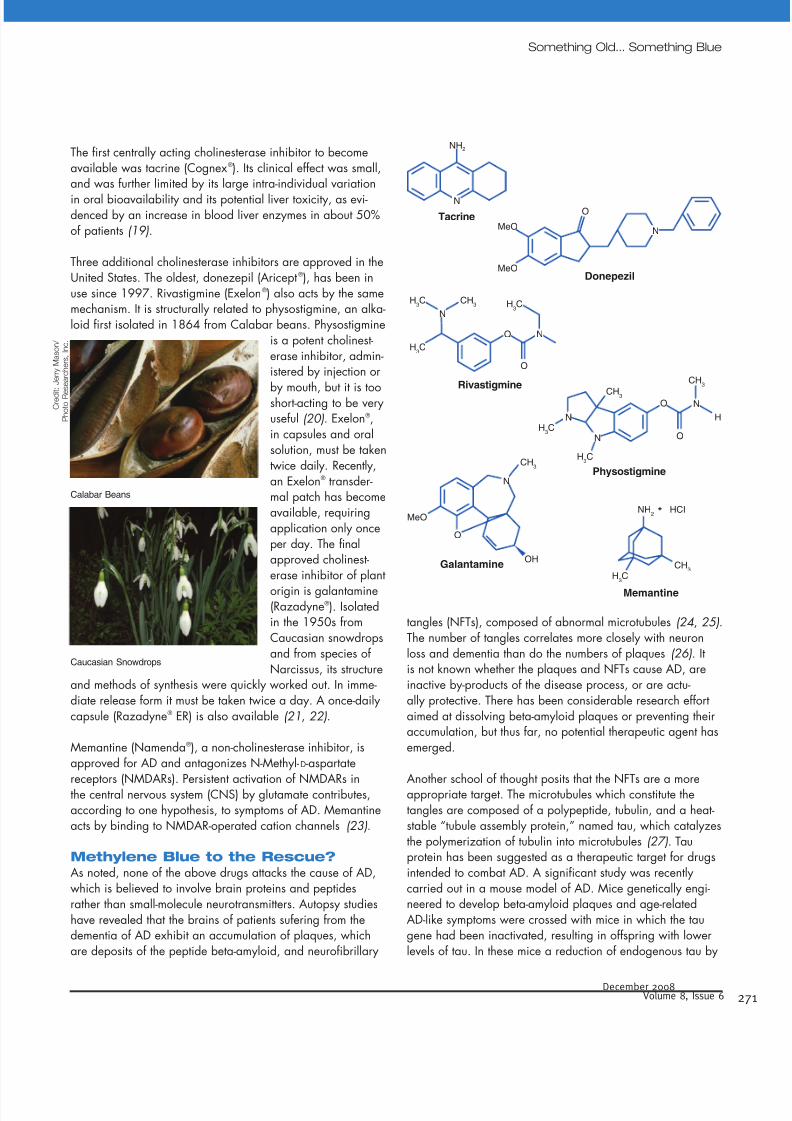
The first centrally acting cholinesterase inhibitor to becomeavailable was tacrine (Cognex®). Its clinical effect was small,and was further limited by its large intra-individual variation
in oral bioavailability and its potential liver toxicity, as evi-denced by an increase in blood liver enzymes in about 50%of patients (19).
Three additional cholinesterase inhibitors are approved in theUnited States. The oldest, donezepil (Aricept®), has been inuse since 1997. Rivastigmine (Exelon®) also acts by the samemechanism. It is structurally related to physostigmine, an alka-loid first isolated in 1864 from Calabar beans. Physostigmine
is a potent cholinest-erase inhibitor, admin-istered by injection or
by mouth, but it is tooshort-acting to be veryuseful (20). Exelon®,in capsules and oralsolution, must be takentwice daily. Recently,an Exelon® transder-mal patch has becomeavailable, requiringapplication only onceper day. The finalapproved cholinest-erase inhibitor of plant
origin is galantamine(Razadyne®). Isolatedin the 1950s fromCaucasian snowdropsand from species ofNarcissus, its structure
and methods of synthesis were quickly worked out. In imme-diate release form it must be taken twice a day. A once-dailycapsule (Razadyne® ER) is also available (21, 22).
Memantine (Namenda®), a non-cholinesterase inhibitor, isapproved for AD and antagonizes N-Methyl-d-aspartate
receptors (NMDARs). Persistent activation of NMDARs inthe central nervous system (CNS) by glutamate contributes,according to one hypothesis, to symptoms of AD. Memantineacts by binding to NMDAR-operated cation channels (23).
Methylene Blue to the Rescue?As noted, none of the above drugs attacks the cause of AD,which is believed to involve brain proteins and peptidesrather than small-molecule neurotransmitters. Autopsy studieshave revealed that the brains of patients sufering from thedementia of AD exhibit an accumulation of plaques, whichare deposits of the peptide beta-amyloid, and neurofibrillary
tangles (NFTs), composed of abnormal microtubules (24, 25).The number of tangles correlates more closely with neuronloss and dementia than do the numbers of plaques (26). Itis not known whether the plaques and NFTs cause AD, areinactive by-products of the disease process, or are actu-ally protective. There has been considerable research effortaimed at dissolving beta-amyloid plaques or preventing theiraccumulation, but thus far, no potential therapeutic agent hasemerged.
Another school of thought posits that the NFTs are a moreappropriate target. The microtubules which constitute thetangles are composed of a polypeptide, tubulin, and a heat-stable “tubule assembly protein,” named tau, which catalyzesthe polymerization of tubulin into microtubules (27). Tauprotein has been suggested as a therapeutic target for drugsintended to combat AD. A significant study was recentlycarried out in a mouse model of AD. Mice genetically engi-neered to develop beta-amyloid plaques and age-relatedAD-like symptoms were crossed with mice in which the taugene had been inactivated, resulting in offspring with lowerlevels of tau. In these mice a reduction of endogenous tau by
C r e d i t : J e r r y M a s o n /
P h o t o R e
s e a r c h e r s ,
I n c .
O
NN
NN
NN
NN
NN
NN
O
O
OO
OO
OO
OH
O
MeO
Donepezil
Tacrine
Rivastigmine
Physostigmine
Memantine
Galantamine
MeO
MeONH
2
CH3
H3C
H3C
H3C
HCI
H3C
H3C
H3C
CH3
CH3
CH3
CH3
H
NH2
NN
NN
Calabar Beans
Caucasian Snowdrops
Something Old... Something Blue

7/21/2019 Early History of Methylene Blue
http://slidepdf.com/reader/full/early-history-of-methylene-blue 5/6272
Reflections
as little as 50% prevented memory loss and other AD symp-toms (28). An earlier in vitro study showed MB blocks thetau-tau interaction that would lead to the formation of NFTs,
whereas other phenothiazines (i.e., neuroleptic drugs such aschlorpromazine or fluphenazine) were inactive in this respect(29). The principal investigator of this study is also a princi-pal in the start-up firm that conducted the clinical trial on MBcited at the beginning of this article (1).
Will MB prove to be the first medicine to make a real dif-ference in AD? There are formidable obstacles. The failurerate is high in clinical Phase III among compounds whichpass Phase II successfully. The extent to which MB crossesthe blood-brain barrier is unknown. Further, its rapid excre-tion via the urine and the absorption problem hinted at in
the ICAD report point to additional potential difficulties.Thus, there are good reasons for expectations to be muted.Nevertheless, if its early promise in AD should be fulfilled,MB would not be the first medicinal to come back fromobscurity. Arsenic trioxide, in use for centuries but deemedworthless in the second half of the twentieth century, is nowapproved for a rare form of leukemia. Thalidomide, the post-er-child of disastrously dangerous drugs, has been rehabili-tated as an orphan drug for multiple myeloma and erythemanodosum leprosum, a painful inflammatory complication ofleprosy. A more benign example is provided by the vitaminfolic acid, which can mask pernicious anemia and hamper itstimely diagnosis. This finding, in 1947, prompted folic acid’s
exclusion from multivitamin products. For about thirty years,the vitamin was relegated to insignificance, until researchin the 1980s and 1990s established that it prevented birthdefects such as spina bifida. As a result, fortification of allenriched grain products with folate has been a government-mandated requirement since 1998.
MB has been in use as a medicinal, to a greater or lesserextent, continuously throughout the past century. It may nowreturn to play an important therapeutic role, either per se oras a structural model for the synthesis of more effective mol-ecules to combat AD. doi:10.1124/mi.8.6.1
References1. en.wikipedia.org/wiki/Alzheimer’s_disease (Accessed Dec 3 2008)
2. www.nia.nih.gov/Alzheimers/Publications/adfact.htm (Accessed Dec 3
2008)3. www.healthline.com/galecontent/alzheimers-disease-3 (Accessed Dec 3
2008)
4. Wischik, C.M., Bentham, P., Wischik, D.J., and Seng, K.M. Tau aggre-
gation inhibitor (TAI) with Lember™ arrests disease progression in
mild and moderate Alzheimer’s disease over 50 weeks. Presented at
International Conference on Alzheimer’s disease 2008 (ICAD), Chicago,
July 29, 2008.
5. Marchione, M. Test drug shows promise in halting Alzheimer’s.
Philadelphia Inquirer , July 30, 2008, p. A6.
6. Dale, H. Paul Ehrlich. Brit. Med. J. 1, 659–665 (1954).
7. Sneader, W. Drug Discovery: The Evolution of Modern Medicines .
Chichester, UK, John Wiley & Sons, p. 250 (1985).
8. Wood, H.C., Jr. The use of methylene blue in malarial fevers. Proc. Phila.
Co. Med. Soc. 25, 281–286 (1904).
9. Grabenko, J.K. Combined methylene blue and glucose intravenoustherapy of malaria. Vrachevna Delo., Kharkov, p. 214. Abstract in JAMA
132, 481 (1946).
10. Vennerstrom, J.L., Mackler, M.T., Angerhoffer, C.K., and Williams, J.A.
Antimalarial dyes revisited: Xanthines, azines, oxazines and thiazines.
Antimic. Agents Chemother. 39, 2671–2677 (1995).
11. Sneader, W. Drug Discovery: A History . Chichester, UK, John Wiley &
Sons, p. 379 (2005).
12. Scheindlin S. The drug that launched a thousand sleds. Mol. Interv. 8,
152–158 (2008).
13. American Drug Index , 51st Ed. St. Louis, MO, Walters Kluwers Health, p.
861 (2007).
14. The Merck Index , 5th Ed. Rahway, NJ, Merck & Co. Inc., p. 353 (1940).
15. Osol, A. and Pratt, R., Editors. United States Dispensatory 27th Ed.
Philadelphia, J.B. Lippincott Company, p. 745 (1973).
16. Bodansky, O. and Gutmann, H. Treatment of methemoglobinemia. J.
Pharmacol. Exp. Ther. 90, 46–56 (1947).
17. Eldadah, M. and Fitzgerald, M. Methemoglobinemia due to skin applica-
tion of benzocaine. Clin. Pediatr. (Phila.) 32, 687–688 (1993).
18. Physicians’ Desk Reference Edition 60. Montvale, NJ, Thomson PDR, p.
1086 (2006).
19. Sweetman, S.C., Editor. Martindale: The Complete Drug Reference 35th
Ed. London, Pharmaceutical Press, pp. 331–332 (2007).
20. “Memory enhancement with oral physostigmine in Alzheimer’s disease”.
New Eng. J. Med. 308, 720–721 (1983).
21. The Merck Index 13th Edition. Whitehouse Station, NJ, Merck & Co. Inc.,
p. 771 (2001).
22. Physicians’ Desk Reference Edition 60. Montvale, NJ, Thomson, p. 2434
(2006).
23. Physicians’ Desk Reference Edition 60. Montvale, NJ, Thomson, p. 1199
(2006).

7/21/2019 Early History of Methylene Blue
http://slidepdf.com/reader/full/early-history-of-methylene-blue 6/6 2 December 2008
Volume 8, Issue 6
24. Brunton, L.L., Lazo, J.S., Parker, K.L., Editors. Goodman & Gilman’s The
Pharmacological Basis of Therapeutics 11th Edition. New York, McGraw
Hill, pp. 538–540 (2006).
25. Tiraboschi, P., Hansen, L.A., Thal, L.J., and Corey-Bloom, J. The impor-
tance of neuritic plaques and tangles to the development and evolutionof AD. Neurology 62, 1984–1989 (2004).
26. Tanzi, R.E. Tangles and neurodegenerative disease––a surprising twist.
New Eng. J. Med. 353, 1853–1855 (2005).
27. Weingarten, M.D., Lockwood, A.H., Hwo, S.-Y., and Kirschner, M.W. A
protein factor essential for microtubule asssembly. Proc. Nat. Acad. Sci.
U.S.A. 72, 1858–1862 (1975).
28. Ashe, K.H. A tale about tau. New Eng. J. Med. 357, 933–935 (2007).
29. Wischik, C.M., Edwards, P.C., Lai, R.Y. et al. Selective inhibition of
Alzheimer’s disease-like tau aggregation by phenothiazines. Proc. Nat.
Acad. Sci. U.S.A. 93, 11213–11218 (1996).
Stanley Scheindlin, DSc,holds a BS in pharmacy fromTemple University and graduate
degrees in pharmaceuticalchemistry from PhiladelphiaCollege of Pharmacy andScience (now University ofSciences in Philadelphia). Hisacademic research dealt withplant constituents and chemical
interactions of vitamins. In his pharmaceutical industry career,he handled new drug formulation developments, and laterregulatory affairs, presiding over the filing of about 100generic new drug applications and two innovative drugapplications. Now retired, his activities include volunteerwork, consulting, and writing Reflections pieces for this
journal. E-mail [email protected]
Something Old... Something Blue